
Abstract
Purpose
Diagnosing epilepsy in the elderly population can be difficult due to mimicking symptoms. Furthermore, epileptic symptoms can also be masked by various symptoms. We hypothesized that elderly patients with epilepsy exhibit specific clinical features among the various symptoms.
Patients and methods
From 2009 to 2017, 177 patients who were older than 65 years were referred to our epilepsy center. Out of this group, the onset of symptoms occurred after reaching the age of 50 years in 152 of the patients, who were additionally being treated at our clinic. We divided their symptoms in accordance with their consciousness levels, which were defined as follows: full wakefulness level I, impaired awareness level II, and loss of consciousness level III. We also classified the duration of the symptoms as <10 seconds, ≥10 seconds but <1 minute, ≥1 minute but <5 minutes, ≥5 minutes but <10 minutes, ≥10 minutes but <1 hour, and ≥1 hour.
Results
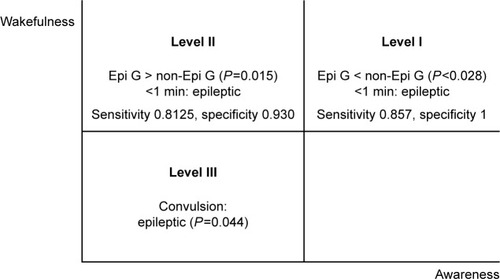
Among the 152 patients analyzed (mean age 72.9 years, standard deviation 6.71, range 65–92), 84 patients had epilepsy (epilepsy group) while 68 did not exhibit epilepsy (nonepilepsy group). For the consciousness levels, there were more level I patients in the nonepilepsy vs epilepsy group (P<0.028), with symptom duration lasting <1 minute (sensitivity 0.857, specificity 1) in the epilepsy group. In contrast, there were more level II patients in the epilepsy vs the nonepilepsy group (P=0.015), with the duration of symptoms lasting <1 minute (sensitivity 0.8125, specificity 0.930) in the epilepsy group. For the level III consciousness, convulsions were more commonly seen in the epilepsy group (P=0.044).
Conclusion
Symptoms that last <1 minute with awareness and impaired awareness might be epileptic in the elderly population.
Introduction
Epilepsy incidence exhibits bimodality in children and the elderly.Citation1 It is known that incidence and prevalence of epilepsy increase with age.Citation2–Citation4 Along with the rapid population growth currently observed in the world, the elderly population is also rapidly increasing.Citation5 However, at present, there has not been a large amount of research into epilepsy in the elderly.Citation4 Moreover, it has been reported that the diagnosis of epilepsy in the elderly population can be difficult.Citation2,Citation6,Citation7 The difficulties in diagnosing epilepsy in the elderly include the fact that epilepsy can be concomitant with post-stroke behavior,Citation8 dementia,Citation9 or the symptoms can mimic other psychiatric symptoms.Citation10,Citation11 Additionally, there are risks of syncope, hypo- and hyperglycemia, and transient ischemic attack in this patient population. Thus, overall these epileptic symptoms can be masked by various symptoms. The hypothesis of our present study was that epilepsy in elderly subjects exhibits specific clinical features that differ among the various other symptoms seen in this population. Furthermore, the main aim of this study was to review the consciousness level and duration of episodes during the clinical manifestation in elderly subjects.
Patients and methods
Study design and ethical approval
The Ethics Committee of Seirei Hamamatsu General Hospital in accordance with the principles of the Declaration of Helsinki approved the protocol for this study. The participants in this cross-sectional, observational, nonrandomized, intrasubjective comparison and case-controlled study were identified via a retrospective electronic chart review that was conducted from August 2009 to December 2017 at the Comprehensive Epilepsy Center, Seirei Hamamatsu General Hospital. Written informed consent was obtained from all patients.
Patients
From August 2009 to December 2017, 177 patients who were older than 65 years of age were referred to our Comprehensive Epilepsy Center. After reviewing the medical records, patients who fulfilled the following criteria were selected: 1) age older than 65 years, 2) onset of the symptoms occurred after reaching 50 years of age, and 3) have been treated at our clinic. Patients with onsets that occurred prior to reaching 50 years of age or that recurred after their 50’s were excluded from the study.
Medical questionnaire and medical interview
Primary outcome measures
The primary outcome measures were the reviews of the consciousness level and duration of the symptoms.
All patients responded to a medical questionnaire form prior to undergoing a medical interview. Board-certified epilepsy specialists (AF and KS) were responsible for obtaining the patient’s detailed medical histories. Information on the medical history and symptoms were obtained not only from the actual patients but during telephone calls with eyewitnesses who directly observed the epilepsy episode. We also examined symptoms that could be observed in videos of the patient that were taken during the epilepsy episodes.
Patient symptoms were classified in accordance with their consciousness level.Citation12,Citation13 Consciousness level I was defined as symptoms that occurred while the patient was at a full wakefulness level. These included focal onset awareness seizure or simple partial seizure that occurred in epilepsy cases. At consciousness level I, it was required that the person was aware of self and environment during the seizure, even if immobile. The subjects were able to remember what had happened during the event. Consciousness level II was defined as symptoms that occurred while the patient was at an impaired awareness level. These included focal onset impaired awareness seizure or complex partial seizures that occurred during epilepsy cases. At consciousness level II, it was required that the person had an impaired awareness during any part of the event. These subjects exhibited impaired awareness of the events without realizing that they occurred. However, consciousness was maintained during this period. Consciousness level III was defined as symptoms that occurred while the patient had lost consciousness. These included bilateral tonic–clonic seizure or secondary generalized seizure that occurred during epilepsy cases. At consciousness level III, it was required that the patients had completely lost consciousness and were not awakened by external stimuli. During the level III evaluations, we also reviewed whether or not the patients exhibited convulsions.
In addition to determining the different consciousness levels, we also reviewed the duration of symptoms. The duration of the symptoms was divided as follows:
<10 seconds
≥10 seconds but <1 minute
≥1 minute but <5 minutes
≥5 minutes but <10 minutes
≥10 minutes but <1 hour
≥1 hour.
Secondary outcome measurements
Secondary outcome measurements investigated included the cognitive impairment, psychiatric symptoms, whether or not the patient was able to drive, traffic accidents caused by the symptoms, diagnosis, etiology of the symptoms, treatment, and amnesia. To survey the cognitive impairment and psychiatric symptoms, we obtained referral letters from each specialist who saw the patient. For the driving and traffic accident surveys, we interviewed the patients, their family, and previous physicians in addition to checking information from referral letters.
Diagnosis and treatment
Diagnosis
All patients underwent brain 3.0-T magnetic resonance image and electroencephalography (EEG) evaluations. The EEGs were objectively read by board-certified clinical neurophysiologists in EEG (AF, KS, TO, and EH). After reading the EEGs, the neurophysiologists in EEG reviewed all of the findings and submitted reports on each of the subjects. If further examinations were required, patients underwent long-term video EEG (VEEG), single photon emission tomography, 2-[18F]fluoro-2-deoxy-D-glucose positron emission tomography, and neuropsychological evaluation. Epilepsy was diagnosed by board-certified epileptologists (AF and KS) on the basis of the patient’s clinical information, which included medical history, EEG reports, 3.0-T magnetic resonance imaging, VEEG, single photon emission tomography, and positron emission tomography. When we encountered difficulties in diagnosing the epilepsy, patients were further discussed during Comprehensive Epilepsy Center conferences. At these conferences, patients were discussed by the authors and other epileptologists (TO, YM, MN, SB, SI, and HE).
Treatment
After the diagnosis of epilepsy, we appropriately adjusted the patient’s antiepilepsy drugs (AEDs), performed epilepsy surgery, vagus nerve stimulation therapy, and, where necessary, took a wait-and-see (WAS) approach considering their social background. If patients were diagnosed as being nonepileptic, we took a WAS approach or sent them to each of the study specialists that included cardiologists, endocrinologists, psychiatrists, etc, for further investigation, treatment, and follow-up.
Statistical analysis
We statistically compared the epilepsy and nonepilepsy groups by using the Mann–Whitney rank-sum test, chi-squared test, and Fisher’s exact test, as appropriate. Statistical significance was set at P<0.05. The cutoff value was calculated by the receiver operating characteristic (ROC) curve analysis. All analyses were performed using Sigma Plot 14 software (Systat Software, San Jose, CA, USA).
Results
Clinical information
Among the 177 patients who were referred to our epilepsy center, 152 patients met the inclusion criteria (mean age 72.9 years, standard deviation 6.71, range 65–92). Among the enrolled patients, 84 (34 females and 50 males) were diagnosed with epilepsy (epilepsy group) while 68 (34 females and 34 males) were diagnosed as not having epilepsy (nonepilepsy group). There was no statistical difference between the groups in terms of age (P=0.621) and sex (P=0.493). presents the clinical information for the patients.
Table 1 Clinical information
Primary outcome measures
Consciousness level I
There were 6 patients who exhibited clinical manifestations under wakefulness (3 motor, 2 sensory, and 1 aphasia with motor manifestation) in the epilepsy group while there were 14 patients in the nonepilepsy group. There were more patients in the nonepilepsy vs the epilepsy group (P<0.028).
The duration in the epilepsy group was shorter than that observed in the nonepilepsy group (P<0.001). ROC curve analysis indicated that the cutoff value was level III. This meant that the duration of the epileptic seizure in elderly patients was <1 minute (sensitivity =1 − false-positive fraction [FPF] =1−0.429=0.857, specificity = true positive fraction [TPF] =1.00).
One patient with epilepsy (Patient No. 76) exhibited aphasia and hand twitching under wakefulness followed by bilateral tonic–clonic convulsion. This patient was classified as level III.
Consciousness level II
There were 57 patients who exhibited a loss of awareness in the epilepsy group, while there were 32 patients who exhibited attention, concentration and performance impairment, etc, in the nonepilepsy group. The difference between these groups was statistically significant (P=0.015). In addition, impaired awareness was more often seen in the epilepsy vs the nonepilepsy group.
There was a shorter duration in the epilepsy vs the non-epilepsy group (P<0.001). ROC curve analysis showed that the cutoff value was level III. This indicated that the duration of the epileptic seizure in the elderly patients was <1 minute (sensitivity =1 − FPF =1−0.1875=0.8125, specificity = TPF =0.930).
There were seven patients who exhibited focal onset impaired awareness seizure followed by bilateral tonic–clonic seizure. These seven patients were classified as level III.
Consciousness level III
There were 22 patients in the epilepsy and 28 patients in the nonepilepsy group who lost consciousness. However, there was no statistically significant difference between these two groups (P=0.075). There was also no statistical difference for the duration between the two groups (P=0.748). In terms of convulsion, there were 22 patients in the epilepsy and 8 in the nonepilepsy group who exhibited generalized convulsions. The difference between the groups was statistically significant (P=0.044).
shows each consciousness level and the duration of symptoms ().
Table 2 Conscious level, duration of symptoms and convulsions
Figure 1 Consciousness level and duration of symptoms.
Secondary outcome measures
Cognitive impairment
There were 58 patients (38.24%) with cognitive impairment, with 39 patients in the epilepsy and 19 in the nonepilepsy group. The difference between the groups was not statistically significant.
There were 23 (59%) patients with mild cognitive impairment (MCI), 7 (17.9%) with Alzheimer disease (AD), 4 (10.3%) with dementia with Lewy body (DLB), 3 (7.7%) with vascular dementia, and 2 (5.1%) with mixed dementia in the epilepsy group.
There were 12 (63.2%) MCI, 4 (21.1%) DLB, 2 (10.5%) AD, and 1 (4.2%) vascular dementia in the nonepilepsy group.
There was no statistically significant difference between the two groups (P=0.916). There was also no statistically significant difference found for the different forms of dementia (MCI P=0.321, AD P=0.703, DLB P=0.246, vs P=1.000).
Psychiatric symptoms
There were 28 (33.3%) patients in the epilepsy and 19 (27.9%) in the nonepilepsy group who exhibited psychiatric symptoms. The difference between the groups was not statistically significant (P=0.590). There were 9 (32.1%) behavioral and psychological symptoms of dementia (BPSD) in the epilepsy and 13 (68.4%) in the nonepilepsy group. The difference between the groups was statistically significant (P=0.019).
Driving
There were 28 patients who continued to drive at the time of diagnosis in the epilepsy and 24 in the nonepilepsy group, which was not statistically significant (P=0.725). There were eight patients with traffic accidents that were associated with their symptoms in the epilepsy and two in the nonepilepsy group, which was not statistically significant (P=0.086).
Diagnosis
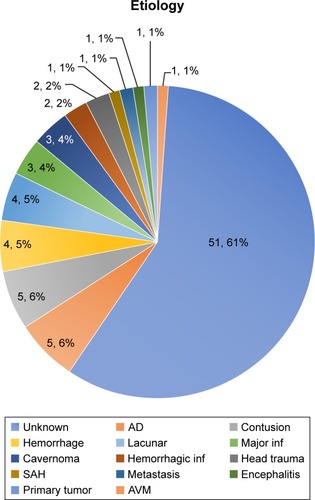
In the Epilepsy group, there were 63 (75.0%) patients with temporal lobe epilepsy (TLE), 12 (14.3%) with frontal lobe epilepsy (FLE), 2 (2.3%) with occipital lobe epilepsy, 1 (1.1%) with temporofrontal lobe epilepsy, 5 (6.0%) with epileptic convulsion, and 1 (1.1%) with focal onset epilepsy. There was no significance difference between the TLE and FLE for the duration (P=0.890) and consciousness level (P=0.304). In the nonepilepsy group, there were 39 (58.8%) nonepileptic patients with an unknown etiology, 10 (14.7%) with syncope, 7 (10.3%) with BPSD, 3 (4.4%) with postprandial hypotension, 3 (4.4%) with psychogenic nonepileptic spells, 2 (2.9%) with hypoglycemia, 2 (2.9%) with Parkinson’s disease or Parkinson’s syndrome, 1 (1.4%) with phenytoin toxicity, and 1 (1.4%) with transient global amnesia. shows the breakdown of the etiology in the nonepilepsy group.
Figure 2 Etiology of epilepsy.
Abbreviations: AD, Alzheimer’s disease; AVM, arteriovenous malformation; SAH, subarachanoid hemorrhage.
Treatment
AED adjustment was performed in 64 (76.2%) patients. Open cranial surgery was performed in 2 (2.3%) patients, while 1 (1.2%) underwent vagus nerve stimulation therapy and 17 (13.1%) were placed in the WAS approach category.
There were 45 (53.6%) patients who achieved seizure freedom, with 23 (27.4%) classified as more than 80% responders and 5 (6.0%) who were more than 50% responders. No appreciable change was observed in 11 (13.1%) patients.
Amnesia
The diagnosis of transient epileptic amnesia (TEA) was made on the basis of the following criteria: 1) there was a history of recurrent witnessed episodes of transient amnesia; 2) cognitive functions other than memory were judged to be intact during typical episodes by a reliable witness; and 3) there was evidence for a diagnosis of epilepsy.Citation14 There were four patients who met the criteria for inclusion in the epilepsy group, and one patient who was diagnosed as transient global amnesia in the nonepilepsy group.
Discussion
Primary outcome measures
The cutoff value for the duration in elderly with epilepsy was <1 minute when our results classified these patients as level I and II consciousness. Although, the duration of focal onset impaired awareness seizures have been reported to typically last more than 1 minute,Citation15,Citation16 symptoms that last <1 minute during impaired awareness might actually be epileptic in the elderly population.
However, it is our belief that it could be fairly difficult for elderly to precisely describe their aura. Thus, this could be the reason why only six patients with wakeful consciousness level (level I) were diagnosed as having epilepsy. Based on these findings, this suggests that diagnosing focal onset awareness seizure in the elderly population could be challenging. Furthermore, since the duration of awareness seizures generally vary,Citation16,Citation17 and the short duration in wakefulness seen in our study might actually be a feature of elderly epilepsy. However, in order to avoid any misdiagnosis, the presence of long-lasting nonconvulsive status epilepticus also should be taken into consideration when evaluating these types of patients.Citation18
As consciousness level and duration of the symptoms could not be used to determine the difference between epileptic and nonepileptic symptoms for the consciousness level III, it might be possible to use the presence of convulsions as a factor to distinguish between the symptoms.
The hypothesis of our present study was that there are specific clinical features associated with elderly subjects with epilepsy. Our results did show that awareness and impaired awareness seizures with less than a 1-minute duration appear to be a specific clinical feature that is associated with elderly patients with epilepsy.
One of the limitations of this study was that the durations of the symptoms were not always meticulously determined during the observations in this study. In fact, while many of the symptoms were recorded by the videos taken of the patient, others came from eyewitness accounts of the symptoms, which at times could be very subjective in nature. To obtain more accurate information on the duration, a further study that performs VEEG and accurately measures the duration in seconds will need to be undertaken in the future.
Secondary outcome measures
Concomitant symptoms
Cognitive impairment was not significantly different in each group. However, BPSD was more commonly seen in the nonepilepsy group. This indicates that there were more MCI with BPSD in the nonepilepsy group.Citation19 Additionally, it is known that there is a higher prevalence of psychosis found in patients with epilepsy compared with the general population.Citation20 This could potentially be explained by the fact that there were relatively many more non-BPSD patients in the epilepsy group vs the number of BPSD patients in the nonepilepsy group. As cognitive impairment and psychiatric symptoms were evenly seen in both groups, this makes the diagnosis of epilepsy difficult. In addition, it is our belief that MCI with BPSD also makes it much more difficult to determine this diagnosis in the elderly population.
Diagnosis and treatment
TLE (75%) followed by FLE were the most commonly seen forms of epilepsy in this study. Since TLE is the most common epilepsy observed in adults, it is likely that the elderly population will also exhibit the same level of occurrence.Citation3 Amyloid deposition is one of the common conditions seen in both AD and cerebral hemorrhage.Citation21 Based on these findings, it has been presumed that the peripheral symptoms related to these disease states might also complicate making a diagnosis for these types of diseases.Citation22
Although the success of treatments aimed at achieving seizure freedom in patients are as low as 53.6%, this level was considered to be refractory enough for these treatments to be introduced for use in our epilepsy center. PanayiotopoulosCitation23 has reported that elderly patients are more likely to suffer from drug-induced disease than derive any benefits from ill-advised AED prescribing. Therefore, when treating elderly patients with epilepsy, it is important to not merely achieve complete seizure freedom, but also consider the balance between treatment efficacy and the adverse effect of AEDs.
Amnesia
A previous study reported on a patient with TEA who did not exhibit any epileptic seizures.Citation24 However, all four patients with TEA in our study had impaired awareness seizure. Thus, these types of cases might be missed impaired awareness seizure due to the very short duration of the seizure.
Driving and traffic accidents
There was no significance difference observed between the epilepsy and nonepilepsy groups in terms of driving (P=0.725). This is likely due to the fact that there are overall issues with driving in the elderly population. Moreover, we also found that there was no statistically significant difference in both groups for traffic accidents related to their symptoms (P=0.086). Thus, these results appear to suggest that epilepsy cannot be definitively cited as a cause of traffic accidents involving elderly.
Conclusion
Symptoms that last <1 minute with awareness and impaired awareness might be epileptic in the elderly population.
Ethical publication statement
We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest concerning the patients or methods used in this study or the findings specified in this paper. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
References
- HauserWAAnnegersJFKurlandLTIncidence of epilepsy and unprovoked seizures in Rochester, Minnesota: 1935–1984Epilepsia19933434534588504780
- BrodieMJElderATKwanPEpilepsy in later lifeLancet Neurol20098111019103019800848
- TanakaAAkamatsuNShouzakiTClinical characteristics and treatment responses in new-onset epilepsy in the elderlySeizure201322977277523849689
- Hernández-RonquilloLAdamsSBallendineSTéllez-ZentenoJFEpilepsy in an elderly population: Classification, etiology and drug resistanceEpilepsy Res2018140909429310076
- GuilbertJJThe World Health report 2006: Working together for healthEduc Health2006193385387
- SirvenJIOzunaJEpilepsy Foundation of America. Diagnosing epilepsy in older adults: what does it mean for the primary care physician?Geriatrics200560103035
- AustinJAbdullaAIdentifying and managing epilepsy in older adultsNurs Times201310932023
- TanakaTYamagamiHIharaMSeizure Outcomes and Predictors of Recurrent Post-Stroke Seizure: A Retrospective Observational Cohort StudyPLoS One2015108e013620026309124
- VosselKATartagliaMCNygaardHBZemanAZMillerBLEpileptic activity in Alzheimer’s disease: causes and clinical relevanceLancet Neurol201716431132228327340
- NaeijeGBachirIGaspardNLegrosBPepersackTEpileptic activities are common in older people with deliriumGeriatr Gerontol Int201414244745123910220
- NaeijeGDepondtCMeeusCKorpakKPepersackTLegrosBEEG patterns compatible with nonconvulsive status epilepticus are common in elderly patients with delirium: a prospective study with continuous EEG monitoringEpilepsy Behav201436182124836528
- Di PerriCStenderJLaureysSGosseriesOFunctional neuroanatomy of disorders of consciousnessEpilepsy Behav201430283224100252
- FisherRSCrossJHFrenchJAOperational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and TerminologyEpilepsia201758452253028276060
- ZemanAZBonifaceSJHodgesJRTransient epileptic amnesia: a description of the clinical and neuropsychological features in 10 cases and a review of the literatureJ Neurol Neurosurg Psychiatry19986444354439576532
- PanayiotopoulosCPThe Epilepsies: Seizures, Syndromes and ManagementOxfordshire, UKBladon Medical Publishing2005
- VillanuevaVSerratosaJMTemporal lobe epilepsy: clinical semiology and age at onsetEpileptic Disord200572839015929909
- WalkerMCSmithSJSisodiyaSMShorvonSDCase of simple partial status epilepticus in occipital lobe epilepsy misdiagnosed as migraine: clinical, electrophysiological, and magnetic resonance imaging characteristicsEpilepsia19953612123312367489701
- MeierkordHHoltkampMNon-convulsive status epilepticus in adults: clinical forms and treatmentLancet Neurol20076432933917362837
- LyketsosCGLopezOJonesBFitzpatrickALBreitnerJDekoskySPrevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the cardiovascular health studyJAMA2002288121475148312243634
- ClancyMJClarkeMCConnorDJCannonMCotterDRThe prevalence of psychosis in epilepsy; a systematic review and meta-analysisBMC Psychiatry2014147524625201
- KeableAFennaKYuenHMDeposition of amyloid beta in the walls of human leptomeningeal arteries in relation to perivascular drainage pathways in cerebral amyloid angiopathyBiochim Biophys Acta18622016510371046
- RamsayREMaciasFMRowanAJDiagnosing epilepsy in the elderlyInt Rev Neurobiol20078112915117433921
- PanayiotopoulosCPPrinciples of therapy in the epilepsiesA Clinical Guide to Epileptic Syndromes and Their TreatmentBerlinSpringer2010173235
- UkaiKWatanabeMTransient epileptic amnesia without epileptic seizures: proposal of a new entityPsychogeriatrics201717649149228345179