
Abstract
Achalasia refers to the lack of smooth muscle relaxation of the distal esophagus. Although nonsurgical treatments such as pneumatic dilatation of the distal esophagus and botulinum toxin injections have been performed, these procedures have limited duration. Similarly, surgical treatment with Heller myotomy is associated with complications. At our institution, we perform the peroral endoscopic myotomy (POEM) in qualified patients. Briefly, POEM involves endoscopic creation of a mid-esophageal submucosal bleb, creation of a submucosal tunnel with the endoscope, and then a distal myotomy, resulting in relaxation of the distal esophagus. The aim of our study is to document perioperative pain and associated pain management for our initial patients undergoing POEM and to review the literature for perioperative complications of this procedure. Therefore, anesthetic and pain management for our initial eleven patients undergoing POEM were reviewed. Patient demographics, pre-POEM pain medication history, perioperative pain medication requirements, and post-POEM pain scores were examined. We found post-POEM pain was usually in the mild–moderate range; a combination of medications was effective (opioids, nonsteroidal anti-inflammatory drugs, acetaminophen). Our literature search revealed a wide frequency range of complications such as pneumoperitoneum and subcutaneous emphysema, with rare serious events such as capnopericardium leading to cardiac arrest. In conclusion, our experience with POEM suggests pain and can be managed adequately with a combination of medications; the procedure appears to be safe and reasonable to perform in an outpatient endoscopy unit.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Patients who suffer from dysphagia, dysfunctional relaxation of the lower esophageal sphincter (LES), and lack of peristalsis of the esophageal body may fit the criteria for achalasia.Citation1 Regurgitation with dysphagia to solids and liquids is also suggestive of this condition, which historically has been treated with pneumatic dilatation of the distal esophagus or surgical myotomy. Botulinum toxin injections became popular owing to its ease, safety, and fairly high initial efficacy, although botulinum toxin injections are less used today due to lack of durability. Surgical treatment consists of the open or laparoscopic Heller myotomy, which is associated with surgical and anesthetic risk and postoperative reflux.
A new minimally invasive, endoscopic procedure to treat achalasia is the peroral endoscopic myotomy (POEM) procedure, of which the first clinical series were reported in 2010.Citation2 A growing body of literature supports POEM as a therapy for achalasia that is both safe and effective, particularly when considering the limitations of the other available surgical and nonsurgical options.Citation3–Citation6 However, large randomized clinical trials are ongoing in an effort to demonstrate long-term (> 1 year) benefit of POEM versus surgery and pneumatic dilation.
The POEM procedure has been extensively described elsewhere.Citation7,Citation8 Briefly, after induction of general endotracheal anesthesia and administration of intravenous antibiotics, the endoscopist identifies the LES and creates a submucosal bleb in the mid esophagus with dyed fluid injection (to identify the demarcation between the muscle layers). The endoscope is inserted into the submucosal space through a longitudinal incision created by an electrocautery knife, and a long tunnel in the submucosal space is created past the LES into the proximal stomach, exposing the inner circular muscle throughout (). Next, the myotomy is carried out from a point several centimeters distal to the mucosal entry point, with a typical length of 8–10 cm above gastroesophageal junction and 2–3 cm into the cardia of the stomach. The circular muscle bundle fibers are targeted and cut, thereby relaxing the distal esophagus.
Figure 1 Endoscope inserted and used to create submucosal tunnel.
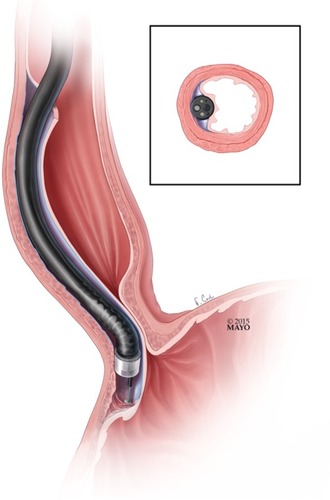
Carbon dioxide (CO2) insufflation is used during the procedure to minimize gas-related complications; however, a number of adverse events have been reported during and after POEM including pneumo/capnothorax, pneumo/capnoperitoneum, tension capnopericardium with cardiac arrest, and subcutaneous emphysema resulting in delayed extubation. Little has been written about perioperative pain management in these patients, who are typically observed overnight in hospital and then dismissed home on clear liquid diet after an esophagram excludes an esophageal leak.
A very limited body of research touches on anesthetic management of the POEM procedure,Citation9,Citation10 including complications of importance to the perioperative clinician and pain management of patients undergoing POEM. Therefore, the twofold purpose of this manuscript is to report on our initial experience with perioperative pain management in this patient population and to provide a narrative review of POEM complications of interest to anesthesiologists and other perioperative clinicians.
Methods
This retrospective study was approved by the Mayo Clinic Institutional Review Board, who deemed written informed consent was not required due to the retrospective nature. We reviewed our anesthetic and pain management experience with the initial eleven patients treated with POEM at our medical center. The medical record was reviewed for patient demographics, pre-POEM pain medication use, intraoperative and postoperative pain medication administration, and post-POEM pain scores. The medical record was also reviewed for any periprocedural complications. Although specific intraoperative anesthetic parameters have been described previously,Citation10 peak airway pressure and highest end-tidal carbon dioxide (ETCO2) are of interest to anesthesiologists; as such, we also gathered this information from our anesthetic record.
To guide a narrative review of complications of interest to anesthesiologists and other perioperative clinicians, we performed a search of the medical literature for reported complications of the POEM procedure (search terms: peroral, myotomy, anesthesia, complications, and adverse events) using Ovid MEDLINE® In-Process & Other Non-Indexed Citations, Ovid MEDLINE®, Embase, EBM Reviews – Cochrane Central Register of Controlled Trials, and EBM Reviews – Cochrane Database of Systematic Reviews for English language articles on POEM for the past 5 years.
Results
Demographic and intraoperative variables are summarized in . All of the patients except one were dismissed from the hospital the next day, and one was dismissed on day 2. This patient had complained of chest pain when he arrived on the hospital floor from postanesthesia care unit, and was transferred to intensive care unit (ICU). There was no evidence of myocardial ischemia and it was concluded that he was experiencing only postprocedure pain. There were no reported procedural or anesthetic complications in these initial eleven patients treated with POEM at our institution. None of the patients required decompression of pneumo/capnoperitoneum, and intraoperative ventilation was not problematic, including management of ETCO2 and peak airway pressures.
Table 1 Demographics and intraoperative variables of patients undergoing POEM for achalasia
Pain scores and medication use are summarized in . On average, pain scores were in the mild–moderate range (3.3 on a 0–10 numeric rating scale), although at least one patient experienced pain in the severe range (eg, 7/10 intensity). Pain scores over the hospital course are shown in , demonstrating a decline in pain severity that was in the mild–moderate range throughout in most patients. Substernal chest discomfort was the most common pain complaint; as noted earlier – one patient complained of post-POEM chest pain and was admitted to ICU for observation. During their hospital course, some patients required several classes of pain medications, including opioids, acetaminophen, and nonsteroidal anti-inflammatory drugs (ketorolac). None of the patients were taking opioids before their procedure.
Figure 2 Pain scores over the hospital course of treatment.
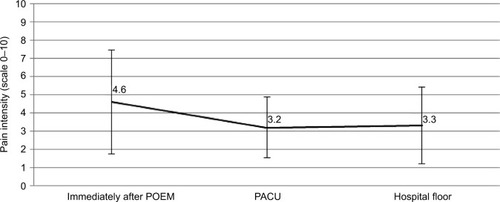
Table 2 Pain scores and pain medication use during and after POEM procedures
Using the aforementioned search criteria, our literature search initially identified 115 publications on POEM, anesthesia, and complications, or adverse events (). However, after deleting duplicates, abstracts, and papers either not associated with POEM or not associated with complications of POEM, 35 manuscripts were included in our review.Citation6,Citation9–Citation42 The common or serious perioperative adverse events, judged to be of interest to anesthesiologists and other perioperative clinicians, are summarized in . To put these complications in perspective in terms of severity and frequency, we also used as reference two recent POEM position papers from the gastrointestinal literature.Citation43,Citation44
Figure 3 Flow chart of study selection process.
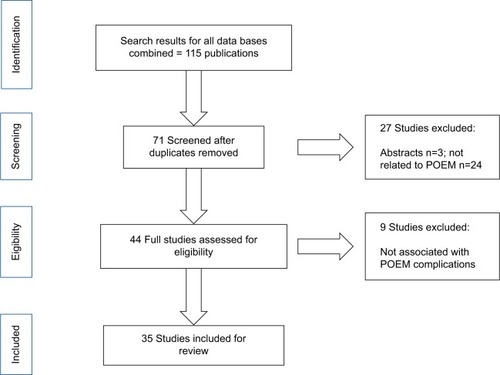
Table 3 Complications and events associated with POEM
Discussion
On the basis of our initial experience and review of the literature, the POEM procedure is a safe and effective minimally invasive technique to treat achalasia. Although the number of patients we have treated is small, no large-scale studies have been published on pain or anesthesia outcomes related to this procedure. We are the first to publish detailed perioperative pain management data. Although Li et alCitation36 noted 24 out of 234 patients (~10%) suffered “severe” pain post-POEM, our results suggest that the procedure does not require large amounts or prolonged treatment with opioids. Chest pain rarely persists for months after the procedure, although this may be due to residual symptoms from chronic achalasia and not postprocedural per se. A multimodal approach to pain management, including a combination of acetaminophen, nonsteroidal anti-inflammatory drugs, and intermediate acting opioids, appears to be adequate in this patient population.
In terms of complications, a wide range of frequencies has been reported. summarizes reported POEM complications judged to be of interest to perioperative clinicians; fortunately, serious and lasting adverse events appear to be rare in experienced centers. Not all of the papers we identified defined how they identified adverse events. In some of the studies, complications were identified only during the procedure (not postoperatively). Various imaging modalities were used to identify outcomes such as pleural effusion (eg, computed tomography [CT] scan versus chest X-ray). Finally, some of the centers were reporting their initial experience with POEM, and may be expected to have a higher rate of adverse events compared to more experienced care providers. Position papers from a national endoscopy society helped to give perspective to these adverse events in terms of risk, frequency, and severity.Citation43,Citation44
Some comorbidities of interest to perioperative clinicians have been deemed contraindications to POEM.Citation44 These include severe pulmonary disease (eg, extensive bullous disease), coagulopathy, or prior endoscopic mucosal resection of the esophagus. Anesthesia professionals should be prepared for the risk of aspiration in this patient population; rapid sequence induction of anesthesia is typically carried out with endotracheal intubation.
Because of the use of CO2 insufflation within the esophageal wall, which is thinly separated from or directly exposed to surrounding structures during the procedure, perioperative clinicians must be vigilant for pneumo/capnothorax, pneumo/capnoperitoneum, and subcutaneous emphysema. Ren et alCitation13 reported a 25% incidence of pneumothorax, although CT scanning was used for diagnosis and not associated with any adverse events except the need for chest tube placement in some patients. In contrast, Kurian et alCitation34 reported only one in 40 patients suffered a capnothorax, which was treated with needle decompression. Significant hemodynamic changes would indicate the need for chest tube placement, especially if there is evidence of tension pneumothorax.
Because of the proximity of the esophagus to the mediastinum and lungs, it is not surprising that pneumo/capnomediastinum, pleural effusion, pneumo/capnothorax, and capnopericardium have been reported. In the case of capnopericardium, a cardiac arrest occurred, but fortunately resulted in a good outcome for the patient.Citation9 Vigilance to changes in airway pressures and hemodynamic perturbations are necessary to ensure early intervention, which requires action on part of both the endoscopy and anesthesia teams. The use of insufflation and CO2 flow should be minimized by the endoscopist, especially when the endoscope is within the submucosal tunnel.
The literature and our experience suggests that in most patients, increasing minute ventilation is all that is required to manage the increase in ETCO2 associated with CO2 insufflation. Subcutaneous emphysema may be slow to resolve in patients with cardiopulmonary disease, requiring intubation for a few hours postprocedure. Exposure of the abdomen during the procedure and careful observation of airway pressures should provide early warning of pneumo/capnoperitoneum, which can be decompressed with a Veress needle (Genicon, Winter Park, FL, USA). Postoperative bleeding is always a concern but apparently is infrequent, with a (highest) reported rate we could find of 7%.Citation23 Long-term adverse events are gastroesophageal reflux disease (in 20%–46% of patients after POEM)Citation45 and incomplete myotomy.
Despite potential adverse events, a body of literature suggests that in high-volume practices with significant experience in POEM, the procedure can be carried out safely in an endoscopy unit rather than a traditional operating room.Citation31 Wherever the procedure is carried out, there must be excellent communication between the endoscopy and anesthesia teams and access to resources for unusual events, such as chest tube insertion by surgery or interventional pulmonology. In our practice, pulmonary medicine shares the same procedural area as therapeutic endoscopy.
We have not found it necessary to use more than standard American Society of Anesthesiologist monitors for POEM, although arterial blood pressure monitoring is a consideration for high-risk patients such as those with significant pulmonary disease.
Limitations
Limitations of our study include the small number of patients and the fact that data were gathered in a retrospective manner. Postprocedure pain management was not standardized for these cases. None of the patients were on preoperative opioids for chronic pain. This provided a homogenous group of subjects for analysis of postprocedure opioid use, but gives no insight into pain after POEM in opioid tolerant patients. More long-term studies of the outcome of POEM are needed, including development of gastroesophageal reflux disease and dysphagia control.
Conclusion
Our initial experience with POEM suggests that patients experience mild–moderate pain that is usually managed with modest doses of opioids. Nonopioid analgesics appear to be a useful part of a multimodal pain management plan. In terms of complications, no reported adverse outcomes occurred in our initial group of eleven patients. However, our literature review revealed a wide range of potential complications of interest to perioperative clinicians, notably pneumo/capnoperitoneum and pneumo/capnothorax, but also more serious events such as capnopericardium and aspiration. Awareness of these possible complications should contribute to the best possible outcome for patients. As always, the care team must communicate effectively and remain vigilant for potential adverse events.
Disclosure
The authors report no conflicts of interest in this work.
References
- BoeckxstaensGEZaninottoGRichterJEAchalasiaLancet20143839911839323871090
- InoueHMinamiHKobayashiYPeroral endoscopic myotomy (POEM) for esophageal achalasiaEndoscopy201042426527120354937
- KhashabMAEl ZeinMKumbhariVComprehensive analysis of efficacy and safety of peroral endoscopic myotomy performed by a gastroenterologist in the endoscopy unit: a single-center experienceGastrointest Endosc201683111712526212369
- WangJTanNXiaoYSafety and efficacy of the modified peroral endoscopic myotomy with shorter myotomy for achalasia patients: a prospective studyDis Esophagus201528872072725214469
- BecharaRIkedaHInoueHPeroral endoscopic myotomy: an evolving treatment for AchalasiaNat Rev Gastroenterol Hepatol201512741042626035678
- AkpinarZAslanFUnsalBPer-oral endoscopic myotomy in treatment of achalasia in a tertiary reference center in TurkeyNeurogastroenterol Motil20152738
- RajaSJegadeesanRThotaPNMeticulous technique of per-oral endoscopic myotomy (POEM) for achalasia is associated with low risk of complicationsGastrointest Endosc20151AB492AB493
- SharataAKurianAADunstCMBhayaniNHReavisKMSwanstromLLTechnique of per-oral endoscopic myotomy (POEM) of the esophagus (with video)Surg Endosc2014284133324570010
- Banks-VenegoniALDesiletsDJRomanelliJREarleDBTension capnopericardium and cardiac arrest as an unexpected adverse event of per-oral endoscopic myotomy (with video)Gastrointest Endosc201582611371139
- TanakaEMurataHMinamiHSumikawaKAnesthetic management of peroral endoscopic myotomy for esophageal achalasia: a retrospective case seriesJ Anesth201428345645924185834
- InoueHSatoHIkedaHPer-oral endoscopic myotomy: a series of 500 patientsJ Am Coll Surg2015221225626426206634
- KhashabMAMessallamAAOnimaruMInternational multicenter experience with peroral endoscopic myotomy for the treatment of spastic esophageal disorders refractory to medical therapy (with video)Gastrointest Endosc20158151170117725634487
- RenZZhongYZhouPPerioperative management and treatment for complications during and after peroral endoscopic myotomy (POEM) for esophageal achalasia (EA) (data from 119 cases)Surg Endosc201226113267327222609984
- VigneswaranYTanakaRGitelisMCarbrayJUjikiMBQuality of life assessment after peroral endoscopic myotomySurg Endosc20152951198120225249144
- Von RentelnDFuchsKHFockensPPeroral endoscopic myotomy for the treatment of achalasia: An international prospective multicenter studyGastroenterology20131452309311.e30323665071
- YangDPannuDZhangQWhiteJDDraganovPVEvaluation of anesthesia management, feasibility and efficacy of peroral endoscopic myotomy (POEM) for achalasia performed in the endoscopy unitEndosc Int Open201534E289E29526357672
- AslanFAkpinarZAlperEThe last innovation in achalasia treatment; per-oral endoscopic myotomyTurk J Gastroenterol201526321822326006194
- CaiMYZhouPHYaoLQZhuBQLiangLLiQLThoracic CT after peroral endoscopic myotomy for the treatment of achalasiaGastrointest Endosc20148061046105524998467
- CostamagnaGMarcheseMFamiliariPTringaliAInoueHPerriVPeroral endoscopic myotomy (POEM) for oesophageal achalasia: preliminary results in humansDig Liver Dis2012441082783222609465
- HuJWLiQLZhouPHPeroral endoscopic myotomy for advanced achalasia with sigmoid-shaped esophagus: long-term outcomes from a prospective, single-center studySurg Endosc20152992841285025492452
- HungnessESTeitelbaumENSantosBFComparison of perioperative outcomes between peroral esophageal myotomy (POEM) and laparoscopic Heller myotomyJ Gastrointest Surg201317222823523054897
- MekaroonkamolPLiLYDachaSGastric peroral endoscopic pyloromyotomy (G-POEM) as a salvage therapy for refractory gastroparesis: a case series of different subtypesNeurogastroenterol Motil20162881272127727197717
- MinamiHIsomotoHYamaguchiNPeroral endoscopic myotomy for esophageal achalasia: clinical impact of 28 casesDig Endosc20142614351
- OrensteinSBRaiganiSWuYVPeroral endoscopic myotomy (POEM) leads to similar results in patients with and without prior endoscopic or surgical therapySurg Endosc20152951064107025249143
- PatelKAbbassi-GhadiNMarkarSKumarSJethwaPZaninottoGPeroral endoscopic myotomy for the treatment of esophageal achalasia: systematic review and pooled analysisDis Esophagus201629780781926175119
- SaleemAMHennesseyHvon RentelnDVassiliouMCAtrial fibrillation as an unexpected complication after peroral endoscopic myotomy (POEM): a case reportSurg Laparosc Endosc Percutan Tech2014245e196e19925222714
- StavropoulosSNModayilRJFriedelDSavidesTThe International Per Oral Endoscopic Myotomy Survey (IPOEMS): a snapshot of the global POEM experienceSurg Endosc20132793322333823549760
- TangXRenYWeiZFactors predicting the technical difficulty of peroral endoscopic myotomy for achalasiaSurg Endosc20163093774378226659228
- UjikiMBYetasookAKZapfMLinnJGCarbrayJMDenhamWPeroral endoscopic myotomy: a short-term comparison with the standard laparoscopic approachSurgery20131544893897 discussion 897–90024074429
- von RentelnDInoueHMinamiHPeroral endoscopic myotomy for the treatment of achalasia: a prospective single center studyAm J Gastroenterol2012107341141722068665
- YangSZengMSZhangZYZhangHLLiangLZhangXWPneumomediastinum and pneumoperitoneum on computed tomography after peroral endoscopic myotomy (POEM): postoperative changes or complications?Acta Radiol201556101216122125277388
- ChiuPWWuJCTeohAYPeroral endoscopic myotomy for treatment of achalasia: from bench to bedside (with video)Gastrointest Endosc2013771293823043852
- InoueHKudoS-EPer-oral endoscopic myotomy (POEM) for 43 consecutive cases of esophageal achalasiaNippon Rinsho201068917491752 Japanese20845759
- KurianAADunstCMSharataABhayaniNHReavisKMSwanstromLLPeroral endoscopic esophageal myotomy: defining the learning curveGastrointest Endosc201377571972523394838
- LeeBHShimKYHongSJPeroral endoscopic myotomy for treatment of achalasia: initial results of a Korean studyClin Endosc201346216116723614126
- LiQLChenWFZhouPHPeroral endoscopic myotomy for the treatment of achalasia: a clinical comparative study of endoscopic full-thickness and circular muscle myotomyJ Am Coll Surg2013217344245123891074
- MeirelesORHorganSJacobsenGRTransesophageal endoscopic myotomy (TEEM) for the treatment of achalasia: the United States human experienceSurg Endosc20132751803180923525881
- RiederESwanstromLLPerrettaSLenglingerJRieglerMDunstCMIntraoperative assessment of esophagogastric junction distensibility during per oral endoscopic myotomy (POEM) for esophageal motility disordersSurg Endosc201327240040522955896
- SwanstromLLPeroral endoscopic myotomy for treatment of achalasiaGastroenterol Hepatol (N Y)20128961361523483860
- SwanstromLLRiederEDunstCMA stepwise approach and early clinical experience in peroral endoscopic myotomy for the treatment of achalasia and esophageal motility disordersJ Am Coll Surg2011213675175621996484
- VerlaanTRohofWOBredenoordAJEberlSRoschTFockensPEffect of peroral endoscopic myotomy on esophagogastric junction physiology in patients with achalasiaGastrointest Endosc2013781394423453184
- ZhouPHLiQLYaoLQPeroral endoscopic remyotomy for failed Heller myotomy: a prospective single-center studyEndoscopy201345316116623389963
- American Society for Gastrointestinal EndoscopyPCChandrasekharaVDesiletsDThe American Society for Gastrointestinal Endoscopy PIVI (preservation and incorporation of valuable endoscopic innovations) on peroral endoscopic myotomyGastrointest Endosc201581510871100e108125799295
- CommitteeNPWPStavropoulosSNDesiletsDJPer-oral endoscopic myotomy white paper summaryGastrointest Endosc201480111524950639
- TantauMCrisanDPeroral endoscopic myotomy: time to change our opinion regarding the treatment of achalasia?World J Gastrointest Endosc20157323724625789094
- ReinersmanJMWigleDABlackmonSHWongKeeSongLMPeroral Endoscopic Myotomy (POEM) Available from http://www.ctsnet.org/article/peroral-endoscopic-myotomy-poemAccessed August 10, 2016