
Abstract
Surgery is a critical period in the survival of patients with cancer. While resective surgery of primary tumors has shown to prolong the life of these patients, it can also promote mechanisms associated with metastatic progression. During surgery, patients require general and sometimes local anesthetics that also modulate mechanisms that can favor or reduce metastasis. In this narrative review, we summarized the evidence about the impact of local, regional and general anesthesia on metastatic mechanisms and the survival of patients. The available evidence suggests that cancer recurrence is not significantly impacted by neither regional anesthesia nor volatile or total intravenous anesthesia.
Keywords:
Introduction
Cancer is a major cause of mortality worldwide with an estimated 9.6 million deaths per year.Citation1 Lung, colorectal, stomach and liver are the most common types of cancer and account for nearly half of cancer-related deaths. By 2040, it is estimated that there will be approximately 30 million new cases of cancer.Citation1 It is projected that a large proportion of patients will need surgery for tumor resection despite rapid and substantial advances in treatments, including chemotherapy, targeted therapy, radiotherapy, and immunotherapy.
Surgery causes the local and systemic release of inflammatory mediators and promotes high levels of angiogenesis. Also, surgery is associated with high concentrations of circulating catecholamines and immunosuppression that can last for days or weeks postoperatively, making this a period of high vulnerability for complications and tumor progression.Citation2,Citation3 Some evidence suggests that certain anesthetics or anesthesia techniques may also affect the growth of the so-called minimal residual disease.Citation4,Citation5 Total intravenous anesthesia (TIVA) with propofol was associated with prolonged overall survival in patients with metastatic and non-metastatic cancers.Citation6 Local anesthetics and regional anesthesia can also modify cancer progression by limiting inflammation, immunosuppression, and angiogenesis.Citation4,Citation7,Citation8 However, a recently published randomized controlled trial concluded that compared to sevoflurane-based general anesthesia, regional anesthesia did not improve the survival nor reduced recurrences after breast cancer surgery.Citation9
Investigators have hypothesized that the technique of general anesthesia (total intravenous vs volatile-based or regional anesthesia) has a significant impact on caner progression. In this narrative review, we will discuss the evidence of the impact of different anesthetics and anesthesia techniques on metastatic progression after surgery. Our work will include current basic, translational and clinical studies addressing the effects and association between different anesthetics and cancer progression.
Perioperative Metastasis Formation
The growth of metastatic colonies outside the primary tumor is a multi-step process. Colonization of distant sites by circulating tumor cells (CTCs) is a rate-limiting step during the metastatic process. In general, it is well accepted that metastasis may be part of a dominant clonal subpopulation that originated within the primary tumor.Citation10 By virtue of tumor-secreted factors and tumor-secreted exosomes, the microenvironment of distant organ sites is modified into prometastatic niches that contain recruited stem cells and stromal cells.Citation11
A critical event in the metastasis process is the epithelial-mesenchymal transition (EMT) that CTCs undergo to increase mobility and invasiveness (). The EMT process is orchestrated by transcription factors (ie, Snail, Slug, Twist, and Zeb1) that, in turn, respond to extracellular molecular signals occurring in the nearby tumor stroma such as inflammation.Citation12 Once in the bloodstream, CTCs interact with other cells, including platelets and lymphocytes. Platelets can provide shelter to CTCs and hide them from lymphocytes such as natural killer (NK) cells. Also, activated platelets can release soluble mediators such as transforming-growth factor beta (TGF-β), platelet-derived growth factor (PDGF), and adenosine triphosphate (ATP). These factors are known to suppress the killing activity of NK cells and enhance vascular permeability.Citation12 Once CTCs extravasate via transendothelial migration (TEM), they find the extracellular tissue stroma where they may reside and proliferate. Some of those cells in the new forming metastatic colony retain features of cancer stem cells (CSC), which have tumor-initiating ability and can drive colony expansion.Citation12
Figure 1 Perioperative events that influence tumor metastasis and cancer recurrence. Surgery for tumor resection triggers the release of catecholamines, immunosuppression, and angiogenesis. It has been speculated that these factors facilitate epithelial-mesenchymal transition (EMT) and promote a conducive microenvironment (tumor niche) for cells to migrate, invade and proliferate.
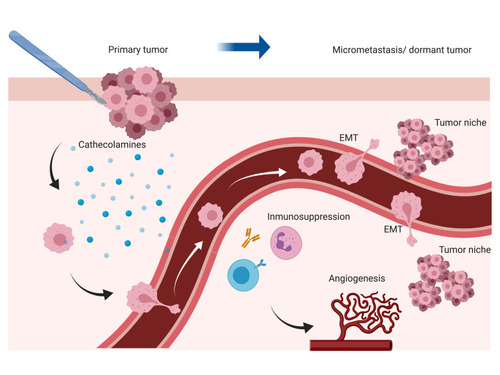
It is speculated that micrometastasis or dormant colonies are contained by immune surveillance or by the lack of supporting factors that can sustain cell proliferation.Citation13 Thus, the transition from single cell or colony of cells to micrometastasis to clinically relevant metastasis can take months to years.Citation12,Citation14 Remarkably, surgery can facilitate the homing of CTCs and growth of micrometastasis by releasing cytokines, angiogenic factors, and catecholamines. In mice, surgery-induced inflammation promoted the outgrowth of T cell restricted distant tumors by mobilizing myeloid cells and recruiting tumor-associated macrophages.Citation15
Neutrophil extracellular traps (NETs) has been recognized as a mechanism that facilitates colonies formation. NETs are web-like structures formed by DNA fragments and proteins that can sequester CTCs.Citation16,Citation17 In mice, surgery promoted NETs and micrometastasis. When mice were treated daily with DNAase after surgery, it reduced tumor growth.Citation16 Circulating neutrophils entrapped in clumps formed by platelets or in the extracellular matrix can also provide a conducive environment for CTCs to survive by further suppressing the activity of NK cells.Citation12
Several studies have shown a decrease in the number and function of circulating NK cells after surgery.Citation3 Subsequently, investigations revealed that surgery-induced reduction in circulating NK killing activity could promote metastasis ().Citation18 Interestingly, it has been demonstrated that the transcriptome profile of circulating NK cells is significantly different from NK cells located in metastasis suggesting that the role of NK cells in the micrometastatic niche during surgery might be different from those circulating.Citation19
It is worth considering that the metastatic process is also affected by factors including the use, timing, and completion of adjuvant therapies (ie, chemotherapy, radiation, and immunotherapies). For instance, it is now well understood that for some malignancies, delaying the return to oncological therapies after surgery has a significant impact on patients’ survival.Citation20 Another important factor associated with cancer progression is the occurrence of complications in the postoperative period and perioperative blood transfusions.Citation21,Citation22 Therefore, it has been suggested that patients undergoing cancer surgery should be evaluated and treated by a multidisciplinary team dedicated to assess modifiable risks and propose a coordinated plan of measures (ie, anemia treatment) tailored to reduce postoperative complications and accelerate recovery.Citation23
In the following sections, we will discuss how anesthetics may or may not interfere with the process involved in the metastatic process and metastatic cancer progression.
Local Anesthetics
Local anesthetics can act on several steps of the metastatic process (). The administration of intravenous lidocaine (1.5 mg/kg followed by infusion of 2 mg/kg) under sevoflurane anesthesia reduced postoperative lung metastasis by decreasing serum concentrations of the metalloproteinase (MMP)-2 in a murine surgical breast cancer model.Citation24,Citation25 It was speculated that changes in MMP-2 resulted in a reduced ability of CTCs to form metastasis.Citation24 Local anesthetics also impair the movement of malignant cells in vitro.Citation26,Citation27 As an example, ropivacaine inhibited migration and invasion of esophageal and colorectal cancer cells.Citation26 Although, the anti-metastatic effects of ropivacaine in esophageal cancer cells were independent of voltage-gated sodium channel (VGSCs) blockade and mediated by inhibition of RhoA, Rac1 and Ras, they were dependent on Nav1.5 blockade in colorectal cancer cells.Citation26,Citation28
Figure 2 Several mechanisms have been associated with the anti-metastatic effects of local anesthetics. Intracellular they inhibit signaling events linked to angiogenesis, migration, and invasion.
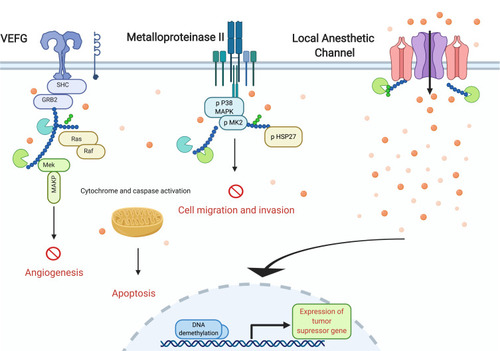
VGSCs regulate the metastatic activity of cancer cells. These channels are located in the cell membrane, in particular in cellular structures called invadopodia, which are essential for degrading the extracellular matrix.Citation29 In the invadopodia, VSGCs promote polymerization of actin filaments via Src signaling.Citation29 In vitro studies demonstrate that downregulation of VSGCs via shRNA inhibits tumor invasion by blocking the invadopodia.Citation30
Local anesthetics have shown anti-angiogenic effects. Lidocaine (30 mg/kg) inhibited tumor growth in mice bearing melanoma tumors by inducing apoptosis in endothelial cells.Citation31 In these cells, lidocaine suppressed VEGF-increased phosphorylation of VEGF receptor 2.Citation31 Similarly ropivacaine induced apoptosis on tumor-associated endothelial cells by inducing mitochondrial dysfunction.Citation32 Local anesthetics also modulate inflammation (). Notably, lidocaine reduced pro-inflammatory cytokines [ie, tumor necrosis factor (TNFα) and interleukin-6 (IL-)] in a mice model having breast cancer surgery.Citation33 Furthermore, lidocaine and ropivacaine inhibited migration and invasion of lung cancer cells by inhibiting TNFα- induced phosphorylation of Src and reducing the expression of ICAM-1 (glycoprotein essential for cellular adhesion).Citation34,Citation35 A reduction in the concentrations of pro-inflammatory concentrations is observed in humans receiving intravenous lidocaine during surgery.Citation36
Figure 3 Effect of local anesthetics on immune and inflammatory cells. Local anesthetics modulate the activity of different immune cells. They potentiate natural killer cells cytotoxicity, facilitate antigen presentation, and have shown to modulate the function of neutrophils, macrophages, and dendritic cells.
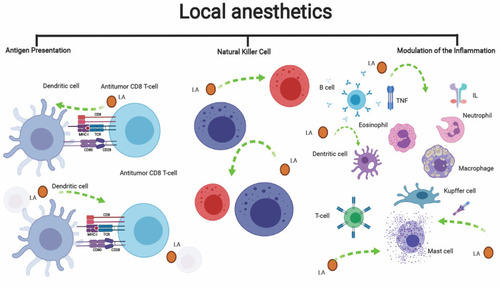
Increased vascular permeability, as it occurs during periods of exaggerated inflammation, facilitates TEM and can promote the implant of metastatic cells. The intravenous administration of lidocaine (1 and 3 mg/kg) to mice inoculated with LPS significantly reduced lung permeability. The postulated mechanisms included a reduction of inflammatory cytokines (TNFα, IL-6, and MCP-1) and impairment of antigen presentation, a process done by dendritic cells (DC) ().Citation37,Citation38 As an example, lidocaine inhibited the expression of proinflammatory cytokines in bone marrow-derived DC that were stimulated with LPS.Citation38
Inflammation also induces DNA methylation, a mechanism linked with metastasis.Citation39,Citation40 Local anesthetics such as lidocaine and ropivacaine induce, in vitro, DNA demethylation in breast cancer cells which correlates with the overexpression of the tumor suppressor genes (RARB2 and RASSF-1A).Citation41–Citation43 Lidocaine also induces modulation of microRNAs.Citation44–Citation47 Treatment of lung cancer cells with 8 mM of lidocaine significantly increased the expression of miR-539, which then induced the downregulation of the epidermal growth factor receptor (EGFR) and suppressed migration and invasion.Citation45 The intravenous injection of lidocaine (1.5 mg/kg) to mice bearing retinoblastoma caused significant tumor reduction by inducing the expression of miR520a-3p and inhibiting EGFR.Citation46 MicroRNAs are also involved in chemo-resistance. Lidocaine, in vitro, inhibited the expression of miR-21 and sensitized chemo-resistant lung cancer cells to cisplatin.Citation48 On the other hand, lidocaine by inducing the expression of miR-493 downregulated the transcription factor Sox-4, which ultimately sensitized melanoma cells to the effect of 5-fluorouracil.Citation49
Another described mechanism that can contribute to the anti-metastatic effects of local anesthetics include the induction of oxidative stress, and a reduced formation of MMP-9.Citation30,Citation34,Citation35,Citation50,Citation51 Local anesthetics act on different components of the innate and adaptive immune system has been investigated experimentally and in humans. We demonstrated that lidocaine in clinically relevant concentrations increased the in vitro cytotoxic activity of NK cells by stimulating the release of perforins ().Citation52,Citation53 In humans with abdominal pain, an intravenous injection of 1 mg/kg of lidocaine preserves the count and function of circulating NK cells.Citation54 Few studies have investigated the impact of intravenous lidocaine on lymphocytes counts or function during and after oncologic surgery.Citation54,Citation55 Wang et al conducted a randomized controlled trial (RCT) in women having a radical hysterectomy and compared the effects of lidocaine versus placebo on peripheral blood lymphocytes. The postoperative proliferative rate of lymphocytes was higher in patients treated with lidocaine.Citation55 The authors speculated that lidocaine protected lymphocytes by preserving the IFN-g/IL-4 ratio and by decreasing inflammation, as demonstrated by lower circulating concentrations of the high mobility group box-1 protein.Citation55 Similarly, patients with abdominal pain had a preserved CD4/CD8 ratio, and normal T and B cell counts after injection of 1.5 mg/kg of lidocaine.Citation54
Local (Infiltration or Intravenous) vs General Anesthesia: Human Studies
To date, there is no strong evidence from human studies indicating that local anesthesia modifies oncologic outcomes after cancer surgery (). Schalengenhauff et al included 4329 patients with melanoma and showed that the use of general anesthesia was associated with a decreased survival rate.Citation56 A more recent retrospective study suggests that tumescent local anesthesia, in comparison to general anesthesia, is associated with longer metastasis-free survival also after melanoma surgery. However, overall and disease-free survival were not affected.Citation57
Table 1 Summary of Clinical Studies, Systematic Reviews and Meta-Analysis on the Impact of Regional Anesthesia/Analgesia in Cancer Outcomes
Zhang et al recently assessed the impact of intravenous lidocaine on cancer progression. The authors reported that the intraoperative use of lidocaine was associated with longer overall survival in patients undergoing pancreatic cancer surgery.Citation58 Several randomized controlled trials are being conducted in patients with breast (NCT01204242; NCT01916317), pancreatic (NCT0408278), lung (NCT04074460) and colorectal (NCT04074460) cancers.
Regional vs Opioid-Based Analgesia: Humans Studies
Since 2008 there has been an increase in human studies testing the impact of regional anesthesia on cancer recurrence or recurrence-free survival after surgery.Citation9,Citation56,Citation59–Citation89 The findings are controversial.Citation8,Citation59,Citation90 However, a recent RCT could not confirm the anti-cancer effects of regional anesthesia in women undergoing breast cancer surgery.Citation9 Patients were randomized to either regional anesthesia (preferentially paravertebral block) with propofol sedation or sevoflurane/opioid-based general anesthesia.Citation9 It can be speculated that regional anesthesia probably did not produce a robust immunomodulatory or anti-inflammatory effect and/or, the concentrations of local anesthetics in micrometastatic niches may not have been high enough to produce significant effects.Citation91–Citation93 In line with this notion, Kim et al concluded that continuous local wound infiltration did not impact one-year recurrence rate after colorectal cancer surgery despite a statistically significant improvement in NK cell function postoperatively.Citation65 Another factor was the short-term exposure to the intervention. Perioperative immune suppression and inflammation can last beyond the “protective” effects of regional anesthesia. Our group demonstrated in patients having major oncologic surgery, the serum IL-6 levels do not return to preoperative concentrations even two weeks after surgery.Citation94 Furthermore, the immune “protective” effects attributed to regional anesthesia in sub-studies of Sessler’s trial indicate that such benefits were not clinically relevant.Citation95,Citation96 Other studies have been designed to test whether regional anesthesia can improve survival or reduce recurrence after bladder (NCT:03597087), non-small cell lung cancer (NCT02840227), colorectal (NCT02786329), and pancreas (NCT03245346).
In summary, the available evidence indicates that the impact of regional anesthesia on cancer recurrence might be negligible or not existent. It remains unknown whether perioperative intravenous lidocaine infusion has any impact on cancer progression.
General Anesthetics and Cancer Progression
Volatile Anesthetics
General anesthetics modify intracellular signaling mechanisms involved in metastasis. Isoflurane (1%-2%) increases migration and invasion of lung cancer cells by promoting Akt/mTOR activation and by promoting the release of MMPs.Citation97 In ovarian cancer cells, two-hour exposure to isoflurane (1.7 MAC), sevoflurane (1.7 MAC), or desflurane (1.7 MAC) stimulated the mRNA expression of VEGF-A, CXCR2, TGF-β and MMP-11, which correlated with increased cell migration.Citation98 Also, in ovarian cancer cells, isoflurane (2%) increased the release of VEGF, angiopoietin-1 and MMP-2, and 9.Citation99 Sevoflurane (3.6%) stimulated the metastatic potential of renal cancer cells and induced their chemo-resistance to cisplatin. These pro-metastatic effects were linked to an increase in the expression of TGF-B1, TGF-BRII and downregulation of Smad3.Citation100 In a melanoma mice model, isoflurane (1.3 MAC) anesthesia promoted pulmonary metastasis.Citation101
As mentioned previously, platelets may play a critical role in CTCs’ ability to survive in the bloodstream and attached the endothelium. Lung cancer cells co-cultured with platelets obtained from patients anesthetized with sevoflurane or isoflurane showed increased invasive properties compared to cancer cells incubated with control platelets.Citation102 Similarly, the culture of colorectal or breast cancer cells with serum obtained from patients receiving sevoflurane anesthesia promoted cell survival in comparison to the serum from propofol-treated patients.Citation103,Citation104
Volatile anesthetics can also impair the immune surveillance system. In animals, volatile anesthetics inhibit the function of NK cells, which correlates with an increased metastatic burden.Citation105 A reduction in the expression of the adhesion molecule leukocyte-associated antigen-1 and decrease in cell-to-cell contact with their target cancer cells has been implicated in the suppressive effects of isoflurane and sevoflurane on NK cells’ activity.Citation106 Interestingly, Meier et al suggested that the impact of volatile anesthetics such as isoflurane on the immune system are sex-depended.Citation107 For instance, when male mice were treated with isoflurane, the author observed not only faster tumor growth compared to controls but also faster tumor growth compared to female counterparts.Citation107 The investigators demonstrated that an immune-mediated mechanism was implicated in their findings since melanoma growth was absent in mice lacking functional T and B cells.Citation107
In vitro and animal studies have also demonstrated that general anesthetics may have anti-metastatic effects.Citation108,Citation109 High concentrations (5% and 10%) of sevoflurane inhibited migration and invasion of osteosarcoma cells, which was associated with the inhibition of EMT markers, including fibronectin and N-cadherin.Citation108 Similarly, sevoflurane (4.1%) inhibited glioma cell migration by inducing the expression of miR-124-3p and suppressing ROCK signaling.Citation109 Colorectal cancer cells also exposed to 1% of sevoflurane showed impaired migration and invasion; an effect that was mediated by inhibition of both, miR-203 expression and ERK signaling.Citation110 Under in vitro hypoxic conditions, sevoflurane (3.5%) suppressed the ability of lung cancer cells to migrate and invade the extracellular matrix by inhibiting the expression of (hypoxia-inducible factor) HIF-1α, which resulted in low levels of XIAP and survivin.Citation111 However, Gallyas et al could not demonstrate that isoflurane influenced the expression of HIF-1α in renal cancer cells.Citation112
Propofol
Propofol is the most common hypnotic used for TIVA. Most in vitro and in vivo animal studies indicate that propofol has significant anti-metastatic effects.Citation113,Citation114 One of the proposed mechanisms is the downregulation of the STAT3/HOTAIR signaling pathway, which suppresses transcription factors Slug and HIF-1α and induces silencing of the NET1 gene; all changes associated with decreased migration and invasion in cancer cells. A second mechanism involves the upregulation of miR-124-3p.1, miR-135b, miR-361, miR-410-3p, miR-328, and lncRNA DGCR5. A consequence of those epigenetic changes is in vitro inhibition of EMT, which correlates with low levels of N-cadherin and MMPs.Citation113
Adhesion molecules located on the surface of endothelial cells are needed to initiate TEM. HUVEC cells treated with different concentrations (5, 25, and 50 µM) of propofol showed low levels of the adhesion molecules E-selectin, VCAM-1, and ICAM-1. These changes in the expression of the adhesion molecules correlated with a reduction in the expression of HIF-1α, and inhibition of Akt and CaMKII phosphorylation.Citation114 Propofol also has anti-angiogenesis effects as demonstrated in experiments in which it suppressed the invasion of endothelial cells and vessel formation.Citation115
The proposed mechanisms behind the anti-angiogenic effects of propofol include the downregulation of S100A4 in endothelial cells and inhibition of the release of VEGF from cancer cells.Citation115,Citation116 Sen et al conducted an RCT to investigate the effect of propofol in combination with regional analgesia (in comparison to sevoflurane anesthesia) on serum concentrations of VEGF in patients having lung cancer surgery.Citation117 Patients receiving sevoflurane had significantly higher concentrations of VEGF.Citation117 Lastly, a proteomic analysis from head and neck cancers demonstrated that the tumors from patients who received sevoflurane anesthesia had higher expression HIF-2α and phosphorylated p38 MAPK in comparison to those receiving propofol.Citation118
Propofol can protect against immunosuppression by promoting cytotoxicity activity of NK cells, decreasing pro-inflammatory cytokines and inhibiting prostaglandin E2 (PGE2) and cyclooxygenase (COX) activity. In vitro, propofol stimulated the function and triggered the proliferation of NK cells obtained from healthy subjects and patients with cancer. Such effect on NK cells has been linked to an increase in the expression of granzyme B, IFNγ, and activating surface receptors (CD16, NKp30, NKp44, and NKG2D) as well as a reduction in the formation of PGE2.Citation119–Citation121 The beneficial effect of propofol in tumor metastasis has been demonstrated in animals. When rats having surgery were anesthetized with propofol the function of NK cells remained unchanged and metastatic formation was lower than animals receiving volatile anesthetics.Citation105
In women undergoing breast or cervical cancer surgery, the use of propofol for TIVA in combination with regional anesthesia increased the number of NK and T helper cells in the primary tumor tissue and it was associated with significantly less lymphopenia.Citation96 Similar findings were observed in circulating lymphocytes of surgical patients with tongue cancer who received TIVA in comparison to sevoflurane.Citation122,Citation123 In contrast two independent groups of investigators, did not observe any significant changes cytokines (IL-6, IL-10, and IL-12 TGF- β) and in regulatory T cell cluster differentiation in women randomized to have breast cancer surgery under TIVA or sevoflurane general anesthesia.Citation124,Citation125 Similarly, inflammatory and immune scores were not different between patients who received general volatile versus TIVA for pancreatic cancer surgery or during cytoreduction with hyperthermic intraperitoneal chemotherapy.Citation126,Citation127
TIVA vs Volatile Anesthesia: Human Studies
Because of the anti-metastatic effects of TIVA in experimental conditions, there has been a growing interest in translating such beneficial effects into human studies.Citation6,Citation9,Citation85,Citation125,Citation128–Citation142 The most extensive study was conducted by Wigmore et al, who retrospectively reviewed the impact of propofol-based general anesthesia vs volatile anesthesia in more than 7000 patients.Citation6 The authors reported a significant benefit in overall survival (HR 95% CI: 1.59, 1.30–1.95) in patients receiving propofol, even after adjusting for metastatic disease.Citation6 Several much smaller retrospective studies have demonstrated similar results (). In 2019, a meta-analysis of 10 retrospective studies concluded that the use of TIVA during cancer surgery is associated with significant improvements in recurrence-free and overall survival.Citation140 However, TIVA was associated with the most significant impact on the survival of patients with gastrointestinal malignancies.Citation140 Since the meta-analysis publication, two retrospective studies that included over 2000 patients did not show any association between TIVA and longer survival. Also, data from an RCT (TIVA vs sevoflurane anesthesia) of patients undergoing breast cancer surgery could not demonstrate differences in 2 years recurrence-free and overall survival. However, survival was not the primary endpoint of the study, which also lacked significant statistical power.Citation125 Our group investigated differences in survival in patients receiving different volatile anesthetics during glioblastoma surgery.Citation136 We observed no association between the use of desflurane or isoflurane in progression-free and overall survival.Citation136
Table 2 Summary of Clinical Studies Comparing TIVA vs Inhalational Anesthesia with Respect to Cancer Outcomes
The VAPOR-C trial (NCT04074460) is a RCT designed to investigate the effect of TIVA versus sevoflurane anesthesia on cancer recurrence in patients having surgery for lung or colorectal cancers.Citation143 The GA-CARES (NCT03034096) study is also a large clinical trial that will randomize patients to TIVA versus volatile anesthesia. The primary endpoint is all-cause mortality. Similar studies also being conducted in patients with pancreatic (NCT03447691) and breast (NCT02839668) cancers.
Conclusion
The perioperative period is a time of vulnerability for patients with cancer because it can promote the seeding of CTCs or the growth of micrometastatic tumors. The evidence from experimental laboratory studies demonstrates that anesthetics can modulate the metastatic behaviors of cancer cells. Anesthetics can also affect immune surveillance and inflammatory responses. Nevertheless, it is less clear about the actual clinical relevance of such changes in patients with cancer progression and patient’s survival.
We think that the strength of evidence is weak to recommend the use of TIVA to improve cancer-related or overall survival after oncologic surgery. As for regional anesthesia, there is strong evidence to conclude that the impact of paravertebral blocks does not influence cancer recurrence after breast cancer surgery. The findings of ongoing and future randomized control trials will bring light on whether an anesthetic technique modifies the long-term survival of patients who had surgery for cancer.
Disclosure
The authors declare no conflicts of interest.
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.2149230207593
- Cata JP, Bauer M, Sokari T, et al. Effects of surgery, general anesthesia, and perioperative epidural analgesia on the immune function of patients with non-small cell lung cancer. J Clin Anesth. 2013;25(4):255–262. doi:10.1016/j.jclinane.2012.12.00723659826
- Ramirez MF, Ai D, Bauer M, et al. Innate immune function after breast, lung, and colorectal cancer surgery. J Surg Res. 2015;194(1):185–193. doi:10.1016/j.jss.2014.10.03025475022
- Cata JP, Gottumukkala V, Sessler DI. How regional anesthesia might reduce postoperative cancer recurrence. Eur J Pain Suppl. 2012;5(S2):345–355. doi:10.1016/j.eujps.2011.08.017
- Hiller JG, Perry NJ, Poulogiannis G, Riedel B, Sloan EK. Perioperative events influence cancer recurrence risk after surgery. Nat Rev Clin Oncol. 2018;15(4):205–218. doi:10.1038/nrclinonc.2017.19429283170
- Wigmore TJ, Mohammed K, Jhanji S. Long-term survival for patients undergoing volatile versus IV anesthesia for cancer surgery: a retrospective analysis. Anesthesiology. 2016;124(1):69–79. doi:10.1097/ALN.000000000000093626556730
- Novy DM, Nelson DV, Koyyalagunta D, Cata JP, Gupta P, Gupta K. Pain, opioid therapy, and survival: a needed discussion. Pain. 2019.
- Wirz S, Schenk M, Kieselbach K. Schmerztherapeutische Aspekte bei Tumoroperationen. Anasthesiol Intensivmed Notfallmed Schmerzther. 2018;53(10):704–717. doi:10.1055/s-0043-10460030423596
- Sessler DI, Pei L, Huang Y, et al. Recurrence of breast cancer after regional or general anaesthesia: a randomised controlled trial. Lancet. 2019;394(10211):1807–1815. doi:10.1016/S0140-6736(19)32313-X31645288
- Naxerova K, Jain RK. Using tumour phylogenetics to identify the roots of metastasis in humans. Nat Rev Clin Oncol. 2015;12(5):258–272. doi:10.1038/nrclinonc.2014.23825601447
- Raskov H, Orhan A, Salanti A, Gogenur I. Premetastatic niches, exosomes and circulating tumor cells: early mechanisms of tumor dissemination and the relation to surgery. Int J Cancer. 2019.
- Lambert AW, Pattabiraman DR, Weinberg RA. Emerging biological principles of metastasis. Cell. 2017;168(4):670–691. doi:10.1016/j.cell.2016.11.03728187288
- Sosa MS, Bragado P, Aguirre-Ghiso JA. Mechanisms of disseminated cancer cell dormancy: an awakening field. Nat Rev Cancer. 2014;14(9):611–622. doi:10.1038/nrc379325118602
- Massague J, Obenauf AC. Metastatic colonization by circulating tumour cells. Nature. 2016;529(7586):298–306. doi:10.1038/nature1703826791720
- Krall JA, Reinhardt F, Mercury OA, et al. The systemic response to surgery triggers the outgrowth of distant immune-controlled tumors in mouse models of dormancy. Sci Transl Med. 2018;10(436):eaan3464. doi:10.1126/scitranslmed.aan346429643230
- Tohme S, Yazdani HO, Al-Khafaji AB, et al. Neutrophil extracellular traps promote the development and progression of liver metastases after surgical stress. Cancer Res. 2016;76(6):1367–1380. doi:10.1158/0008-5472.CAN-15-159126759232
- Eustache JH, Tohme S, Milette S, Rayes RF, Tsung A, Spicer JD. Casting A wide net on surgery: the central role of neutrophil extracellular traps. Ann Surg. 2019. doi:10.1097/SLA.0000000000003586
- Sorski L, Melamed R, Matzner P, et al. Reducing liver metastases of colon cancer in the context of extensive and minor surgeries through beta-adrenoceptors blockade and COX2 inhibition. Brain Behav Immun. 2016;58:91–98. doi:10.1016/j.bbi.2016.05.01727235931
- de Andrade LF, Lu Y, Luoma A, et al. Discovery of specialized NK cell populations infiltrating human melanoma metastases. JCI Insight. 2019;4(23). doi:10.1172/jci.insight.133103.
- Kim BJ, Caudle AS, Gottumukkala V, Aloia TA. The impact of postoperative complications on a timely return to intended oncologic therapy (RIOT). Int Anesthesiol Clin. 2016;54(4):e33–e46. doi:10.1097/AIA.000000000000011327623128
- Han WH, Oh YJ, Eom BW, Yoon HM, Kim Y-W, Ryu KW. Prognostic impact of infectious complications after curative gastric cancer surgery. Eur J Surg Oncol. 2020;46(7):1233–1238. doi:10.1016/j.ejso.2020.04.03232362466
- Cata JP, Wang H, Gottumukkala V, Reuben J, Sessler DI. Inflammatory response, immunosuppression, and cancer recurrence after perioperative blood transfusions. Br J Anaesth. 2013;110(5):690–701. doi:10.1093/bja/aet06823599512
- Della Rocca G, Vetrugno L, Coccia C, et al. Preoperative evaluation of patients undergoing lung resection surgery: defining the role of the anesthesiologist on a multidisciplinary team. J Cardiothorac Vasc Anesth. 2016;30(2):530–538. doi:10.1053/j.jvca.2015.11.01827013123
- Wall TP, Crowley PD, Sherwin A, Foley AG, Buggy DJ. Effects of lidocaine and src inhibition on metastasis in a murine model of breast cancer surgery. Cancers. 2019;11(10):1414. doi:10.3390/cancers11101414
- Freeman J, Crowley PD, Foley AG, et al. Effect of perioperative lidocaine, propofol and steroids on pulmonary metastasis in a murine model of breast cancer surgery. Cancers. 2019;11(5):613. doi:10.3390/cancers11050613
- Zhang Y, Peng X, Zheng Q. Ropivacaine inhibits the migration of esophageal cancer cells via sodium-channel-independent but prenylation-dependent inhibition of Rac1/JNK/paxillin/FAK. Biochem Biophys Res Commun. 2018;501(4):1074–1079. doi:10.1016/j.bbrc.2018.05.11029777701
- Jiang Y, Gou H, Zhu J, Tian S, Yu L. Lidocaine inhibits the invasion and migration of TRPV6-expressing cancer cells by TRPV6 downregulation. Oncol Lett. 2016;12(2):1164–1170. doi:10.3892/ol.2016.470927446413
- Baptista-Hon DT, Robertson FM, Robertson GB, et al. Potent inhibition by ropivacaine of metastatic colon cancer SW620 cell invasion and Na V 1.5 channel function. Br J Anaesth. 2014;113:i39–i48. doi:10.1093/bja/aeu10424852501
- Brisson L, Driffort V, Benoist L, et al. NaV1.5 Na(+) channels allosterically regulate the NHE-1 exchanger and promote the activity of breast cancer cell invadopodia. J Cell Sci. 2013;126(Pt 21):4835–4842. doi:10.1242/jcs.12390123902689
- Brackenbury WJ. Voltage-gated sodium channels and metastatic disease. Channels. 2014;6(5):352–361. doi:10.4161/chan.21910
- Gao J, Hu H, Wang X. Clinically relevant concentrations of lidocaine inhibit tumor angiogenesis through suppressing VEGF/VEGFR2 signaling. Cancer Chemother Pharmacol. 2019;83(6):1007–1015. doi:10.1007/s00280-019-03815-430887179
- Yang J, Li G, Bao K, Liu W, Zhang Y, Ting W. Ropivacaine inhibits tumor angiogenesis via sodium-channel-independent mitochondrial dysfunction and oxidative stress. J Bioenerg Biomembr. 2019;51(3):231–238. doi:10.1007/s10863-019-09793-930847691
- Johnson MZ, Crowley PD, Foley AG, et al. Effect of perioperative lidocaine on metastasis after sevoflurane or ketamine-xylazine anaesthesia for breast tumour resection in a murine model. Br J Anaesth. 2018;121(1):76–85. doi:10.1016/j.bja.2017.12.04329935598
- Piegeler T, Schlapfer M, Dull RO, et al. Clinically relevant concentrations of lidocaine and ropivacaine inhibit TNFalpha-induced invasion of lung adenocarcinoma cells in vitro by blocking the activation of Akt and focal adhesion kinase. Br J Anaesth. 2015;115(5):784–791. doi:10.1093/bja/aev34126475807
- Piegeler T, Votta-Velis E, Liu G, et al. Antimetastatic potential of amide-linked local anesthetics: inhibition of lung adenocarcinoma cell migration and inflammatory Src signaling independent of sodium channel blockade. Anesthesiology. 2012;117(3):548–559. doi:10.1097/ALN.0b013e318266197722846676
- Yardeni IZ, Beilin B, Mayburd E, Levinson Y, Bessler H. The effect of perioperative intravenous lidocaine on postoperative pain and immune function. Anesth Analg. 2009;109(5):1464–1469. doi:10.1213/ANE.0b013e3181bab1bd19843784
- Chen LJ, Ding YB, Ma PL, et al. The protective effect of lidocaine on lipopolysaccharide-induced acute lung injury in rats through NF-kappaB and p38 MAPK signaling pathway and excessive inflammatory responses. Eur Rev Med Pharmacol Sci. 2018;22(7):2099–2108. doi:10.26355/eurrev_201804_1474329687869
- Shin E-C, Jeon Y-T, Na H, Ryu H, Chung Y. Modulation of dendritic cell activation and subsequent Th1 cell polarization by lidocaine. PLoS One. 2015;10(10): e0139845.26445366
- Hmadcha A, Bedoya FJ, Sobrino F, Pintado E. Methylation-dependent gene silencing induced by interleukin 1beta via nitric oxide production. J Exp Med. 1999;190(11):1595–1604. doi:10.1084/jem.190.11.159510587350
- Qian X, Huang C, Cho CH, Hui WM, Rashid A, Chan AO. E-cadherin promoter hypermethylation induced by interleukin-1beta treatment or H. pylori infection in human gastric cancer cell lines. Cancer Lett. 2008;263(1):107–113. doi:10.1016/j.canlet.2007.12.02318249489
- Lirk P, Hollmann MW, Fleischer M, Weber NC, Fiegl H. Lidocaine and ropivacaine, but not bupivacaine, demethylate deoxyribonucleic acid in breast cancer cells in vitro. Br J Anaesth. 2014;113(Suppl 1):i32–38. doi:10.1093/bja/aeu20124946779
- Lirk P, Berger R, Hollmann MW, Fiegl H. Lidocaine time- and dose-dependently demethylates deoxyribonucleic acid in breast cancer cell lines in vitro. Br J Anaesth. 2012;109(2):200–207. doi:10.1093/bja/aes12822542536
- Li K, Yang J, Han X. Lidocaine sensitizes the cytotoxicity of cisplatin in breast cancer cells via up-regulation of RARbeta2 and RASSF1A demethylation. Int J Mol Sci. 2014;15(12):23519–23536. doi:10.3390/ijms15122351925526566
- Zhu J, Han S. Lidocaine inhibits cervical cancer cell proliferation and induces cell apoptosis by modulating the lncRNA-MEG3/miR-421/BTG1 pathway. Am J Transl Res. 2019;11(9):5404–5416.31632519
- Sun H, Sun Y. Lidocaine inhibits proliferation and metastasis of lung cancer cell via regulation of miR-539/EGFR axis. Artif Cells Nanomed Biotechnol. 2019;47(1):2866–2874. doi:10.1080/21691401.2019.163680731299862
- Xia W, Wang L, Yu D, Mu X, Zhou X. Lidocaine inhibits the progression of retinoblastoma in vitro and in vivo by modulating the miR520a3p/EGFR axis. Mol Med Rep. 2019;20(2):1333–1342. doi:10.3892/mmr.2019.1036331173241
- Sui H, Lou A, Li Z, Yang J. Lidocaine inhibits growth, migration and invasion of gastric carcinoma cells by up-regulation of miR-145. BMC Cancer. 2019;19(1):233. doi:10.1186/s12885-019-5431-930876463
- Yang Q, Zhang Z, Xu H, Ma C. Lidocaine alleviates cytotoxicity-resistance in lung cancer A549/DDP cells via down-regulation of miR-21. Mol Cell Biochem. 2019;456(1–2):63–72. doi:10.1007/s11010-018-3490-x30644017
- Wang Y, Xie J, Liu W, Zhang R, Huang S, Xing Y. Lidocaine sensitizes the cytotoxicity of 5-fluorouacil in melanoma cells via upregulation of microRNA-493. Pharmazie. 2017;72(11):663–669. doi:10.1691/ph.2017.761629442040
- House CD, Vaske CJ, Schwartz AM, et al. Voltage-gated Na+ channel SCN5A is a key regulator of a gene transcriptional network that controls colon cancer invasion. Cancer Res. 2010;70(17):6957–6967. doi:10.1158/0008-5472.CAN-10-116920651255
- Gong X, Dan J, Li F, Wang L. Suppression of mitochondrial respiration with local anesthetic ropivacaine targets breast cancer cells. J Thorac Dis. 2018;10(5):2804–2812. doi:10.21037/jtd.2018.05.2129997943
- Cata JP, Ramirez MF, Velasquez JF, et al. Lidocaine stimulates the function of natural killer cells in different experimental settings. Anticancer Res. 2017;37(9):4727–4732. doi:10.21873/anticanres.1187928870891
- Ramirez MF, Tran P, Cata JP. The effect of clinically therapeutic plasma concentrations of lidocaine on natural killer cell cytotoxicity. Reg Anesth Pain Med. 2015;40(1):43–48. doi:10.1097/AAP.000000000000019125469757
- Yokoyama M, Itano Y, Mizobuchi S, et al. The effects of epidural block on the distribution of lymphocyte subsets and natural-killer cell activity in patients with and without pain. Anesth Analg. 2001;92(2):463–469. doi:10.1213/00000539-200102000-0003511159252
- Wang H-L, Yan H-D, Liu -Y-Y, et al. Intraoperative intravenous lidocaine exerts a protective effect on cell-mediated immunity in patients undergoing radical hysterectomy. Mol Med Rep. 2015;12(5):7039–7044. doi:10.3892/mmr.2015.423526299324
- Schlagenhauff B, Ellwanger U, Breuninger H, Stroebel W, Rassner G, Garbe C. Prognostic impact of the type of anaesthesia used during the excision of primary cutaneous melanoma. Melanoma Res. 2000;10(2):165–169. doi:10.1097/00008390-200004000-0000910803717
- Kofler L, Breuninger H, Häfner H-M, et al. Lymph node dissection for melanoma using tumescence local anaesthesia: an observational study. Eur J Dermatol. 2018;28(2):177–185. doi:10.1684/ejd.2018.325029620000
- Zhang H, Yang L, Zhu X, et al. Association between intraoperative intravenous lidocaine infusion and survival in patients undergoing pancreatectomy for pancreatic cancer: a retrospective study. Br J Anaesth. 2020. doi:10.1016/j.bja.2020.03.034
- Pérez-González O, Cuéllar-Guzmán LF, Soliz J, Cata JP. Impact of regional anesthesia on recurrence, metastasis, and immune response in breast cancer surgery: a systematic review of the literature. Reg Anesth Pain Med. 2017;42(6):751–756. doi:10.1097/AAP.000000000000066228953508
- Pei L, Tan G, Wang L, et al. Comparison of combined general-epidural anesthesia with general anesthesia effects on survival and cancer recurrence: a meta-analysis of retrospective and prospective studies. PLoS One. 2014;9(12):e114667–e114667. doi:10.1371/journal.pone.011466725548913
- Cummings KC 3rd, Xu F, Cummings LC, Cooper GS. A comparison of epidural analgesia and traditional pain management effects on survival and cancer recurrence after colectomy: a population-based study. Anesthesiology. 2012;116(4):797–806. doi:10.1097/ALN.0b013e31824674f622273991
- Gottschalk A, Ford JG, Regelin CC, et al. Association between epidural analgesia and cancer recurrence after colorectal cancer surgery. Anesthesiology. 2010;113(1):27–34. doi:10.1097/ALN.0b013e3181de6d0d20508494
- Gupta A, Bjornsson A, Fredriksson M, Hallbook O, Eintrei C. Reduction in mortality after epidural anaesthesia and analgesia in patients undergoing rectal but not colonic cancer surgery: a retrospective analysis of data from 655 patients in central Sweden. Br J Anaesth. 2011;107(2):164–170. doi:10.1093/bja/aer10021586443
- Day A, Smith R, Jourdan I, Fawcett W, Scott M, Rockall T. Retrospective analysis of the effect of postoperative analgesia on survival in patients after laparoscopic resection of colorectal cancer. Br J Anaesth. 2012;109(2):185–190. doi:10.1093/bja/aes10622525284
- Kim SY, Kim NK, Baik SH, et al. Effects of postoperative pain management on immune function after laparoscopic resection of colorectal cancer: a randomized study. Medicine (Baltimore). 2016;95(19):e3602. doi:10.1097/MD.000000000000360227175664
- Zimmitti G, Soliz J, Aloia TA, et al. Positive impact of epidural analgesia on oncologic outcomes in patients undergoing resection of colorectal liver metastases. Ann Surg Oncol. 2016;23(3):1003–1011. doi:10.1245/s10434-015-4933-126511261
- Gao H, Meng X-Y, Wang H-Q, et al. Association between anaesthetic technique and oncological outcomes after colorectal carcinoma liver metastasis resection. Int J Med Sci. 2019;16(2):337–342. doi:10.7150/ijms.2801630745816
- Garland M, Addis D, Russell G, et al. The effect of regional anesthesia on oncologic outcomes after resection of colorectal hepatic metastases. Am Surg. 2018;84(1):29–32.29642984
- Pérez-González O, Cuéllar-Guzmán LF, Navarrete-Pacheco M, Ortiz-Martínez JJ, Williams WH, Cata JP. Impact of regional anesthesia on gastroesophageal cancer surgery outcomes: a systematic review of the literature. Anesth Analg. 2018;127(3):753–758. doi:10.1213/ANE.000000000000360229958224
- Zheng L, Hagan KB, Villarreal J, Keerty V, Chen J, Cata JP. Scalp block for glioblastoma surgery is associated with lower inflammatory scores and improved survival. Minerva Anestesiol. 2017;83(11):1137–1145. doi:10.23736/S0375-9393.17.11881-X28497933
- Cata JP, Bhavsar S, Hagan KB, et al. Scalp blocks for brain tumor craniotomies: a retrospective survival analysis of a propensity match cohort of patients. J Clin Neurosci. 2018;51:46–51. doi:10.1016/j.jocn.2018.02.02229514747
- Lai R, Peng Z, Chen D, et al. The effects of anesthetic technique on cancer recurrence in percutaneous radiofrequency ablation of small hepatocellular carcinoma. Anesth Analg. 2012;114(2):290–296. doi:10.1213/ANE.0b013e318239c2e322104077
- Merquiol F, Montelimard A-S, Nourissat A, Molliex S, Zufferey PJ. Cervical epidural anesthesia is associated with increased cancer-free survival in laryngeal and hypopharyngeal cancer surgery: a retrospective propensity-matched analysis. Reg Anesth Pain Med. 2013;38(5):398–402. doi:10.1097/AAP.0b013e31829cc3fb23881179
- Cata JP, Gottumukkala V, Thakar D, Keerty D, Gebhardt R, Liu DD. Effects of postoperative epidural analgesia on recurrence-free and overall survival in patients with nonsmall cell lung cancer. J Clin Anesth. 2014;26(1):3–17. doi:10.1016/j.jclinane.2013.06.00724095887
- Lee EK, Ahn HJ, Zo JI, Kim K, Jung DM, Park JH. Paravertebral block does not reduce cancer recurrence, but is related to higher overall survival in lung cancer surgery: a retrospective cohort study. Anesth Analg. 2017;125(4):1322–1328. doi:10.1213/ANE.000000000000234228857802
- Huang -W-W, Zhu W-Z, Mu D-L, et al. Perioperative management may improve long-term survival in patients after lung cancer surgery: a retrospective cohort study. Anesth Analg. 2018;126(5):1666–1674. doi:10.1213/ANE.000000000000288629517574
- Wu H-L, Tai Y-H, Chan M-Y, Tsou M-Y, Chen -H-H, Chang K-Y. Effects of epidural analgesia on cancer recurrence and long-term mortality in patients after non-small-cell lung cancer resection: a propensity score-matched study. BMJ Open. 2019;9(5):e027618. doi:10.1136/bmjopen-2018-027618
- Gottschalk A, Brodner G, Van Aken HK, Ellger B, Althaus S, Schulze HJ. Can regional anaesthesia for lymph-node dissection improve the prognosis in malignant melanoma? Br J Anaesth. 2012;109(2):253–259. doi:10.1093/bja/aes17622705968
- de Oliveira GS Jr., Ahmad S, Schink JC, Singh DK, Fitzgerald PC, McCarthy RJ. Intraoperative neuraxial anesthesia but not postoperative neuraxial analgesia is associated with increased relapse-free survival in ovarian cancer patients after primary cytoreductive surgery. Reg Anesth Pain Med. 2011;36(3):271–277. doi:10.1097/AAP.0b013e318217aada21519312
- Lin L, Liu C, Tan H, Ouyang H, Zhang Y, Zeng W. Anaesthetic technique may affect prognosis for ovarian serous adenocarcinoma: a retrospective analysis. Br J Anaesth. 2011;106(6):814–822. doi:10.1093/bja/aer05521436156
- Capmas P, Billard V, Gouy S, et al. Impact of epidural analgesia on survival in patients undergoing complete cytoreductive surgery for ovarian cancer. Anticancer Res. 2012;32(4):1537–1542.22493398
- Lacassie HJ, Cartagena J, Brañes J, Assel M, Echevarría GC. The relationship between neuraxial anesthesia and advanced ovarian cancer-related outcomes in the Chilean population. Anesth Analg. 2013;117(3):653–660. doi:10.1213/ANE.0b013e3182a0704623868889
- Tseng JH, Cowan RA, Afonso AM, et al. Perioperative epidural use and survival outcomes in patients undergoing primary debulking surgery for advanced ovarian cancer. Gynecol Oncol. 2018;151(2):287–293. doi:10.1016/j.ygyno.2018.08.02430185381
- Zhong S, Zhong X, Zhong X, Liu Y. Comparison between the effect of epidural anesthesia combined with epidural analgesia and general anesthesia combined with intravenous analgesia on prognosis of ovarian cancer patients. Oncol Lett. 2019;17(6):5662–5668. doi:10.3892/ol.2019.1021631186789
- Elias KM, Kang S, Liu X, Horowitz NS, Berkowitz RS, Frendl G. Anesthetic selection and disease-free survival following optimal primary cytoreductive surgery for stage III epithelial ovarian cancer. Ann Surg Oncol. 2015;22(4):1341–1348.25287437
- Grandhi RK, Lee S, Abd-Elsayed A. The Relationship Between Regional Anesthesia and Cancer: a Metaanalysis. Ochsner J. 2017;17(4):345–361.29230120
- Lee BM, Singh Ghotra V, Karam JA, Hernandez M, Pratt G, Cata JP. Regional anesthesia/analgesia and the risk of cancer recurrence and mortality after prostatectomy: a meta-analysis. Pain Manag. 2015;5:387–395.26250850
- Chipollini J, Alford B, Boulware DC, et al. Epidural anesthesia and cancer outcomes in bladder cancer patients: is it the technique or the medication? A matched-cohort analysis from a tertiary referral center. BMC Anesthesiol. 2018;18(1):157. doi:10.1186/s12871-018-0622-530390636
- Cakmakkaya OS, Kolodzie K, Apfel CC, Pace NL. Anaesthetic techniques for risk of malignant tumour recurrence. Cochrane Database Syst Rev. 2014;11:CD008877.
- Ma D, Pei L, Tan G, et al. Comparison of combined general-epidural anesthesia with general anesthesia effects on survival and cancer recurrence: a meta-analysis of retrospective and prospective studies. PLoS One. 2014;9(12): e114667.25548913
- Deegan CA, Murray D, Doran P, Ecimovic P, Moriarty DC, Buggy DJ. Effect of anaesthetic technique on oestrogen receptor-negative breast cancer cell function in vitro. Br J Anaesth. 2009;103(5):685–690. doi:10.1093/bja/aep26119776028
- Deegan CA, Murray D, Doran P, et al. Anesthetic technique and the cytokine and matrix metalloproteinase response to primary breast cancer surgery. Reg Anesth Pain Med. 2010;35(6):490–495. doi:10.1097/AAP.0b013e3181ef4d0520975461
- O’Riain SC, Buggy DJ, Kerin MJ, Watson RW, Moriarty DC. Inhibition of the stress response to breast cancer surgery by regional anesthesia and analgesia does not affect vascular endothelial growth factor and prostaglandin E2. Anesth Analg. 2005;100(1):244–249. doi:10.1213/01.ANE.0000143336.37946.7D15616085
- Velasquez JF, Ramirez MF, Ai DI, Lewis V, Cata JP. Impaired immune function in patients undergoing surgery for bone cancer. Anticancer Res. 2015;35(10):5461–5466.26408709
- Buckley A, McQuaid S, Johnson P, Buggy DJ. Effect of anaesthetic technique on the natural killer cell anti-tumour activity of serum from women undergoing breast cancer surgery: a pilot study. Br J Anaesth. 2014;113(Suppl 1):i56–62. doi:10.1093/bja/aeu20025009196
- Desmond F, McCormack J, Mulligan N, Stokes M, Buggy DJ. Effect of anaesthetic technique on immune cell infiltration in breast cancer: a follow-up pilot analysis of a prospective, randomised, investigator-masked study. Anticancer Res. 2015;35(3):1311–1319.25750280
- Zhang W, Shao X. Isoflurane promotes non-small cell lung cancer malignancy by activating the Akt-mammalian target of rapamycin (mTOR) signaling pathway. Med Sci Monit. 2016;22:4644–4650. doi:10.12659/MSM.89843427897153
- Iwasaki M, Zhao H, Jaffer T, et al. Volatile anaesthetics enhance the metastasis related cellular signalling including CXCR2 of ovarian cancer cells. Oncotarget. 2016;7(18):26042–26056. doi:10.18632/oncotarget.830427028996
- Luo X, Zhao H, Hennah L, et al. Impact of isoflurane on malignant capability of ovarian cancer in vitro ‡. Br J Anaesth. 2015;114(5):831–839. doi:10.1093/bja/aeu40825501719
- Ciechanowicz S, Zhao H, Chen Q, et al. Differential effects of sevoflurane on the metastatic potential and chemosensitivity of non-small-cell lung adenocarcinoma and renal cell carcinoma in vitro. Br J Anaesth. 2018;120(2):368–375. doi:10.1016/j.bja.2017.11.06629406185
- Moudgil GC, Singal DP. Halothane and isoflurane enhance melanoma tumour metastasis in mice. Can J Anaesth. 1997;44(1):90–94. doi:10.1007/BF030143318988831
- Liang H, Yang CX, Zhang B, Zhao ZL, Zhong JY, Wen XJ. Sevoflurane attenuates platelets activation of patients undergoing lung cancer surgery and suppresses platelets-induced invasion of lung cancer cells. J Clin Anesth. 2016;35:304–312. doi:10.1016/j.jclinane.2016.08.00827871548
- Xu YJ, Li SY, Cheng Q, et al. Effects of anaesthesia on proliferation, invasion and apoptosis of LoVo colon cancer cells in vitro. Anaesthesia. 2016;71(2):147–154. doi:10.1111/anae.1333126669824
- Jaura AI, Flood G, Gallagher HC, Buggy DJ. Differential effects of serum from patients administered distinct anaesthetic techniques on apoptosis in breast cancer cells in vitro: a pilot study. Br J Anaesth. 2014;113(Suppl 1):i63–67. doi:10.1093/bja/aet58125009197
- Melamed R, Bar-Yosef S, Shakhar G, Shakhar K, Ben-Eliyahu S. Suppression of natural killer cell activity and promotion of tumor metastasis by ketamine, thiopental, and halothane, but not by propofol: mediating mechanisms and prophylactic measures. Anesth Analg. 2003;97(5):1331–1339. doi:10.1213/01.ANE.0000082995.44040.0714570648
- Tazawa K, Koutsogiannaki S, Chamberlain M, Yuki K. The effect of different anesthetics on tumor cytotoxicity by natural killer cells. Toxicol Lett. 2017;266:23–31. doi:10.1016/j.toxlet.2016.12.00727940100
- Meier A, Gross ETE, Schilling JM, et al. Isoflurane impacts murine melanoma growth in a sex-specific, immune-dependent manner. Anesth Analg. 2018;126(6):1910–1913. doi:10.1213/ANE.000000000000290229570154
- Gao K, Su Z, Liu H, Liu Y. Anti-proliferation and anti-metastatic effects of sevoflurane on human osteosarcoma U2OS and Saos-2 cells. Exp Mol Pathol. 2019;108:121–130. doi:10.1016/j.yexmp.2019.04.00530974101
- Gao C, Shen J, Meng Z-X, He X-F. Sevoflurane inhibits glioma cells proliferation and metastasis through miRNA-124-3p/ROCK1 axis. Pathol Oncol Res. 2019.
- Fan L, Wu Y, Wang J, He J, Han X. Sevoflurane inhibits the migration and invasion of colorectal cancer cells through regulating ERK/MMP-9 pathway by up-regulating miR-203. Eur J Pharmacol. 2019;850:43–52. doi:10.1016/j.ejphar.2019.01.02530685432
- Liang H, Yang CX, Zhang B, et al. Sevoflurane suppresses hypoxia-induced growth and metastasis of lung cancer cells via inhibiting hypoxia-inducible factor-1alpha. J Anesth. 2015;29(6):821–830. doi:10.1007/s00540-015-2035-726002230
- Gallyas F, Sumi C, Matsuo Y, et al. Cancerous phenotypes associated with hypoxia-inducible factors are not influenced by the volatile anesthetic isoflurane in renal cell carcinoma. PLoS One. 2019;14(4): e0215072.30986231
- Zhang YF, Li CS, Zhou Y, Lu XH. Effects of propofol on colon cancer metastasis through STAT3/HOTAIR axis by activating WIF-1 and suppressing Wnt pathway. Cancer Med. 2020 ;9(5):1842–1854.31953926
- Qi J, Wu Q, Zhu X, et al. Propofol attenuates the adhesion of tumor and endothelial cells through inhibiting glycolysis in human umbilical vein endothelial cells. Acta Biochim Biophys Sin (Shanghai). 2019. doi:10.1093/abbs/gmz105
- Guo XG, Wang S, Xu YB, Zhuang J. Propofol suppresses invasion, angiogenesis and survival of EC-1 cells in vitro by regulation of S100A4 expression. Eur Rev Med Pharmacol Sci. 2015;19(24):4858–4865.26744878
- Xu YB, Du QH, Zhang MY, Yun P, He CY. Propofol suppresses proliferation, invasion and angiogenesis by down-regulating ERK-VEGF/MMP-9 signaling in Eca-109 esophageal squamous cell carcinoma cells. Eur Rev Med Pharmacol Sci. 2013;17(18):2486–2494.24089228
- Sen Y, Xiyang H, Yu H. Effect of thoracic paraspinal block-propofol intravenous general anesthesia on VEGF and TGF-β in patients receiving radical resection of lung cancer. Medicine. 2019;98(47):e18088. doi:10.1097/MD.000000000001808831764844
- Ferrell JK, Cattano D, Brown RE, Patel CB, Karni RJ. The effects of anesthesia on the morphoproteomic expression of head and neck squamous cell carcinoma: a pilot study. Transl Res. 2015;166(6):674–682. doi:10.1016/j.trsl.2015.09.00126423449
- Liu D, Sun X, Du Y, Kong M. Propofol promotes activity and tumor-killing ability of natural killer cells in peripheral blood of patients with colon cancer. Med Sci Monit. 2018;24:6119–6128. doi:10.12659/MSM.91121830174326
- Zhou M, Dai J, Zhou Y, et al. Propofol improves the function of natural killer cells from the peripheral blood of patients with esophageal squamous cell carcinoma. Exp Ther Med. 2018;16(1):83–92.29977357
- Inada T, Kubo K, Shingu K. Promotion of interferon-gamma production by natural killer cells via suppression of murine peritoneal macrophage prostaglandin E(2) production using intravenous anesthetic propofol. Int Immunopharmacol. 2010;10(10):1200–1208. doi:10.1016/j.intimp.2010.06.02720633531
- Zhang T, Fan Y, Liu K, Wang Y. Effects of different general anaesthetic techniques on immune responses in patients undergoing surgery for tongue cancer. Anaesth Intensive Care. 2019;42(2):220–227. doi:10.1177/0310057X1404200209
- Liu S, Gu X, Zhu L, et al. Effects of propofol and sevoflurane on perioperative immune response in patients undergoing laparoscopic radical hysterectomy for cervical cancer. Medicine. 2016;95(49):e5479. doi:10.1097/MD.000000000000547927930529
- Oh C-S, Lee J, Yoon T-G, et al. Effect of equipotent doses of propofol versus sevoflurane anesthesia on regulatory T cells after breast cancer surgery. Anesthesiology. 2018;129(5):921–931. doi:10.1097/ALN.000000000000238230074934
- Yan T, Zhang GH, Wang BN, Sun L, Zheng H. Effects of propofol/remifentanil-based total intravenous anesthesia versus sevoflurane-based inhalational anesthesia on the release of VEGF-C and TGF-beta and prognosis after breast cancer surgery: a prospective, randomized and controlled study. BMC Anesthesiol. 2018;18(1):131. doi:10.1186/s12871-018-0588-330243294
- Soliz JM, Ifeanyi IC, Katz MH, et al. Comparing postoperative complications and inflammatory markers using total intravenous anesthesia versus volatile gas anesthesia for pancreatic cancer surgery. Anesthesiol Pain Med. 2017;7(4):e13879. doi:10.5812/aapm.13879
- Owusu-Agyemang P, Cata JP, Fournier KF, et al. Evaluating the impact of total intravenous anesthesia on the clinical outcomes and perioperative NLR and PLR profiles of patients undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol. 2016;23(8):2419–2429. doi:10.1245/s10434-016-5176-526975738
- Cata JP, Nguyen LT, Ifeanyi-Pillette IC, et al. An assessment of the survival impact of multimodal anesthesia/analgesia technique in adults undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy: a propensity score matched analysis. Int J Hyperthermia. 2019;36(1):369–375. doi:10.1080/02656736.2019.157498530829082
- Lee JH, Kang SH, Kim Y, Kim HA, Kim BS. Effects of propofol-based total intravenous anesthesia on recurrence and overall survival in patients after modified radical mastectomy: a retrospective study. Korean J Anesthesiol. 2016;69(2):126–132. doi:10.4097/kjae.2016.69.2.12627066202
- Yoo S, Lee H-B, Han W, et al. Total intravenous anesthesia versus inhalation anesthesia for breast cancer surgery: a retrospective cohort study. Anesthesiology. 2019;130(1):31–40. doi:10.1097/ALN.000000000000249130376457
- Lai H-C, Lee M-S, Lin K-T, et al. Propofol-based total intravenous anesthesia is associated with better survival than desflurane anesthesia in intrahepatic cholangiocarcinoma surgery. Medicine (Baltimore). 2019;98(51):e18472. doi:10.1097/MD.000000000001847231861027
- Wu Z-F, Lee M-S, Wong C-S, et al. Propofol-based total intravenous anesthesia is associated with better survival than desflurane anesthesia in colon cancer surgery. Anesthesiology. 2018;129(5):932–941. doi:10.1097/ALN.000000000000235730028726
- Jun I-J, Jo J-Y, Kim J-I, et al. Impact of anesthetic agents on overall and recurrence-free survival in patients undergoing esophageal cancer surgery: a retrospective observational study. Sci Rep. 2017;7(1):14020. doi:10.1038/s41598-017-14147-929070852
- Zheng X, Wang Y, Dong L, et al. Effects of propofol-based total intravenous anesthesia on gastric cancer: a retrospective study. Onco Targets Ther. 2018;11:1141–1148. doi:10.2147/OTT.S15679229535538
- Oh TK, Kim -H-H, Jeon Y-T. Retrospective analysis of 1-year mortality after gastric cancer surgery: total intravenous anesthesia versus volatile anesthesia. Acta Anaesthesiol Scand. 2019;63(9):1169–1177. doi:10.1111/aas.1341431180151
- Cata JP, Hagan KB, Bhavsar SD, et al. The use of isoflurane and desflurane as inhalational agents for glioblastoma surgery. A survival analysis. J Clin Neurosci. 2017;35:82–87. doi:10.1016/j.jocn.2016.10.00627765559
- Lai H-C, Lee M-S, Lin C, et al. Propofol-based total intravenous anaesthesia is associated with better survival than desflurane anaesthesia in hepatectomy for hepatocellular carcinoma: a retrospective cohort study. Br J Anaesth. 2019;123(2):151–160. doi:10.1016/j.bja.2019.04.05731171343
- Oh TK, Kim K, Jheon S, et al. Long-term oncologic outcomes for patients undergoing volatile versus intravenous anesthesia for non-small cell lung cancer surgery: a retrospective propensity matching analysis. Cancer Control. 2018;25(1):1073274818775360. doi:10.1177/107327481877536029739245
- Xu Q, Shi N-J, Zhang H, Zhu Y-M. Effects of combined general-epidural anesthesia and total intravenous anesthesia on cellular immunity and prognosis in patients with non‑small cell lung cancer: A comparative study. Mol Med Rep. 2017;16(4):4445–4454. doi:10.3892/mmr.2017.714428765974
- Yap A, Lopez-Olivo MA, Dubowitz J, Hiller J, Riedel B. Anesthetic technique and cancer outcomes: a meta-analysis of total intravenous versus volatile anesthesia. Can J Anaesth. 2019;66(5):546–561. doi:10.1007/s12630-019-01330-x30834506
- Hong B, Lee S, Kim Y, et al. Anesthetics and long-term survival after cancer surgery-total intravenous versus volatile anesthesia: a retrospective study. BMC Anesthesiol. 2019;19(1):233. doi:10.1186/s12871-019-0914-431852445
- Jin Z, Li R, Liu J, Lin J. Long-term prognosis after cancer surgery with inhalational anesthesia and total intravenous anesthesia: a systematic review and meta-analysis. Int J Physiol Pathophysiol Pharmacol. 2019;11(3):83–94.31333811
- Lim A, Braat S, Hiller J, Riedel B. Inhalational versus propofol-based total intravenous anaesthesia: practice patterns and perspectives among Australasian anaesthetists. Anaesth Intensive Care. 2018;46(5):480–487. doi:10.1177/0310057X180460050930189822