
Abstract
Background
A postacute phase needs reliable routine screening instruments in order to identify the patients to be referred for a clinical interview with a psychologist. The aim of this study was to estimate the clinical cutoff scores of the anxiety and depression questionnaires and their clinical validity using a gold standard.
Methods
The study involved 177 patients with pulmonary, cardiac, or neurological disease undergoing in-hospital rehabilitation. Receiver operating characteristic curves were used to determine the best concordance between questionnaire’s scores and the gold standards.
Results
There was a significant difference (P<0.001) between clinically anxious and depressed patients and nonclinical subjects. The receiver operating characteristic curve for anxiety indicated that the best area under the curve for State Anxiety Inventory is obtained with a cutoff point of 21 for males and 25 for females; for depression scores, the highest area under the curve for Depression Questionnaire-Reduced Form is obtained with a cutoff point of six for males and eight for females.
Conclusion
Using appropriate cutoff values, the State Anxiety Inventory and Depression Questionnaire-Reduced Form allow psychologists to optimize early clinical intervention strategies selecting patients with significant needs.
Introduction
Many studies have established the presence of a high rate of psychological complaints among nonpsychiatric hospital patients.Citation1 Symptoms of anxiety and depression may confuse a patient’s clinical image, reduce compliance with therapeutic programs and affect the medium- or long-term outcomes pursued during the course of hospitalization,Citation2–Citation4 predict health-related quality of life,Citation5 and predict the influence of symptoms of anxiety and depression on medication noncompliance.Citation6,Citation7
The American Heart Association recently published a Science Advisory with the recommendation that patients with coronary heart disease (CHD) should be screened for depressive symptoms.Citation8–Citation10 Ziegelstein et alCitation11 maintain that for routine screening of CHD patients for depression to be recommended, screening tests must be sufficiently sensitive, specific, and validated, because cutoff scores used in primary care may not work equivalently in patients with CHD.Citation12 In a very recent review,Citation13 it is noted that there are few examples of screening tools with high sensitivity and specificity using an a priori defined cutoff score in >1 CHD sample.
Mild-to-moderate symptoms of anxiety and/or depression have also been observed in patients with chronic obstructive pulmonary disease (COPD) and current recommendations indicate that they should not be ignored. Appropriate outcome measures for mental health are needed for this patient population.Citation14 Similarly, depression and anxiety were significant for the outcomes regarding readmissions to hospital or death 6 months after a stroke. These are the reasons why clinicians need to identify specific patients with stroke with preexisting mental health conditions for which additional psychotherapy treatment may result in improved stroke outcomes.Citation15
A Cochrane reviewCitation16 indicated that psychological intervention in CHD patients did produce small to moderate improvements in depression and anxiety but there was no consistent evidence of a positive effect on health-related quality-of-life (HRQOL) or other psychological outcomes, including perceived stress, Type-A behavior, anger, and perceived exhaustion or Vital Exhaustion. All the aforementioned reasons and results support our search for clinical level of anxiety or depression in a rehabilitation setting and that both will be specific to the medical conditions of the patients concerned.
The aim of this study was to use receiver operating characteristic (ROC) curves to determine the best concordance between STAI-X3 and Depression Questionnaire-Reduced Form (acronym AD-R) scores using the opinion of a psychologist after a semi-structured clinical interview as gold standard.
Materials and methods
Patient population and data collection
The present observational study involved consecutively enrolled patients with pulmonary, cardiac, or neurological and neuromuscular disease undergoing in-hospital rehabilitation at the Salvatore Maugeri Foundation, IRCCS, Scientific Institute Division of Respiratory, Cardiac, and Neuromotor Rehabilitation during a period of 6 months in 2010. As a rule, the subjects completed the AD-R within the second to third day from the hospital admission. On the same day, a psychologist independently assessed their anxiety and depression status using a semistructured interviewCitation17,Citation18 and decided the appropriate psychological support needed. The psychologist was blinded to the AD-R scores. Exclusion criteria were as follows: the inability to complete questionnaires and a history of a severe psychiatric disease. The protocol was reviewed and approved by an internal review board for ethical protection of subjects (Comitato Tecnico Scientifico), and written informed consent of all the participants was obtained.
Measures
With the aim of making the screening process more rapid and accurate, we developed the ten-item version of the State Anxiety Inventory (STAI-X3)Citation19–Citation21 and the 15-item QD-R both with validated and reliable criteria (concurrent and predictive content).Citation22,Citation23 The reduced form of STAI-X3, consists of 10 items asking the subjects how they feel “right now” that are scored using a 4-point Likert scale (total score 10–40). The QD-R measures depressive symptoms and was originally constructed with reference to Diagnostic and Statistical Manual of Mental Disorders (DSM)-III and meets all of the DSM-IV RevisedCitation24 criteria for major depressive disorder (depressed mood; loss of interest or pleasure; variations in appetite and weight; insomnia/hypersomnia; psychomotor agitation/slowing; fatigability; self-depreciation; poor concentration; recurrent thoughts of death). For more details on the reduction methods, see Vidotto et al.Citation22 The two questionnaires in the reduced form take ~5 minutes to complete.
It simplifies screening of patients in hospital settings as it is suitable for subjects with mild/moderate or subclinical depression.Citation22,Citation23 The QD-R has 15 items, each consisting of a statement (eg, “The future looks very bleak”) to be answered “yes” or “no” (total score 0–15) and excludes somatic symptoms, thereby avoiding potential confounding by the somatic symptoms in hospitalized patients. The instructions ask that the questions should be answered “thinking about how you feel at this moment”, with the subject being asked to ponder the time span corresponding to that required to complete the survey.
Using Cronbach’s alpha score, the internal consistency of the QD-R is 0.77; any value between 0.7 and 0.8 is considered satisfactory for comparing groups.Citation25 STAI-X3 showed an internal consistency assessed with Cronbach’s alpha of 0.90 in healthy subjects.Citation20
Semistructured clinical interview: gold standard
In order to structure and maintain a single criterion for defining the gold standard, we used a “semistructured clinical interview” form based on and in respect of the DSM-IV anxiety and depression (DSM code 300.4) criteria. Inter-rater agreement with the psychological judgment for anxiety state (Cohen’s K =3.60; concordance 76%) and for depressive reaction (Cohen’s K =2.39; concordance =86%) has been found in a previously published study.Citation17 The “semistructured clinical interview” form is divided into three sections: anxiety, depression, and an area in which the diagnostic criteria for such disturbances overlap.
The interview began with a series of unstructured questions with the aim of establishing a cooperative relationship between the patient and the psychologist, and acquiring diagnostically useful information. At the end of the interview, the clinical psychologist had to judge whether the subject showed no anxiety/depression or one or both of these characteristics. If this was the case, the subject was invited to attend further sessions for clinical psychological support.
Statistical analysis
R software 3.3.0 (R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.; language and environment for statistical computing and graphics)Citation26 was used to analyze the data sample and analysis of variance to verify the significance of the differences in mean QD-R and STAI-X3 scores between males and females and between the disease groups. The construct validity of the AD-R schedule as a measure of depression and anxiety was assessed by examining the differences in mean value between the clinical groups as classified by the psychologist. Bonferroni’s correction was applied for the type I error inflation due to multiple comparisons.
ROC curves were used to identify the AD-R cutoff points. ROC analysis quantifies the accuracy of diagnostic tests (or further appraisal types) used to discriminate between two states or conditions. The discriminatory accuracy of a diagnostic test is quantified by its ability to suitably classify between subjects with and without disease.Citation27 A ROC plot displays the performance of a dichotomous classification procedure with continuous or discrete ordinal outcome. In the ROC space, the area under the curve (AUC) measures the performance of a classifying variable and is frequently applied for method comparison. A higher AUC means a better classification.Citation28 AUCs are computed with trapezoids.Citation29 In our case, ROC curves were used to identify the AD-R cutoff points. This technique is commonly used in medical decision-making research in order to determine how well a potential classifier discriminates two classes.Citation27–Citation32 In the context of this study, the potential classifying variables were the total AD-R scores, and the two classes were the binary classification of the presence/absence of the clinically relevant psychological variables (anxiety and depression).
The confidence intervals (CIs) were computed with bootstrap for AUCs.Citation33 The 95% CIs of the AD-R cutoff points and the sensitivity and specificity values were computed with bootstrap resampling (stratified manner), and the averaging methods described by Fawcett.Citation32 In all bootstrap CIs, the subjects were resampled and the modified curve was built before the statistics of interest were computed.
Results
One hundred and seventy-seven subjects (101 males and 76 females) completed the AD-R schedule and the interview with the psychologist at the beginning of their in-hospital rehabilitation period. and show their characteristics. The main pulmonary diseases were asthma, COPD, and respiratory failure; the main cardiac diseases were coronary artery disease (myocardial infarction, angina pectoris), congestive heart failure, and valvular heart disease; and the main neurological or neuromuscular diseases were stroke and myopathy.
Table 1 Characteristics of the diseases
Table 2 Characteristics of the sample
Comparing the three disease groups, no significant differences were found either for STAI-X3 scores (F(2,174)=0.252, P=0.778) or for QD-R scores (F(2,174))=0.186, P=0.830).
shows the distribution of the AD-R scores on the basis of the psychologist’s diagnosis of depression and anxiety. Based on the psychologist’s judgment, 53 subjects were “possible case for anxiety” (prevalence =29.9%) and 42 were “possible case for depression” (prevalence =23.7%). There was a significant difference in mean STAI-X3 scores between the subjects with and without clinically relevant anxiety (t(175)=14.813, P<0.001), and in mean QD-R scores between the subjects with and without clinically relevant depression (t(175)=12.864, P<0.001).
Table 3 Construct validity of the AD-Rschedule
Cutoff scores
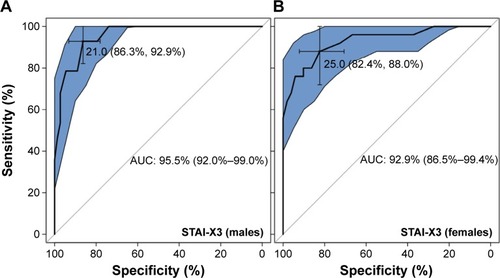
The best AUC for STAI-X3 was obtained with a cutoff point of 21.0 for males and 25.0 for females (). CI of AUC for STAI-X3 sample of males (equal to 95.5%) was 92.0%–99.0%, whereas CI of AUC for STAI-X3 sample of females (equal to 92.9%) was 86.5%–99.4%.
Figure 1 ROC curves and cut-off scores for STAI-X3.
Abbreviations: AUC, area under the curve; ROC, receiver operating characteristic; STAI-X3, state anxiety inventory.
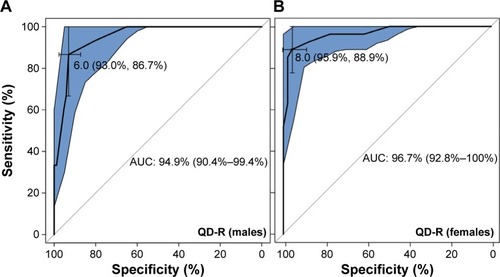
The best AUC for QD-R was obtained with a cutoff point of 6.0 for males and 8.0 for females (). CI of AUC for QD-R sample of males (equal to 94.9%) was 90.4%–99.4%, whereas CI of AUC for QD-R sample of females (equal to 96.7%) was 92.8%–100.0%.
Figure 2 ROC curves and cut-off scores for QD-R.
Abbreviations: AUC, area under the curve; QD-R, questionnaire depression-reduced; ROC, receiver operating characteristic.
shows the CIs of cutoff points of STAI-X3 and QD-R in male and female samples. The table also shows the sensitivity, specificity, positive predictive value (what is the probability that the disease is present when the test is positive) and negative predictive value (what is the probability that the disease is not present when the test is negative), positive likelihood ratio (what is the ratio between the probability of a positive test result given the presence of the disease and the probability of a positive test result given the absence of the disease) and negative likelihood ratio (what is the ratio between the probability of a negative test result given the presence of the disease and the probability of a negative test result given the absence of the disease); 95% CIs for each index are also reported.
Table 4 The CI of cutoff points of STAI-X3 and QD-R on the basis of the ROC method in relation to the clinical judgment expressed by the psychologist after the semistructured interview
The difference between sexes in STAI-X3 scores was not significant (t(175)= −0.952, P=0.342), whereas female showed higher (t(175)=−2.415, P=0.017) QD-R scores (5.51±3.4) than male (4.37±3.2). The bootstrap test for ROCs (2,000 resampling) indicates that the differences between curves for males and females were not significant both for STAI X-3 (D =0.679, P-value =0.497), and QD-R (D =0.356, P-value =0.721).
Discussion
Granted that assessing depression and anxiety in patients undergoing rehabilitation in a hospital is of major importance, it is necessary to devise an efficient way of completing such assessments.Citation34–Citation38 In this study, we searched the cutoff score of the STAI-X3 and QD-R not referring particularly to the specific disease (ie, CHD, COPD), but to the hospitalized condition in general, considering that DSM criteria suggest to pay attention to symptoms that are clearly due to a general medical condition, not to a specific medical condition.Citation24 When identifying a cutoff score for a routine screening, we also found that the QD-R was sensible and specific for a clinically relevant state of depression worthy of a deeper psychological examination, not to identify a major depressive disorder to be treated with antidepressants. This avoids the risk suggested by some authorsCitation11 that antidepressant medications may be initiated merely based on a positive depression screen.
From a clinical perspective, our findings support the use of AD-R cutoff scores as a means of screening psychological status in rehabilitation and hospital settings. Additionally, there were no differences between the disease groups. This would allow the multidisciplinary team to devise therapeutic interventions designed to improve both physical and psychological symptoms across disease conditions, which may be the best method to optimize functioning.Citation39–Citation44
The AD-R schedule is clearly subdivided in a solid measure of anxiety and another of depression, with different scores and cutoff points. Some questionnaires measuring depression focus narrowly on anhedonia, defined as a reduced ability to experience pleasure; it is too much to expect that ill patients will discriminate the intended meaning from their experience of not wanting to engage in previously pleasurable activities because of pain, fatigue, and other physical impairment.Citation45
The use of ROC curves provide information concerning AD-R cutoff values, which allow psychologists to optimize early clinical interventions during rehabilitation or in the provision of secondary prevention by identifying a clinically relevant state of depression and/or anxiety worthy of a deeper examination. In our sample, we found a STAI-X3 cutoff point of 21 for males and 25 for females. This means that a score ≥21 for males and ≥25 for females is indicative of a clinical level of anxiety that needs to be evaluated further by a psychologist. For QD-R, we found a cutoff point of 6 for males and 8 for females. This means that a score ≥6 for males and $8 for females is indicative of a critical mood level suggestive of a level of depression that requires a more complete evaluation by a psychologist.
Regarding construct validity, we found higher cutoff scores in females compared to males, as has been reported.Citation23 These results may be due to sex differences in illness perception: females, compared to males, are more likely to attribute cardiovascular disease (CVD) to causes beyond their control and perceive CVD as a chronic, untreatable condition.Citation46 Screening, especially for depression, is strongly recommended even in primary care.Citation47 Furthermore, in our previous paper, QD-R scores significantly correlated with meters walked in the 6-m walking test by 252 patients during cardiovascular rehabilitation, and patients with QD-R scores ranging from 0 to 5 showed a progressive reduction in the total distance walked during the test. In that study, a fall in walking distance corresponded to a value of 6 in the depression score as measured by QD-R.Citation14 Further research could be performed to observe the trend of functional performance along clinical cutoff points and to evaluate the effectiveness of integrated and multidisciplinary stepped care,Citation48,Citation49 and studies with hospitalized subjects.Citation50–Citation53
Limitations
We collected a sample from a single hospital; our results essentially describe what was found in the sample, but the extent to which those results might generalize beyond the center where the study was conducted is unknown. We also studied patients with pulmonary, cardiac, or neurological and neuromuscular diseases with very heterogeneous characteristics. However, this situation reproduces the proportion of patients usually followed by a psychologist during the rehabilitation phase in our institute. Further study with a larger sample and with different diseases would be required to test the validity of the AD-R cutoff scores for the screening of hospitalized patients that need a specific psychological support.
Conclusion
Using these cutoff values, the STAI-X3 and QD-R allow psychologists to optimize early clinical intervention strategies.
Acknowledgments
The authors wish to thank and acknowledge Alessandra Ianni for her help in collecting and organizing the data set. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
- GilbodySMHouseAOSheldonTARoutinely administered questionnaires for depression and anxiety: systematic reviewBMJ2001322728340640911179161
- BaladyGJAdesPAComossPCore components of cardiac rehabilitation/secondary prevention programs: a statement for health-care professionals from the American Heart Association and the American Association of Cardiovascular and Pulmonary Rehabilitation Writing GroupCirculation200010291069107310961975
- British Thoracic Society Standards of Care Subcommittee on Pulmonary RehabilitationPulmonary rehabilitationThorax2001561182783411641505
- PoolerABeechRExamining the relationship between anxiety and depression and exacerbations of COPD which result in hospital admission: a systematic reviewInt J Chron Obstruct Pulmon Dis2014931533024729698
- BlakemoreADickensCGuthrieEDepression and anxiety predict health-related quality of life in chronic obstructive pulmonary disease: systematic review and meta-analysisInt J Chron Obstruct Pulmon Dis2014950151224876770
- SundbomLTBingeforsKThe influence of symptoms of anxiety and depression on medication nonadherence and its causes: a population based survey of prescription drug users in SwedenPatient Prefer Adherence2013780581123983459
- DiMatteoMRLepperHSCroghanTWDepression is a risk factor for non-compliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherenceArch Intern Med2000160142101210710904452
- LichtmanJHBiggerJTJrBlumenthalJAAHA science advisory. Depression and coronary heart disease. Recommendations for screening, referral, and treatment. A science advisory from the American Heart Association Prevention Committee to the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care Outcomes Research. Endorsed by the American Psychiatric AssociationProg Cardiovasc Nurs2009241192619261139
- GallagherRTrotterRDonoghueJPreprocedural concerns and anxiety assessment in patients undergoing coronary angiography and percutaneous coronary interventionsEur J Cardiovasc Nurs201091384419846343
- IguchiASenjyuHHayashiYRelationship between depression in patients with chronic obstructive pulmonary disease and the percent predicted FEV1, BODE index, and health-related QOLRespir Care201358233433922782453
- ZiegelsteinRCThombsBDCoyneJCde JongePRoutine screening for depression in patients with coronary heart disease never mindJ Am Coll Cardiol2009541088689019712796
- WilliamsJWJrPignoneMRamirezGPerez StellatoCIdentifying depression in primary care: a literature synthesis of case-finding instrumentsGen Hosp Psychiatry200224422523712100833
- ThombsBDRosemanMCoyneJCDoes Evidence Support the American Heart Association’s recommendation to screen patients for depression in cardiovascular care? An updated systematic reviewPLoS One201381e5265423308116
- CafarellaPAEffingTWUsmaniZAFrithPATreatments for anxiety and depression in patients with chronic obstructive pulmonary disease: a literature reviewRespirology201217462763822309179
- DossaAGlickmanMEBerlowitzDAssociation between mental health conditions and rehospitalization, mortality, and functional outcomes in patients with stroke following inpatient rehabilitationBMC Health Serv Res20111131122085779
- WhalleyBReesKDaviesPPsychological interventions for coronary heart diseaseCochrane Database Syst Rev20118CD00290221833943
- ZottiAMBertolottiGMichielinPSanavioEVidottoG– CBA-H. Cognitive Behavioural Assessment forma Hospital. ManualeFirenzeGiunti OS2010
- VedanaLBaiardiPSommarugaMClinical validation of an anxiety and depression screening test for intensive in-hospital rehabilitationMonaldi Arch Chest Dis200258210110612418422
- SpielbergerCDGorsuchRLLusheneRManual for the State-Trait Anxiety InventoryPalo Alto, CAConsulting Psychologists Press1983
- BertolottiGMichielinPSanavioEVidottoGZottiAMA computerized approach to cognitive behavioral assessment: an introduction to CBA-2.0 primary scalesJ Behav Ther Exp Psychiatry199021121272197296
- VidottoGBertolottiGUna valutazione base dell’ansia di stato. La versione ridotta dello STAI X-1. [A basic assessment of state anxiety. The STAI X – 1 reduced version]Bollettino Psicologia Applicata19911983340
- VidottoGMoroniLBurroRA revised short version of the depression questionnaireEur J Cardiovasc Prev Rehabil201017218719720215970
- MoroniLBettinardiOVidottoGAnxiety and Depression Short Scale: norms for its use in rehabilitationMonaldi Arch Chest Dis200666425526317312844
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders4th-edWashington, D.CAmerican Psychiatric Press2000
- BlandJMAltmanDGStatistics notes. Cronbach’s alphaBMJ199731470805729055718
- R Core TeamR: A Language and Environment for Statistical ComputingVienna, AustriaR Foundation for Statistical Computing2016 Available from: http://www.R-project.org/Accessed April 5, 2016
- PepeMSThe Statistical Evaluation of Medical Tests for Classification and PredictionNew YorkOxford University Press2003
- HanczarBHuaJSimaCWeinsteinJBittnerMDoughertyERSmall-sample precision of ROC-related estimatesBioinformatics201026682283020130029
- ZweigMHCampbellGReceiver-operating characteristic (ROC) plots: a fundamental evaluation tool in clinical medicineClin Chem19933945615778472349
- BartfayEBartfayWJAccuracy assessment of prediction in patient outcomesJ Eval Clin Pract200814111018211637
- LindenAMeasuring diagnostic and predictive accuracy in disease management: an introduction to receiver operating characteristic (ROC) analysisJ Eval Clin Pract200612213213916579821
- FawcettTAn introduction to ROC analysisPattern Recogn Lett200627861874
- CarpenterJBithellJBootstrap confidence intervals: when, which, what? A practical guide for medical statisticiansStat Med20001991141116410797513
- LouPZhuYChenPPrevalence and correlations with depression, anxiety, and other features in outpatients with chronic obstructive pulmonary disease in China: a cross-sectional case control studyBMC Pulm Med2012125322958576
- KamphuisMHKalmijnSTijhuisMADepressive symptoms as risk factor of cardiovascular mortality in older European men: the Finland, Italy and Netherlands Elderly (FINE) studyEur J Cardiovasc Prev Rehabil200613219920616575273
- SchroederVBornerUGutknechtSSchmidJPSanerHKohlerHPRelation of depression to various markers of coagulation and fibrinolysis in patients with and without coronary artery diseaseEur J Cardiovasc Prev Rehabil200714678278718043299
- Putman-CasdorphHMcCroneSChronic obstructive pulmonary disease, anxiety, and depression: state of the scienceHeart Lung2009381344719150529
- CoventryPAGemmellIToddCJPsychosocial risk factors for hospital readmission in COPD patients on early discharge services: a cohort studyBMC Pulm Med2011114922054636
- MurphyBMElliottPCHigginsROAnxiety and depression after coronary artery bypass graft surgery: most get better, some get worseEur J Cardiovasc Prev Rehabil200815443444018677168
- GaryRADunbarSBHigginsMKMusselmanDLSmithALCombined exercise and cognitive behavioral therapy improves outcomes in patients with heart failureJ Psychosom Res201069211913120624510
- FreedlandKESkalaJACarneyRMTreatment of depression after coronary artery bypass surgery: a randomized controlled trialArch Gen Psychiatry200966438739619349308
- TselebisAPachiAIliasIKosmasEBratisDMoussasGTzanakisNStrategies to improve anxiety and depression in patients with COPD: a mental health perspectiveNeuropsychiatr Dis Treat20161229732810.2147/NDT.S7935426929625
- HynninenMJBjerkeNPallesenSBakkePSNordhusIHA randomized controlled trial of cognitive behavioral therapy for anxiety and depression in COPDRespir Med2010104798699420346640
- BravermanDLCardiac rehabilitation: a contemporary reviewAm J Phys Med Rehabil201190759961121765277
- CoyneJCvan SonderenENo further research needed: abandoning the Hospital and Anxiety Depression Scale (HADS)J Psychosom Res201272317317422325694
- GraceSLKrepostmanSBrooksDIllness perceptions among cardiac patients: relation to depressive symptomatology and sexJ Psychosom Res200559315316016198188
- ReynoldsCF3rdFrankEUS Preventive Services Task Force Recommendation statement on screening for depression in adults: Not good enoughJAMA Psychiatry201673318919026815331
- PanagiotiMScottCBlakemoreACoventryPAOverview of the prevalence, impact, and management of depression and anxiety in chronic obstructive pulmonary diseaseInt J Chron Obstruct Pulmon Dis201491289130625419126
- TselebisAPachiAIliasIStrategies to improve anxiety and depression in patients with COPD: a mental health perspectiveNeuropsychiatr Dis Treat20161229732826929625
- WuYSLinPYChienCYAnxiety and depression in patients with head and neck cancer: 6-month follow-up studyNeuropsychiatr Dis Treat2016121029103627175080
- NovickDMontgomeryWAguadoJPengXHaroJMImpact of anxiety symptoms on outcomes of depression: an observational study in Asian patientsNeuropsychiatr Dis Treat20161279580027114710
- YanartasOKaniHTBicakciEThe effects of psychiatric treatment on depression, anxiety, quality of life, and sexual dysfunction in patients with inflammatory bowel diseaseNeuropsychiatr Dis Treat20161267368327069364
- GerezMSuárezESerranoCCastanedoLTelloAThe crossroads of anxiety: distinct neurophysiological maps for different symptomatic groupsNeuropsychiatr Dis Treat20161215917526848265