
Abstract
The Closure Fast™ Endovenous Radiofrequency Ablation Catheter is the latest version of a minimally invasive system for the treatment of patients with superficial venous disease. The Closure Fast™ catheter heats the vein wall to 120°C, causing denaturation of the collagen of the vein wall and contraction of the vessel such that no blood can flow through it. Nearly one million systems have been sold since the product was launched. Many, if not all, patients can be treated under local anesthesia with the Closure Fast™ catheter. Duplex ultrasound reports occlusion rates for the treated vein of 94%–98% at 1 year and 85%–93% at 3 years. The system produces average postoperative pain scores of less than 2 out of 10 on a visual analog score. In the first postoperative week, 76% of patients do not require analgesia. Some 45% of patients return to normal activity on the first postoperative day. Serious complications appear to be rare following the Closure Fast™ procedure. Transient paresthesia occurs in 0.2% of cases, thrombophlebitis in 1%–10%, and thromboembolic events in up to 1.4%, mainly heat-induced thrombosis. Closure Fast™ adds significant costs to treating superficial venous disease but studies have shown it to be cost-effective when used in an office setting.
Aim
This paper aims to analyze current published research on the Closure Fast™ Endovenous Radiofrequency Ablation Catheter.
Introduction
The introduction of minimally invasive endovenous radiofrequency ablation (RFA) has revolutionized the treatment of venous incompetence. Endovenous RFA was approved for used by the National Institute for Health and Clinical Excellence (NICE) in the UK in 2001 and the guidance published in September 2003. NICE guidance states that “Current evidence on the safety and efficacy of radiofrequency ablation of varicose veins appears adequate to support the use of this procedure as an alternative to saphenofemoral ligation and stripping, provided that the normal arrangements are in place for consent, audit and clinical governance.”Citation1 There are several perceived advantages of endovenous RFA over traditional surgery, including reduced pain, faster recovery times, and lower complication rates.
The Closure Fast™ (formally known as VNUS® ClosureFAST, Covidien, Dublin, Ireland) Endovenous Radiofrequency Ablation Catheter is the latest version of a minimally invasive system for the treatment of patients with superficial venous disease. Covidien manufactures the catheter and the associated procedure is termed Venefit™. Nearly one million systems have been sold since the product was launched (personal communication with Covidien Sales, January, 2014). Along with laser ablation systems, and foam sclerotherapy and its predecessors (Closure™ and Closure plus™),Citation2 Closure Fast™ has helped to revolutionize the way that patients with varicose veins can be treated.
Methods
A systematic review of online databases, web of knowledge, and PubMed was carried out. The following search terms were used: “ClosureFast,” “Radiofrequency Ablation catheter,” “varicose veins,” “saphenous vein.” A total of 30 papers were deemed acceptable for the criteria required to answer the question posed by this paper.
Mechanism of action
Closure Fast™ is one of a class of systems that uses thermal energy to destroy both the endothelium and the collagen within the walls of veins. The Closure Fast™ catheter heats the vein wall to 120°C. This temperature has been shown to be sufficient to cause proteins in the wall of the vein to denature. Thermal injury results in changes in the collagen of the vein wall and contraction of the vessel such that no blood can flow through it.Citation3 Over time, the vein is gradually reabsorbed by the body’s natural mechanisms so that there is little, if any risk of recanalization.
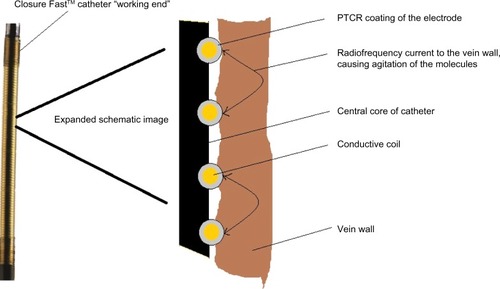
The patent for Closure Fast™ was filed in 2005 and granted in 2009 (US patent 7517349 B2).Citation4 It is described as an electrosurgical instrument and method for treating varicose veins using an elongated catheter. “The distal end carries a coiled electrode with a positive temperature coefficient of resistance (PTCR) surface and an electrode with a pressure sensitive variable resistance to provide a smart surface for controlling radiofrequency current fow at the interface between the electrosurgical surface and the tissue.”Citation4 In plain English, this means a coil of wire around a catheter with a feedback system that ensures that the wire heats tissue to a constant temperature of 120°C, independent of the temperature and conductivity of the tissue, and avoids the formation of charring. Along with its predecessors and radiofrequency competitors, the Closure Fast™ uses bi-polar radiofrequency to cause ohmic heating of tissue. The conductive coil delivers a radiofrequency current to the vein wall, causing agitation of the molecules in the wall, heating, and then denaturation of the proteins (). As the tissue heats up, it warms the PTCR coating of the electrode, which in turn reduces the radiofrequency flow and avoids overheating and subsequent charring of the tissue. This problem occurred with the Closure™ and Closure plus™ systems and requires cleaning of the electrode. It is also known to occur with the Celon system.
Figure 1 Image of the distal end of the Closure Fast™ catheter (ClosureFAST, Covidien, Dublin, Ireland) with expanded schematic diagram to illustrate the process of radiofrequency ablation of the vein wall.
Description of Venefit technique
Along with other thermal systems, Celon,Citation5 and laser and steam,Citation6 the Closure Fast™ catheter can only be used in relatively straight vessels such as the great saphenous, small saphenous, and anterior saphenous veins.Citation7 It is necessary to ablate these vessels in order to reduce the risk of a failed procedure.Citation8 The patients should be positioned supine for treatment of the great saphenous or anterior thigh vein, and in the prone position for ablation of the small saphenous or inter-saphenous veins.
The Venefit procedure, using Closure Fast™, is similar to other methods of minimally invasive vein therapy. Briefly, the patient’s symptoms need to be assessed and their varicose veins examined using duplex ultrasound. Once it has been established that the truncal vein is incompetent, the procedure involves percutaneous cannulation and insertion of a 7F sheath into the target vein.Citation9 Using ultrasound, the Closure Fast™ catheter is advanced through the sheath and into the lumen of the vein to the most proximal part that needs to be treated. The final placement of the catheter tip must be 2 cm from the saphenofemoral junction. If the vein has a tortuous or kinked section, a 0.18-inch guidewire can be advanced along the vein and the catheter can be introduced in a standard over-the-wire technique.
The “working end” of the Closure Fast™ comes in two lengths – 7 cm and 3 cm. Clinicians mostly use the longer system, with the shorter one being reserved for situations where only a short length of vein needs to be treated. The 3 cm length was introduced in 2010, possibly to address one of the perceived advantages of a competing system (the Olympus Celon RF system).Citation5
The site of cannulation is determined by the anatomy of the patient, but clinicians should aim to introduce the device as distally as possible, in order to treat the maximum amount of incompetent vein. There is little point in introducing the 7 cm system within 10 cm of the junction between the superficial truncal vein and its connection to the deep vein. In shorter sections of this type, the 3 cm device can be used.
Provided the clinician can cannulate the vein and introduce a sheath, most truncal veins can be treated. Problems can occur if the preoperative duplex fails to identify areas of scarring within the vein; this can make it difficult to pass the catheter and results in an abandoned procedure with the attendant frustration and cost. It is therefore essential that the clinician fully examines the truncal vein with ultrasound to exclude any areas of scarring. In a long vein with a single area of scarring or severe tortuosity, the catheter can be introduced above and below the abnormal area via two punctures and two sheaths. These same problems and solutions occur with laser fibers and the Celon catheter. If there is too much scarring, then foam sclerotherapy of the vein should be considered.
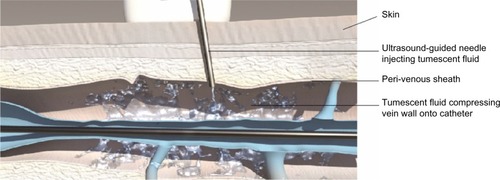
In order to reduce the risk of collateral damage to nerves and other tissue, it is essential that the Venefit procedure is performed in combination with tumescent anesthesia. This involves the injection of crystalloid solution, usually combined with a locally acting anesthetic, along the length of the vein to be treated. As compression is used, veins which have sections of more than 1.5 cm diameter can be treated using Closure Fast™. Once the catheter is in place with the patient’s foot elevated, using ultrasound, the tumescent crystalloid fluid is injected into the perivenous sheath so that the whole vein is surrounded by a “halo” of fluid which compresses the vein wall onto the catheter and insulates structures that surround the vein (). Tumescent anesthesia is also used with laser and steamCitation10,Citation11 systems and means that many, if not all, patients can be treated under local anesthesia. This is often cited as being better for patients, allows procedures to be done in an “outpatient” or “office” environment, and reduces the cost of the procedure.Citation12
Figure 2 Diagram showing the injection of tumescent fluid, using ultrasound control, into the perivenous sheath in order to compress the vein wall onto the Closure Fast™ catheter (ClosureFAST, Covidien, Dublin, Ireland).
Once tumescent anesthesia has been correctly infused into the patient’s leg, the catheter is then attached to a generator (), which, when switched on, delivers the radiofrequency energy. Each section of vein (7 cm or 3 cm) is heated for 20 seconds before the energy is automatically switched off. The catheter is then manually withdrawn to the next marker on the catheter (7 cm or 3 cm, respectively) and energy is then applied to the next section. In this way, a typical great saphenous vein can be treated in under 3 minutes (49 cm takes 7 × 20 seconds =140 seconds) without the operator having to withdraw the catheter at a steady rate as is required for laser ablation or the Celon system. It is therefore very easy to use. Ultrasound examination of the vein wall normally demonstrates that it is thickened and more echogenic than before the procedure with a smaller total vein diameter.Citation13 This normally indicates successful treatment. Double treatment of each 7 cm section has been suggested to improve outcomes but one small study of 67 treatments showed no benefit at 1 year, although the reduction in diameter was greater.Citation14
Figure 3 Image of the Closure Fast™ catheter (ClosureFAST, Covidien, Dublin, Ireland) connected to the Venefit™ Generator.

Once completed, the Closure Fast™ system and sheath are removed. The system can be used multiple times on the same patient during the same operating session and is then disposed of as it is designed for single patient use. There are reports of reprocessed devices being used in order to save institutions US$178 per procedure without any apparent detrimental outcome.Citation15 There are no reports of cross-infections as a result.
Once the Venefit™ procedure has been completed, any residual varices can be left alone, removed by phlebectomies, or treated by foam sclerotherapy.Citation13
Findings from literature search
There have been several studies reporting the efficacy of the Closure Fast™ system. Duplex ultrasound reports occlusion rates of 100% at 1 week,Citation16 97%–99.7% at 3 months,Citation13,Citation17 94%–98% at 1 year,Citation13,Citation16,Citation18,Citation19 and 85%–93% at 3 years.Citation11,Citation13
When compared with other techniques such as laser, steam, traditional surgery, and foam sclerotherapy, it appears that Closure Fast™ is equally efficacious but may have a lower pain and side effect profile.Citation6
Pain
One of the advantages of Closure Fast™ is reduced postoperative pain when compared with other endothermal methods and traditional surgery. In studies done under local anesthesia, Closure Fast™ produced average pain scores of between 3 and 4 out of 10 on a visual analog scale during the procedure (from the injection of tumescence). The average postoperative pain scores were less than 2 in the first week, with up to 76% of patients not requiring analgesia and those that did taking only paracetamol and simple non-steroidal anti-inflammatory drugs.Citation18,Citation20,Citation21 The 46 patients in the RECOVERY study had pain scores of less than 1 at 48 hours reducing still further over the first week.Citation22
Return to normal activity
In a study of 104 patients, 45% returned to normal activity on the first postoperative day, with 100% at 1 week.Citation20 Other studies have reported the number of days unable to work after the procedure to be 1 day, with a range of 0–28 days.Citation17,Citation18,Citation21
Complications
Serious complications appear to be rare following the Closure Fast™ procedure. No articles were identified in a literature search that specifically assessed complications following the use of Closure Fast™. The complications described below have been obtained from the various studies describing clinical outcomes but include a recent article analyzing over 2,000 treatments, 317 of whom had Closure Fast™.Citation23
There have been no published reports of intra-operative complications as have been seen with laser treatment.Citation24 The senior author has, however, seen photographs of the coiled element unwound after the operator using the needle for tumescent anesthesia damaged it.
Another intra-operative injury reported by personal communications included direct thermal damage to the skin when the 7 cm “working” end was partly in the patient and partly in the sheath used to access the target vein. Clinicians need to ensure that the sheath is removed when they see the “hatched” markings on the catheter, indicating that the “working end” is close to the vein puncture site. Skin burns occurred in 0.7% of patients in two studies reporting the complication.Citation23
Both of these intra-operative complications were due to operator error rather than device failures.
Paresthesia, probably related to either thermal injury or the effects of inflammation on cutaneous nerves occurs in 0.2%–13.7% of patients.Citation11,Citation13,Citation16,Citation18,Citation22 Most symptoms are transitory and tend to settle within a few weeks of treatment.
Skin pigmentation is reported to occur in 0.2%–5.5% of treatments.Citation11,Citation13,Citation16,Citation18,Citation22 This is likely to occur in patients where the treated vein runs close to the skin, as occurs in slim patients. It can also occur when the clinician treats a tributary of the truncal vein rather than treating the vein in its perivenous sheath. It has been suggested that veins close to the skin might be better treated with phlebectomies to avoid such a side effect.
Thrombophlebitis after Closure Fast™ treatment is reported to occur in 1%–10% of patients.Citation8,Citation12,Citation15–Citation18
Iatrogenic arteriovenous fistula formation has been reported to occur following endovenous laser ablation and there is at least one report of it occurring following the Closure Fast™ procedure. In order to avoid this and possibly many of the complications associated with the technique, it is essential that adequate tumescent fluid is injected around the target vein, particularly where it is close to the deep venous system (the saphenofemoral junction).Citation25
Thromboembolic events occurred in up to 1.4% of patients.Citation11,Citation13,Citation16,Citation18,Citation19 There are reports of a specific complication related to endothermal ablation techniques – endovascular heat-induced thrombosis (EHIT). This can occur in up to 8% of treatments and is characterized by protrusion of the thrombus from the truncal vein into the deep vein, causing a partial occlusion. It appears to be more likely following treatment of the small saphenous veins, in large veins, and in patients with an underlying thombophilia.Citation26,Citation27 EHIT also appears to occur if the distance between the deep vein and the most proximal point of treatment is less than 2.5 cm.Citation28 The problem normally presents as a finding on posttreatment duplex scans and can resolve without any anticoagulation treatment. A four-level classification system and management strategies have been suggested for EHIT.Citation28,Citation29 Patients with complete occlusion of the deep vein by EHIT should be treated with anticoagulation while partial occlusion may be left to the clinician’s discretion, although debate continues on the matter. The advice is that all patients should have duplex follow-up after the first week, although many units may not do so.
Cost
The “cost of sales” of the Closure Fast™ system adds a significant expense to treating a patient with venous disease when compared with the cheap disposable stripping devices used for conventional surgery. This additional cost has, in the past, prohibited more widespread use, but there is some evidence that when used for local anesthetic procedures, with minimal additional staff, Closure Fast™ can be a cost-effective alternative.
In Germany, the impact of the introduction of Closure Fast™ to the statutory health insurance catalog was assessed.Citation30 Using a multi-cohort Markov model, which looks at the number of procedures a patient needs to remain free of the symptoms of varicose veins over 5 years, the introduction of Closure Fast™ would save €19.1 million when compared with open surgery. If Closure Fast™ was not used, of the estimated 1.6 million procedures done over 5 years, 38% would have required an inpatient stay. With the introduction of Closure Fast™, this was calculated to reduce to 32%. The indirect cost savings of an early return to work were not calculated, but if they were, then the benefit for the country as a whole would have been greater.
A clinical effectiveness and economic evaluation performed in the UK was not as favorable as the German model, but marginally favored less invasive techniques such as Closure Fast™, when compared with surgery.Citation31 The UK researchers stated that there is considerable uncertainty in the cost differences between treatments. Their analysis suggests that the additional costs of Closure Fast™ would have to be no more than £24 per case when compared with stripping, to be considered cost-effective at a quality of added life year (QALY) of £20,000. In real terms, this means that the cost of personnel and location required to perform the procedure needs to be reduced from the stripping under general anesthesia cost of £1,100 to less than £700 given the cost of the Closure Fast™ system; the introducer kit and generator in the UK is in the order of £400. For most hospitals, that means the procedure needs to be done under local anesthesia in an outpatient setting.
Research from the US confirms that systems like Closure Fast™ are cost-effective when used in the office setting. When performed in an operating theatre, Closure Fast™ would cost the hospital $1,123 (revenue $3,761, cost of procedure $4,884) while an office-based procedure would lead to a “profit” of $845 (revenue $1,919, cost $1,074).Citation12
Conclusion
There have been a variety of articles, meta-analyses, and systematic reviews on the various methods to treat patients with superficial venous disease.Citation6,Citation32 At scientific meetings across the world, there continues to be heated debates on which method is best, often fuelled by personal preferences and statements, typical of surgical egos, namely “my way is best”. The evidence from all of these comparative studies suggests that patients can be offered any of the various treatment options, with very similar results and side-effect profiles when Closure Fast™ is compared with other thermal techniques. The sales figures from the manufacturers and some of the cost-effectiveness studies also suggest that Closure Fast™ has an important place in the treatment of superficial venous disease.
While clinician preference determines what method is currently used, it seems that the scientific results show Closure Fast™ to be safe and efficacious with a low side-effect profile, with a cost-effective bonus included.
Disclosure
The authors have no conflicts of interest. They have never received funding from Covidien or VNUS technologies.
References
- National Institute for health and Care Excellence (NICE)Radiofrequency Ablation of Varicose Veins. IPG8London, UKNICE2003 Available from: http://publications.nice.org.uk/radiofrequency-ablation-of-varicose-veins-ipg8/guidanceAccessed March 20, 2014
- SiribumrungwongBNooritPWilasrusmeeCAttiaJThakkinstianAA systematic review and meta-analysis of randomised controlled trials comparing endovenous ablation and surgical intervention in patients with varicose veinEur J Vasc Endovasc Surg20124421422322705163
- ThomisSVerbrugghePMilleretRVerbekenEFourneauIHerijgersPSteam ablation versus radiofrequency and laser ablation: an in vivo histological comparative trialEur J Vasc Endovasc Surg20134637838223835108
- TruckaiCShadduckJHinventorsVnus Medical Technologies, Inc., original assigneeElectrosurgical instrument and method United States patent US 7517349 B24142009
- GoodeSDChowdhuryACrockettMLaser and radiofrequency ablation study (LARA study): a randomised study comparing radiofrequency ablation and endovenous laser ablation (810 nm)Eur J Vasc Endovasc Surg20104024625320537570
- EklöfBPerrinMReview of randomized controlled trials comparing endovenous thermal and chemical ablationRev Vasc Med201421112
- GoodeSDKuhanGAltafNSuitability of varicose veins for endovenous treatmentsCardiovasc Intervent Radiol20093298899119536594
- JonesLBraithwaiteBDSelwynDCookeSEarnshawJJReprinted article “Neovascularisation is the principal cause of varicose vein recurrence: results of a randomised trial of stripping the long saphenous vein”Eur J Vasc Endovasc Surg201142Suppl 1S57S6021855024
- HiggsZCMacafeeDABraithwaiteBDMaxwell-ArmstrongCAThe Seldinger technique: 50 years onLancet20053661407140916226619
- MilleretRHuotLNicoliniPGreat saphenous vein ablation with steam injection: results of a multicentre studyEur J Vasc Endovasc Surg20134539139623410966
- RasmussenLHLawaetzMBjoernLVennitsBBlemingsAEklofBRandomized clinical trial comparing endovenous laser ablation, radiofrequency ablation, foam sclerotherapy and surgical stripping for great saphenous varicose veinsBr J Surg2011981079108721725957
- LinJCNerenzDRMigliorePYoungRShepardADWeaverWDCost analysis of endovenous catheter ablation versus surgical stripping for treatment of superficial venous insuffciency and varicose vein diseaseJ Vasc Surg Venous Lymphat Disord2014298103
- ProebstleTMAlmJGöckeritzOThree-year European follow-up of endovenous radiofrequency-powered segmental thermal ablation of the great saphenous vein with or without treatment of calf varicositiesJ Vasc Surg20115414615221439757
- García-MadridCPastor ManriqueJOSánchezVASala-PlanellEEndovenous radiofrequency ablation (Venefit Procedure): impact of different energy rates on great saphenous vein shrinkageAnn Vasc Surg20132731432123384556
- IsobeJHSentellKCNicholsLASimmsCSTwelve-month experience using reprocessed ClosureFast radiofrequency cathetersJ Vasc Surg Venous Lymphat Disord20142115116
- TolvaVSCireniLVBianchiPGLombardoAKellerGCCasanaRMRadiofrequency ablation of the great saphenous vein with the ClosureFAST™ procedure: mid-term experience on 400 patients from a single centreSurg Today20134374174422932839
- NordonIMHinchliffeRJBrarRA prospective double-blind randomized controlled trial of radiofrequency versus laser treatment of the great saphenous vein in patients with varicose veinsAnn Surg201125487688121934487
- BisangUMeierTOEnzlerMThalhammerCHusmannMAmann-VestiBRResults of endovenous ClosureFast treatment for varicose veins in an outpatient settingPhlebology20122711812321572060
- ZunigaJMHingoraniAAscherEShort-term outcome analysis of radiofrequency ablation using ClosurePlus vs ClosureFast catheters in the treatment of incompetent great saphenous veinJ Vasc Surg2012551048105122386145
- RoosMTBorger van der BurgBLWeverJJPain perception during and after VNUS ClosureFAST™ procedurePhlebology20112620921221357621
- ShepherdACGohelMSBrownLCMetcalfeMJHamishMDaviesAHRandomized clinical trial of VNUS® ClosureFAST™ radiofrequency ablation versus laser for varicose veinsBr J Surg20109781081820473992
- AlmeidaJIKaufmanJGöckeritzORadiofrequency endovenous ClosureFAST versus laser ablation for the treatment of great saphenous reflux: a multicenter, single-blinded, randomized study (RECOVERY study)J Vasc Interv Radiol20092075275919395275
- DermodyMO’DonnellTFBalkEMComplications of endovenous ablation in randomized controlled trialsJ Vasc Surg Venous Lymphat Disord20131427436.e1
- HoldstockJMMarshPWhiteleyMSPriceBAIt is possible to cause damage to a laser fibre during delivery of tumescent anaesthesia for endovenous laser ablation (EVLA)Eur J Vasc Endovasc Surg20083647347618675563
- RudarakanchanaNBerlandTLChasinCSadekMKabnickLSArteriovenous fistula after endovenous ablation for varicose veinsJ Vasc Surg2012551492149422119247
- JacobsCEPinzonMMOrozcoJHuntPJRiveraAMcCarthyWDeep venous thrombosis after saphenous endovenous radiofrequency ablation: is it predictable?Ann Vasc Surg201428367968524211409
- SufianSArnezALabropoulosNLakhanpalSIncidence, progression, and risk factors for endovenous heat-induced thrombosis after radiofrequency ablationJ Vasc Surg Venous Lymphat Disord20131159164
- SadekMKabnickLSRockmanCBIncreasing ablation distance peripheral to the saphenofemoral junction may result in a diminished rate of endothermal heat-induced thrombosisJ Vasc Surg Venous Lymphat Disord20131257262
- Harlander-LockeMJimenezJCLawrencePFDerubertisBGRigbergDAGelabertHAEndovenous ablation with concomitant phlebectomy is a safe and effective method of treatment for symptomatic patients with axial reflux and large incompetent tributariesJ Vasc Surg20135816617223571079
- KuhlmannAPrenzlerAHackerJGraf von der SchulenburgJMImpact of radiofrequency ablation for patients with varicose veins on the budget of the German statutory health insurance systemHealth Econ Rev20133923551943
- CarrollCHummelSLeavissJClinical effectiveness and cost-effectiveness of minimally invasive techniques to manage varicose veins: a systematic review and economic evaluationHealth Technol Assess201317ixvi114124176098
- PerrinMEndovenous radiofrequency ablation of saphenous vein reflux. The VNUS Closureprocedure with ClosureFAST. An updated reviewInt Angiol20102930330720671647