Abstract
Schizoaffective disorder is characterized by the presence of symptoms of both schizophrenia and a major mood disorder. The coexistence of these symptoms can be difficult to manage, and these patients are generally treated with antipsychotics as well as mood stabilizers and/or antidepressants. Additionally, no established treatment guidelines exist for this disorder. This review describes the combined results of two international, double-blind, placebo-controlled clinical studies of paliperidone extended-release (ER), an atypical antipsychotic recently approved in the US for the treatment of schizoaffective disorder. Subjects in these six-week trials were aged 18–65 years, had a diagnosis of schizoaffective disorder based on the Structural Clinical Interview for DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th Edition) Disorders, and were experiencing an acute exacerbation. The subjects from these studies had significant symptomatology as evidenced by a mean (standard deviation) baseline Positive and Negative Syndrome Scale total score of 92.8 (13.0). Based on Young Mania Rating Scale and/or a 21-item Hamilton Rating Scale for Depression score of ≥16 at baseline, 79.5% and 66.9% of subjects presented with prominent manic and depressive symptoms, respectively, and 46.4% presented with mixed symptoms. Approximately half (45%) of subjects were taking adjunctive mood stabilizers and/or antidepressants. Paliperidone ER was found to be effective in improving psychotic and mood symptoms in these subjects. Paliperidone ER was also effective as monotherapy or adjunctive to mood stabilizers and/or antidepressants for subjects with prominent manic, depressive, or mixed symptoms at baseline. No new tolerability signals were observed in this population. To the best of our awareness, these pooled data provide the largest data set of patients with schizoaffective disorder, and extend our knowledge of disease characteristics and treatment response.
Introduction
The term “schizoaffective”, used to describe patients with concurrent schizophrenic and mood symptoms, was first introduced more than 75 years ago.Citation1 Diagnosis of schizoaffective disorder requires that patients experience an uninterrupted period of illness with concurrent psychotic and mood symptoms. The psychotic symptoms must be present without any prominent mood symptoms for at least two weeks, yet mood episodes must represent a substantial portion of the total duration of illness. Patients with schizoaffective disorder are further classified as having the bipolar or depressive type (Diagnostic and Statistical Manual of Mental Disorders, 4th Edition [DSM-IV]). Epidemiologic data suggest that schizoaffective disorder is about one third as common as schizophrenia, with a lifetime prevalence of 0.3%, compared with 0.9% for schizophrenia,Citation2 and such patients are regularly encountered in psychiatric clinic populations. A recent cross-national study found that nearly one third of a globally diverse population of patients with symptoms of psychosis who visited psychiatric settings had schizoaffective disorder.Citation3 However, when patients with mental illness are characterized by their need for inpatient psychiatric care, those with a diagnosis of schizophrenia and schizoaffective disorder are almost equally represented,Citation4 suggesting that patients with schizoaffective disorder may be more disabled by their illness and consume a disproportionately large share of available inpatient mental health resources.
Characteristics of the schizoaffective disorder population
Compared with the large number of clinical trials for the treatment of schizophrenia and mood disorders, fewer randomized studies have been conducted for schizoaffective disorder.Citation5–Citation10 As such, the demographic and clinical characteristics of the schizoaffective population are not fully understood. Cheniaux and coworkers have suggested that some aspects of schizoaffective disorder, such as the female-to-male gender ratio, age of illness onset, total number of episodes, deficits in cognition, and response to treatment, lie midrange in a spectrum between schizophrenia and mood disorders.Citation11 The number of hospitalizations and the number of suicide attempts, however, are higher among those with schizoaffective disorder than in those with either schizophrenia or mood disorder.Citation11
A study comparing patients with schizophrenia and patients with schizoaffective disorder (matched for intelligence quotient, education, length of illness, and attention span) found that those with schizoaffective disorder had a less marked negative syndrome and less social avoidance but higher levels of depression and guilt.Citation12 Patients with schizoaffective disorder were also more cognitively intact, had shorter inpatient stays, and had a higher prevalence of substance abuse in their families compared with those who had schizophrenia.Citation12 A recent analysis of a large Medicaid database found that patients with schizoaffective disorder were significantly younger, more likely to be female, and more likely to be white, Hispanic, or of other non-African American race or ethnicity compared with patients with schizophrenia.Citation13 Patients with schizoaffective disorder also were significantly more likely to receive concomitant treatment for substance use or for an anxiety, depressive, bipolar, or other mental disorder, and significantly more likely to be treated with mood stabilizers, antidepressants, and anxiolytics. Citation13 In addition to distinctions based on demographic and clinical characteristics, emerging molecular genetic analyses have suggested that schizoaffective disorder may have distinctive genetic risk factors compared with other psychiatric disorders.Citation14–Citation16
Treatment strategies
Coexistent psychotic and prominent affective symptoms can be difficult to address, and management is complicated by the variability in clinical presentations. A combination of medications and psychotherapy is typically required for these patients, yet there are no established treatment guidelines. Atypical antipsychotics have mood-stabilizing properties in addition to antipsychotic efficacy,Citation17–Citation19 and thus have the potential to be central in the pharmacologic treatment of schizoaffective disorder. Several small or open-label studies with risperidone in schizoaffective disorder have shown positive results.Citation7,Citation20–Citation22 A post hoc analysis of a schizoaffective subpopulation from a comparative study of olanzapine and haloperidol found greater benefits from olanzapine in measures of psychosis and depression, although more improvement was seen in those diagnosed with the bipolar type than the depressive type of illness.Citation23 Similarly, two additional post hoc analyses of subpopulations from placebo-controlled studies of ziprasidone and aripiprazole suggested that these agents were efficacious in patients with schizoaffective disorder.Citation24,Citation25
To manage the affective and psychotic symptoms, many patients with schizoaffective disorder also receive adjunctive treatment with mood stabilizers and/or antidepressants.Citation26–Citation28 A recent Medicaid prescription claims database found that approximately one half of those with schizoaffective disorder were prescribed an antipsychotic plus a mood stabilizer or an antipsychotic plus an antidepressant.Citation13 A study of hospitalized patients with schizoaffective disorder in the US determined that antipsychotics and mood stabilizers and/or antidepressants were prescribed together in 87% of cases.Citation28 A recent multinational study found that antipsychotics alone was prescribed for 33.9% of patients with schizoaffective disorder, whereas 23.1% were taking an antipsychotic plus a mood stabilizer, 27.7% were taking an antipsychotic plus an antidepressant, and 7.7% were taking an antipsychotic plus a mood stabilizer and an antidepressant.Citation3 However, the benefits and risks of atypical antipsychotics administered alone or in combination with other treatments have not been established.
Paliperidone extended-release for schizoaffective disorder
Two large, international, double-blind, placebo-controlled, randomized, six-week studies with paliperidone extended- release (ER) were conducted for schizoaffective disorder.Citation29,Citation30 Paliperidone ER is the first agent approved by the US Food and Drug Administration and several other countries (Australia, Brazil, New Zealand, and Philippines) to treat patients with schizoaffective disorder, both as monotherapy and as adjunctive therapy with mood stabilizers and/or antidepressants.Citation31 In contrast with other antipsychotics, paliperidone ER undergoes limited hepatic metabolism and is therefore less likely to cause hepatically mediated drug–drug interactions in patients receiving multiple medications.Citation32–Citation34 This review of pooled data from the combined studies covers the largest data set of patients with schizoaffective disorder from randomized controlled trials to date, and provides insights into the characteristics and treatment responses of this understudied population.
Description of the studies
Subjects in these studies were aged 18–65 years, with a diagnosis of schizoaffective disorder based on the Structured Clinical Interview for DSM-IV Disorders (SCID). All were experiencing an acute exacerbation of illness as evidenced by a Positive and Negative Syndrome Scale (PANSS)Citation35 total score ≥ 60 and a score ≥ 4 on at least two of the PANSS items for hostility, excitement, tension, uncooperativeness, and poor impulse control. Prominent mood symptoms were reflected in a score ≥ 16 on the Young Mania Rating Scale (YMRS)Citation36 and/or the 21-item Hamilton Rating Scale for Depression (HAM-D-21).Citation37 In the first study, subjects received fixed dosages of paliperidone ER, ie, either the higher dosage (12 mg/day, with the option to reduce to 9 mg/day) or the lower dosage (6 mg/day, with the option to reduce to 3 mg/ day).Citation29 In the second study, paliperidone ER was flexibly dosed, beginning at a dosage of 6 mg/day, with a range of 3 to 12 mg/day.Citation30 For both studies, any dosing changes had to occur within the first 15 days. Subjects receiving stable regimens of mood stabilizers and/or antidepressants were permitted to continue their ongoing treatment to allow the study of paliperidone ER either as monotherapy or as an adjunct to mood stabilizers and/or antidepressants.
Change in PANSS total score from baseline to endpoint was the primary outcome measure for both studies. Secondary efficacy measures were changes from baseline to endpoint for the Clinical Global Impressions of Severity for Schizoaffective Disorder (CGI-S-SCA),Citation38 PANSS factor scores,Citation39 a composite response (≥30% improvement in PANSS total score and Clinical Global Impressions of Change for Schizoaffective Disorder [CGI-C-SCA] of 1 or 2 [much or very much improved]), and the YMRS and HAM-D-21 scales. Safety assessments included adverse event reporting, clinical laboratory tests (including prolactin levels), and assessment of movement disorders with the Simpson-Angus Scale (SAS), Barnes Akathisia Scale (BAS), and Abnormal Involuntary Movement Scale (AIMS).Citation40–Citation42
Randomization for both studies was stratified by center and by treatment with concomitant medications (with or without mood stabilizers and/or antidepressants). Data from the two schizoaffective studies were integrated (paliperidone ER versus placebo) for all statistical analyses. Efficacy was analyzed using the intent-to-treat analysis set, which included all randomized subjects who received ≥1 dose of study medication and had a baseline and ≥1 postbaseline PANSS assessment. The safety population included randomized subjects who received ≥1 dose of study medication. For each continuous parameter, treatment group differences were analyzed using separate analysis-of-covariance (ANCOVA) models with treatment, protocol, country-within-protocol, concomitant medication stratum as fixed-effect design factors, and baseline score as a covariate. To assess consistency of treatment effect within each subgroup, separate ANCOVA models were fit. A Forest plot by subgroups was generated showing least-squares mean estimates and 95% confidence intervals (CIs) for pairwise differences between paliperidone ER and placebo at week 6 last-observation-carried- forward (LOCF) endpoint. Change from baseline in efficacy measures (observed case) was also analyzed using a repeated-measures mixed-effects linear model. This model included baseline PANSS total score as a covariate; treatment, protocol, country-within-protocol, concomitant medication stratum, and time (scheduled assessment visits on day 4 and at weeks 1, 2, 3, 4, and 6) as factors; and the interaction between time and treatment. The correlation of the repeated measures is modeled with an unstructured covariance matrix. Between-group differences in percentage of subjects who met the composite response were evaluated using Fisher’s exact test. Effect sizes were calculated using Cohen’s d methodology. Relative risks (RRs) and their corresponding 95% CIs were calculated for adverse events with ≥5% incidence for paliperidone ER or placebo. RR analyses were considered potentially significant (P = 0.05) when the 95% CIs did not include 1. No adjustments were made for multiplicity.
Population characteristics
A total of 627 randomized subjects were in the pooled analysis (). In the intent-to-treat analysis set (n = 614), 414 subjects received paliperidone ER and 200 received placebo. The mean (standard deviation [SD]) age of the combined population was 37.4 (9.9) years (). In contrast with the male-to-female ratio of patients with schizoaffective disorder in the literature, but typical of the ratio among subjects included in clinical studies, there were more male than female subjects. The majority (90.9%) of subjects had a chart diagnosis of schizoaffective disorder prior to screening, and more subjects were diagnosed with the bipolar type than the depressive type. The mean age at first schizoaffective disorder diagnosis was approximately six years later than the age at first psychiatric diagnosis, which was consistent with other observations that the diagnosis emerges over time.Citation43 Subjects had received various other previous diagnoses, with schizophrenia being the most common. Nearly one third of subjects had attempted suicide; one half of this group of subjects had made two or more suicide attempts. Mean baseline scores for the PANSS total, YMRS, and HAM-D-21 scales indicated that subjects had significant symptoms. Two hundred and seventy-five subjects (45%) were receiving adjunctive mood stabilizers and/or antidepressants at baseline and continued these medications during the study; 69% were taking a mood stabilizer, and 49% were taking an antidepressant. Valproic acid was the most frequently used mood stabilizer; the most frequently used antidepressants were escitalopram, sertraline, and venlafaxine (). Also, 14% of subjects in the total population were using medications for extrapyramidal symptoms, and 50% were using nonbenzodiazepine hypnotics and anxiolytics.
Figure 1 Study flow diagram.
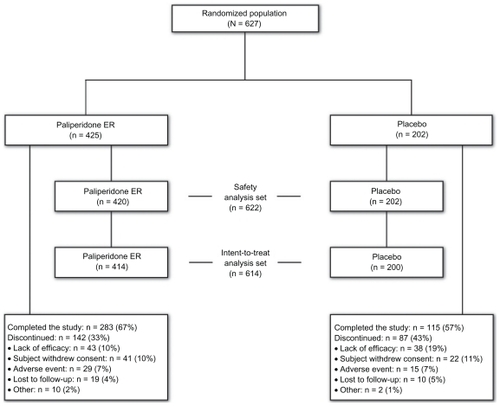
Table 1 Baseline demographics and clinical characteristics in two studies of paliperidone ER for schizoaffective disorder (intent-to-treat analysis set)
Table 2 Specific medications used by subjects in the adjunctive mood stabilizers and/or antidepressants group (n = 275)
The studies were designed to include dosages from 3 to 12 mg/day, based on the recommended dose range for schizophrenia.Citation31 The mean (SD) modal dosage of paliperidone ER in the combined studies was 8.6 (2.8) mg/day. Sixty-seven percent of subjects receiving paliperidone ER and 57% of those receiving placebo completed the study. The most common cause for discontinuation was lack of efficacy for 10% of the paliperidone ER subjects and 19% for the placebo subjects ().
Efficacy
The PANSS total score improved significantly more with paliperidone ER than with placebo from day 4 through to the study endpoint: placebo-adjusted least-squares mean (standard error) difference at LOCF endpoint (paliperidone ER minus placebo), −7.8 (1.7); P < 0.001 ( and ). The effect size was 0.41. Improvements on other measures, including the PANSS factor scores and CGI-S-SCA total and domain scores, were greater with paliperidone ER than with placebo (). Results using a repeated-measures linear model were consistent with those of the LOCF analysis (). Composite response rates were higher with paliperidone ER (50%) than with placebo (35%, P < 0.001, ).
Figure 2 Mean PANSS total score over time (intent-to-treat analysis set).
Abbreviations: ANCOVA, analysis-of-covariance; BL, baseline; ER, extended-release; LOCF, last-observation-carried-forward; PANSS, Positive and Negative Syndrome Scale; SE, standard error.
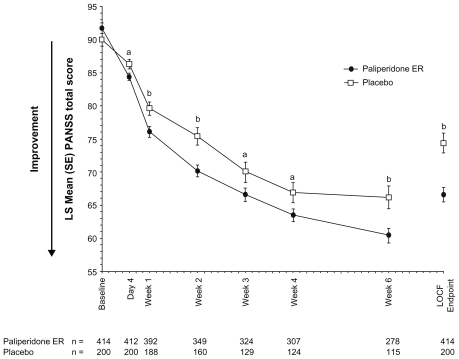
Figure 3 Adjusted mean differences and 95% CIs for PANSS total change scores at endpoint with paliperidone ER versus placebo (intent-to-treat analysis set).
Abbreviations: CI, confidence interval; ER, extended-release; HAM-D-21, 21-item Hamilton Rating Scale for Depression; LS, least-squares; MS/ADs, mood stabilizers/ antidepressants; PANSS, Positive and Negative Syndrome Scale; YMRS, Young Mania Rating Scale.
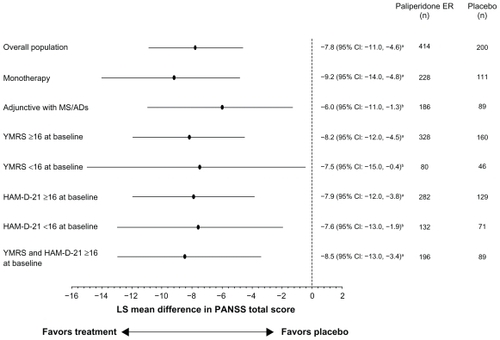
Figure 4 Composite clinical response ratea at endpoint in the overall population and by concomitant medication stratum (intent-to-treat analysis set).
Abbreviations: ER, extended-release; CGI-C-SCA, Clinical Global Impressions of Change for Schizoaffective Disorder; MS/AD, mood stabilizer/antidepressant.
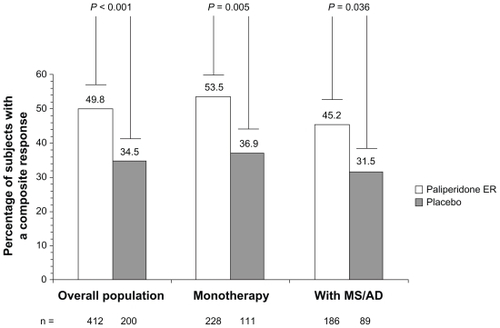
Table 3 Efficacy results for the pooled population (n = 614)Table Footnotea
Paliperidone ER alone or adjunctive to mood stabilizers and/or antidepressants
Approximately one half of the population was receiving mood stabilizers and/or antidepressants at baseline and continued these medications during the study, which allowed examination of the efficacy of paliperidone ER with or without mood stabilizers and/or antidepressants. Mean (SD) PANSS total scores at baseline were similar for subjects in both groups at 93.1 (13.0) for subjects receiving paliperidone ER as monotherapy and 93.5 (13.6) in those receiving paliperidone ER adjunctive to mood stabilizers and/or antidepressants. Improvement at the six-week endpoint was greater with paliperidone ER than with placebo in both groups ().
Subjects with prominent manic, depressive, or mixed symptoms
The size of the pooled population allowed for additional subgroup analyses based on the prominence of baseline affective symptoms (subjects with YMRS and/or HAM-D-21 score ≥ 16 at baseline). PANSS total scores improved significantly more with paliperidone ER than with placebo in each of these groups at endpoint ().
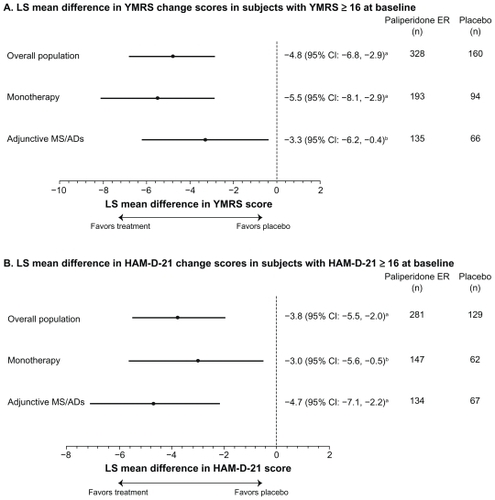
Further analyses of these subgroups examined the effect of paliperidone ER on mood symptoms. Improvements in YMRS and HAM-D-21 were greater with paliperidone ER than with placebo, as measured by placebo-adjusted least-squares mean (95% CI) changes from baseline of −4.8 (−6.8, −2.9) and −3.8 (−5.5, −2.0), respectively. Both YMRS and HAM-D-21 scores improved with paliperidone ER as monotherapy or as adjunctive therapy with mood stabilizers and/or antidepressants ().
Figure 5 Adjusted mean differences and 95% confidence intervals for total YMRS and HAM-D-21 change scores at endpoint with paliperidone ER versus placebo in patients with manic or depressive symptoms at baseline (intent-to-treat analysis set).
Abbreviations: CI, confidence interval; ER, extended-release; HAM-D-21, 21-item Hamilton Rating Scale for Depression; LS, least-squares; MS/ADs, mood stabilizers/ antidepressants; PANSS, Positive and Negative Syndrome Scale; YMRS, Young Mania Rating Scale.
Tolerability
The most frequent adverse events (≥5.0% in paliperidone ER subjects) among subjects receiving paliperidone ER versus placebo were headache (14.3% versus 14.9%), tremor (8.1% versus 3.5%), dizziness (6.7% versus 5.9%), insomnia (6.7% versus 6.9%), nausea (6.4% versus 5.9%), akathisia (5.5% versus 4.5%), hypertonia (5.5% versus 2.0%), dyspepsia (5.5% versus 2.5%), somnolence (5.2% versus 2.0%), and sedation (5.0% versus 3.5%). An analysis of RR found a greater risk of tremor with paliperidone ER than with placebo (RR = 2.34; 95% CI = 1.05, 5.18, ). Significance for increased risk (defined as the 95% CI not including 1) of the other adverse events was not observed.
Figure 6 Most frequent (in ≥ 5.0% of paliperidone ER subjects) adverse events sorted by relative risk (safety analysis set) by concomitant medication stratum.
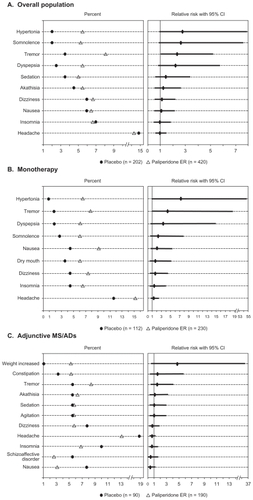
The overall adverse event rate was higher in subjects who received paliperidone ER as adjunctive therapy to mood stabilizers and/or antidepressants (70.4%, paliperidone ER; 70.0%, placebo) than in those who received paliperidone ER as monotherapy (60.5%, paliperidone ER; 49.1%, placebo). An analysis of RR found a greater risk of tremor with paliperidone ER than with placebo (RR = 4.38; 95% CI = 1.04, 18.56) in the monotherapy group (). Significance for increased risk of adverse events was not observed in the mood stabilizer and/or antidepressant group.
The percentage of discontinuations due to adverse events was similar for both the paliperidone ER- and the placebo-treated groups (each 7%) but was slightly higher in the group receiving paliperidone ER adjunctive to mood stabilizers and/or antidepressants (8.2%) than in the group receiving paliperidone ER as monotherapy (5.0%).
Adverse events of particular relevance with antipsychotic therapy are extrapyramidal symptoms, weight and metabolic changes, and prolactin elevation. Extrapyramidal symptoms were reported in 19.8% of subjects receiving paliperidone ER and in 10.9% of those receiving placebo. The severity of extrapyramidal symptoms as measured using the SAS, AIMS, and BAS was low (global score < 1) in both groups at baseline and endpoint.
At endpoint, mean (SD) changes in prolactin levels (ng/mL) were greater with paliperidone ER versus placebo for both males (12.6 [20.1] versus −3.6 [13.3]) and females (51.4 [62.1] versus −13.9 [32.4]). There were 9 (2.1%) subjects receiving paliperidone ER and one (0.5%) subject receiving placebo who experienced a potentially prolactin- related adverse event. The mean (SD) weight change was 1.0 (2.7) kg for paliperidone ER and 0.2 (2.1) kg for placebo. There were no clinically relevant differences in the lipid profile or fasting glucose levels for paliperidone ER compared with placebo.
Additionally, no clinically relevant differences were found in the incidence of extrapyramidal symptoms or in changes in mean weight, lipid profile, fasting glucose level, or prolactin level between subjects who received paliperidone ER as monotherapy and those who received paliperidone ER adjunctive to mood stabilizers and/or antidepressants ().
Table 4 Change in prolactin, lipid parameters, fasting glucose, and weight by concomitant medication stratum (safety analysis set)
Discussion
To our awareness, this review covers the largest data set of patients with schizoaffective disorder, and provides additional knowledge of patient characteristics and treatment responses to paliperidone ER. Although differential diagnosis across the psychosis and mood continuum can be challenging, over 90% of subjects carried a chart diagnosis of schizoaffective disorder prior to enrollment in the studies. Interestingly, the mean age at first schizoaffective disorder diagnosis was approximately six years later than the age at first psychiatric diagnosis. This is consistent with the longitudinal nature of the diagnosis, which requires assessment of the duration of mood symptoms relative to the total duration of illness, and suggests that full symptom expression emerges over time. All subjects’ diagnoses were confirmed by the Structured Clinical Interview for DSM-IV Disorders at study entry. Their mean age was approximately 37 years, with an average of six psychiatric hospitalizations per subject, and a previous suicide attempt reported in over 30% of subjects. These subjects were acutely ill at study entry and displayed high levels of concurrent psychotic, manic, and depressive symptoms. Notably, approximately one half of this population was receiving concomitant mood stabilizers and/or antidepressants at baseline.
The data presented here demonstrate that patients with schizoaffective disorder can be successfully treated with paliperidone ER. Although the mean modal dosage of paliperidone ER in these data was 8.6 mg/day, the recommended dosage for schizoaffective disorder is 6 mg/day, with a range of 3 to 12 mg/day. The dosing recommendation is supported by the study designs that utilize this range, and the majority of subjects randomized to paliperidone ER were initiated at 6 mg/day. Additionally, although the lower-dosage group (3 to 6 mg/day) in the two-dose group study was not superior to placebo with regard to PANSS total change, it was associated with a significantly higher composite response rate.Citation29
Treatment-emergent adverse events (including extrapyramidal symptom-related adverse events) and changes in weight and metabolic parameters that were identified in these studies were similar to those found in studies of paliperidone ER in schizophrenia.Citation44 As expected, the potent DCitation2 antagonism of paliperidone ER compared with other atypical antipsychotics resulted in an elevation in serum prolactin levels, with females having a higher increase than males. Of note, a previously reported study found that use of paliperidone ER resulted in increases in prolactin levels similar to those found with the use of risperidone.Citation45
Because patients with schizoaffective disorder are commonly treated with antipsychotics and mood stabilizers and/or antidepressants,Citation26–Citation28 results suggesting that paliperidone ER is efficacious both as monotherapy and adjunctive to mood stabilizers and/or antidepressants may be particularly valuable to the clinician. With the exception of tremor, the tolerability of paliperidone ER was comparable when used as monotherapy or adjunctive to mood stabilizers and/or antidepressants. However, it must be noted that although randomization was stratified by mood stabilizer and/or antidepressant use, the study was not designed to compare monotherapy with adjunctive therapy or to compare the relative efficacy of various adjunctive combinations, and the benefits and risks of specific combinations of paliperidone ER and mood stabilizers and/or antidepressants have not been studied. Nonetheless, no unique tolerability issues were identified with paliperidone ER in this population. Because of its limited liability for hepatically mediated drug–drug interactions, paliperidone ER may be a useful option for patients who follow complex medication regimens.Citation32–Citation34
Several additional factors must be considered in the interpretation of these results. First, this study population may have been biased toward subjects experiencing manic symptoms because of the specified entry criteria. Nevertheless, in addition to the 80% of subjects who displayed prominent manic symptoms, 67% of subjects displayed prominent depressive symptoms at baseline. Moreover, subjects with prominent manic, depressive, or mixed symptoms at baseline had significant psychotic and mood symptom improvement with paliperidone ER compared with placebo. Finally, long-term maintenance treatment with paliperidone ER has not yet been studied in this population. However, such a trial is planned with paliperidone palmitate, the once-monthly injectable formulation of paliperidone.
Conclusion
Although schizoaffective disorder is commonly encountered in populations of patients with mental illness, this disorder has not been methodically studied, and no established guidelines exist for the management of these patients. Data pooled from two large, international, placebo-controlled, six-week studies with paliperidone ER are now available, demonstrating that acutely ill patients with schizoaffective disorder manifest high levels of psychotic, manic, and depressive symptoms at baseline. Patients who received paliperidone ER, either as monotherapy or adjunctive to mood stabilizers and/or antidepressants, experienced significant improvement in schizoaffective symptoms. Subjects with prominent manic, depressive, or mixed symptoms at baseline showed significant psychotic and mood symptom improvement with paliperidone ER compared with placebo. Additionally, no new tolerability signals were detected in this patient population. These data demonstrate the efficacy and tolerability of paliperidone ER as monotherapy or adjunctive to mood stabilizers and/or antidepressants in the acute treatment of schizoaffective disorder.
Acknowledgment
The authors wish to acknowledge Mariana Ovnic, Matthew Grzywacz, and ApotheCom (funding supported by Ortho- McNeil Janssen Scientific Affairs, LLC, Titusville, NJ) for technical assistance in the development and submission of this manuscript.
Disclosure
This study was supported by Ortho-McNeil Janssen Scientific Affairs, LLC. CM Canuso and I Turkoz are employees of Johnson & Johnson Pharmaceutical Research and Development, LLC, and Johnson & Johnson stockholders. CA Bossie and DJ Fu are employees of Ortho-McNeil Janssen Scientific Affairs, LLC, and Johnson & Johnson stockholders.
References
- KasaninJThe acute schizoaffective psychoses. 1933Am J Psychiatry1994151Suppl 61441548192190
- PeralaJSuvisaariJSaarniSILifetime prevalence of psychotic and bipolar I disorders in a general populationArch Gen Psychiatry200764192817199051
- CanusoCMKosik-GonzalezCSheehanJFrequency of schizoaffective disorder diagnosis in patients with psychotic disorders using the mini-international neuropsychiatric interviewSchizophr Res20109830530620189355
- KentSFogartyMYellowleesPHeavy utilization of inpatient and outpatient services in a public mental health servicePsychiatr Serv199546125412578590110
- MattesJANayakDLithium versus fluphenazine for prophylaxis in mainly schizophrenic schizo-affectivesBiol Psychiatry1984194454496722235
- BrockingtonIFKendellREKellettJMCurrySHWainwrightSTrials of lithium, chlorpromazine and amitriptyline in schizoaffective patientsBr J Psychiatry1978133162168354733
- JanicakPGKeckPEJrDavisJMA double-blind, randomized, prospective evaluation of the efficacy and safety of risperidone versus haloperidol in the treatment of schizoaffective disorderJ Clin Psychopharmacol20012136036811476119
- OkumaTYamashitaITakahashiRA double-blind study of adjunctive carbamazepine versus placebo on excited states of schizophrenic and schizoaffective disordersActa Psychiatr Scand1989802502592573234
- ChengappaKNRDavidJKHaranathPA placebo-controlled, random-assignment, parallel-group pilot study of adjunctive topiramate for patients with schizoaffective disorder, bipolar typeBipolar Disord2007960961717845276
- GreilWLudwig-MayerhoferWErazoNLithium vs carbamazepine in the maintenance treatment of schizoaffective disorder: A randomised studyEur Arch Psychiatry Clin Neurosci199724742509088805
- CheniauxELandeira-FernandezJLessaTLDoes schizoaffective disorder really exist? A systematic review of the studies that compared schizoaffective disorder with schizophrenia or mood disordersJ Affect Disord200810620921717719092
- LindenmayerJPKaySRvanPHDistinction of schizoaffective from schizophrenic profile. Independent validationSchizophr Res198924234242487183
- OlfsonMMarcusSCWanGJTreatment patterns for schizoaffective disorder and schizophrenia among Medicaid patientsPsychiatr Serv20096021021619176415
- CraddockNJonesLJonesIRStrong genetic evidence for a selective influence of GABAA receptors on a component of the bipolar disorder phenotypeMol Psychiatry20101514615319078961
- HamshereMLGreenEKJonesIRGenetic utility of broadly defined bipolar schizoaffective disorder as a diagnostic conceptBr J Psychiatry2009195232919567891
- LenczTLipskyRHDeRossePBurdickKEKaneJMMalhotraAKMolecular differentiation of schizoaffective disorder from schizophrenia using BDNF haplotypesBr J Psychiatry200919431331819336781
- MalhiGSBerkMBourinMAtypical mood stabilizers: A “typical” role for atypical antipsychoticsActa Psychiatr Scand Suppl2005111Suppl 426293816104066
- DerrySMooreRAAtypical antipsychotics in bipolar disorder: Systematic review of randomised trialsBMC Psychiatry200774017705840
- CruzNSanchez-MorenoJTorresFGoikoleaJMValentiMVietaEEfficacy of modern antipsychotics in placebo-controlled trials in bipolar depression: A meta-analysisInt J Neuropsychopharmacol20101351419638254
- KeckPEJrMcElroySLStrakowskiSMSchizoaffective disorder: Role of atypical antipsychoticsSchizophr Res199935SupplS5S1210190221
- VietaEGoikoleaJMCorbellaBRisperidone safety and efficacy in the treatment of bipolar and schizoaffective disorders: Results from a 6-month, multicenter, open studyJ Clin Psychiatry20016281882511816872
- LasserRBossieCAGharabawiGEerdekensMNasrallahHAEfficacy and safety of long-acting risperidone in stable patients with schizoaffective disorderJ Affect Disord20048326327515555724
- TranPVTollefsonGDSangerTMLuYBergPHBeasleyCMJrOlanzapine versus haloperidol in the treatment of schizoaffective disorder. Acute and long-term therapyBr J Psychiatry1999174152210211146
- KeckPEJrReevesKRHarriganEPthe Ziprasidone Study GroupZiprasidone in the short-term treatment of patients with schizoaffective disorder: Results from two double-blind, placebo-controlled, multicenter studiesJ Clin Psychopharmacol200121273511199944
- GlickIDMankoskiREudiconeJMMarcusRNTranQVAssunção-TalbottSThe efficacy, safety, and tolerability of aripiprazole for the treatment of schizoaffective disorder: Results from a pooled analysis of a sub-population of subjects from two randomized, double-blind, placebo-controlled, pivotal trialsJ Affect Disord2009115182619230981
- LevinsonDFUmapathyCMusthaqMTreatment of schizoaffective disorder and schizophrenia with mood symptomsAm J Psychiatry19991561138114810450252
- McElroySLKeckPEJrStrakowskiSMAn overview of the treatment of schizoaffective disorderJ Clin Psychiatry199960Suppl 5162110192403
- FlynnJGriegerTABenedekDMPharmacologic treatment of hospitalized patients with schizoaffective disorderPsychiatr Serv200253949611773657
- CanusoCMLindenmayerJPKosik-GonzalezCA randomized, double-blind, placebo-controlled study of 2 dose ranges of paliperidone extended-release in the treatment of subjects with schizoaffective disorderJ Clin Psychiatry20107158759820492853
- CanusoCMSchoolerNCarothersJPaliperidone ER in schizoaffective disorder: A randomized controlled study comparing a flexible dose with placebo in patients treated with and without antidepressants and/or mood stabilizersJ Clin Psychopharmacol20103048749520814330
- Invega® (paliperidone) extended-release tablets [Prescribing Information]Titusville, NJJanssen, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc2010
- ConleyRRKellyDLDrug-drug interactions associated with second-generation antipsychotics: Considerations for clinicians and patientsPsychopharmacol Bull200740779717285099
- VermeirMNaessensIRemmerieBAbsorption, metabolism, and excretion of paliperidone, a new monoaminergic antagonist, in humansDrug Metab Dispos20083676977918227146
- BerwaertsJCletonAHerbenVThe effects of paroxetine on the pharmacokinetics of paliperidone extended-release tabletsPharmacopsychiatry20094215816319585395
- KaySRFiszbeinAOplerLAThe positive and negative syndrome scale (PANSS) for schizophreniaSchizophr Bull1987132612763616518
- YoungRCBiggsJTZieglerVEMeyerDAA rating scale for mania: Reliability, validity and sensitivityBr J Psychiatry1978133429435728692
- HamiltonMDevelopment of a rating scale for primary depressive illnessBr J Soc Clin Psychol196762782966080235
- AllenMHBartkoJJLindenmayerJPDevelopment and psychometric exploration of a clinical global impressions scale for schizoaffective disorder (CGI-SCA)Poster presented at 49th Annual New Clinical Drug Evaluation Unit Meeting2009 Jun 29–Jul 2Hollywood, FL
- MarderSRDavisJMChouinardGThe effects of risperidone on the five dimensions of schizophrenia derived by factor analysis: Combined results of the North American trialsJ Clin Psychiatry1997585385469448657
- SimpsonGMAngusJWA rating scale for extrapyramidal side effectsActa Psychiatr Scand Suppl197021211194917967
- GuyWAbnormal Involuntary Movement ScaleECDEU Assessment Manual for PsychopharmacologyWashington, DCU.S. Public Health Service1976
- BarnesTRA rating scale for drug-induced akathisiaBr J Psychiatry19891546726762574607
- SalvatorePBaldessariniRJTohenMMcLean-Harvard international first-episode project: Two-year stability of DSM-IV diagnoses in 500 first-episode psychotic disorder patientsJ Clin Psychiatry20097045846619200422
- MeltzerHYBoboWVNuamahIFEfficacy and tolerability of oral paliperidone extended-release tablets in the treatment of acute schizophrenia: Pooled data from three 6-week, placebo-controlled studiesJ Clin Psychiatry20086981782918466043
- BerwaertsJCletonARossenuSA comparison of serum prolactin concentrations after administration of paliperidone extended-release and risperidone tablets in patients with schizophreniaJ Psychopharmacol2010241011101819825908