
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objective
The purposes of this study are 1) to estimate the prevalence of common mental disorders including depressive disorder in patients with head and neck cancer (HNC) at baseline and at the 6-month follow-up and 2) to test the validity of two self-reported questionnaires, the Hospital Anxiety and Depression Scale (HADS) and the Taiwanese Depression Questionnaire (TDQ), for screening depression in patients with HNC.
Methods
Participants were recruited from the outpatient collaborative care clinic for HNC of a tertiary hospital in Taiwan between January 2010 and January 2011. Ninety-three patients with HNC were enrolled and assessed using the HADS, TDQ, and Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, fourth edition, Patient edition, at baseline and at the 6-month follow-up. Conventional validity indices of the HADS and TDQ were examined.
Results
Our results showed that the validity of the TDQ was satisfactory and comparable to that of both the HADS depression subscale and the HADS total scale. The cutoff scores of the HADS and TDQ for screening possible depressive disorders were 8 and 15, respectively. The areas under the receiver operating characteristic curve of the HADS and TDQ were mean 0.975±0.015 and 0.966±0.019, respectively. Thirteen participants (14%) were diagnosed with depressive disorders at the 6-month follow-up, compared with 8.5% at baseline.
Conclusion
Our results indicate that both the HADS and TDQ are valid instruments for screening depression in patients with HNC.
Introduction
Head and neck cancer (HNC) is the sixth most common cancer worldwide and was responsible for an estimated 300,000 deaths in 2008.Citation1 In the United States, ~52,610 incident cases of HNC were estimated to occur in 2012.Citation2 In Taiwan, oral cancer ranked as the fifth most common cause of cancer mortality in 2013 and was the fourth most common cause of cancer mortality among men.Citation3 The overall 5-year survival rate for patients with HNC is one of the lowest among different cancers, and this has not significantly changed during the last 2 decades.Citation4
Survival and quality of life are the main treatment goals for cancer patients. Previous studies have shown that patients with HNC are often comorbid with depressive disorders.Citation5 The reported prevalence of depressive symptoms in HNC patients varied from 9% to 52%, and depressive disorders were diagnosed in 3.7%–47% of patients.Citation5–Citation8 Depression in cancer patients is associated with poor quality of life and shorter survival time. Therefore, early screening to identify depression and the provision of effective treatment are crucial for holistic care of patients with HNC.
To date, most studies have used self-reported depression questionnaires to assess depression in cancer patients, but only a few studies have assessed depression using structured standardized clinical interviews as diagnostic instruments.Citation6 The main reasons for using self-administered depression rating scales in those studies might be that they are less time-consuming and less expensive for identifying depression in patients with cancer compared with standardized structured interviews. However, self-reported questionnaires are used for assessing “depressive symptoms” not “depressive disorder”, raising the concern of their validity for diagnosing depression.
The Hospital Anxiety and Depression Scale (HADS) was initially designed to assess the psychological distress of medically ill patients.Citation9 Previous studies have shown that the HADS is useful for screening psychiatric morbidity in cancer patients.Citation10,Citation11 The Mandarin version of the HADS was first used to detect depression in chronic headache patients and was found to have satisfactory validity.Citation12 This version of the HADS was later used for screening minor mental disorders in a cancer hospital in Taiwan and was reported to have fair sensitivity and specificity.Citation13 The validation of the Mandarin version of the HADS for detecting depression in patients with HNC has never been assessed.
We developed a culture-sensitive depression screening questionnaire, the “Taiwanese Depression Questionnaire” (TDQ).Citation14 The TDQ has shown its ability to screen depression in a community sample; it had a Cronbach’s α coefficient (internal consistency of reliability) of 0.90, and the area under the receiver operating characteristic curve (AUC) was 0.922. The 18-item TDQ had a sensitivity of 0.89 and a specificity of 0.92 at a cutoff point of 19.Citation14 These results suggested that the TDQ can be adapted for screening depression in the community. We also completed a study examining the validity of the TDQ for detecting depression in chronic pain patients, which resulted in a satisfactory validity index. At a cutoff point of 24, it achieved a sensitivity of 76.7%, specificity of 85.2%, positive predictive value (PPV) of 93.3%, negative predictive value (NPV) of 57.5%, efficiency of 79%, and AUC of 0.829.Citation15 During the last decade, the TDQ has been widely used as a screening instrument for the detection of depression in TaiwanCitation16–Citation18 and in Turkey.Citation19 The TDQ has been applied to assess depression at oncological services in recent years and had fair validity.Citation20 However, the validation of the TDQ to evaluate depression in patients with HNC has never been studied. Whether the HADS or TDQ can effectively detect depression in HNC patients should be further explored.
In addition, numerous somatic symptoms of depression overlap with those of cancer and the side effects of cancer treatments; thus, accurate detection of depression in these patients is difficult. Some studies have questioned the validity of the self-rated depression questionnaires in examining depression in medical patients, especially the somatic items of these rating scales.Citation21,Citation22 One study comparing the validity of the Beck Depression Inventory and TDQ for detecting depression in chronic pain patients found that two factors, the somatization tendency of patients and the somatic components of the questionnaires, influenced the validity of these questionnaires.Citation15 Whether the TDQ total score or its cognitive/affective component is valid for screening depression in cancer patients remains unknown.
The aims of this study included 1) estimating the prevalence of depressive disorders among patients with HNC at baseline and at the 6-month follow-up and 2) testing the validity of the TDQ and HADS in identifying depression among HNC patients. Furthermore, we investigated whether the somatic items of the TDQ influenced the validity of screening depression.
Methods
Participants
This study used a prospective design with consecutive sampling. Participants were recruited from the outpatient collaborative care clinic for HNC at a tertiary hospital from March 2010 to July 2011. This hospital has 2,754 beds with yearly services to 5,000 cancer patients in southern Taiwan. The inclusion criteria were as follows: 1) patients newly diagnosed with HNC and 2) patients with the ability to understand the study procedure and complete the questionnaires. Participants with dementia or delirium were excluded.
Assessments
Hospital Anxiety and Depression Scale
The HADS has been accepted as an effective screening instrument for anxiety and depression and has been extensively used in clinical settings and psycho-oncology research. The HADS is composed of two seven-item subscales, one specifically targeting anxiety (HADS-A) and the other focusing on depression (HADS-D).Citation9 The items excluded somatic symptoms and therefore avoided symptom overlap between somatic illnesses and mood disorders. Since both the HADS total scale (HADS-T) and the HADS depression subscale (HADS-D) can be used to detect depression, the validity of the HADS-T and HADS-D was analyzed separately.
Taiwanese Depression Questionnaire
The TDQ is a culture-sensitive self-reported instrument for screening depression in Taiwan.Citation14 This questionnaire is composed of 18 items related to mood, sleeping problems, appetite, energy, interest in normal activities, crying and feelings about the future, and so on. The participants were asked to indicate whether each item has been experienced and how frequently on a 4-point Likert scale (ranging from 0 to 3). The TDQ had satisfactory reliability and validity in a community study and among patients with chronic pain.Citation14,Citation15
Structured Clinical Interview for DSM-IV, Clinician Version
Psychiatric diagnoses were made using the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), Clinician Version (SCID-CV), a structured diagnostic interview based on DSM-IV criteria.Citation23 The SCID was designed to be administered by a clinician or mental health professional who has relevant professional training. The diagnosis was supplemented by the DSM-IV criteria for primary insomnia (which was not included in the SCID). The SCID interview by a trained psychiatrist is regarded as a gold standard of psychiatric diagnosis.
Procedures
Ethical approval was obtained from the human research ethics committee of Chang Gung Memorial Hospital. Study procedures were as follows: 1) newly diagnosed patients visiting our collaborative care clinic were invited consecutively to take part in this study. After explaining the study procedure and aims, those who agreed to sign the informed consent form were enrolled in the study; 2) psychiatric diagnoses were made by a senior psychiatrist (YL) using the SCID; 3) the HADS, TDQ, and clinical and demographic data were collected by a trained research assistant. Patients who were diagnosed with dementia or delirium were excluded. The earlier mentioned questionnaires and structured diagnostic interview were completed at baseline (pretreatment period), the 3-month follow-up, and the 6-month follow-up, respectively.
Statistical analyses
The differences in demographic data and clinical characteristics between participants with and without depressive disorders were tested by chi-square or student’s t-test, where appropriate. Cronbach’s α was applied to evaluate the internal consistency of the HADS and TDQ. The Cronbach’s α values of the HADS-T, HADS-D, and TDQ were 0.88, 0.75, and 0.84, respectively, suggesting that these questionnaires were acceptable and had good reliability in this study. The SCID interview results were used as the “gold standard” of psychiatric diagnosis against the TDQ or HADS. Sensitivity, specificity, PPV, NPV, and overall misclassification rate (OMR) were presented as indices used to demonstrate the validity of the HADS and TDQ. Receiver operating characteristic (ROC) curve analysis was performed to optimize the cutoff points for the HADS and TDQ. Patients were categorized as cases and noncases, based on the various cutoff scores, with a pair of sensitivity and specificity values for each cutoff score. Sensitivity was plotted against the false positive rate for every possible cutoff point, where the largest AUC was weighed to have the best validity.Citation24 A method developed by Hanley and McNeilCitation25 was utilized to assess whether there was a difference in the AUCs between the two questionnaires, to compare their validity. A critical ratio z was defined as:
(1) where A1 and SE1 were the observed area and the estimated standard error of the AUC of one questionnaire; A2 and SE2 were the corresponding values of the other questionnaire; and r was the estimated correlation between A1 and A2. All analyses were conducted using SPSS for Windows Version 16.0 (IBM, Armonk, New York). The significance level was set at P<0.05.
Results
Sample characteristics
A total of 119 patients were referred for the study; eleven declined to participate and two did not fulfill the inclusion criteria (one had recurrent cancer and the other had Alzheimer’s disease), resulting in 106 patients who completed baseline measures. The response rate was 89%. Those who declined to take part in the study included four who had privacy considerations and seven who lacked the time to complete the assessment. At the 6-month follow-up, three of the participants were deceased and ten were lost contact, resulting in 93 patients who completed the 6-month assessment. There was no statistically significant difference in sociodemographic data between these 93 participants and the 13 who lost follow-up. The follow-up rate was 87.7%.
Of the 93 patients who completed the 6-month assessment, 86% were male. The average age of the subjects was 52.7±9.5 years, and 26.9% were currently unemployed. Approximately 74.2% of the participants were married, and the mean educational level was 9.9±3.6 years. Sixty-five percentage of the patients had advanced (stages III and IV) disease. Approximately 63.4% and 41.9% of the participants had the habit of smoking cigarettes and drinking alcohol, respectively. There was no difference in demographic and clinical variables between the depressed and nondepressed participants ().
Table 1 Demographic and clinical characteristics of the depressive and nondepressive patients with head and neck cancer at the 6-month follow-up
At the baseline assessment, 54.7% of participants were diagnosed with a psychiatric disorder. At the first visit, adjustment disorder (19.8%) was the most prevalent psychiatric disorder, followed by alcohol use disorder (18.9%), depressive disorders (8.5%), anxiety disorders (7.5%), and primary insomnia (2.8%). However, at the 6-month follow-up, only 38.7% of the participants had a psychiatric disorder. The most prevalent psychiatric disorder at the 6-month follow-up was alcohol use disorder (20.4%), followed by depressive disorders (14%), primary insomnia (4.3%), anxiety disorders (2.2%), and adjustment disorder (1.1%). Major depressive disorder (12.9%) predominated among the depressive disorders, followed by depressive disorder not otherwise specified (1.1%). The proportion of major depressive disorder was 4.7% at the index evaluation, increasing to 9.6% at the 3-month follow-up and 12.9% at the 6-month follow-up. Approximately one-fifth of patients had adjustment disorder at baseline and this dropped to 1% at the 6-month follow-up ().
Table 2 Psychiatric diagnoses of patients with head and neck cancer at the first visit, the 3-month follow-up, and the 6-month follow-up
Optimal HADS-T, HADS-D, and TDQ cutoff scores and conventional validity index
To determine the optimal cutoff point to detect depression in HNC patients, we drew ROC curves based on various cutoff points for the TDQ (). The more the curve arched toward the upper left corner, the better the validity of the test in differentiating depression from nondepression. We found that 93.4% of the subjects were accurately classified at a cutoff point of 15. The AUC was 0.966±0.019 (margin of error, ). Using the same method, the optimal cutoff points of the HADS-T and HAD-D were 8 and 6, respectively. At these two points, 90.5% and 92.5% of the subjects were accurately classified. The AUCs of the HADS-T and HAD-D were 0.975±0.015 and 0.976±0.014, respectively ().
Figure 1 Receiver operating characteristic curve and optimal cutoff score for the TDQ, the HADS-T, and the HADS-D among patients with head and neck cancer.
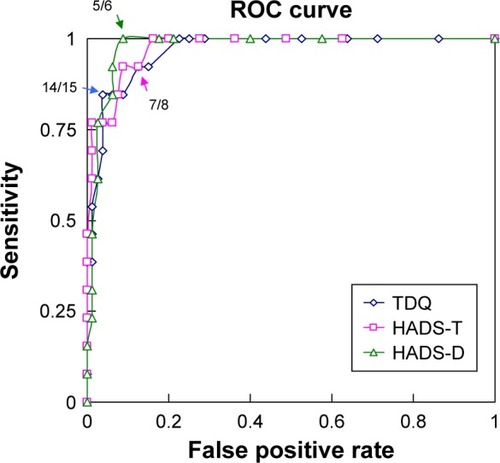
We obtained the sensitivity, specificity, PPV, NPV, and OMR of the TDQ, HADS-T, and HADS-D using ROC curve analysis at various cutoff points. The results showed that a cutoff point of 15 for the TDQ achieved a sensitivity of 84.6%, specificity of 96.2%, PPV of 78.6%, NPV of 96.3%, and OMR of 6.4% ().
Table 3 Sensitivity, specificity, positive and negative predictive values, and overall misclassification rate of the TDQ total scale and TDQ cognitive scale
For the HADS-T, a cutoff point of 8 achieved a sensitivity of 92.3%, specificity of 91.3%, PPV of 63.2%, NPV of 97.4%, and OMR of 9.5%. At the statistically obtained cutoff point of 6 for the HADS-D, sensitivity was 92.3%, specificity 93.8%, PPV 70.6%, NPV 97.4%, and OMR 7.5% (). The data suggested that the validity of the TDQ, HADS-T, and HADS-D was good and satisfactory.
Table 4 Sensitivity, specificity, positive and negative predictive values, and overall misclassification rate of the HADS total scale (HADS-T) and HADS depression subscale (HADS-D)
Comparison of the validity of the TDQ, HADS-T, and HADS-D
To test whether there was any difference in validity among the TDQ, HADS-T, and HADS-D, we did the following analyses using the method developed by Hanley and McNeil.Citation25 Upon comparison of the AUCs of the TDQ, HADS-T, and HADS-D, the AUCs were 0.966 (SE =0.018), 0.975 (SE =0.015), and 0.976 (SE =0.014) for the TDQ, HADS-T, and HADS-D, respectively. Our analysis showed that the AUC of the TDQ was very close to that of the HADS-D (z=0.655, P=0.257), indicating that the validity of the TDQ was comparable to that of the HADS-D in detecting depression in patients with HNC. We found that the AUCs of the TDQ and HADS-T were not significantly different (z=0.551, P=0.291). This result suggested that the validity of the TDQ and HADS-T was comparable. Also, the AUC of the HADS-T was very close to that of the HADS-D (z=0.117, P=0.453), implying that the validity of the HADS-T was comparable to that of the HADS-D.
Validity of the cognitive/affective subscales of the TDQ
To examine if the somatic items of the TDQ confounded its ability to identify depression in HNC patients, we performed additional ROC curve analyses of the cognitive/affective subscales of the TDQ.
The TDQ was divided into two subscales: cognitive/affective and somatic, as determined by factor analysis in our previous study.Citation15 For the cognitive component of the TDQ, the optimal TDQ cutoff point was 8, using ROC curve analysis. The AUC of the TDQ was 0.977±0.014 (margin of error). Ninety-two percent of subjects were accurately classified at a cutoff point of 8, which achieved a sensitivity of 92.3%, specificity of 93.8%, PPV of 70.6%, NPV of 96.2%, and OMR of 8.3% (). These data demonstrated that the validity of the cognitive/affective subscales of the TDQ was satisfactory.
Comparison of the validity of the total scale and cognitive/affective subscale of the TDQ
To examine whether removing the somatic items from the TDQ would affect its ability to identify depression, we compared the AUC of the TDQ with that of the cognitive/affective subscale of the TDQ using Hanley and McNeil’sCitation25 method. We found no significant difference between the AUC of the TDQ and the AUC of its cognitive/affective subscale (z=0.712, P=0.239). This result suggested that the somatic items did not significantly affect the validity of the TDQ in detecting depression in HNC patients.
Discussion
Our study suggested a high psychiatric morbidity among HNC patients from the initial pretreatment period to the post-treatment 6-month follow-up. The most prevalent psychiatric diagnosis of this study at baseline without cancer treatment was adjustment disorder (19.8%), followed by alcohol use disorder (18.9%) and depressive disorder (8.5%). This is partially supported by Kugaya’s report.Citation26 Kugaya et alCitation26 investigated psychiatric disorders in 107 consecutive patients with HNC by structured psychiatric interview before the initial cancer treatment. They found that 13.1% of patients had adjustment disorder, 3.7% had major depression, and 33.6% met the criteria for alcohol dependence.Citation26 The results of a meta-analysis of 66 studies conducted in oncological and hematological settings with 9,574 individuals across 14 countries were also in line with our results.Citation27 Mitchell et alCitation27 reported that a pooled prevalence of adjustment disorder and depression using DSM-IV criteria or International Classification of Diseases 10 was 19.4% and 16.3%, respectively. The small discrepancies between previous studies and ours may be attributed to differences in study populations, diagnostic criteria, cancer types and stages, or research instruments.
The morbidity of depressive disorders changed during the 6-month follow-up: the prevalence of depressive disorders in our study was 8.1% at the first visit, increasing to 24.5% at the 3-month follow-up, and dropping to 14% at the 6-month follow-up. Consistent with a previous review study, depression rates were particularly high at diagnosis, during treatment and even 6 years after treatment.Citation5 The clinical implication for this finding is that cancer patients may suffer from depressive disorder at any disease stage, especially at 3 months posttreatment. Therefore, clinicians should pay more attention to those who are susceptible to depression and render a prompt diagnosis and treatment to improve their quality of life and even prolong survival.
The prevalence of depressive disorders in our study was 14.0%, which is in line with that of previous hospital-based studies using standardized psychiatric interviews. To date, only five studies have used structured clinical interviews to estimate the prevalence of depressive disorder in patients with HNC; the prevalence in those studies ranged from 3.7% to 43%.Citation8,Citation26,Citation28–Citation30 Excluding one study that focused only on geriatric cancer patients,Citation30 the prevalence in the other four studies was 3.7%, 20%, 26.1%, and 43%, respectively. Our result is similar to the results of these four studies, implying that the prevalence of depressive disorder in HNC patients obtained by the structured clinical interview is lower than the prevalence in studies using self-rated depression scales, which ranges from 9% to 52%.Citation5,Citation6 Compared with those using structured clinical interviews, the strength of our study is that we recruited newly diagnosed HNC patients prospectively and consecutively, resulting in better generalization for clinical practice.
Our study demonstrated the efficacy of the Mandarin version of the HADS and TDQ as screening instruments for HNC patients, in terms of their good validity and AUC. The earlier mentioned results indicated that the validity of the TDQ, HADS-T, and HADS-D was good and comparable when used to identify depression in patients with HNC. The clinical implication of the satisfactory validity of earlier mentioned two self-reported questionnaires is the TDQ, a culture relevant instrument, as well as the HADS to detect depression in patients with HNC at Chinese oncological settings.
Previous Western country-based studies reported cutoff scores for the HADS-T that varied from to 8 to 20,Citation8,Citation31,Citation32 and cutoff scores for the HADS-D ranging between 5 and 8Citation11,Citation33 for detecting depression in cancer patients. Our results showed cutoff scores for the HADS-T and HADS-D of 8 and 6, respectively, which put the HADS-D within the range of prior reports, but the HADS-T at the lower limit of previous results. The possible explanation for our lower cutoff scores for the HADS-T is underreporting of depressive symptoms, possibly because the cancer patients were hesitant to admit depression so as to maintain a fighting spirit.Citation34
A recent cancer study on the validity of the HADS in Taiwan reported that cutoff points of 8 and 15 were optimal for the HADS-D and HADS-T, with sensitivities and specificities of 72% and 86% for the HADS-D and 84% and 68% for the HADS-T, respectively.Citation13 The cutoff scores in our study for both the HADS-D and HADS-T were lower than those in the earlier mentioned study. Possible explanations for this difference between the two studies are 1) the prior study focused on screening for psychological distress, but ours targeted depression, and 2) differences in subpopulations (cancer type and geographic regions) may have led to a higher prevalence of psychiatric morbidity in that study.Citation13 Nevertheless, the sensitivity and specificity of the HADS in these two studies were from 68% to 92%, which should be considered as suitable for identifying depression or psychological distress in cancer patients in Taiwan.
In a meta-analysis of the identification of depression in cancer patients, the HADS-T and HADS-D had a pooled sensitivity and specificity of 82.0% and 77.0%; 71.6% and 82.6%, respectively.Citation10,Citation31 In our results, the sensitivity and specificity of HADS-T and HADS-D were 92.3% and 91.3% and 92.3% and 93.8%, respectively. Our findings, along with those of previous studies, suggested that HADS is a fairly good screening tool for depression in cancer patients, no matter whether total score or depression subscore.
The TDQ effectively screened depression in patients with HNC and showed satisfactory sensitivity, specificity, PPV, NPV, and AUC (0.966). This result is as good as that in our previous community-based study testing the validity of the TDQ (AUC =0.92)Citation14 and is probably better than that in a previous validity study on detecting depression in chronic pain patients (AUC =0.829).Citation15 The validity indices are excellent, except the relatively low PPV. One should note that the PPV of a screening rating scale is dependent on the prevalence of the condition of interest, ie, PPV declines as prevalence decreases.Citation35 In our study, the prevalence of depressive disorders was <20%, which can account for the low PPV.
A previous study used the TDQ for screening depression in cancer inpatients and found that the AUC, sensitivity, specificity, PPV, NPV, and cutoff scores of the TDQ were 0.72, 71.9%, 56.4%, 32.9%, 90.4%, and 26, respectively.Citation20 Possible explanations for differences in the previous studies and our study are: 1) the previous study used the TDQ to screen for major depression and our study screened for all depressive disorders (including major depression, dysthymia, and depressive disorder NOS), which resulted in higher cutting scores in the previous study than in ours; 2) screening in the previous study was performed by several trained nursing staff members as a routine survey, and our study was administered by one trained research assistant, thereby avoiding inter-rater variations. This is a possible reason for our better validity index; and 3) the previous study included all cancer patients and ours enrolled only HNC patients.
The optimal, if not the best method for assessing depression in the medically ill, as well as in cancer patients, is still a subject of debate. Cancer patients frequently have somatic symptoms, including fatigue, insomnia, and poor appetite, which might influence the validity of self-administered depression questionnaires. Since the somatic items in the TDQ might confound the ability of these rating scales to detect depression in HNC patients, we examined the validity of the cognitive/affective component of this rating scale alone. After removing the somatic items, the validity index for the TDQ increased slightly, but not significantly, ie, the validity of the TDQ was not affected after removing the somatic items. Thus, the TDQ had good validity in its cognitive/affective component. A case–control study detected cognitive deficits in drug-free patients with major depressive disorderCitation36 using the TDQ and found that the cognitive subdomain of the TDQ was correlated with cognitive function. The aforementioned study supports the satisfactory validity of the cognitive aspect of the TDQ, suggesting that it may accurately assess depression in cancer patients. The increasing bodies of research have found that depression in cancer patients is related to several biological factors although the findings are mixed and inconsistent. Such biological correlates include chemotherapeutic agents, natural killer cells, gamma interferon-γ, cytokines (such as interleukin 2 [IL-2], IL-6), omega 3 fatty acid, and so on.Citation6,Citation37,Citation38 Besides detecting possible depression in patients with HNC, we should further focus on relevant biological factors for understanding pathophysiology, predicting prognosis, and seeking more effective treatment in the future.
The high response rate and the use of a structured clinical interview by a psychiatrist are the strengths of the present study. However, certain limitations should be noted when interpreting these data. First, our participants were recruited from a tertiary hospital, so our results may not be generalizable to other treatment settings. Second, the sample size in this study was relatively small. Large-scale studies should be used in the future to assess and confirm our results.
Conclusion
Our findings indicate that the HADS and TDQ have good validity for identifying depression among HNC patients. Further studies of other cancer types are required to confirm our findings.
Acknowledgments
This study was supported by a grant from Kaohsiung Chang Gung Memorial Hospital, Taiwan (CMRPG891321). We also acknowledge the excellent performance of our research assistant, PY Chao.
Disclosure
The authors report no conflicts of interest in this work.
References
- FerlayJShinHRBrayFFormanDMathersCParkinDMEstimates of worldwide burden of cancer in 2008: GLOBOCAN 2008Int J Cancer2010127122893291721351269
- TarverTCancer Facts & Figures 2012. American Cancer Society (ACS)J Consum Health Internet2012163366367
- Health Promotion AdministrationTaiwan cancer registry [Online]2013
- ChenYJChangJTLiaoCTHead and neck cancer in the betel quid chewing area: recent advances in molecular carcinogenesisCancer Sci20089981507151418754860
- Haisfield-WolfeMEMcGuireDBSoekenKGeiger-BrownJDe ForgeBRPrevalence and correlates of depression among patients with head and neck cancer: a systematic review of implications for researchOncol Nurs Forum2009363E107E12519403439
- ArcherJHutchisonIKorszunAMood and malignancy: head and neck cancer and depressionJ Oral Pathol Med200837525527018312300
- DuffySARonisDLValensteinMDepressive symptoms, smoking, drinking, and quality of life among head and neck cancer patientsPsychosomatics200748214214817329608
- KatzMRKopekNWaldronJDevinsGMTomlinsonGScreening for depression in head and neck cancerPsychooncology200413426928015054731
- ZigmondASSnaithRPThe hospital anxiety and depression scaleActa Psychiatr Scand19836763613706880820
- MitchellAJMeaderNSymondsPDiagnostic validity of the Hospital Anxiety and Depression Scale (HADS) in cancer and palliative settings: a meta-analysisJ Affect Disord2010126333534820207007
- ÖzalpESoygürHCankurtaranETurhanLAkbiyikDGeyikPPsychiatric morbidity and its screening in Turkish women with breast cancer: a comparison between the HADS and SCID testsPsychooncology200817766867517992701
- JuangKDWangSJLinCHFuhJLUse of the hospital anxiety and depression scale as a screening tool for patients with headacheZhonghua Yi Xue Za Zhi (Taipei)1999621174975510575802
- WangGLHsuSHFengACThe HADS and the DT for screening psychosocial distress of cancer patients in TaiwanPsychooncology201120663964621626611
- LeeYYangMJLaiTJChiuNMChauTTDevelopment of the Taiwanese Depression QuestionnaireChang Gung Med J2000231168869411190378
- LeeYLinPYHsuSTCing-ChiYYangLCWenJKComparing the use of the Taiwanese Depression Questionnaire and Beck Depression Inventory for screening depression in patients with chronic painChang Gung Med J200831436937718935795
- ChenKCYangYKLeeIHYehTLLuRBChenPSSexual dysfunction and physicians’ perception in medicated patients with major depression in TaiwanDepress Anxiety2008259E56E6217551923
- WangLJChenCKHsuSCLeeSYWangCSYehWYActive job, healthy job? Occupational stress and depression among hospital physicians in TaiwanInd Health201149217318421173533
- YenYCRebokGWYangMJLungFWA multilevel analysis of the influence of Apolipoprotein E genotypes on depressive symptoms in late-life moderated by the environmentProg Neuropsychopharmacol Biol Psychiatry200832247948617967500
- KursatSColakHBToramanAEkmekciCTekceHAliciTThe relationship between depression–malnutrition and echocardiographic-blood pressure parameters in chronic hemodialysis patientsInt Urol Nephrol200840379379918409016
- TuCHHsuMCChiSCLinHYYenYCRoutine depression screening and diagnosing strategy for cancer inpatientsPsychooncology20142391057106724798464
- GeisserMERothRSRobinsonMEAssessing depression among persons with chronic pain using the Center for Epidemiological Studies-Depression Scale and the Beck Depression Inventory: a comparative analysisClin J Pain19971321631709186024
- WesleyALGatchelRJPolatinPBKinneyRKMayerTGDifferentiation between somatic and cognitive/affective components in commonly used measurements of depression in patients with chronic low-back pain: let’s not mix apples and orangesSpine (Phila Pa 1976)1991166 supplS213S2151830701
- FirstMBSpitzerRLGibbonMWilliamsJBUser’s Guide for the Structured Clinical Interview for DSM-IV Axis I Disorders SCID-I: Clinician VersionArlington, VAAmerican Psychiatric Pub1997
- HsiaoJKBartkoJJPotterWZDiagnosing diagnoses: receiver operating characteristic methods and psychiatryArch Gen Psychiatry19894676646672735814
- HanleyJAMcNeilBJA method of comparing the areas under receiver operating characteristic curves derived from the same casesRadiology198314838398436878708
- KugayaAAkechiTOkuyamaTPrevalence, predictive factors, and screening for psychologic distress in patients with newly diagnosed head and neck cancerCancer200088122817282310870066
- MitchellAJChanMBhattiHPrevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studiesLancet Oncol201112216017421251875
- GilbertJHamanKLDietrichMSBlakelyRDSheltonRCMurphyBADepression in patients with head and neck cancer and a functional genetic polymorphism of the serotonin transporter geneHead Neck201234335936421604315
- McCaffreyJCWeitznerMKamboukasDHaselhuhnGLamondeLBooth-JonesMAlcoholism, depression, and abnormal cognition in head and neck cancer: a pilot studyOtolaryngol Head Neck Surg20071361929717210341
- MortonRPDaviesADBakerJBakerGAStellPMQuality of life in treated head and neck cancer patients: a preliminary reportClin Otolaryngol Allied Sci1984931811856488570
- BjellandIDahlAAHaugTTNeckelmannDThe validity of the Hospital Anxiety and Depression Scale: an updated literature reviewJ Psychosom Res2002522697711832252
- KugayaAAkechiTOkuyamaTOkamuraHUchitomiYScreening for psychological distress in Japanese cancer patientsJpn J Clin Oncol19982853333389703862
- LoveAWGrabschBClarkeDMBlochSKissaneDWScreening for depression in women with metastatic breast cancer: a comparison of the Beck Depression Inventory Short Form and the Hospital Anxiety and Depression ScaleAust N Z J Psychiatry200438752653115255825
- HollandJCBreitbartWSJacobsenPBLederbergMSLoscalzoMJMcCorkleRPsycho-OncologyOxfordOxford University Press2010
- TsuangMTTohenMGepZTextbook in Psychiatric EpidemiologyNew York, NYWiley1995229242
- HuengTTLeeIHGuogYJIs a patient – administered depression rating scale valid for detecting cognitive deficits in patients with major depressive disorder?Psychiatry Clin Neurosci2011651707621265938
- YangMMoonCNeurotoxicity of cancer chemotherapyNeural Regen Res20138171606161425206457
- SavardJVillaJIversHSimardSMorinCMPrevalence, natural course, and risk factors of insomnia comorbid with cancer over a 2-month periodJ Clin Oncol200927315233523919738124