
Abstract
Maintaining therapeutic plasma concentrations of an antipsychotic agent is essential in preventing relapse of symptoms in schizophrenia. Long-acting injectable (LAI) formulations provide extended exposure to antipsychotic therapy and have been useful in addressing treatment nonadherence. Aripiprazole is an atypical antipsychotic used in the treatment of schizophrenia and is available in 2 chemically different (aripiprazole monohydrate and aripiprazole lauroxil [AL]) and pharmaceutically different LAI formulations (aripiprazole once-monthly 400 mg [AOM 400] and AL). The pharmaceutical difference is that AL, unlike AOM 400, is a prodrug that requires additional metabolic steps to form the active drug aripiprazole. We present data demonstrating that aripiprazole plasma concentrations are similar for AOM 400 and the 882 mg dose of AL when administered once every 4 weeks and that both provide similar therapeutic plasma concentrations of aripiprazole when compared with therapeutic oral doses.
Introduction
Schizophrenia is a chronic disease for which continuous antipsychotic treatment substantially reduces the risk of relapse.Citation1 Thus, maintaining plasma drug concentrations within an agent’s therapeutic window is critical for achieving optimal outcomes. Aripiprazole, a second-generation antipsychotic, is a dihydrocarbostyril (quinolinone) discovered by Otsuka Pharmaceutical Co., Ltd. (Abilify®; Otsuka Pharmaceutical Co., Ltd., Tokyo, Japan).Citation2 It is indicated for the treatment of schizophrenia at recommended oral starting and target doses of 10–15 mg per day, and it has been shown to be effective over a dose range of 10–30 mg per day.Citation2 The median minimum plasma concentration at steady state (Cmin,ss) with oral aripiprazole 10 mg daily (the lowest effective dose) has been reported to be 94.0 ng/mL.Citation3,Citation4 Two long-acting injectable (LAI) pharmaceutical alternatives have subsequently become available: aripiprazole once-monthly 400 mg (AOM 400; Abilify Maintena®; Otsuka Pharmaceutical Co., Ltd.) and aripiprazole lauroxil (AL; Aristada®; Alkermes, Inc., Waltham, MA, USA). AL is a prodrug of aripiprazole that differs chemically from AOM, has a higher molecular weight (660.7 g/mol vs 466.4 g/mol, respectively),Citation5,Citation6 and undergoes 2 steps of hydrolysis for bioconversion to the active drug compound.Citation7 The first step is an enzymatic hydrolysis of AL to form N-hydroxy-methyl aripiprazole, which is subsequently hydrolyzed in the second step to aripiprazole.Citation7 Given that AOM 400 and AL are chemically and pharmaceutically distinct, differences in pharmacokinetics (PK) and bioavailability are possible. For example, to achieve therapeutic aripiprazole concentrations during initiation of therapy, the first dose of AL should be accompanied by daily oral aripiprazole for 21 days,Citation6 and the first dose of AOM should be accompanied by daily oral aripiprazole (or the patient’s current oral antipsychotic) for 14 days.Citation2 Though dose reductions may be indicated in some patients, such as those with a known P450 CYP2D6 polymorphism resulting in poor metabolism of aripiprazole, 400 mg given every 4 weeks is the standard recommended starting and maintenance dose for AOM.Citation5 Several dose strengths of AL are available, leading to the question of which AL dose and dose schedule compares most closely with AOM 400. Herein we present simulated and observed steady-state aripiprazole plasma concentrations after administration of AOM 400 and AL (as available in the public domain) to compare the plasma concentrations of the 2 products.
Sources and description of data
PK parameters presented
All plasma concentration PK values are shown at steady state (ss) and are derived from either simulated or observed plasma concentration data, as described in the following text. Simulations provide the average plasma concentration at steady state (Cavg,ss), which is an average of plasma levels during a dosing interval. Cavg,ss is calculated by dividing the area under the concentration-time curve (ie, all plasma concentrations during a dosing interval) by the dosing interval. The minimum plasma concentration observed over a dosing interval once steady state is reached, Cmin,ss, is typically used as a clinically relevant concentration related to efficacyCitation8 and is usually lower than Cavg,ss for a given agent and dosing regimen. Based on available data, this report presents simulated predictions of aripiprazole Cavg,ss for AOM 400 and AL, as well as observed aripiprazole Cmin,ss for each.
In this study, the lower boundary of the therapeutic window for aripiprazole is defined as the median Cmin,ss of the lowest, approved, safe, and effective oral dose (10 mg once daily) of aripiprazole in schizophrenia (94.0 ng/mL),Citation3,Citation4 and each aripiprazole LAI product is compared with this median Cmin,ss value.
Data sources
AOM
Simulated aripiprazole Cavg,ss for AOM 400 was derived from a population PK model. Individual empirical Bayes estimates of PK parameters were obtained for the final PK models using data from previously reported studies in patients who received either deltoid (n=84) or gluteal (n=91) injections of AOM 400.Citation9,Citation10 These estimates were used to predict individual steady-state PK profiles after 12 once-monthly doses using the numeric integration and basic PK modeling processes of NONMEM® (ICON plc, Dublin, Ireland).Citation11 From the simulated datasets, plasma aripiprazole concentrations on post-dose days 0, 4, 8, 12, 16, 20, 24, and 28 for both deltoid and gluteal AOM 400 administration were utilized to estimate Cavg values. Simulated Cavg,ss for oral aripiprazole 10 mg, 20 mg, and 30 mg were derived from a series of simulations using a dataset of 10,000 cytochrome P450 2D6 extensive metabolizers randomly generated based on observed significant covariate relationships (Otsuka America Pharmaceutical, Inc., unpublished data, 2011). This population was used to predict individual steady-state PK profiles, with corresponding para meter estimates taken from a previously developed population PK model for aripiprazole oral tablets and the numeric integration process of NONMEM. The final PK model simulated 100 once-daily oral aripiprazole doses for each dose level to estimate the Cavg,ss during the dosing interval.
Observed aripiprazole Cmin,ss following multiple doses of AOM 400 at the deltoid site were available from 86 patients with schizophrenia who participated in a randomized, open-label trialCitation9 and from 3 additional studies that evaluated aripiprazole Cmin,ss following multiple doses of AOM 400 at the gluteal site.Citation10,Citation12,Citation13 Two of these studies were randomized controlled phase III trials that contributed data from 165 and 214 patients, respectively;Citation12,Citation13 the third study was a randomized, open-label PK study that provided data from 10 patients.Citation10
AL
Simulated aripiprazole Cavg,ss following AL approved doses (441 mg, 662 mg, and 882 mg once monthly; 882 mg every 6 weeks) and oral aripiprazole doses of 10 mg, 20 mg, and 30 mg are available from the Center for Drug Evaluation and Research (CDER) of the US Food and Drug Administration (FDA).Citation14 The simulations are based on population PK modeling, using data from 4 phase I clinical trials (ALK9072-001, ALK9072-101, ALK9072-002 [NCT01493726], and ALK9072-102) and a single, 12-week, phase III trial (ALK9072-003 [NCT01469039]) conducted by Alkermes and involving a total of 616 subjects. The resulting estimates were used to predict PK profiles after 8 once-monthly doses or 6 every 6 weeks doses.
Median values for the observed Cmin,ss of aripiprazole are publically available only for AL 441 mg and 882 mg given every 4 weeks by intragluteal injection, as evaluated in a 12-week, randomized, double-blind, placebo-controlled trial.Citation14,Citation15
Results
Simulated Cavg,ss for AOM 400 when given at the deltoid and gluteal sites were 269 ng/mL and 291 ng/mL, respectively () (Otsuka America Pharmaceutical, Inc., unpublished data, 2014), and for the 441 mg and 882 mg doses of AL, given every 4 weeks, were 117 ng/mL and 225 ng/mL, respectively ().Citation14 Thus, simulated median Cavg,ss values for AOM 400 and AL 882 mg every 4 weeks were comparable, while simulated values for AL 441 mg were substantially lower than those for AOM 400. Likewise, simulated median Cavg,ss values for the 662 mg every 4 weeks and 882 mg every 6 weeks AL doses were below that of AOM 400 (178 ng/mL and 150 ng/mL, respectively).Citation14
Figure 1 Simulated aripiprazole Cavg,ss for oral aripiprazole 10–30 mg/d and AOM 400 (A), and observed aripiprazole Cmin,ss for AOM 400 (B).
Abbreviations: AOM 400, aripiprazole once-monthly 400 mg; Cavg,ss, average plasma concentration at steady state; Cmin,ss, minimum plasma concentration at steady state.
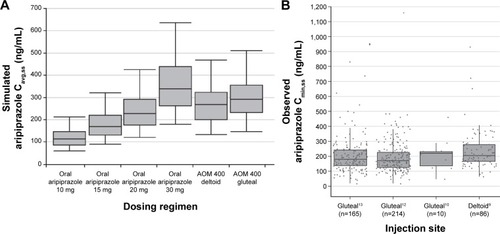
Figure 2 Simulated aripiprazole Cavg,ss for oral aripiprazole 10–30 mg/d, AL 441 mg every 4 weeks, and AL 882 mg every 4 weeks (A), and observed Cmin,ss for AL 441 mg and 882 mg every 4 weeks (B).
Abbreviations: AL, aripiprazole lauroxil; Cavg,ss, average plasma concentration at steady state; Cmin,ss, minimum plasma concentration at steady state.
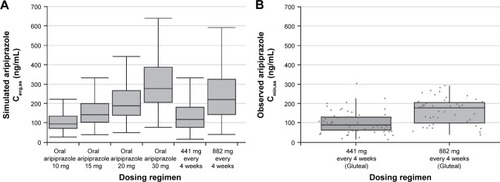
Previously reported clinical trials have shown that observed Cmin,ss values with AOM 400 are comparable between deltoid and gluteal injection sites ().Citation9,Citation10,Citation12,Citation13 These data also show that the median observed aripiprazole Cmin,ss with AOM 400 (~200 ng/mL; ) is slightly higher than the median aripiprazole Cmin,ss with AL 882 mg every 4 weeks (~175 ng/mL; ), following intragluteal injection of each. At least half of the observed aripiprazole Cmin,ss for AL 441 mg were below the median Cmin,ss for oral aripiprazole 10 mg daily. For AOM 400, 8.4% of patients overall had aripiprazole Cmin,ss values below 94 ng/mL.
Discussion
The data reviewed here show that different milligram dosages of the 2 available LAI formulations of aripiprazole, AOM 400 and AL 882 mg given every 4 weeks, provide similar aripiprazole plasma concentrations, despite the fact that AOM 400 provides 400 mg of aripiprazole and AL 882 mg injection contains 600 mg of aripiprazole.Citation6 This finding demonstrates that the absolute quantity of drug injected is not an appropriate comparison of the relative efficacy of different formulations. Rather, plasma concentrations are the relevant comparator for efficacy because they reflect not just the dose administered but also the absorption of the drug from the intramuscular space.
AOM 400 has previously been shown to provide median Cmin,ss within the plasma concentration range of oral aripiprazole 10–30 mg daily,Citation3,Citation10 and it has been shown to significantly delay relapse versus placebo in the maintenance treatment of schizophrenia for up to 52 weeks.Citation13 These data led to FDA approval of AOM 400 for the treatment of schizophrenia. As reviewed here, observed aripiprazole plasma concentrations across 4 clinical trials consistently demonstrated that treatment with AOM 400 provides a median Cmin,ss of ~200 ng/mL.
Plasma concentration data reviewed by the CDER indicate that 882 mg dose of AL given every 4 weeks provides a median Cmin,ss of ~175 ng/mL. The lowest approved dose of AL, 441 mg every 4 weeks, which provided an observed median Cmin,ss below 94.0 ng/mL, was shown to have similar efficacy to that of the 882 mg every 4 weeks dose over 12 weeks in the treatment of acute schizophrenia.Citation15 However, no long-term data are available to show comparable efficacy between these 2 AL doses. Because controlled efficacy data beyond 12 weeks are not currently available, the efficacy of AL for delaying symptomatic relapse has not been established.
Available observed plasma concentration data suggest that the aripiprazole median Cmin,ss for AL 882 mg administered every 4 weeks is similar to the aripiprazole median Cmin,ss for AOM 400, though it should be noted that these data were not obtained from a simultaneous comparison between the 2 LAI formulations. Because the data were derived from different studies, plasma samples were obtained from subjects who may have differed in demographics or clinical characteristics. Upon review of the published reports, no notable differences were observed in subjects in these studies with regard to age (mean age ranged between ~40 and 47 years), sex (primarily male), or body mass index (mean index ~28 kg/m2).Citation9,Citation10,Citation12,Citation13,Citation15 In most studies, the majority of patients were white, though 1 study enrolled primarily black patients (76%).Citation9
It should be recognized that because the data shown for AL in are from a publicly available summary report,Citation14 it was not possible to conduct an analysis using patient-level data. It should also be acknowledged that the simulations for Cavg,ss are based on different time points for AOM and AL. As noted in the prescribing information for each LAI, steady state for each product is reached after 4 once-monthly injections,Citation5,Citation6 and the number of doses used in the PK modeling for each product go well beyond this time point. Nevertheless, the Cmin,ss values based on observed data for each product provide the primary basis for our conclusions, and these steady-state values remain constant regardless of the number of doses.
Conclusion
Observed plasma concentrations can be used to compare different formulations of the same antipsychotic agent. Based on observed data from patients with schizophrenia, steady-state aripiprazole plasma concentrations are similar when LAI formulations are administered every 4 weeks as AOM 400 or as AL 882 mg.
Acknowledgments
Editorial support for development of this manuscript was provided by Sheri Arndt, PharmD, at C4 MedSolutions, LLC (Yardley, PA), a CHC Group company, and funded by Otsuka Pharmaceutical Development & Commercialization, Inc., and H. Lundbeck A/S.
Disclosure
PM Salzman, A Raoufinia, and S Legacy are employees of Otsuka Pharmaceutical Development & Commercialization, Inc.; P Such is an employee of H. Lundbeck A/S; and A Eramo is an employee of Lundbeck LLC. The authors report no other conflicts of interest in this work.
References
- HasanAFalkaiPWobrockTWFSBP Task Force on Treatment Guidelines for SchizophreniaWorld Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, part 2: update 2012 on the long-term treatment of schizophrenia and management of antipsychotic-induced side effectsWorld J Biol Psychiatry201314124423216388
- ABILIFY® (aripiprazole) [prescribing information]TokyoOtsuka Pharmaceutical Co., Ltd2016
- MallikaarjunSSalazarDEBramerSLPharmacokinetics, tolerability, and safety of aripiprazole following multiple oral dosing in normal healthy volunteersJ Clin Pharmacol200444217918714747427
- Center for Drug Evaluation and ResearchApplication Number: 202971Orig1s000 Clinical Pharmacology and Biopharmaceutics Review(s)Silver SpringFood and Drug Administration2011
- Abilify Maintena® US (aripiprazole) [prescribing information]TokyoOtsuka Pharmaceutical Co., Ltd2016
- Aristada® (aripiprazole lauroxil) [prescribing information]WalthamAlkermes, Inc2016
- RohdeMM RkNHåkanssonAEBiological conversion of aripiprazole lauroxil – an N-acyloxymethyl aripiprazole prodrugResults Pharma Sci20144192525756003
- HiemkeCBaumannPBergemannNAGNP consensus guidelines for therapeutic drug monitoring in psychiatry: update 2011Pharmacopsychiatry2011446195235
- RaoufiniaAPeters-StricklandTNylanderAGAripiprazole once-monthly 400 mg: comparison of pharmacokinetics, tolerability, and safety of deltoid versus gluteal administrationInt J Neuropsychopharmacol Epub2017215
- MallikaarjunSKaneJMBricmontPPharmacokinetics, tolerability and safety of aripiprazole once-monthly in adult schizophrenia: an open-label, parallel-arm, multiple-dose studySchizophr Res2013150128128823890595
- MouldDRUptonRNBasic concepts in population modeling, simulation, and model-based drug developmentCPT Pharmacometrics Syst Pharmacol20121e623835886
- FleischhackerWWSanchezRPerryPPAripiprazole once-monthly for treatment of schizophrenia: double-blind, randomised, non-inferiority studyBr J Psychiatry2014205213514424925984
- KaneJMSanchezRPerryPPAripiprazole intramuscular depot as maintenance treatment in patients with schizophrenia: a 52-week, multicenter, randomized, double-blind, placebo-controlled studyJ Clin Psychiatry201273561762422697189
- Center for Drug Evaluation and ResearchApplication Number: 207533Orig1s000 Clinical Pharmacology and Biopharmaceutics Review(s) (Addendum to PBPK, Pharmacometric, Clin Pharm Reviews and Clin Pharm Addendum) and Pharmacometric ReviewSilver SpringFood and Drug Administration2015
- MeltzerHYRisingerRNasrallahHAA randomized, double-blind, placebo-controlled trial of aripiprazole lauroxil in acute exacerbation of schizophreniaJ Clin Psychiatry20157681085109026114240