
Abstract
Background
The body dysmorphic disorder is prevalent in general population and in psychiatric, dermatological, and plastic-surgery patients, but there lacks a structure-validated, comprehensive self-report measure of body image concerns, which is established through both exploratory and confirmatory factor analyses.
Methods
We have composed a 34-item matrix targeting the body image concerns and trialed it in 328 male and 365 female Chinese university students. Answers to the matrix dealt with treatments including exploratory factor analyses, reserve of qualified items, and confirmatory factor analyses of latent structures.
Results
Six latent factors, namely the Social Avoidance, Appearance Dissatisfaction, Preoccupation with Reassurance, Perceived Distress/Discrimination, Defect Hiding, and Embarrassment in Public, were identified. The factors and their respective items have composed a 24-item questionnaire named as the Body Image Concern Scale. Each factor earned a satisfactory internal reliability, and the intercorrelations between these factors were in a median level. Women scored significantly higher than men did on the Appearance Dissatisfaction, Preoccupation with Reassurance, and Defect Hiding.
Conclusion
The Body Image Concern Scale has displayed its structure validation and gender preponderance in Chinese university students.
Introduction
The body dysmorphic disorder is characterized by the preoccupation with appearance or self-image, which causes significant distress or impairment of daily functions to an individual.Citation1 Its weighted prevalence in community adults was about 1.9%, in adolescents 2.2%, in students 3.3%, in psychiatric outpatients 5.8%, and in psychiatric inpatients 7.4%.Citation2 Various psychiatric problems such as depression, suicidality, social isolation, or withdrawal are comorbid with the body dysmorphic disorder.Citation3–Citation6 This disorder is also diagnosed in 7%–15% patients who seek treatment from dermatologists or plastic surgeons.Citation7 Regarding gender differences, men are more likely to be preoccupied with their genitals, muscles, and hair styles,Citation8 while women are more likely to be preoccupied with their weight, hips, breasts, legs, and body hairs, to hide perceived defects with various camouflaging techniques.Citation9,Citation10
Besides some questionnaires measuring other psychosomatic problems together with the body dysmorphic disorder, there are some specific inventories measuring the body image concerns in both male and female participants. However, none of these specific ones is structure-validated after both exploratory and confirmatory factor analyses, and none has covered a broader concern of body image. For instance, the Body Dysmorphic Disorder QuestionnaireCitation11 measures the preoccupation with physical appearance such as body weight and its effects on daily life; however, the questionnaire does not comprehensively assess the body dysmorphic disorder.Citation12 Another one is the Yale-Brown Obsessive-Compulsive Scale Modified for Body Dysmorphic Disorder,Citation13 which measures the symptom severity and its changes over time, and the adaptation to the symptoms similar to those of the obsessive-compulsive disorder. The third one is the Body Dysmorphic Disorder Examination,Citation14 which focuses on the body dysmorphic symptoms. However, it requires a face-to-face interview by a trained interviewer, which is time-consuming. The fourth (the Dysmorphic Concern Questionnaire)Citation15 and the fifth (the Body Dysmorphic Symptom Scale)Citation16 ones also measure the physical appearance in a unidimensional manner only.Citation17,Citation18
In the current study, we would like to develop a structure-validated self-report to measure a broader range of body image concerns. Based on the previous documentation, our first hypothesis is that such an assessment should be composed of the following six aspects. The first aspect includes the negative evaluation of and preoccupation with appearance. An example statement is “I am dissatisfied with my appearance defect,” as mentioned in previous studies.Citation11,Citation13–Citation16 The second aspect is the distress caused by the appearance defect. One example is “I am often upset when concentrating on my appearance,” as studied previously.Citation11,Citation13,Citation14,Citation16 The third one is the embarrassment in public, and the feeling of being scrutinized by others. One sample is “I feel uneasy or embarrassed in public situations such as city streets or restaurants where I concentrate on my appearance,” as mentioned previously.Citation14,Citation16 The fourth is the repetitive behaviors or mental acts relating to appearance. An example is “I often camouflage my appearance defect with clothes or makeup,” as covered in previous studies.Citation13–Citation16 The fifth one is the avoidance of social activities or physical contacts with others. An example is “Because of my appearance, I avoid appearing in social situations such as parties or speaking to authority figures,” as previously reported.Citation11,Citation13,Citation14,Citation16 The sixth one is the preliminary exclusion of other mental disorders. For example, “I have suffered from one or more of the following: eating disorder, obsessive-compulsive disorder, anxiety disorder, major depressive disorder, or other mental disorders,” as noted previously.Citation14
We, therefore, have developed an item matrix, and trialed it in Chinese university students. Our second hypothesis is that women score higher than men do on the negative evaluation of and the preoccupation with appearance, and on the repetitive behaviors (or mental acts) relating to appearance. We would apply both exploratory and confirmatory factor analyses to the item matrix, look for its latent factors and their possible gender differences, and develop a questionnaire measuring these body image concerns. We have expected that the emerged factors, the internal reliability of and the gender differences on these factors, and their interfactor relationships might help to describe the structure of the questionnaire.
Methods
Participants
Six hundred and ninety-three university students were invited to participate in the study: 328 men (mean age: 19.86 years with 1.78 SD; age range: 17–27 years) and 365 women (mean age: 20.42±2.16; age range: 17–26). There was no significant age difference between genders (t=−1.84, 95% confidence interval = [−0.58, 0.02], P=0.07). All participants were free from somatic or psychiatric illnesses and were asked to be drug or alcohol free for at least 72 hours prior to the test. The study protocol was approved by the Ethics Committee of Zhejiang University School of Public Health (No ZGL201606-1-1), and conformed to the Helsinki Declaration concerning human rights, and followed correct procedures concerning treatment of humans in research. All participants gave their written informed consent (guardians signed written informed consent for the young adolescents) for the current study.
Measures
The item matrix regarding the body image concerns covered the following aspects: (a) nine items for the negative evaluation of and preoccupation with appearance; (b) four items for the distress caused by the appearance defect; (c) six items for the embarrassment in public, and feeling of being scrutinized by others; (d) seven items for the repetitive behaviors or mental acts relating to appearance; (e) seven items for the avoidance of social activities or physical contacts with others; (f) one item for the preliminary exclusion of other mental disorders. The initial scale offers five alternatives with five-point Likert format: 1 – very unlike me, 2 – moderately unlike me, 3 – somewhat like and unlike me, 4 – moderately like me, and 5 – very like me.
Statistical analyses
Answers to the 34-item matrix were first subjected to a principal axis factoring analysis using the SPSS, Release Version 23.0.0 (IBM Corp., Armonk, NY, USA). Components extracted were treated as latent factors; the factor loadings were then rotated orthogonally using the varimax normalized methods. Items that were loaded less heavily (<0.40) on a target factor or cross-loaded heavily (>0.35) on more than one factor were removed from subsequent analyses one by one. The procedure continued until no further item needed to be removed.
The factor model fits were evaluated by confirmatory factor analysis for structural equation modeling using the Analysis of Moment Structures version 17.0 (AMOS Development Corp., 2008, Crawfordville, FL, USA). Following Schermelleh-Engel et al,Citation19 and Hu and Bentler,Citation20 we used the following parameters to identify the model fit: the χ2/df (better <3.0), goodness-of-fit index (better >0.9), adjusted goodness-of-fit index (better >0.9), comparative fit index (better >0.8), Tucker–Lewis index (better >0.8), root mean square error of approximation (better <0.05), and standardized root mean square residual (better <0.08). Afterwards, the factors and their related items were defined.
Furthermore, a questionnaire was developed based on the results of these exploratory and confirmatory factor analyses. The internal reliabilities (the Cronbach alphas) of the questionnaire factors were then calculated. The scores of each factor were submitted to multivariate analysis of variance (MANOVA) in the two gender groups. A P-value of <0.05 was considered to be significant. Moreover, the inter-relationships between factors in all participants were evaluated by the Pearson correlation test. To reduce the chance of Type I error regarding correlations, a P-value of <0.01 was considered to be significant.
Results
When analyzing the answers to the 34 items, after the principal axis factoring analysis, seven factors emerged with eigenvalues larger than 1.00: 31.98, 7.95, 5.04, 4.78, 3.76, 3.45, and 3.04. The visual speculation, the Minimum Average Partial test, and the Parallel Analysis suggested four- to seven-factor models; the first four, five, six, and seven factors altogether accounted for 49.74%, 53.50%, 56.96%, and 60.00%, respectively, of total variance. Items with higher target-loadings and lower cross-loadings on the respective factors were determined. According to the parameter values of the model fit () and the item numbers for each factor, the six-factor model was the optimal one. The standardized structure of the six-factor model is illustrated in .
Figure 1 Standardized factor structures for a confirmatory factor analysis of the six-factor Body Image Concern Scale model.
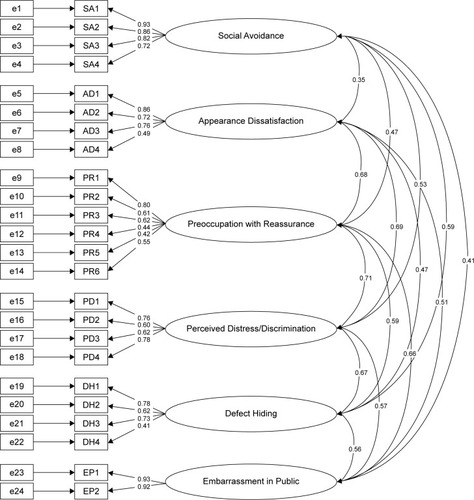
Table 1 Multiple-factor fitting models of the item matrix regarding the body image concerns in 693 participants
Factor 1 was loaded with items relating to the avoidance of social activities, thus was named as Social Avoidance. Factor 2 with items relating to the dissatisfaction of body appearance defect was then called Appearance Dissatisfaction. Factor 3 with items describing the repetitive attempts to improve the appearance and obsessive thoughts about the defect was called Preoccupation of Reassurance. Factor 4 with items describing the excessive high attention to others’ opinions of appearance and the distress thoughts of discrimination due to appearance was called Perceived Distress/Discrimination. Factor 5 with items describing the actions to hide defect or camouflage was called Defect Hiding. Factor 6 with items describing the embarrassment in public or social situations was called Embarrassment in Public. The determined items to be left altogether formed an inventory called the Body Image Concern Scale (). In all participants (N=693), the internal reliabilities (the Cronbach alphas) of these six factors were 0.90, 0.79, 0.75, 0.78, 0.71, and 0.92, respectively, and the intercorrelations between factors were in a medium level ().
Table 2 Item loadings on six factors in 693 participants
Table 3 The Body Image Concern Scale factor scores (mean ± SD) in two gender groups, and their internal reliabilities and intercorrelations in all participants
Moreover, MANOVA had found a significant gender difference on factor scores (Wilks’ λ=0.934, F [6, 686] =8.04, P<0.001). Specifically, women scored significantly higher on Appearance Dissatisfaction (F [1, 691] =16.41, P<0.001, mean square effect [MSE] =238.60), Preoccupation with Reassurance (F [1, 691] =22.12, P<0.001, MSE =362.57), and Defect Hiding (F [1, 691] =7.32, P=0.007, MSE =98.12) than men did ().
Discussion
Using both exploratory and confirmatory factor analyses on the 34-item matrix regarding the body image concerns, we have developed a structure-validated self-report, the 24-item Body Image Concern Scale in Chinese university students. The disclosure of six factors namely Social Avoidance, Appearance Dissatisfaction, Preoccupation with Reassurance, Perceived Distress/Discrimination, Defect Hiding, and Embarrassment in Public has partly confirmed our first hypothesis. Being distinct from each other, the six factors composed a satisfactory model, and some of them displayed a female preponderance. Each factor had a satisfactory internal reliability, and was intercorrelated with other factors in a medium level. In this case, our second hypothesis has been confirmed.
Factor 1, Social Avoidance, covered the avoidance of social situations or activities in public and the avoidance of physical contacts with others. This aspect was presented before in the Body Dysmorphic Disorder Questionnaire, the Body Dysmorphic Disorder Examination, the modified Yale-Brown Obsessive-Compulsive Scale, and the Body Dysmorphic Symptom Scale.Citation11,Citation13,Citation14,Citation16 This factor corresponds to the clinical features of body dysmorphic disorder, for instance, the appearance preoccupation causes significant secondary social anxiety and avoidance,Citation21 and some aspects of the social anxiety contribute to the functional impairment of the disorder in return.Citation4
Factor 2, Appearance Dissatisfaction, covered the negative evaluation of appearance, which corresponds to the core feature of body dysmorphic disorder.Citation1 The aspect was also considered in other similar measures such as the Body Dysmorphic Disorder Questionnaire, the Body Dysmorphic Disorder Examination, the modified Yale-Brown Obsessive-Compulsive Scale, and the Body Dysmorphic Symptom Scale.Citation11,Citation13,Citation14,Citation16 Patients with body dysmorphic disorder tended to overfocus on the negative appearance attributes.Citation22 The preoccupation with dissatisfaction also triggered the explicit symptoms of the body dysmorphic disorder, eg, the significant distress or impairment in important areas of daily functioning.Citation23 Normally, women pay more attention to their appearance than men do,Citation24 and the physical beauty is a central component of female concerns.Citation25 Our female participants scored higher on Appearance Dissatisfaction, which was in line with these notions.
Factor 3, Preoccupation with Reassurance, covered the excessive self-evaluation of appearance, which led to the frequently physical camouflaging, body checking, and reassurance seeking from others. The factor corresponds well to the repetitive behaviors and mental acts in clinicsCitation1 and in previous report.Citation26 On the other hand, patients with body dysmorphic disorder selectively attend to their appearance flaws and mostly ignore the rest of their body,Citation27 which is similar to those patients with obsessive-compulsive disorder.Citation28,Citation29 Women scored higher on this factor, which was also consistent with the previous reportCitation8 where women performed more increased mirror-checking and cloth-changing behaviors than men did.
Factor 4, Perceived Distress/Discrimination, covered the preoccupation with negative appearance evaluation from others and the perceived discrimination from others leading to distress. This factor was described in previous measurements of the body dysmorphic disorder.Citation14,Citation16 In clinics, however, some patients with body dysmorphic disorder present ideas or delusions of reference.Citation1 To relieve distress, patients tended to accept plastic surgery for both social and personal reasons.Citation30 The factor also helps to understand the comorbidity between body dysmorphic disorder and social anxiety disorder.Citation31
Factor 5, Defect Hiding, covered avoidance of physical contacts with others and camouflaging appearance with body posture, which corresponds to the clinical description of body dysmorphic disorder,Citation1 and these patients frequently show rituals to correct, fix, or hide body parts.Citation14–Citation16,Citation26 The higher score in women was in accordance with the previous investigation that women more often altered their body position to hide their perceived defect.Citation8
Factor 6, Embarrassment in Public, covered self-consciousness, embarrassment, and feeling of being scrutinized in public or social situations, which also corresponds to the clinical manifestation of body dysmorphic disorder.Citation1 Previous measurements of this kind, such as the Body Dysmorphic Disorder Examination and the Body Dysmorphic Symptom Scale, have described the embarrassment due to appearance defect.Citation14,Citation16 In addition, these patients presented feelings of inferiority,Citation32 which corresponds with shame being a defensive response to threats and social attractiveness losses.Citation33
One should also bear in mind the limitations of the current study design. First, our participants were young university students; thus, results obtained in this age group might not be generalized to a broader age population. Second, our results were based on the healthy participants, and whether they would be valid in psychiatric conditions such as the obsessive-compulsive disorder and eating disorder remains to be seen. Third, personality traits might influence the body imaging report, but that merits further investigation. Future studies might be designed to address the validation of the scale, such as sensitivity, discriminant validity, and test–retest reliability, and convergent validity with other instruments assessing body dysmorphic disorder symptoms. Nevertheless, the questionnaire we developed was a structure-validated one, which might help a precise description of body dysmorphic disorder and related problems in clinics. The earlier detection would ensure an earlier psychotherapy applying to the disorder; for instance, the cognitive-behavioral therapy has proven to be effective in these patients by relieving symptoms and improving self-esteem and quality of life.Citation34
Acknowledgments
The study was supported by grants from the Natural Science Foundation of China (No 81571336) to the corresponding author (Dr W Wang). WH, QMZ, and YJ had contributed equally to the current study.
Disclosure
All authors report no conflicts of interest in this work.
References
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5®)ArlingtonAmerican Psychiatric Pub2013
- VealeDGledhillLJChristodoulouPHodsollJBody dysmorphic disorder in different settings: A systematic review and estimated weighted prevalenceBody Image20161816818627498379
- FangAHofmannSGRelationship between social anxiety disorder and body dysmorphic disorderClin Psychol Rev20103081040104820817336
- KellyMMWaltersCPhillipsKASocial anxiety and its relationship to functional impairment in body dysmorphic disorderBehav Ther201041214315320412881
- FangAAsnaaniAGutnerCCookCWilhelmSHofmannSGRejection sensitivity mediates the relationship between social anxiety and body dysmorphic concernsJ Anxiety Disord201125794694921741203
- AngelakisIGoodingPAPanagiotiMSuicidality in body dysmorphic disorder (BDD): a systematic review with meta-analysisClin Psychol Rev201649556627607741
- JakubietzMJakubietzRJKlossDFGruenertJJBody dysmorphic disorder: diagnosis and approachPlast Reconstr Surg200711961924193017440376
- PhillipsKAMenardWFayCGender similarities and differences in 200 individuals with body dysmorphic disorderCompr Psychiatry2006472778716490564
- PerugiGAkiskalHSGiannottiDFrareFDi VaioSCassanoGBGender-related differences in body dysmorphic disorder (dysmorphophobia)J Nerv Ment Dis199718595785829307620
- PhillipsKADiazSFGender differences in body dysmorphic disorderJ Nerv Ment Dis199718595705779307619
- PhillipsKAThe broken mirror: understanding and treating body dysmorphic disorderOxford University PressUSA1996
- LittletonHLAxsomDPuryCLDevelopment of the body image concern inventoryBehav Res Ther200543222924115629752
- PhillipsKAHollanderERasmussenSAAronowitzBRA severity rating scale for body dysmorphic disorder: development, reliability, and validity of a modified version of the Yale-Brown Obsessive Compulsive ScalePsychopharmacol Bull199733117229133747
- RosenJCReiterJDevelopment of the body dysmorphic disorder examinationBehav Res Ther19963497557668936758
- OosthuizenPLambertTCastleDJDysmorphic concern: prevalence and associations with clinical variablesAust NZ J Psychiatry1998321129132
- KaymakYTanerEŞimşekIBody dysmorphic disorder in university students with skin diseases compared with healthy controlsActa Derm Venereol200989328128419479126
- MancusoSGKnoesenNPCastleDJThe dysmorphic concern questionnaire: a screening measure for body dysmorphic disorderAust NZ J Psychiatry2010446535542
- PicavetVGabriëlsLJorissenMHellingsPWScreening tools for body dysmorphic disorder in a cosmetic surgery settingLaryngoscope2011121122535254122109751
- Schermelleh-EngelKMoosbruggerHMüllerHEvaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measuresMethods of psychological research online2003822374
- HuLBentlerPMCutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternativesStructural Equation Modeling199961155
- PintoAPhillipsKASocial anxiety in body dysmorphic disorderBody Image20052440140517075614
- GreenbergJLReumanLHartmannASKasarskisIWilhelmSVisual hot spots: An eye tracking study of attention bias in body dysmorphic disorderJ Psychiatric Res201457125132
- BuhlmannUEtcoffNLWilhelmSFacial attractiveness ratings and perfectionism in body dysmorphic disorder and obsessive-compulsive disorderJ Anxiety Disord200822354054717624717
- BergnerMRemerPWhetsellCTransforming women’s body image: a feminist counseling approachWomen Ther1985432538
- Striegel-MooreRHFrankoDLBody image issues among girls and womenCashTFPruzinskyTBody image: A handbook of theory, research, and clinical practiceNew YorkGuilford2002183191
- FangAWilhelmSClinical features, cognitive biases, and treatment of body dysmorphic disorderAnnu Rev Clin Psycho201511187212
- DeckersbachTSavageCRPhillipsKACharacteristics of memory dysfunction in body dysmorphic disorderJ Intern Neuropsychol Soc2000606673681
- RachmanSA cognitive theory of obsessionsBehav Res Ther19973597938029299799
- SavageCRBaerLKeuthenNJBrownHDRauchSLJenikeMAOrganizational strategies mediate nonverbal memory impairment in obsessive–compulsive disorderBiol Psychiatry199945790591610202579
- ParkLECalogeroRMYoungAFDiraddoAMAppearance-based rejection sensitivity predicts body dysmorphic disorder symptoms and cosmetic surgery acceptanceJ Soc Clin Psychol2010295489509
- BuhlmannUMcNallyRJWilhelmSFlorinISelective processing of emotional information in body dysmorphic disorderJ Anxiety Disord200216328929812214814
- VealeDRileySMirror, mirror on the wall, who is the ugliest of them all? The psychopathology of mirror gazing in body dysmorphic disorderBehav Res Ther200139121381139311758697
- GilbertPMilesJBody shame: Conceptualisation, research and treatmentNew York, NYBrunner–Routledge2014267282
- GreenbergJLMarkowitzSPetronkoMRTaylorCEWilhelmSWilsonGTCognitive-behavioral therapy for adolescent body dysmorphic disorderCogn Behav Pract2010173248258