
Abstract
Dental implants are placed endosseously, and the bone is the ultimate bearer of the occlusal load. Patients are not uniform in the maximum bite force they can generate. The occlusal biting load in the posterior jaw is usually about three times of that found in the anterior. It is possible for supporting implants to be overloaded by the patients’ biting force, resulting in bone loss and failure of the fixture. Bite force measurement may be an important parameter when planning dental implant treatment. Some patients can generate extreme biting loads that may cause a luxation of the fixture and subsequent loss of osseointegration. A patient with low biting force may be able to have a successful long-term outcome even with poor anatomical bone qualities. Patients with a high bite force capability may have an increased risk for late component fracture or implant failure. There is no correlation of any bite force value that would indicate any overload of a given implant in a given osseous site. Nonetheless, after bite force measurement, a qualitative judgement may be made by the clinician for the selection of an implant diameter and length and prosthetic design.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
A major indicator of the functional state of the masticatory system is the generated biting force.Citation1 The ability to bite is a function of the craniomandibular structures, including the muscles of mastication, the temporomandibular joint and the dentition, be it natural or artificial.Citation1
Biting and eating is an interaction of the physical properties of food and the mastication complex.Citation2 The mechanical factors of this interaction, where muscle contraction adaption to the food texture and density, are largely unknown.Citation2 The initial encounter of the jaws with the food is the factor that determines the subsequent muscle force in mastication.Citation2 Slow jaw velocity induces a low bite force for mastication.Citation2 Appropriate mastication is a quality-of life-issue, and the primary goal of implant supported dental rehabilitation.
In the course of dental implant treatment, failures are to be expected. Failures can occur early or late in treatment. There is controversy as to the causes for failures. Nonetheless, one cause for failure can be occlusal overload.Citation3,Citation4 Human mastication, dietary habits and parafunctional loads are cyclic and multidirectional and of variable magnitudes.Citation5–Citation7 The posterior human bite force magnitude is about three times that of the anterior.Citation7
Off-axial loads can be detrimental for a dental implant that is not embedded in an adequate thickness of cortical bone.Citation7–Citation9 To address an overload potential, it may be important to measure the maximal biting load a patient can generate. If the clinician suspects a potential for an overload, then a more substantial implant may be planned. This may be especially true when treating the anterior maxilla where almost all loading is inherently off axial.
The importance of bite force and its measurement for dental implant rehabilitation may become an integral part of the complete oral examination.Citation10,Citation11
Materials and methods
A MEDLINE PubMed literature search was made using the keywords: “jaw biting force AND bite load” and “bite force measurement”. Ninety-seven articles were retrieved, and 30 were deemed appropriate and discussed herein as well as additional articles deemed required for citation evidence.
Case example
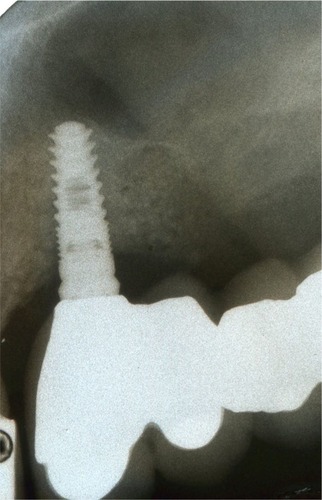
A 70-year-old male, with an unremarkable medical history and missing maxillary posterior teeth, desired a fixed partial denture to facilitate his prandial life pleasures. A complete oral clinical and radiographic examination was performed. A pneumatized antrum precluded implant placement at the maxillary left second premolar and first molar sites without augmentation. The patient declined a sinus floor elevation osseous augmentation to provide osseous volume to these sites. A long-span two-implant-supported fixed partial denture was planned for an anterior guidance occlusal scheme and treatment implemented. A 3.7×10 mm anterior implant and a 5.7×8 mm distal implant were used (). After 3 months of uneventful service, the anterior-most implant failed. The distal implant did not fail. An anterior guided occlusal scheme directs the bite forces axially, but the facial excursion of the lower jaw can place lateral loads on the anterior-most implant.
Figure 1 A 3.7×10 mm implant was placed and found to be inadequate to resist the patient’s extreme occlusal load of 1,200N.
A bite force measurement was taken and surprisingly was found to be 1,200 newtons (N), well above the published usual maximal of 900N. After removal and debridement, a larger diameter and longer (4.7×13 mm) mesial implant was placed, and after healing, a new fixed partial denture was fabricated and delivered ( and ). This prosthesis has had 2 years of uneventful service with no failure or unusual bone loss.
Figure 2 A larger and longer implant was placed to support the long-span fixed partial denture.
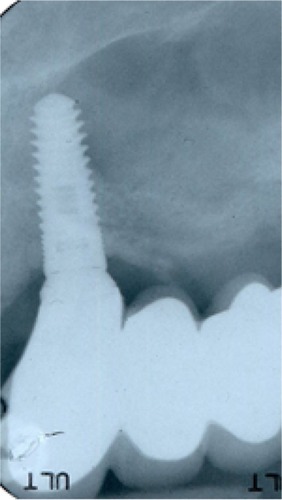
Figure 3 Two years of successful loading has occurred.

The patient in the case example has provided written informed consent for publication of the case details including images to this review.
Discussion
The biting force that a given patient is able to deliver may be an issue in case planning for oral rehabilitation. An assessment of the occlusal scheme, bone quality, volume, dietary habits, parafunction and patient biting force may be considered the parameters for implant treatment. Some studies show that dental patients can generally deliver a maximum jaw force in a range of 50–900N.Citation1,Citation12 However, the upper limit found in these studies may be in error. Anecdotally, this author has found a few outlying patients who can generate >900N.
Dentate patients develop osseous stress that causes apposition for increased osseous density around natural teeth. Under low loads, osseous apposition around dental implants can also occur.Citation13 Under high loads, implants can experience bone resorption or fracture.Citation13 Measuring this maximum force parameter may be important for implant selection and for prosthetic and occlusal design.
Occlusal forces are distributed through the mid-face skeleton in five vertical and two horizontal buttress planes.Citation14 The buttress planes are the nasomaxillary, zygomaticomaxillary, pterygo-maxillary, sagittal, frontal, zygomatic and maxillary. These osseous buttress planes resist the patient’s jaw force.
Cortical bone has been shown to be the primary support in the maxillary anterior.Citation14 However, both cortical and trabecular bones are equally involved in load resistance in the posterior maxilla.Citation14 Nonetheless, osseous quality remains as the primary parameter for implant support.Citation14
Loss of periodontal osseous support in natural teeth does not reduce bite force capability.Citation15 Thus, jaw bite force is muscle dependent and not tooth support or proprioception dependent.Citation15
Dental implant-supported prostheses are successful in functional occlusal loading, but still jaw forces are borne ultimately by the supporting bone.Citation7,Citation8,Citation16 Control of these forces by a well-designed occlusal scheme is an important parameter in treatment planning. Ascertaining the numerical value of a given patient’s maximum jaw biting force capability can be used to design an occlusal scheme and an array of implant size, number and position. However, the clinical assessment of a bite force value is obscure.
Various jaw positions induce activity in different muscles. In edge-to-edge jaw position, incisal loading induces masseter muscle activity.Citation16 The masseter muscles also dominate the action of the temporalis muscles during submaximal incisal biting function.Citation16 The relative activity of other muscles of mastication during function is difficult to measure due to their deep anatomical location.
Chronic and excessive incisal loads can induce stress to the temporomandibular joint (TMJ) complex.Citation16 Thus, patients who can generate excessive loads may induce a TMJ strain.Citation16 Additionally, “habitual chewing side syndrome” is a favoring of chewing on one jaw side characterized by a steeper condylar path, flatter lateral anterior guidance and habitual chewing on the symptomatic jaw side.Citation17
Implant design affects peri-implant bone stress in the anterior maxilla.Citation18 Implant designs with platform switching cause lower osseous stresses and strains than other implant designs.Citation19 This design induces less osseous strain than other designs with a patient with an increased biting load and thus may have less risk for marginal bone loss and overloading.Citation19
A high bite force can result in fractured implant components.Citation20 A cyclic off-axial force is capable of causing an abutment screw fracture.Citation20 Patients with a high bite force may have an increased risk for component fracture.Citation20
Patients with conventional removable non-implant-edentulous-ridge-supported complete dentures do not deliver as much of a load as compared to dentate patients.Citation21 However, implant-retained complete overdentures enable higher occlusal forces than conventional complete dentures.Citation21 There is improved stability and enhanced masticatory function with implant retention and support. In distal extensions, the implant-retained overdentures have a higher hydrostatic stress on mucosa at the posterior mandible.Citation21 The distal of the complete denture is in effect a cantilever when there is anterior implant retention. Hydrostatic pressure on the underlying mucosa correlates with bone resorption, which can induce mandibular ridge resorption.Citation21 The mean bone height loss after 10 years can be 0.5 mm.Citation13,Citation21 Nonetheless, control of occlusal loading by the occlusal scheme may help to minimize osseous resorption.Citation21 Removable prosthetic occlusal schemes are limited by the remaining osseous support, soft tissue and patient accommodation, among other factors. Interestingly, even if there is bone volume loss, bone density may be increased.Citation13,Citation21
Generally, a group function or lingualized occlusion is appropriate for removable dentures, but some patients do function with an anterior guided scheme. An anterior guided scheme directs the load to the anterior teeth where the loading force is about a third of that of the posterior region. Nonetheless, a high occlusal force can over load the anterior teeth or supporting bone.Citation5
Functioning of implant supported prosthetics is subjected to variable loads in direction and magnitude, and the occlusal scheme should direct the loads so as to minimize the ridge contact.Citation7,Citation8
Some patients are capable of delivering a range of bite loads that may affect the longevity of implant-supported prostheses.Citation7,Citation8 Supporting bone of adequate volume and density is very able to resist axial loads.Citation7 Nonetheless, off-axial loads may not be as well tolerated, and the supporting bone quality is the important issue here.Citation7,Citation8 A circumferential bone thickness of 1.8–2.0 mm may be required for a long-term functional and esthetic outcome.Citation9 Off-axial loads are directed to the four anatomical directions: mesial, distal, lingual and facial. Interproximal bone is generally dense and thick especially if there are natural teeth that are adjacent or a broad volume of supportive bone.Citation9 Interproximal bone does not have a facial or lingual osseous fossa or an apical concavity.Citation22 Lingual bone is generally thicker than facial bone and thus is more supportive and more likely able to resist off-axial loads.Citation22
Anterior facial cortical bone generally is thinner or absent and resorbs as socket healing progresses from the apex of the healing socket.Citation22 Poor healing may result in a site that provides poor resistance to facial off-axial loads due to a thin poorly supportive cortex.Citation22 There will be no buttressing that would be provided by thick cortical bone. Thick lingual bone or a broad proximal expanse of an edentulous ridge can provide adequate support for loads directed in these directions. Thus, thin facial bone may be prone to microfracture and resorption under off-axial loads and lead to early or late implant failure.Citation9 Thus, the density and thickness of the facial bone may be the most important factors in long-term function because off-axial loads directed toward the facial may be most at risk for an overload.Citation9 Nonetheless, a patient with a very low generated jaw force may be able to have a successful prosthesis supported by low-volume or poor quality bone. Nonetheless, the critical event value of a biting load for a particular osseous density is not known.
The axial and buffered loading of mini implants that retain a complete mandibular overdenture may not cause marginal bone loss.Citation23 One study of two mini implants (1.8×15 mm) retaining a complete mandibular overdenture did not demonstrate marginal bone loss even after 15 months of function.Citation23 The mini implants in this study were very narrow (1.8 mm) but very long (15 mm). Loads on these implants may be less because removable complete denture patients do not generate as great a load as dentate patients. The denture retainers are soft and give under load, thus buffering or damping the load stress. Nonetheless, bite force measurement in these patients may aid in treatment design for a successful prosthesis. Patients with high bite force capability may overload narrow diameter implants and need longer or wider implants to resist the delivered higher load.
Off-axial loading may be an issue for implant or component fracture.Citation19 In the anterior maxilla where all loads are off axial, measurement of these patient’s bite force may indicate the use of wider diameter implants or implant splinting to better resist this type of load. In one in vitro study, an off-axial load of >250N resulted in fracture of the abutment screw or the implant cervical.Citation19 Thus, a preoperative bite load measurement may prevent late prosthetic complications by increasing the number or size of the supporting implants.
A patient’s diet and bite force load may work in tandem to overload an implant-supported prosthesis. For example, some patients have a chronic popcorn habit that may induce an off-axial over load.Citation5 A patient with high bite force may overload implants, especially from crunching on un-popped kernels. A patient with low biting load may have a successful prosthesis regardless of any detrimental eating habits or parafunction.
The patient’s state of mind may influence the ability to measure the maximum force.Citation11 During the measurement of a bite force, patient reluctance to cooperate or fatigue may cause a reduced reading.Citation11
At prosthetic delivery, leaving the occlusal surface approximately 30 microns short of the opposing contact does not appear to significantly reduce loading during food mastication.Citation24 It is the practice of many dentists to leave a slight occlusal gap to prevent the sole occlusal contact of the implant crown during functional intrusion of the adjacent natural teeth. The hope is to lessen the loading impact on the prosthesis in parafunction. Nevertheless, this may not lessen the load created during mastication.
Taken together, all the physiologic treatment planning parameters may be significantly influenced by a very high or very low bite force. With a low force, the bone can be less dense and still tolerate the occlusal load. An anterior guided scheme may be tolerated, prosthetic teeth can be esthetically ramped, implants can be placed off axially without detriment and narrow diameter implants may be used. It remains to be seen that loads can be successfully tolerated by a high bite force.
Bite force measurement devices
Bite force can be easily measured using any of several devices available.Citation10
One device measures the submaximal bite force with a sensor and a strain gauge bite fork.Citation1 This device reported a range of 50–800N with a 93% reliability.Citation1
Another electrically passive device safe for intraoral use is a fiber Bragg grating bite force recorder.Citation25 It has a measurement range of 0–900N.Citation25 This is calibrated with a Micro Universal Testing Machine (UTM) to a resolution of 0.54N. A measured range of 176–635N was found.Citation25
Another device comprises a quartz force transducer sensor and a microprocessor with a liquid crystal display (LCD), contained in a steel housing.Citation12 This device measured a mean maximal bite force of 847N for men and 597N for women. All readings were taken in the posterior jaw.Citation12
A piezoelectric device uses a flexible polyimide electrode and barium titanate-based multilayer ceramic capacitors.Citation26 This sensor has high fracture strength and good sensing properties. This low-cost device has a 5% error range.Citation26
Lipski and coworkers evaluated a device manufactured by Tekscan (South Boston, MA, USA) and found it useful in determining the jaw bite force ().Citation11 It comprises of a pressure sensor, a computer and proprietary pressure measurement software. The sensor consists of layers of pressure sensitive films and adhesives connected to a circuit (–). As the bite force increases, the electronic resistance decreases, and this is measured and converted to newtons ( and ). The pressure sensor is sheathed in a plastic sleeve for contamination control (). The device is positioned on or very near the arch site of the proposed implant (). After cajoling the patient into a relaxed normalized jaw position, the patient is then asked to gradually bite down on the sensor with as much force as they can. Patients may not be able to exert their true maximum biting force for various reasons.Citation11 Several readings may be needed to insure consistency. Patients need to ease their muscle contraction before they feel discomfort. The load value in newtons is then displayed by the software, and this is recorded in the patient’s chart.
Figure 4 The pressure sensor.
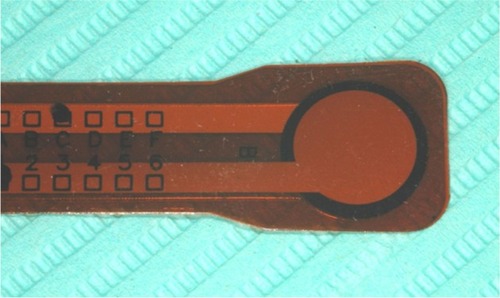
Figure 5 Schematic of sensor construction.
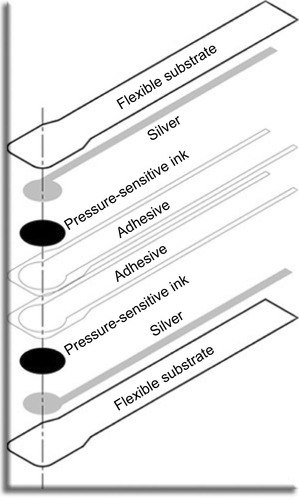
Figure 6 Circuitry of a sensor.
Abbreviations: Vout, voltage out; VT, voltage transfer power source.
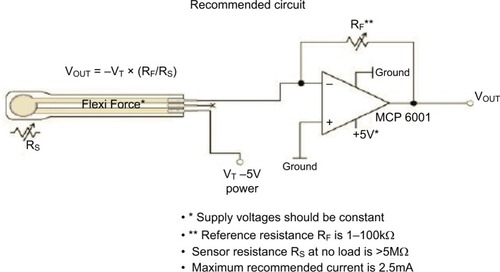
Figure 7 As the force on the sensor increases, the electronic resistance decreases, and this is measured.
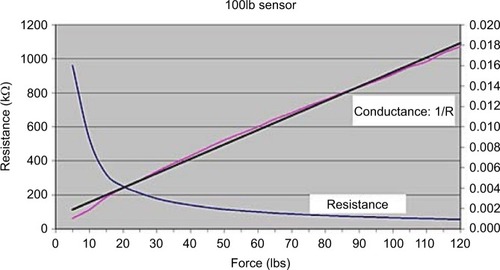
Figure 8 The pressure sensor with cushioned flexible pads to allow for accurate biting registration.

Figure 9 The pressure sensor is placed in the patient’s mouth in the site where the loading will occur and the patient is instructed to bite with maximum force.

In an in vitro study, Rottner and coworkers found that a piezoelectric transducer foil of 33 microns thick can accurately measure the biting force.Citation27 These use the pressure-dependent electric resistance quality of the piezoelectric foil to measure the biting load. These subjects were instructed to bite down as hard as they could for 1 second. They found that occlusal morphology influenced the results. Cusp angles caused a wedging effect that gave higher measurements.Citation27 Because of differing occlusal morphology individual calibration of the device is required for accuracy.Citation27 Thus, any measuring device needs a sensor design that eliminates individual wedging occlusal tooth anatomy as a confounding factor.
Jaw force measurements may need to be normalized with electromyography to a maximal voluntary bite before measurement to insure an accurate reading; otherwise, maximal bite force values may be distorted by uncoordinated muscle activity.Citation28 Surface electromyography may eliminate a confounding muscle issue for bite force recordings.Citation29 Soft bite surfaces on the sensors are needed for reliability when measuring the maximum voluntary bite force.Citation30
The load value measurement is evaluated in relation to the range of reported human bite forces. A clinical judgement can then be made about occlusal scheme, the number of implants and size, splinting and implant positioning. The range of a human jaw biting force is 50–800N.Citation1 If the patient is measured at the high end of this range, then planning may need to include: ridge splitting expansion to increase bone volume, additional implants and splinting for support, narrow flat plane occlusal tables, anterior guided occlusal scheme, parafunction and dietary considerations.Citation7 Extracortical bone grafting may not provide as much support as a ridge-expanded site.Citation7 Patients at the low end of the bite force range probably need no preemptive prosthetic design features. Although implant-supported maxillary anterior prosthetics especially need to be designed with occlusal loads in mind.Citation7
Bruxism during sleep was measured by Nishigawa and coworkers.Citation31 They found a nocturnal mean amplitude of 22.5 kilogram-force (kgf) with a mean duration of 7.1 seconds.Citation31 The average daytime force measured on the subjects was 79.0 kgf with a range of 51.8–99.7 kgf. Thus, the nocturnal bruxism force was 53.1% of the daytime generated force. However, a few subjects did generate a higher magnitude of nocturnal bruxing force than daytime generated voluntary bite force.Citation31
Conclusions
Bite force may be an important parameter in implant selection and prosthetic case planning especially in patients who are capable of delivering very high occlusal loads. Since the facial cortical bone may be at most risk for overload and subsequent implant failure, the magnitude of the patient’s bite force may be an issue for a long-term successful outcome, especially in maxillary anterior prostheses. There are available devices and methods that provide a convenient way to measure the generated load of a patient.
Bite force may be an important planning parameter. A patient that generates an excessive load may need to have the implant size and the number and occlusal design features that can adequately resist the load.
A high bite force capability may indicate a high risk for a late component fracture. Multiple or wide or long implants, implant positioning, an anterior guided occlusal scheme, splinting and ridge expansion augmentation, as opposed to extracortical grafting, may be considered to increase the osseous support or deflect or minimize the occlusal load. A patient with low biting force may be able to have a successful long-term outcome even with poor anatomical bone qualities.
Nonetheless, at this time, there is no correlation of any bite force value that would indicate any overload of any particular implant in any particular osseous site.
Acknowledgments
The author has no interest, financial or otherwise, of any of the products and methods discussed herein. All images are taken from the patients record and written informed consent for treatment and medical education was obtained for this study. All images were obtained with permission from the commercial entities involved.
Disclosure
The author reports no conflicts of interest in this work.
References
- FernandesCPGlantzPOSvenssonSABergmarkAA novel sensor for bite force determinationsDent Mater200319211812612543117
- DanHKohyamaKInteractive relationship between the mechanical properties of food and the human response during the first biteArch Oral Biol200752545546417178099
- PeixotoCDAlmasKThe implant surface characteristics and periimplantitis. An evidence-based updateOdontostomatol Trop201639153233527434917
- DemenkoVLinetskiyILinetskaLPrognosis of implant longevity in terms of annual bone loss: a methodological finite element studyComput Methods Biomech Biomed Eng2016192180187
- FlanaganDDiet and implant complicationsJ Oral Implantol201642330531026451670
- MeskoMEAlmeidaRCPortoJAKollerCDda RosaWLBoscatoNShould occlusal splints be a routine prescription for diagnosed bruxers undergoing implant therapy?Int J Prosthodont201427320120324905259
- NagasawaMTakanoRMaedaTUoshimaKObservation of the bone surrounding an overloaded implant in a novel rat modelInt J Oral Maxillofac Implants201328110911623377055
- Ben-GalGLipovetsky-AdlerMHaramatyOSharonESmidtAExisting concepts and a search for evidence: a review on implant occlusionCompend Contin Educ Dent201334Spec No2631 quiz 32
- SprayJRBlackCGMorrisHFOchiSThe influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncoveringAnn Periodontol20005111912811885170
- FlanaganDJaw bite force measuring deviceJ Oral Implantol201238436136420822470
- LipskiTKijakEWitaszekEGaskaDMargielewiczJApplication of dental dynamometer in biomechanicsJ Meas Eng2015311722
- WaltimoAKönönenMA novel bite force recorder and maximal isometric bite force values for healthy young adultsScand J Dent Res199310131711758322012
- MosnegutuAWismeijerDGeraetsWImplant-supported mandibular overdentures can minimize mandibular bone resorption in edentulous patients: results of a long-term radiologic evaluationInt J Oral Maxillofac Implants20153061378138626574862
- JanovicASaveljicIVukicevicAOcclusal load distribution through the cortical and trabecular bone of the human mid-facial skeleton in natural dentition: a three-dimensional finite element studyAnn Anat2015197162325458179
- KleinfelderJWLudwigtKMaximal bite force in patients with reduced periodontal tissue support with and without splintingJ Periodontol200273101184118712416777
- Santana-MoraUMartínez-ÍnsuaASantana-PenínUdel PalomarAPBanzoJCMoraMJMuscular activity during isometric incisal bitingJ Biomech201447163891389725442299
- Santana-MoraULópez-CedrúnJMoraMJOteroXLSantana-PenínUTemporomandibular disorders: the habitual chewing side syndromePLoS One201384e5998023593156
- YamanishiYYamaguchiSImazatoSNakanoTYataniHEffects of the implant design on peri-implant bone stress and abutment micromovement: three-dimensional finite element analysis of original computer-aided design modelsJ Periodontol2014859e33e338
- TanasićITihacek-SojićLMilić-LemićAFinite element analysis of compressive stress and strain of different implant forms during vertical loadingInt J Comput Dent201417212513325098160
- FlanaganDIliesHMcCulloughPMcQuoidSMeasurement of the fatigue life of mini dental implants: a pilot studyJ Oral Implantol200834171118390237
- ChenKWLinTMLiuPRAn analysis of the implant-supported overdenture in the edentulous mandibleJ Oral Rehabil2013401435023121231
- FlanaganDA comparison of facial and lingual cortical thicknesses in edentulous maxillary and mandibular sites measured on computerized tomogramsJ Oral Implantol200834525625819170291
- JofreJHamadaTNishimuraMKlattenhoffCThe effect of maximum bite force on marginal bone loss of mini-implants supporting a mandibular overdenture: a randomized controlled trialClin Oral Impl Res201021243249
- ZhaoXZhangLSunJYangZYXieQFThree-dimensional finite element analysis of influence of occlusal surface height on stress distribution around posterior implant-supported single crownBeijing Da Xue Xue Bao20164819410026885916
- UmeshSPadmaSAsokanSSrinivasTFiber Bragg grating based bite force measurementJ Biomech201649132877288127432747
- LinKRChangCHLiuTHLinSWLinCHExperimental and numerical estimations into the force distribution on an occlusal surface utilizing a flexible force sensor arrayJ Biomech201144101879188421565347
- RottnerKRichterEJEffect of occlusal morphology on the accuracy of bite force measurements using thin film transducersInt J Prosthodont200417551852315543907
- CrawfordSRBurdenAMYatesJMZiouposPWinwoodKCan masticatory electromyography be normalised to submaximal bite force?J Oral Rehabil201542532333025600826
- FerrarioVFSforzaCZanottiGTartagliaGMMaximal bite forces in healthy young adults as predicted by surface electromyographyJ Dent200432645145715240063
- SerraCMMannsAEBite force measurements with hard and soft bite surfacesJ Oral Rehabil201340856356823692029
- NishigawaKBandoENakanoMQuantitative study of bite force during sleep associated bruxismJ Oral Rehabil200128548549111380790