
Abstract
Aim
Cognitive impairment is an important predictor of functional outcome in patients with attention deficit/hyperactivity disorder (ADHD). However, the neurophysiology of ADHD-related cognitive impairments remains unclear. Event-related potentials (ERPs) represent the noninvasive measurement of neural correlates of cognitive function. Mismatch negativity (MMN) is an ERP component that is presumed to index the preattentive monitoring of changes in the auditory environment.
Materials and methods
Previous studies have shown altered MMN amplitude and latency in patients with ADHD. However, little is known about the relationship between MMN and ADHD-symptom severity. To address this, we measured the amplitude and latency of MMN in ERPs and assessed correlations with the clinical severity of ADHD, as measured by the ADHD Rating Scale IV – Japanese version. Participants were 51 treatment-naïve children and adolescents with ADHD (mean age 10.42±3.35 years) and 15 normally developing age- and sex-matched children (mean age 11.8±3.36 years).
Results
In the ADHD group, MMN amplitudes were attenuated at the central electrode and MMN latencies prolonged at the parietal electrode (Pz) relative to those in the control group. Furthermore, MMN amplitudes at Pz were negatively correlated with ADHD full-scale and hyperactivity–impulsivity and inattention subscale scores, and MMN latency at Pz was positively correlated with ADHD hyperactivity–impulsivity subscale scores.
Conclusion
Our data suggest that MMN reflects the severity of ADHD symptoms in children and adolescents, and provides support for the use of ERPs in evaluating ADHD symptoms in patients.
Introduction
Attention deficit/hyperactivity disorder (ADHD) is a highly prevalent condition in children and adolescents that is characterized by inattention, hyperactivity, impulsivity, and abnormalities in one or more cognitive processes. With regard to cognitive abnormalities, children with ADHD have difficulties inhibiting responses, and consequently tend to make more errors. These deficits are similar to those reported for patients with frontal lobe lesions.Citation1,Citation2 Indeed, several neuroimaging studies have reported that deficits in inhibitory control are associated with structural and functional disorganization with respect to the connectivity between the basal ganglia and the prefrontal cortex (PFC) in individuals with ADHD.Citation3,Citation4
Event related potentials (ERPs) represent a sensitive, noninvasive reflection of covert brain activity. ERPs are obtained by measuring voltage fluctuations in electroencephalography (EEG) data, time-locked to an event of interest. The P300 is a well-characterized late-ERP component that has been implicated in various psychiatric disorders. It is thought to reflect executive and attentional function, including the updating of working memory, event categorization, and attentional reorientation.Citation5 Previous studies have reported that the P300 amplitude is lower in children with ADHD compared with control participants.Citation6–Citation9 In addition, several studies have reported that the latency of the P300 is longer in children with ADHD compared with controls.Citation9,Citation10 Previously, our group examined the P300 component in treatment-naïve children and adolescents with ADHD during an auditory oddball task, and found a positive correlation between ADHD-subscale rating and P300 amplitude at the central electrode (Cz), as well as P300 latency at the frontal electrode (Fz), Cz, and the parietal electrode (Pz).Citation11 These data suggest that the characteristics of P300 can be correlated with the severity of ADHD symptoms in patients. However, the P300 may reflect a late stage of the inhibitory process,Citation12 and is thus likely to be affected by preceding cognitive factors. For this reason, mismatch negativity (MMN), which is a pre-P300 component that provides an index of preattentive auditory sensory memory function, has become the focus of recent research. MMN is thought to reflect information processing more accurately than the P300, and is closely related to attention deficits. MMN is generated in response to occasional variations (eg, duration, frequency, intensity) in acoustic stimuli, and occurs about 100–200 ms after the onset of deviant stimulation, with peak amplitudes observed at the frontocentral leads.Citation13,Citation14 Additionally, MMN reflects an automatic cerebral discrimination process that is not under attentional control.Citation15 Several studies have demonstrated that methylphenidate, an ADHD medication, normalizes decreased MMN amplitudes in children with ADHD.Citation16 Correspondingly, Sawada et al reported a correlation between ADHD severity and MMN components in children with pervasive developmental disorder with ADHD-like symptoms.Citation17 However, no studies have directly examined whether MMN amplitude and latency vary according to the severity of ADHD symptoms in ADHD-only patients.
To address this, we evaluated the relationship between changes in MMN and the severity of ADHD symptoms in treatment-naïve children and adolescent patients with ADHD. We hypothesized that more severe ADHD symptoms would be associated with lower MMN amplitude and longer MMN latency. To our knowledge, our study is the first to investigate direct correlations among MMN amplitude, latency, and symptom severity in children and adolescents with ADHD.
Materials and methods
Participants
We recruited 51 patients with ADHD (41 boys, mean age 9.74±3.08 years, and ten girls, mean age 13.2±3.5 years) from the outpatient clinic at the Department of Psychiatry at Nara Medical University, Japan (). We recruited 15 healthy individuals (eleven boys, mean age 11.8±2.77 years, and four girls, mean age 11.8±3.77 years) as controls. We confirmed the absence of psychiatric illness in the control group using a standard clinical assessment that included a psychiatric evaluation and a structured diagnostic interview (Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) Axis Disorders Nonpatient Edition). This study was approved by the Institutional Review Board at Nara Medical University and carried out in accordance with the Declaration of Helsinki. All study participants or their legal guardians provided written informed consent for participation prior to initiation of the study.
Table 1 Participant characteristics
Patients were deemed eligible for inclusion if they had a diagnosis of ADHD according to the DSM-IV-Text Revision (DSM-IV-TR) as described in the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children – Present and Lifetime Version,Citation18 as evaluated by one or more experienced psychiatrists. Exclusion criteria were as follows: presence of a neurological disorder, head injury, serious medical condition, or history of substance abuse/dependence. A trained psychologist assessed intelligence using the Wechsler Intelligence Scale for Children, fourth edition, and participants with a full-scale intelligence quotient (FIQ) score below 70 were also excluded. None of the included participants had comorbid obsessive–compulsive disorder, major depressive disorder, schizophrenia, or epilepsy. Five patients had comorbid autism-spectrum disorder, one patient had comorbid tic disorder, and one patient had comorbid conduct disorder. All patients included were naïve to medical treatment.
Assessment of ADHD symptoms
We evaluated ADHD symptoms and symptom severity in all patients using the ADHD Rating Scale IV – Japanese version (ADHD-RS-IV-J) of the ADHD-RS-IV – home version.Citation19 The ADHD-RS-IV-J is an 18-item scale based on the DSM-IV-TR, and is reliable and easy to administer for the assessment of ADHD symptoms. Each statement on the ADHD-RS-IV-J is rated on a 4-point Likert scale (never or rarely, sometimes, often, or very often), and the scale yields an ADHD-RS-IV-J full (ARF) score, an ADHD-RS-IV-J inattention subscale (ARI) score, and an ADHD-RS-IV-J hyperactivity–impulsivity subscale (ARH) score, where higher scores represent more severe ADHD symptoms.
Measurement of ERPs
Based on guidelines for the measurement of evoked potentials, we elicited MMN components using an auditory oddball task.Citation20 We used a Multi Stim II auditory stimulus system (NEC, Tokyo, Japan) to present stimuli to both ears of the participants through headphones. Standard stimuli were 1,000 Hz tone bursts (P=0.9), and deviant stimuli were 1,100 Hz bursts (P=0.1). Stimuli were presented for 50 ms at 500 ms intervals and at 80 dB intensities. Frequent and infrequent stimuli were presented in a randomized fashion. MMN components were measured while participants read books or magazines of their choice. The participants were asked not to pay attention to the auditory stimuli.
Recording and analyses
ERPs were recorded with an MEB 2200 evoked potential-measuring system (Nihon Kohden, Tokyo, Japan). EEG readings were recorded at the Fz, Cz, Pz, C3, and C4 positions on the scalp using disk electrodes. All electrodes were re-referenced off-line to the average of two mastoid electrodes. Electrode impedance was set to ≤5 kΩ. MMN was analyzed between the 50 ms prestimulus and the 360 ms poststimulus. Artifact-free responses to stimuli were summated and averaged for EEG-amplitude data ≥100 μV. To reduce high-frequency content irrelevant to the components of interest, a digital 0.5–70 Hz band-pass filter (attenuation by 12 dB/octave) was applied to all data prior to analysis. Finally, data were corrected for eye-movement artifacts.Citation21
The duration of each auditory oddball task was 250 seconds, and infrequent and frequent stimuli were presented 50 and 450 times, respectively. The sample rate was 5,000 Hz. The 450 responses to frequent standard stimuli and the 50 responses to infrequent deviant stimuli were averaged separately, and a waveform was calculated as the difference between the averaged waveforms (frequent minus infrequent). The MMN was identified from the difference waveform as a negative wave with a peak latency between 100 ms and 250 ms, and its latency and amplitude were recorded. To prevent participants from habituating to the stimuli, each trial was conducted only once.
Statistical analyses
Statistical calculations were conducted with the assistance of PASW Statistics 18.0 J for Windows (SPSS, Chicago, IL, USA). Data are expressed as means ± standard deviation (SD). We calculated Spearman’s correlation coefficient (ρ) for the relationships between ADHD-RS-IV-J scores (including ARF, ARI, and ARH subscale scores) and electrophysiological variables. Bonferroni-adjusted P-values are reported. P-values <0.05 were considered to be statistically significant.
Results
Demographic data
Age, sex, FIQ, and ADHD-RS-IV-J scores, including ARF, ARI, and ARH subscale scores, are shown in . The participant groups did not differ in terms of mean age (t=−0.63, df=64; P=0.26), sex (χ2=0.01, df=1; P=0.97), or FIQ (t=−0.68, df=64; P=0.25). The mean ARF, ARH, and ARI subscale scores of patients with ADHD were 27.37 (SD 14.35, range 6–51), 11.57 (SD 8.13, range 0–26), and 15.8 (SD 7.59, range 2–27), respectively.
Comparison of MMN-component characteristics between patients with ADHD and control participants
Consistent with previous reports,Citation10,Citation22,Citation23 we found that the grand average of the MMN amplitude in the ADHD group was significantly smaller than that in the control group at Cz (t=−1.97, df=64; P<0.05). Also, we found that the grand average of the MMN latency in the ADHD group was significantly longer than that in the control group at Pz (t=−2.33, df=64; P<0.05) ( and ).
Figure 1 Mismatch negativity (MMN) grand-average waveforms from children and adolescents with attention deficit/hyperactivity disorder (ADHD) and healthy controls.
Abbreviations: Fz, frontal electrode; Cz, central electrode; Pz, parietal electrode.
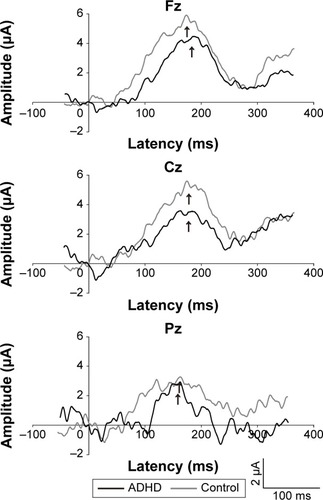
Table 2 MMN amplitudes and latencies
Correlation between MMN-component characteristics and ADHD-RS-IV-J subscale scores
We calculated Spearman correlation coefficients (with Bonferroni-adjusted P-values) for MMN amplitude and latency, as well as ADHD-RS-IV-J subscale scores ( and –). We identified negative correlations between the amplitude of MMN at Pz and ARF (ρ=−0.32, Bonferroni-corrected P<0.05), ARH (ρ=−0.322, Bonferroni-corrected P<0.05), and ARI (ρ=−0.295, Bonferroni-corrected P<0.05) scores. Furthermore, we found positive correlations between ARH scores and MMN latency at Pz (ρ=0.33, Bonferroni-corrected P<0.05).
Figure 2 Correlations between the mismatch negativity (MMN) component and ADHD Rating Scale IV – Japanese version full (ARF) scores.
Abbreviations: ADHD, attention deficit/hyperactivity disorder; Fz, frontal electrode; Cz, central electrode; Pz, parietal electrode; MMN, mismatch negativity; ARF, ADHD Rating Scale IV – Japanese version full.
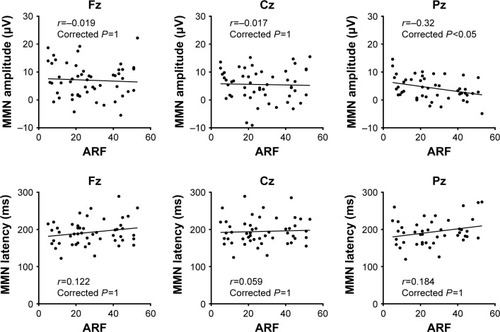
Figure 3 Correlations between the mismatch negativity (MMN) component and ADHD Rating Scale IV – Japanese version hyperactivity–impulsivity subscale scores.
Abbreviations: ADHD, attention deficit/hyperactivity disorder; ARH, ADHD Rating Scale IV – Japanese version hyperactivity–impulsivity subscale; Fz, frontal electrode; Cz, central electrode; Pz, parietal electrode; MMN, mismatch negativity.
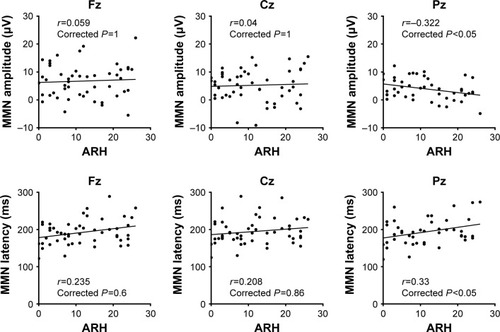
Figure 4 Correlations between the mismatch negativity (MMN) component and ADHD Rating Scale IV – Japanese version inattention subscale scores.
Abbreviations: ADHD, attention deficit/hyperactivity disorder; ARI, ADHD Rating Scale IV – Japanese version inattention-subscale; Fz, frontal electrode; Cz, central electrode; Pz, parietal electrode; MMN, mismatch negativity.

Table 3 Correlations between ERP components and ADHD-RS-IV-J scores
Discussion
To the best of our knowledge, this is the first study to investigate the relationship between MMN characteristics and the clinical severity of ADHD in treatment-naïve children and adolescents. As mentioned, MMN is produced in the frontal cortex in association with shifts in attention following the automatic detection of changes in stimuli by the auditory cortex.Citation24,Citation25 Accordingly, MMN is a preattentive ERP component. Indeed, MMN amplitudes have been suggested to reflect preattentive cognitive operations.Citation26 Previous studies have indicated that MMN has reduced amplitude and prolonged latency in children with ADHD relative to control participants.Citation10,Citation22,Citation23 MMN abnormalities have also been reported in several psychiatric disorders, including schizophrenia,Citation27 bipolar affective disorder,Citation28 and major depression.Citation29 Furthermore, MMN has been posited as an index of general cognitive decline in a broad spectrum of clinical disorders.Citation13 Our data are in agreement with these findings: in the present study, we observed that reductions in the MNN amplitude at Pz correlated with ADHD-symptom severity, as measured by the scores for all subscales of the ADHD-RS-IV-J. Additionally, the MMN latency at Pz was positively correlated with the severity of hyperactivity–impulsivity symptoms, suggesting that MMN latency may be a specific indicator of cognitive abnormality in children and adolescents with ADHD.
Neuropsychological theories of ADHD highlight the role of impaired frontal lobe function, especially in the PFC. Functional magnetic resonance imaging studies of patients with ADHD have indicated abnormal activity in the dorsolateral and ventrolateral PFC.Citation30,Citation31 These findings are consistent with the observation that working memory, which is thought to primarily involve the PFC, is a core cognitive function that is affected in individuals with ADHD.Citation32 On the other hand, patients with ADHD have been found to have increased activity in the parietal lobe,Citation33,Citation34 an area that plays a role in attention.Citation35 Our findings of significant correlations among MMN-component characteristics over the PFC and the clinical severity of ADHD symptoms emphasize the relevance of the PFC in ADHD.
In patients with schizophrenia, reports about a negative correlation between MMN amplitude and symptom severity have been inconsistent. However, MMN has been consistently associated with scores on the Global Assessment of Functioning scaleCitation25,Citation36,Citation37 and other measurements of social and occupational status.Citation38,Citation39 Sawada et al examined MMN components during an auditory oddball task in ten individuals with pervasive developmental disorder with ADHD symptoms.Citation17 They found that scores on the ADHD-RS-IV-J tended to be positively associated with MMN latency and were significantly and strongly negatively correlated with MMN amplitude. We found that lower MMN amplitude and prolonged MMN latency were correlated with the severity of subdomains of the ADHD-RS-IV-J (ie, the ARH). These findings indicate that MMN may be a common index of preattentive auditory sensory memory function in several psychiatric disorders, including ADHD.
There are some limitations that should be taken into consideration when interpreting our findings. First, our sample size was relatively small, and six patients with ADHD had comorbid psychiatric illnesses, including autism-spectrum disorder (n=4), tic disorder (n=1), and conduct disorder (n=1). Future studies using a larger cohort are needed to validate our findings and to determine whether MMN-component characteristics can distinguish patients with ADHD from those with other neurodevelopmental disorders. Second, since our study evaluated ADHD symptoms using only the ADHD-RS-IV-J, future studies employing other neuropsychological tests would be helpful in increasing the strength of our hypothesis. Third, the methods employed in our study did not allow a focus on altered patterns of connectivity. Recently, functional magnetic resonance imaging studies have produced evidence supporting the necessity of network integration during response inhibition, and have confirmed altered functional connectivity in individuals with ADHD.Citation40–Citation42 Fourth, the MMN baseline interval used in our study was short, which might have reduced the reliability of the signal. However, our group has taken ERP measurements using this method during several investigations of psychiatric disorders,Citation17,Citation43,Citation44 and these findings were consistent with those of our previous studies. Given these limitations, future studies should be conducted to determine whether abnormalities in the frontal lobe are resultant from or causative of altered functional connectivity.
Conclusion
The present study demonstrates that changes in MMN amplitude and latency can predict the severity of ADHD symptoms, and thus indicates that these may be important signals for the neurophysiological mechanisms underlying ADHD. Furthermore, our findings support the notion that ERPs represent a clinically useful and noninvasive method for estimating disease severity in children and adolescents with ADHD.
Author contributions
KY, TO, JI, YN, NK, and TK were involved in data collection and wrote the first draft of the manuscript. JI and TK supervised the entire project, were critically involved in study design, and contributed to the editing of the final manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
We wish to thank the study participants for their valuable contribution. The authors would also like to thank NEC for the NEC Multi Stim II equipment and their skilled technical and methodological support.
Disclosure
The authors report no conflicts of interest in this work.
References
- IaboniFDouglasVIBakerAGEffects of reward and response costs on inhibition in ADHD childrenJ Abnorm Psychol199510412322407897047
- TrommerBLHoeppnerJALorberRArmstrongKJThe go-no-go paradigm in attention deficit disorderAnn Neurol19882456106143202613
- CaseyBJCastellanosFXGieddJNImplication of right frontostriatal circuitry in response inhibition and attention-deficit/hyperactivity disorderJ Am Acad Child Adolesc Psychiatry19973633743839055518
- CastellanosFXToward a pathophysiology of attention-deficit/hyperactivity disorderClin Pediatr (Phila)19973673813939241475
- PolichJUpdating P300: an integrative theory of P3a and P3bClin Neurophysiol2007118102128214817573239
- FrankYSeidenJANapolitanoBEvent-related potentials to an “oddball” auditory paradigm in children with learning disabilities with or without attention deficit hyperactivity disorderClin Electroencephalogr19942541361417813092
- KutasMMcCarthyGDonchinEAugmenting mental chronometry: the P300 as a measure of stimulus evaluation timeScience19771974305792795887923
- MaglieroABashoreTRColesMGDonchinEOn the dependence of P300 latency on stimulus evaluation processesPsychophysiology19842121711866728983
- OzdagMFYorbikOUlasUHHamamciogluKVuralOEffect of methylphenidate on auditory event related potential in boys with attention deficit hyperactivity disorderInt J Pediatr Otorhinolaryngol200468101267127215364497
- WinsbergBGJavittDCSilipoGSDoneshkaPMismatch negativity in hyperactive children: effects of methylphenidatePsychopharmacol Bull19932922292338290670
- YamamuroKToyosakuOIidaJEvent related potentials correlate with the severity of child and adolescent patients with attention deficit/hyperactivity disorderNeuropsychobiology201673313113827055108
- NieuwenhuisSYeungNvan den WildenbergWRidderinkhofKRElectrophysiological correlates of anterior cingulate function in a go/no-go task: effects of response conflict and trial type frequencyCogn Affect Behav Neurosci200331172612822595
- NaatanenRKujalaTEsceraCThe mismatch negativity (MMN): a unique window to disturbed central auditory processing in ageing and different clinical conditionsClin Neurophysiol2012123342445822169062
- NäätänenRPaavilainenPRinneTAlhoKThe mismatch negativity (MMN) in basic research of central auditory processing: a reviewClin Neurophysiol2007118122544259017931964
- JonkmanLMKemnerCVerbatenMNEvent-related potentials and performance of attention-deficit hyperactivity disorder: children and normal controls in auditory and visual selective attention tasksBiol Psychiatry19974155956119046992
- SawadaMIidaJOtaTEffects of osmotic-release methylphenidate in attention-deficit/hyperactivity disorder as measured by event-related potentialsPsychiatry Clin Neurosci201064549149820923428
- SawadaMNegoroHIidaJKishimotoTPervasive developmental disorder with attention deficit hyperactivity disorder-like symptoms and mismatch negativityPsychiatry Clin Neurosci200862447948118778448
- KaufmanJBirmaherBBrentDSchedule for Affective Disorders and Schizophrenia for School-Age Children – Present and Lifetime Version (K-SADS-PL): initial reliability and validity dataJ Am Acad Child Adolesc Psychiatry19973679809889204677
- DuPaulGJPowerTGAnastopoulosADReidRADHD Rating Scale-IV: Checklists, Norms, and Clinical InterpretationNew YorkGuilford Press1998
- PictonTWBentinSBergPGuidelines for using human event-related potentials to study cognition: recording standards and publication criteriaPsychophysiology200037212715210731765
- GrattonGColesMGDonchinEA new method for off-line removal of ocular artifactElectroencephalogr Clin Neurophysiol19835544684846187540
- KemnerCVerbatenMNKoelegaHSEvent-related brain potentials in children with attention-deficit and hyperactivity disorder: effects of stimulus deviancy and task relevance in the visual and auditory modalityBiol Psychiatry19964065225348879473
- KilpelaäinenRPartanenJKarhuJReduced mismatch negativity (MMN) suggests deficits in pre-attentive auditory processing in distractible childrenNeuroreport199910163341334510599842
- JahshanCWynnJKBreitmeyerBGGreenMFNonconscious and conscious color priming in schizophreniaJ Psychiatr Res201246101312131722785333
- JahshanCCadenheadKSRisslingAJKiriharaKBraffDLLightGAAutomatic sensory information processing abnormalities across the illness course of schizophreniaPsychol Med2012421859721740622
- UmbrichtDKrljesSMismatch negativity in schizophrenia: a meta-analysisSchizophr Res200576112315927795
- PerezVBWoodsSWRoachBJAutomatic auditory processing deficits in schizophrenia and clinical high-risk patients: forecasting psychosis risk with mismatch negativityBiol Psychiatry201475645946924050720
- CattsSVShelleyAMWardPBBrain potential evidence for an auditory sensory memory deficit in schizophreniaAm J Psychiatry199515222132197840354
- UmbrichtDKollerRSchmidLHow specific are deficits in mismatch negativity generation to schizophrenia?Biol Psychiatry200353121120113112814863
- RubiaKOvermeyerSTaylorEHypofrontality in attention deficit hyperactivity disorder during higher-order motor control: a study with functional MRIAm J Psychiatry1999156689189610360128
- VaidyaCJAustinGKirkorianGSelective effects of methylphenidate in attention deficit hyperactivity disorder: a functional magnetic resonance studyProc Natl Acad Sci U S A1998952414494144999826728
- KoflerMJRapportMDBoldenJSarverDERaikerJSADHD and working memory: the impact of central executive deficits and exceeding storage/rehearsal capacity on observed inattentive behaviorJ Abnorm Child Psychol201038214916119787447
- SchweitzerJBFaberTLGraftonSTTuneLEHoffmanJMKiltsCDAlterations in the functional anatomy of working memory in adult attention deficit hyperactivity disorderAm J Psychiatry2000157227828010671402
- DurstonSTottenhamNTThomasKMDifferential patterns of striatal activation in young children with and without ADHDBiol Psychiatry2003531087187812742674
- PetersenSEPosnerMIThe attention system of the human brain: 20 years afterAnnu Rev Neurosci201235738922524787
- KiangMLightGAPrughJCoulsonSBraffDLKutasMCognitive, neurophysiological, and functional correlates of proverb interpretation abnormalities in schizophreniaJ Int Neuropsychol Soc200713465366317521483
- KawakuboYKasaiKSupport for an association between mismatch negativity and social functioning in schizophreniaProg Neuropsychopharmacol Biol Psychiatry20063071367136816603302
- RasserPESchallUToddJGray matter deficits, mismatch negativity, and outcomes in schizophreniaSchizophr Bull201137113114019561058
- WynnJKSugarCHoranWPKernRGreenMFMismatch negativity, social cognition, and functioning in schizophrenia patientsBiol Psychiatry2010671094094720074704
- FairDAPosnerJNagelBJAtypical default network connectivity in youth with attention-deficit/hyperactivity disorderBiol Psychiatry201068121084109120728873
- MennesMPotlerNVKellyCDi MartinoACastellanosFXMilhamMPResting state functional connectivity correlates of inhibitory control in children with attention-deficit/hyperactivity disorderFront Psychiatry201128322470352
- van RooijDHartmanCAMennesMAltered neural connectivity during response inhibition in adolescents with attention-deficit/hyperactivity disorder and their unaffected siblingsNeuroimage Clin2015732533525610797
- YamamuroKOtaTNakanishiYEvent-related potentials in drug-naive pediatric patients with obsessive-compulsive disorderPsychiatry Res2015230239439926410771
- YamamuroKOtaTIidaJEvent-related potentials reflect the efficacy of pharmaceutical treatments in children and adolescents with attention deficit/hyperactivity disorderPsychiatry Res201624228829427318633