Abstract
Background
The distal saphenous nerve is commonly known to provide cutaneous innervation of the medial side of the ankle and distally to the base of the great toe. We hypothesize that the saphenous nerve innervates the periosteum of the medial malleolus and joint capsule.
Methods
Five fresh limbs were dissected and the saphenous nerve was traced distally with magnification. The medial malleolus, talus, and soft tissue were fixed in formaldehyde, decalcified, and embedded in paraffin and sectioned. Histologic slides were then prepared using S100 antibody nerve stains.
Results
Histologic slides were examined and myelinated nerves could be observed within the medial capsule and periosteum in all the specimens.
Conclusion
We have demonstrated that the saphenous nerve innervates the periosteum of the medial malleolus and joint capsule.
Keywords:
Introduction
The saphenous nerve is commonly known to contribute to the sensory innervation of the lower extremity. The medical and anatomic literature describes the saphenous nerve as providing sensory innervation of the medial leg and calf, terminating distally at the “ball” of the great toe.Citation1–Citation5 The importance of this nerve providing sensory supply to the medial ankle area appears to be underappreciated. One anatomic studyCitation6 of the nerve supply to the ankle joint concluded that the saphenous nerve along with the tibial, superficial, deep peroneal, and sural nerves provide the articular branches.
The saphenous nerve is classically described in most anatomic texts as the longest branch of the femoral nerve. It arises from the femoral nerve in the femoral triangle and descends laterally to the femoral vessels to enter the adductor canal. The nerve then crosses the femoral vessels to lie on their medial side at the distal portion of the adductor magnus muscle. It then pierces the sartorial fascia between the sartorius and gracilis tendons just above the medial aspect of the knee and becomes subcutaneous thereafter, giving rise to the infrapatellar branch supplying the skin over the anterior inferior knee, and may form communication with the anterior cutaneous branches of the femoral nerve. Below the infrapatellar branch, the saphenous nerve provides the medial crural nerves that supply cutaneous innervation to the anterior and medial leg. Below the knee, the saphenous nerve follows the course of the greater saphenous vein to the medial side of the ankle and foot, and is said to terminate as far as the medial aspect of the first metatarsal head. It is understood that there is often variability in the terminal cutaneous branches. Mercer et alCitation7 and KosinskiCitation8 found in 19 and 96 specimens, respectively and combined, only one instance of the nerve extending to the medial first metatarsophalangeal joint.
Although cursory descriptions of the saphenous nerve anatomy as it approaches the ankle have been described,Citation7–Citation9 the importance of its distribution at the ankle appears to be lacking regarding possible sensory innervation of the ankle joint. Approximately 3 cm proximal to the tip of the medial malleolus, the nerve is said to divide into anterior and posterior branches in relation to the saphenous vein.Citation7 These branches are then described to terminate in the integument over the medial malleolus, while the saphenous vein continues into the foot.
In our clinical experience with regional anesthesia, popliteal block alone does not provide adequate coverage for surgery or postoperative pain management following major ankle surgeries, including arthrodesis, arthroplasty, and fractures. When the addition of a saphenous nerve block is performed following foot and ankle surgery, we have found the pain relief to be excellent (American Orthopaedic Foot & Ankle Society, unpublished data, 2009).
The purpose of this study was to correlate our clinical experience with anatomic and histologic evidence of the bone and medial ankle joint capsule innervation by the saphenous nerve.
Materials and methods
This study was reviewed and approved by the institutional review board at the Mayo Clinic. Five fresh limbs, devoid of pathology in the foot or ankle, were obtained after surgical amputation through the proximal tibia or knee to perform dissections of the saphenous nerve supply to the foot. The nerve was traced distally with the aid of a dissecting microscope or loupe magnification, and particular attention was paid to the nerve divisions at and just below the medial malleolus. Demonstration of the nerve fibers from the saphenous nerve in the ankle capsule was carried out by resecting a block of the medial malleolus and talus with the medial ankle mortise and its soft tissue. The specimen was fixed in formalin, decalcified (Fisher Scientific, Hampton, NH), and embedded in paraffin to allow serial sections. Histologic slides were then prepared using S100 antibody nerve stains (Dako North America, Carpinteria, CA). S100 protein is a highly sensitive marker for myelinated nerves in the peripheral nervous system. S100 monoclonal antibody is directed against a calcium-binding protein present in the nucleus and cytoplasm of Schwann cells.Citation10
Results
Findings of dissection and histology
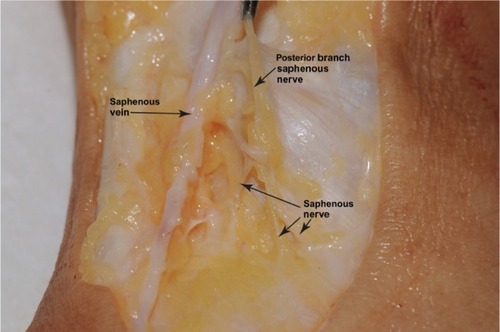
At the mid level of the tibia, the saphenous nerve was observed to divide into two or more branches that gave rise to additional nerves supplying the skin and subcutaneous tissues. Near the medial supramalleolar region, we found a consistent division of the nerve into branches that were anterior and posterior to the greater saphenous vein. The posterior branch terminated into several fine nerves just below the medial malleolus that macroscopically attached to the ankle capsule and deltoid ligament (). The anterior branch appeared to course over the medial anterior ankle and terminated in the subcutaneous tissues. In none of the specimens was there an identifiable nerve following the vein into the medial foot.
Figure 1 Gross dissection of medial ankle.
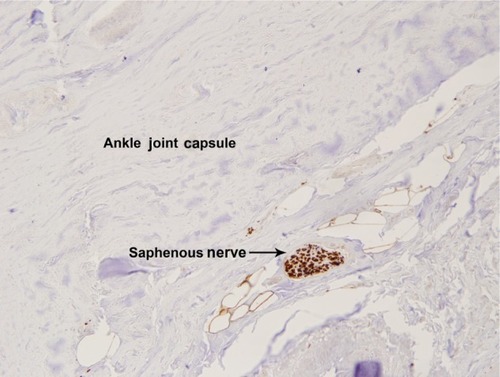
Photographs of the sectioned block () and photomicrographs of the slides were examined for orientation. In the histologic slides, we could identify fine branches of the saphenous nerve within the medial capsule and periosteum in all the specimens ( and ).
Figure 2 Paraffn-embedded specimen of medial ankle.
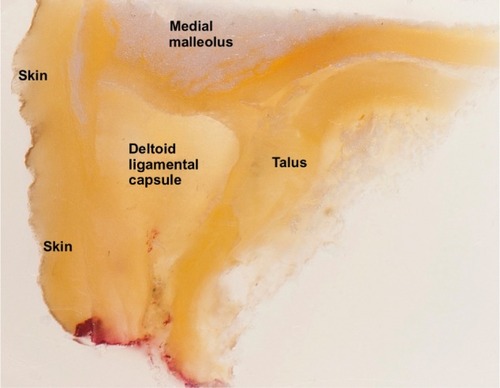
Figure 3 Photograph of histologic slide of saphenous nerve in the joint capsule.
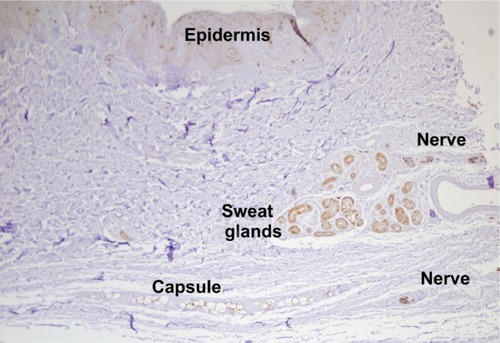
Figure 4 Photograph of histologic slide of saphenous nerve in the periosteum, 40×.
Discussion
We have verified histologically that the saphenous nerve innervates the periosteum of the medial malleolus and joint capsule. Gross anatomic studies by Sarrafian confirmed variations of the saphenous nerve to the periosteum of the distal tibia, medial malleolus, and joint capsule.Citation11 Our results correlate with the findings of Blumenthal et al of improved dynamic pain scores with addition of a continuous femoral catheter to a continuous popliteal sciatic catheter following major ankle surgery.Citation12 The importance of the saphenous nerve innervating the medial ankle is overlooked in the anesthesia literature. We recognize that patients frequently have significant medial pain following ankle joint surgery. Our current practice for analgesia following these ankle procedures is to place both a popliteal and saphenous nerve catheter. We place our saphenous blocks distally to the adductor canal in an effort to avoid the motor branch to the vastus medialis, as described by Kapoor et al.Citation13
In conclusion, the distal saphenous nerve is a cutaneous branch to the medial ankle and forefoot, and also innervates the periosteum of the medial malleolus and medial joint capsule. Block of the saphenous nerve, in addition to the sciatic nerve, is essential for complete anesthesia and analgesia of the hind foot and ankle.
Acknowledgments
The authors would like to acknowledge Pamela A Kreinest for slide preparation. Financial support was provided by the Mayo Clinic, Jacksonville, FL.
Disclosure
The authors report no conflicts of interest in this work.
References
- HadzicATextbook of Regional Anesthesia and Acute Pain ManagementNew York, NYMcGraw-Hill Professional2006
- CraigEJClinchotDMFemoral neuropathyFronteraWRSilverJKRizzoTDEssentials of Physical Medicine and Rehabilitation2nd edPhiladelphia, PASaunders Elsevier2008
- WedelDJHorlockerTTNerve blocksMillerRDMiller’s Anesthesia7th edPhiladelphia, PAChurchill Livingstone Elsevier2010
- CanaleSTBeatyJHCampbell’s Operative OrthopaedicsPhiladelphia, PAMosby Elsevier2008
- MarxJHockbergerRWallsRRosen’s Emergency Medicine – Concepts and Clinical PracticePhiladelphia, PAMosby Elsevier2010
- MentzelMFleischmannWBauerGKinzlLAnkle joint denervation. Part 1. Anatomy: the sensory innervation of the ankle jointFoot Ankle Surg199951520
- MercerDMorrellNTFitzpatrickJThe course of the distal saphenous nerve: a cadaveric investigation and clinical implicationsIowa Orthop J20113123123522096447
- KosinskiCThe course, mutual relations and distribution of the cutaneous nerves of the metazonal region of leg and footJ Anat19266027429717104102
- HuelkeDFThe origin of the peroneal communicating nerve in adult manAnat Rec1958132819213627490
- Gonzalez-MartinezTPerez-PineraPDiaz-EsnalBVegaJAS-100 proteins in the human peripheral nervous systemMicrosc Res Tech20036063363812645010
- SarrafianSKKelikianASSarrafian’s anatomy of the foot and ankleKelikianASSarrafian’s Anatomy of the Foot and Ankle3rd edPhiladelphia, PALippincott Williams & Wilkins2011
- BlumenthalSBorgeatANeudorferCBertoliniREspinosaNAguirreJAdditional femoral catheter in combination with popliteal catheter for analgesia after major ankle surgeryBr J Anaesth201110638739321169609
- KapoorRAdhikarySDSiefringCMcQuillanPMThe saphenous nerve and its relationship to the nerve to the vastus medialis in and around the adductor canal: an anatomical studyActa Anaesthesiol Scand20125636536722335278