
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Performance of neuraxial blockade using a midline approach can be technically difficult. It is therefore important to optimize factors that are under the influence of the clinician performing the procedure. One of these factors might be the chosen point of insertion of the needle. Surprisingly few data exist on where between the tips of two adjacent spinous processes the needle should be introduced. A geometrical model was adopted to gain more insight into this issue. Spinous processes were represented by parallelograms. The length, the steepness relative to the skin, and the distance between the parallelograms were varied. The influence of the chosen point of insertion of the needle on the range of angles at which the epidural and subarachnoid space could be reached was studied. The optimal point of insertion was defined as the point where this range is the widest. The geometrical model clearly demonstrated, that the range of angles at which the epidural or subarachnoid space can be reached, is dependent on the point of insertion between the tips of the adjacent spinous processes. The steeper the spinous processes run, the more cranial the point of insertion should be. Assuming that the model is representative for patients, the performance of neuraxial blockade using a midline approach might be improved by choosing the optimal point of insertion.
Introduction
Neuraxial blockade using a midline approach can be technically difficult. This might be, eg, due to degenerative changes of the spine of the patient or due to a limited ability of the patient to flex his hips. It is usually performed after palpation of the tips of the spinous processes above and under the intended level of entry of the needle. Several factors have been implicated to determine the difficulty of the intended puncture. Both patient-related factors – eg, age,Citation1 body mass index,Citation1 deformities of the spine,Citation2,Citation3 the ability of the patient to flex his back,Citation3 palpability of bony landmarksCitation2,Citation3 – and non-patient-related factors – eg, equipment used, experience of the person performing the procedure,Citation4 patient position chosen by the clinicianCitation1 – have been described in the literature. It would be very useful to know, how to optimize factors that are under the influence of the clinician performing the procedure because repeated attempts increase the incidence of complications and patient discomfort.Citation5-Citation7 One of these factors might be the optimal place to insert the needle. To the best of our knowledge, surprisingly few data exist on where between the tips of the spinous processes the needle should be introduced to approach the subarachnoid (SAS) or epidural space (ES) without bone contact (for simplicity, in the subsequent text we mean both the SAS and the ES, where only the ES is mentioned). Data on this subject would be very useful, eg, to instruct a resident how to perform neuraxial anesthesia when using a midline approach.
For example, PitkänenCitation8 gives no hint for an optimal point of insertion in Cousins et al’s textbook of regional anesthesia. He advises to direct the needle at 10° when performing lumbar spinal anesthesia. The same textbookCitation9 advises “[…] insertion closer to the superior spinous process and with a slight upward angulation […]” for lumbar epidural anesthesia and “[…] extreme upward angulation […]” for epidural anesthesia in the mid-thoracic region. No further details are provided here. For thoracic epidural anesthesia, Brull et alCitation10 point out that the distance travelled by the needle is modified by a more perpendicular angle. However, they do not suggest an optimal point of insertion at the different levels. According to Fettes et al, the needle should be introduced “[…] precisely in the mid-line, mid-way between the posterior spines […]” for lumbar puncture. This suggestion is not substantiated by clinical or experimental data.Citation11 In one paper it is suggested that puncture at the lumbar region should involve insertion of the needle at the superior aspect of the spinous process that lies inferior to the space to be entered.Citation12 Here, too, the authors provide no further explanation for this approach.
We hypothesize that the point of insertion of the needle determines the range of angles at which the ES can be reached (explained in ). It is assumed, that the larger this range is, the bigger the chance of successfully reaching this space in one attempt. We have tested this hypothesis in a simple geometrical model.
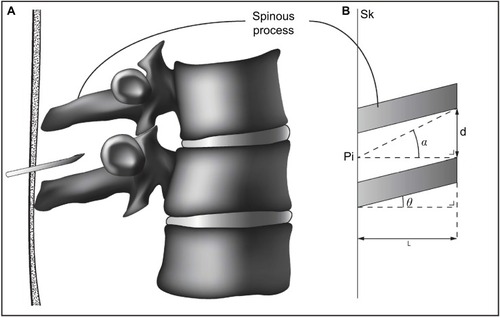
Figure 1 The adopted geometrical model: two adjacent spinous processes represented by two parallelograms.
Methods
Geometrical model
represents the model. Two adjacent spinous processes of two vertebrae (A) are represented by two parallelograms ([B], shaded areas).
The following variables were chosen in the model ():
the angle (θ) of the spinous processes relative to the virtual skin (Sk).
The distance between two adjacent spinous processes (d).
The length of the spinous processes (L) perpendicular to the Sk.
The point where the needle is inserted is Pi. The range of angles at which the ES can be reached by the tip of the needle is represented by α ().
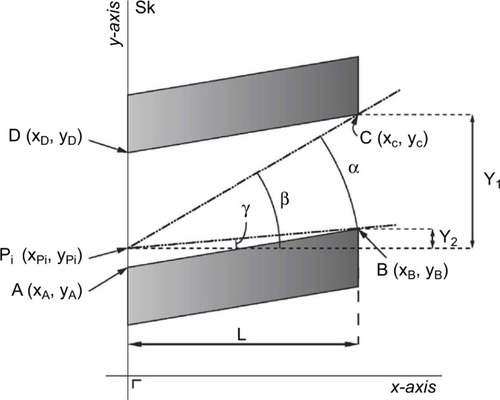
Calculation of α, : Sk represents the patient’s skin surface. Points A, B, C, and D represent the boundaries of the space between two adjacent spinous processes. Variables x and y were attributed to A, B, C, and D; for point A xA and yA, and similarly for B, C, and D. The needle is inserted at point Pi (xPi, yPi). All points were placed in a grid. The range of angles at which the ES can be reached is represented by α:
(1)
(2) and
(3)
Figure 2 Two adjacent spinous processes are depicted (shaded areas).
The variables θ, d, and L were varied over a wide range, in order to be able to make solid statements of their effects on α; θ varied from 0° to 72°. Calculations were performed in Excel spreadsheets (Microsoft Office, 2007). In all these various cases, α (y-axis) was plotted as a function of the points of insertion (x-axis, Pi) in diagrams. A total number of 196 spreadsheets were made. A representative selection of the results is shown in the results section. Data sets are available on request by email.
Results
In (left part) the angle θ (explained in ) is varied, resulting in a horizontal () to steep () position of the spinous processes relative to the Sk. In all these cases, α is maximal when Pi is chosen at the point that is the projection of the point halfway between points b and c on the skin (explained more extensively in the figure). This optimal point of insertion is represented by Pi,opt in .
Figure 3 Four sets of two adjacent spinous processes and their corresponding plots are depicted.
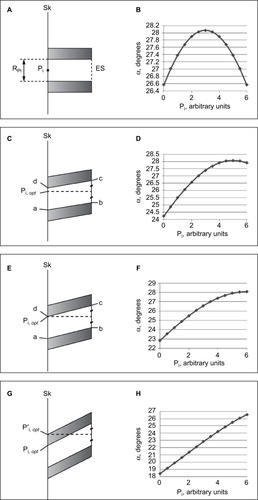
The corresponding plots, which vary in shape, are shown in (right part). When the spinous processes run horizontally, α is maximal when the point of insertion is chosen halfway between points a and d (). When θ increases, the point of insertion where α is maximal gradually shifts cranially, ie, Pi, opt approaches point d.
In the point of insertion where α is maximal corresponds with point d. This means that when steeper angles θ are chosen than in this particular situation, Pi, opt is consistently at point d, ie, the most cranial point between two adjacent spinous processes ().
According to this model, the chosen point of insertion between the spinous processes determines the value of α. This dependency is most pronounced when the spinous processes run steeply. In the situation of , the absolute increase of α – when it is compared to the least favorable point of insertion, ie, point a (compare ) is 9° (from 18° to 27°), which is a relative increase of 50%. For the situations of , these numbers are 1° and 4%, 4° and 17%, and 6° and 27%, respectively.
Discussion
Our geometrical model clearly demonstrated, that the range of angles at which the ES can be reached, is dependent on the point of insertion between the tips of the spinous processes when using a midline approach. Many anesthesiologists perform both lumbar and thoracic neuraxial blockade by using a midline approach.Citation13 Therefore, this finding is relevant for daily anesthetic practice. Especially in patients where neuraxial anesthesia turns out to be technically difficult – eg, due to degenerative changes of the spine – choosing the optimal point of insertion may enhance the chance of successfully reaching the ES.
Although we studied the median approach in neuraxial anesthesia, some anesthesiologists advocate a paramedian approach. Comparative studies in the literature, we found, usually focused on the lumbar region of the spine. Indeed, some studies found an advantage for the paramedian approach eg, in terms of a higher success rate at the first puncture attempt,Citation14 or time needed to reach the ES.Citation15 Other studies, however, could not confirm that the paramedian approach is superior to the median approach. These studies were for example looking at predictors for success during the first puncture attemptCitation7 or the incidence of post-dural puncture headache.Citation16 Apparently, more and larger studies are needed to answer the question ‘which approach under what conditions should be preferred’.
According to our results, the optimal point of insertion of the needle shifts cranially when the spinous processes run steeper. Choosing a more cranial point of insertion of the needle will not only increase the range of angles at which the SAS and ES can be reached, but will also shorten the puncture route.
The borders of spinous processes are not smooth, straight lines in vivo and adjacent spinous processes do not run perfectly parallel to each other as in our model. However, these simplifications enabled us to make calculations and eventually enabled us to test our hypothesis that the point of insertion of the needle is an important determinant for the chance of reaching the ES.
Ultrasound imaging is increasingly used for neuraxial blockade. However, many – if not the majority of – anesthesiologists still use the landmark-guided technique, probably since it is relatively effective and the use of ultrasound requires additional skills.Citation17 It would be of interest to investigate if ultrasound can be helpful to find the optimal point of insertion of the needle.
Previously, it has been shown that a change in flexion of the hips changes the curvature of the spine.Citation18 Consequently, a change in the curvature of the spine, will probably also change the width between adjacent spinous processes. Indeed, several papers describe the influence of patient positioning on the interspinous space width in the lumbar region of the spine.Citation19-Citation22 We are not aware of studies of the thoracic region of the spine. For example, in the study by Fisher et al, the absolute increase in width between lumbar interspaces was 1 mm or less in 60% (21 of 35 measurements) of the studied cases and 1 to 2 mm in 31%. The corresponding relative increases varied from 5% to 14% (cases with an absolute increase of 1 mm or less) and from 12% to 33% (cases with an absolute increase of 1 to 2 mm).Citation19 In the study by Sanodoval et al (when comparing the sitting position with unsupported feet to sitting with supported feet), the absolute increase in width between spinous processes was 1 mm or less in nine of 16 cases, 1 to 2 mm in four of 16 cases, and more than 2 mm in three cases (being 2.1, 2.4, and 3.6 mm respectively).Citation20 Since our model did not take the role of patient positioning into account, our results should be interpreted with caution. On the other hand, as we discussed above, the changes in interspinous space width when changing from a position with no or limited hip flexion to more hip flexion seem to be limited, both in absolute and in relative numbers. Furthermore, the influence of changing patient positioning on the ease of performing a neuraxial blockade seems also to be limited.Citation23-Citation25 From the available data, it is difficult to predict how changes in the spinal curvature and forthcoming changes in the angulations of the spinous processes will affect the optimal point of needle insertion. Therefore, it is worthwhile to test the findings in our model in patients, both with and without flexion of their hips. Results from these future studies may further substantiate a scientific rationale, how to perform neuraxial anesthesia when using a midline approach.
Acknowledgments
The authors wish to thank Koen Terra MSc for preparation of the figures.
Disclosure
The authors report no conflicts of interest in this work.
References
- RuzmanTGulamDHarsanji DrenjancevicIVenzera-AzenicDRuzmanNBurazinJFactors associated with difficult neuraxial blockadeLocal Reg Anesth20147475225336987
- AtallahMMDemianADShorrabAADevelopment of a difficulty score for spinal anaesthesiaBr J Anaesthesia2004923354360
- GuglielminottiJMentréFBedairiaEMontravesPLamgroisDDevelopment and evaluation of a score to predict difficult epidural placement during laborReg Anesth Pain Med201338323323823518864
- KimJHSongSYKimBJPredicting the difficulty in performing a neuraxial blockadeKorean J Anaesthesiol2011615377381
- PuolakkaRHaasioJPitkänenMTKallioMRosenbergPHTechnical aspects and postoperative sequelae of spinal and epidural anesthesia: a prospective study of 3,230 orthopedic patientsReg Anesth Pain Med200025548849711009234
- KangXHBaoFPXiongXXMajor complications of epidural anesthesia: a prospective study of 5083 cases at a single hospitalActa Anaesthesiol Scand201458785886624961586
- de FilhoGRGomesHPda FonsecaMHHoffmanJCPederneirasSGGarciaJHPredictors of successful neuraxial block: a prospective studyEur J Anaesthesiol200219644745112094920
- PitkänenMSpinal (subarachnoid) blockadeCousinsMJCarrDBHorlockerTTBridenbaughPOCousins and Bridenbaugh’s neural blockade in clinical anesthesia and pain medicine4th edLippincott Williams & Wilkins2009213240
- VeeringBTCousinsMJEpidural neural blockadeCousinsMJCarrDBHorlockerTTBridenbaughPOCousins and Bridenbaugh’s neural blockade in clinical anesthesia and pain medicine4th edLippincott Williams & Wilkins2009241295
- BrullRMacFarlaneAJChanVWSpinalEpiduralCaudal Anesthesia:Miller’s anesthesia8th edPhiladelphia, PAElsevier Saunders201516841720
- FettesPDJanssonJRWildsmithJAFailed spinal anaesthesia: mechanisms, management, and preventionBr J Anaesth2009102673974819420004
- BoonJMAbrahamsPHMeiringJHWelchTLumbar puncture: anatomical review of a clinical skillClin Anat200417754455315376294
- WantmanAHancoxNHowellPRTechniques for identifying the epidural space: a survey of practice amongst anaesthetists in the UKAnaesthesia200661437037516548958
- RabinowitzABourdetBMinvilleVThe paramedian technique: a superior initial approach to continuous spinal anesthesia in the elderlyAnesth Analg200710561855185718042894
- LeedaMStienstraRArbousMSLumbar epidural catheter insertion: the midline vs. the paramedian approachEur J Anaesthesiol2005221183984216225718
- MosaffaFKarimiKMadadiFKhoshnevisSHDaftari BesheliLEajaziAPost-dural puncture headache: a comparison between median and paramedian approaches in orthopedic patientsAnesth Pain Med201112666925729658
- ChinKJKarmakarMKPengPPUltrasonography of the adult thoracic and lumbar spine for central neuraxial blockadeAnesthesiology201111461459148521422997
- StokesIAAberyJMInfluence of the hamstring muscles on lumbar spine curvature in sittingSpine (Phila Pa 1976)1980565255287466461
- FisherALupuLGurevitzBBrillSMargolinEHertzanuYHip flexion and lumbar puncture: a radiological studyAnaesthesia200156326226611251435
- SandovalMShestakWStürmannKHsuCOptimal patient positioning for lumbar puncture, measured by ultrasonographyEmerg Radiol200410417918115290485
- AboAChenLJohnstonPSantucciKPositioning for lumbar puncture in children evaluated by bedside ultrasoundPediatrics20101255e1149115320403933
- CapognaGCellenoDSimonettiCLupoiDAnatomy of the lumbar epidural region using magnetic resonance imaging: a study of dimensions and a comparison of two posturesInt J Obst Anesth1997629710015321289
- FisherKSArnholtATDouglasMEVandiverSLNguyenDHA randomized trial of the traditional sitting position versus the hamstring stretch position for labor epidural needle placementAnesth Analg2009109253253419608828
- MohammadiSSHassaniMMarashiSMComparing the squatting position and traditional sitting position for ease of spinal needle placement: a randomized clinical trialAnesth Pain Med201442e1396924790901
- BiswasBKAgarwalBBhattaraiBDeySBhattacharyyaPStraight versus flex back: Does it matter in spinal anaesthesia?Indian J Anaesth201256325926422923825