
Abstract
Objectives
It has been well documented that elevation of serum prolactin (PRL) level and weight gain are common in patients receiving treatment with atypical antipsychotics. The existing evidences show that serum PRL is elevated in schizophrenic patients treated with olanzapine. However, little is known about the long-term effects of olanzapine on PRL levels and weight gain in female patients with schizophrenia.
Materials and methods
This study addressed this issue by investigating the relationship between serum PRL level and body mass index (BMI). Seventy-nine female patients with first-episode schizophrenia were recruited and received olanzapine monotherapy for 12 weeks. Serum PRL level and BMI were measured at baseline and at 4, 8, 12 weeks. Thirty-five age-matched healthy female individuals were recruited as controls. The severity of psychiatric symptoms was evaluated using the Positive and Negative Syndrome Scale.
Results
The olanzapine treatment for 12 weeks significantly increased serum PRL (P<0.01) level and BMI (P<0.01). A positive correlation between the pre- and posttreatment changes in serum PRL level and BMI was observed (r=0.247, P=0.028).
Conclusion
Our findings suggest that PRL might conceivably modulate weight gain in female patients with schizophrenia receiving olanzapine treatment; however, the exact mechanism remains unclear.
Keywords:
Introduction
Schizophrenia is a chronic and debilitating psychiatric disorder characterized by positive and negative symptoms. Antipsychotics have been widely used to treat schizophrenia since first-generation antipsychotics (FGAs) were approved for clinical practice in the 1950s. Compared with FGAs, second-generation antipsychotics (SGAs) seem to have more pronounced clinical effects. Therefore, SGAs are currently preferentially prescribed to patients with schizophrenia.Citation1,Citation2
Olanzapine is a class of medications called atypical antipsychotics and is one of the most frequently prescribed SGAs.Citation3 However, olanzapine is known to induce weight gain. For example, a head-to-head meta-analysis reported that olanzapine causes the highest amount of weight gain.Citation4 Additionally, there is ample evidence showing that it is likely that a complex biological mechanism is involvedCitation5 and that neuroendocrine alternation may play an important role in olanzapine-induced weight gain.Citation6,Citation7
A major adverse effect of antipsychotics on the endocrine system is hyperprolactinemia that causes sexual dysfunction and galactorrhea. Clinical observations have shown that olanzapine induces elevated PRL concentrations in a dose-dependent manner and has less effect on PRL levels than other SGAs such as risperidone.Citation8–Citation10 However, subsequent studies have not reached a consensus.Citation11 One possible reason for this inconsistency is the neglect of gender differences in the research designs of related studies. There is evidence of gender-specific effects of olanzapine on PRL elevation in Japanese drug-naïve schizophrenia patients.Citation12 As such, gender difference needs to be taken into consideration when evaluating the effect of olanzapine on PRL elevation.Citation10 Although females are more prone to be affected by antipsychotic-induced hyperprolactinemia than males,Citation13 there is little literature reporting the trajectory of olanzapine-induced PRL elevation in females and its relationship with body mass index (BMI).
To address this issue, we carried out a 12-week longitudinal prospective study in female drug-naïve patients with first-episode schizophrenia under olanzapine monotherapy.
Materials and methods
Patients
All patients were Han Chinese and provided written informed consent before any study-related procedures were performed. All procedures were reviewed and approved by the Institution Review Board of Wenzhou Kangning Hospital. This study was performed in accordance with the guidelines laid out in the Declaration of Helsinki as revised in 1989.
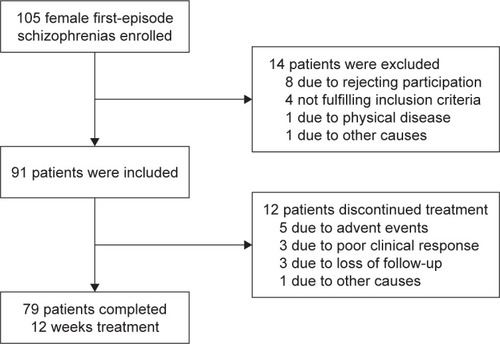
Ninety-one female first-episode drug-naïve (FEDN) inpatients were recruited at their initial evaluation for psychosis, shortly before antipsychotic treatment was started. The definition of the first episode was that patients had experienced their first-ever onset of psychotic symptoms. They were followed for about 12 weeks as inpatients after admission to establish a diagnosis of schizophrenia as per the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV). Diagnostic assessments were completed by two independent senior psychiatrists for each patients and confirmed with the Structured Clinical Interview for DSM-IV (SCID). For all subjects, a questionnaire survey was conducted by trained research staff to collect general information, demographic characteristics, and physical illness histories. Complete medical histories, physical examinations, and laboratory tests were collected from medical records and collateral resources. Patients who completed 12 weeks of follow-up were included in the analysis. Finally, a total of 79 female FEDN patients completed 12 weeks of treatment. The average age and education level of these patients were 34.30±8.88 and 8.97±3.14 years, respectively. The clinical subtypes were: paranoid=38 (48.1%), disorganized=31 (39.2%), residual=4 (5.1%), and undifferentiated=6 (7.6%). A flow diagram of study screening, enrollment, and reasons for termination is shown in .
Figure 1 Subject flow through the study of olanzapine.
From admission, all patients received three meals daily consisting of a balanced diet directly from the hospital and had the opportunity for one hour of physical exercise per day. All patients had similar food. During hospitalization, their family members or friends occasionally supplemented them with fruit or snacks. The patients in the present study could be considered a representative sample of institutionalized patients with schizophrenia in China.
Thirty-five healthy Han Chinese control subjects were recruited from the local community in Wenzhou city. Their current mental health status and personal or family history of mental disorders were assessed by unstructured interviews. None of the healthy control subjects had a personal or family history of psychiatric disorder.
Subjects with on-going allergies, infections, or a history of autoimmune disorders were excluded. Neither the schizophrenic patients nor the control subjects suffered from substance dependence or abuse other than of tobacco, received immunosuppressive drugs, or took medications for physical diseases. Furthermore, subjects who were pregnant or lactating were excluded.
Clinical measures
On the day when blood was sampled, the patient’s psychopathology was assessed with the Positive and Negative Syndrome Scale (PANSS) by one of the three psychiatrists. The psychiatrists had simultaneously attended a training session in the use of the PANSS before the study began. To ensure consistency and reliability of the PANSS ratings after training, the paired ratings of two psychiatrists for each patient assessment were compared at each of the repeated assessments during the study. In those comparisons, they maintained a correlation coefficient >0.8 on the PANSS total score.
Height was measured at enrollment, and body weight and BMI (weight/height) were collected following an overnight fast at baseline, and at the end of 4, 8, and 12 weeks. The same scale and the same wall-mounted height measurement device were used for the entire study. Body weight was taken with subjects wearing light clothing and no shoes, and after having emptied their pockets. All measurements were repeated three times for each patient, and mean values were reported. Olanzapine treatment was initiated at 5 mg/day and increased to ~20 mg/day after 2 weeks according to clinical judgments. Low doses of benzodiazepines were used if necessary. The baseline BMI data were collected from the FEDN patients at the initial evaluation for psychosis, shortly before antipsychotic treatment was started.
Serum PRL assay
Serum samples were collected from all participants between 7:00 AM and 9:00 AM following an overnight fast. Samples were taken at baseline and 4, 8, and 12 weeks after beginning olanzapine treatment. The serum was separated, aliquoted, and stored at −80°C until they were assayed.
Serum PRL was assayed using the standard of the Advia-Centaurs Chemiluminescence (Advia-Centaur CP, Siemens Healthcare Diagnostics, Germany) immunoassay method.Citation14 Each assay was run in duplicates. All samples were measured by the same investigator who was blind to the study. The inter- and intraassay coefficients of variation were 9% and 7%, respectively.
Statistical analysis
The normality of the data’s distribution was tested using Kolmogorov–Smirnov tests. All the demographic and clinical data, including BMI, were normally distributed (all P>0.05) in both patients and normal control subjects. Independent t-tests, ANOVAs, and chi-squared tests were carried out to compare the two groups in terms of basic sociodemographic and clinical characteristics. Data are presented as mean ± SD. Repeated measures multivariate analysis of covariance assessed changes in body weight, BMI, and serum PRL level between groups at 4, 8, and 12 weeks. Lastly, Pearson’s correlation coefficient was used to determine the association between serum PRL level change (pre- and posttreatment) and sociodemographic variables, especially PRL level change and BMI gain. Bonferroni corrections were applied to each test to adjust for multiple testing. All tests were two-tailed, with the significant level set at 0.05.
Results
Demographic data
shows the subjects’ demographic data. There was no significant difference between the patients and the healthy control subjects in terms of age, education, height, and weight. There were significant differences in BMI (P=0.004) and serum prolactin level (P=0.001). Mean weight and BMI gain in patients since recruitment were 5.63±4.01 kg and 2.20±1.56 kg/m2, respectively.
Table 1 Demographics of FEDN with schizophrenia and healthy controls
Serum PRL assay
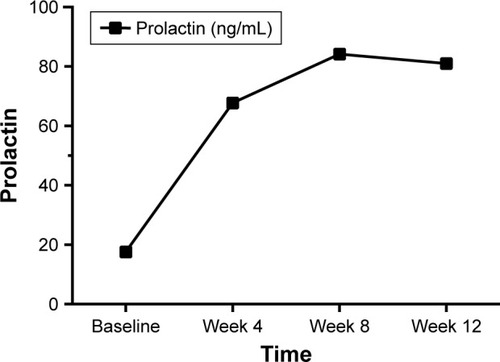
The initial serum PRL level in patients with schizophrenia was 17.61±2.28 ng/mL, significantly higher than that in healthy controls (12.12±3.08 ng/mL; P<0.001; ), and increased significantly to 67.70±47.45 ng/mL after treatment for 4 weeks, and to 84.14±47.70 ng/mL after treatment for 8 weeks. However, another 4 weeks’ treatment did not yield further increases in serum PRL level, although it remained significantly higher than at baseline ( and ).
Table 2 Weight-related, BMI and prolactin effects of olanzapine during 12 weeks of treatment
Figure 2 The change of prolactin during 12-week treatment with olanzapine.
Correlations between serum PRL and BMI gain
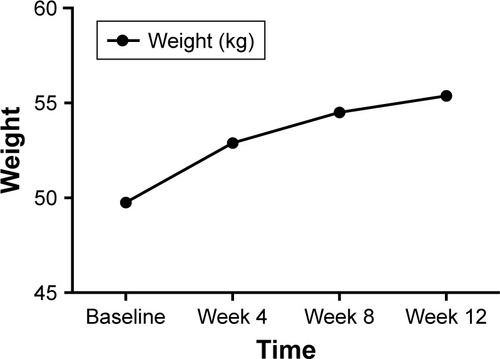
After 12 weeks of treatment, the average weight of patients increased to 55.37±7.20 kg, which was significantly higher than that at baseline (F=27.21, P<0.001), and the BMI was also significantly higher than that at baseline (F=25.07, P<0.001) ( and ).
Figure 3 The change of weight during 12 weeks treatment with olanzapine.
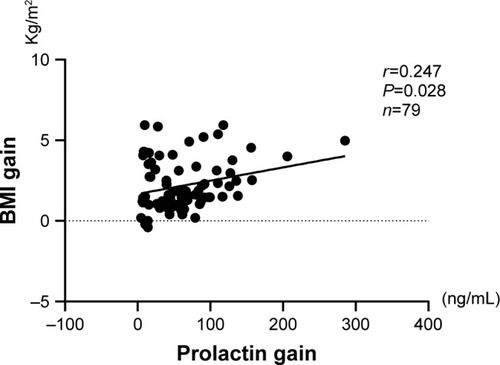
Regarding the correlation between serum PRL level change and sociodemographic variables, after Bonferroni correction for multiple testing, a significant positive relationship was found in BMI gain (r=0.247, P=0.028) and age (r=0.312, P=0.005). No relationship was noted between PRL change and education ().
Figure 4 The correlation between the increase of BMI and the change in serum prolactin at pre- and posttreatment with olanzapine.
Discussion
Olanzapine is an SGA with an orexigenic effect that induces serious metabolic problems in humans.Citation15 In this study, we observed that female patients with first-episode schizophrenia had significantly increased BMIs after 12 weeks of olanzapine monotherapy. This is consistent with most previous clinical and preclinical studies.Citation16,Citation17 In parallel with weight gain, the serum PRL levels in such patients also seemed to significantly increase. Early literature has documented that olanzapine elevates PRL levelsCitation11,Citation18–Citation20 in a dose-dependent manner.Citation21 Further analysis have shown that there was a correlation between the increases in BMI and PRL level.
It was reported that PRL may contribute to hyperphagia in females.Citation22 Early preclinical studies showed that exogenous PRL administration leads to increased food intake and weight gain in female rats.Citation23 Clinical observations also showed that hyperprolactinemia in humans may be associated with a high prevalence of obesity and that normalization of PRL levels could result in weight loss in 79% of prolactinomas patients.Citation24,Citation25 As such, our findings suggest that olanzapine-induced PRL elevation may conceivably modulate weight gain in females. Although most SGAs are associated with body weight gain, a meta-analysis indicated that olanzapine causes the highest weight gain in first-episode psychosis patients.Citation26 However, olanzapine produces a modest increase of PRL compared with other SGAs such as paliperidone and risperidone.Citation27 Therefore, PRL elevation may not fully explain the olanzapine-induced weight gain. Olanzapine is believed to work by its multiple-receptor-blocking profile. A recent study demonstrated that olanzapine causes weight gain by targeting serotonin receptor 2C (5-HT2C).Citation28 As such, our findings imply that PRL elevation may be a component of weight gain in olanzapine-treated patients. However, it remains unknown whether PRL contributes more to weight gain with paliperidone treatment than with olanzapine. Further studies are required to investigate these relationships.
Several studies have reported increased serum prolactin levels in FEDN schizophrenia patients.Citation29,Citation30 Recently, Aston et alCitation31 and Shrivastava and TamhaneCitation32 also concluded that elevated serum PRL levels at baseline might be preexisting in some drug-naïve patients with schizophrenia. High PRL levels at baseline could be used for long-term prognosis and psychopathology but are not indicators in the short term. Furthermore, a complicating issue in defining standard ranges for PRL levels is that they may depend on one or more biological or clinical factors, such as gender, age, BMI, nutrition, stress, exercise, sex-steroid concentrations, core temperature, and medications.Citation33
Some other studies found higher BMI in FEDN schizophrenia patients (compared to age-matched controls) after the first weeks of treatment but found no significant difference before medication.Citation34 The underlying mechanisms of weight gain are not completely understood. We speculate that several factors, such as differences in exercise load and intensity, nutrition intake, schizophrenia subtype, definitions of “drug-naïve,” or biological heterogeneity may be responsible for differences in baseline BMI and prolactin level.
Perhaps the dysfunction of the PRL level is more sensitive or more vulnerable than that of weight gain in the early course of schizophrenia illness. However, this is only our speculation and we cannot offer reasonable mechanisms that explain why PRL was associated with BMI in our first-episode schizophrenia patients. Further research is necessary to clarify the relationship between PRL, BMI, and the onset of schizophrenia.
The variability of prolactin and weight measurement was reduced in this study by processing all samples in a single batch. If different blood samples and subjects were assayed at different times or if significant random batch-to-batch variation were present, the reliability of the measurements would be somewhat lower than the values calculated here. By assaying all blood samples and subjects in the same batch, we avoided any systematic time trends in the assay results.
This study has several limitations. First, the small sample size might increase the possibility of type II errors and make it difficult to generalize the findings. Moreover, it is unfortunate that the control cohort was much smaller than the patient cohort, as this may lead to bias in the statistical analysis. Second, this study employed female patients with first-episode schizophrenia and, thus, our conclusions may not be generalized to the whole schizophrenia population. Third, we did not measure the duration of the untreated first-episode patients with schizophrenia in this study. This could also contribute to the high BMI and prolactin levels observed before treatment. Fourth, we did not include male patients with schizophrenia as a comparison group, which we suggest is the primary limitation. Fifth, we could not measure estrogen levels and menstrual cycles, which might be considered a limitation. Sixth, we did not demonstrate the number of children and pregnancies in the present study. Seventh, the study would be more interesting if other atypical and classical antipsychotic medications were included. Such research ought to be performed in the future.
Conclusion
We performed a prospective, open-label, 12-week observational study to investigate the effect of olanzapine mono-therapy on female patients with first-episode schizophrenia. Our findings provided evidence that prolactin might conceivably modulate weight gain in schizophrenia patients receiving olanzapine treatment; however, the exact mechanism remains unclear. Further investigations and replications are needed to provide more robust conclusions in this field.
Author contributions
FY drafted the manuscript, FY, LC, XF, KZ, CZhu, CX were responsible for clinical data collection and lab experiments. WT and CZha was responsible for study design and manuscript preparation. All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Acknowledgments
The authors are grateful to all participants. This study was supported by the Wenzhou Science and Technology Commission Foundation (Y20140426) and (Y20160103). The funding sources of this study had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
Disclosure
The authors report no conflicts of interest in this work.
References
- StroupTSMcEvoyJPSwartzMSThe National Institute of Mental Health Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) project: schizophrenia trial design and protocol developmentSchizophr Bull2003291153112908658
- BuckleyPFBroad therapeutic uses of atypical antipsychotic medicationsBiol Psychiatry2001501191292411743945
- SongWSChaJHYoonSHChoYSParkKYKimMHThe atypical antipsychotic olanzapine disturbs depotentiation by modulating mAChRs and impairs reversal learningNeuropharmacology201711411127866902
- Rummel-KlugeCKomossaKSchwarzSHead-to-head comparisons of metabolic side effects of second generation antipsychotics in the treatment of schizophrenia: a systematic review and meta-analysisSchizophr Res20101232–322523320692814
- KinonBJKaiserCJAhmedSRotelliMDKollack-WalkerSAssociation between early and rapid weight gain and change in weight over one year of olanzapine therapy in patients with schizophrenia and related disordersJ Clin Psychopharmacol200525325525815876905
- EversSSCalcagnoliFvan DijkGScheurinkAJOlanzapine causes hypothermia, inactivity, a deranged feeding pattern and weight gain in female Wistar ratsPharmacol Biochem Behav201097116316920570692
- EversSSBoersmaGJTamashiroKLScheurinkAJvan DijkGRoman high and low avoidance rats differ in their response to chronic olanzapine treatment at the level of body weight regulation, glucose homeostasis, and cortico-mesolimbic gene expressionJ Psychopharmacol201731111437145228892416
- MadhusoodananSParidaSJimenezCHyperprolactinemia associated with psychotropics – a reviewHum Psychopharmacol201025428129720521318
- FraguasDCorrellCUMerchán-NaranjoJEfficacy and safety of second-generation antipsychotics in children and adolescents with psychotic and bipolar spectrum disorders: comprehensive review of prospective head-to-head and placebo-controlled comparisonsEur Neuropsychopharmacol201121862164520702068
- SuzukiYFukuiNWatanabeJGender differences in the relationship between the risperidone metabolism and the plasma prolactin levels in psychiatric patientsProg Neuropsychopharmacol Biol Psychiatry20103471266126820621147
- SuzukiYSugaiTFukuiNDifferences in plasma prolactin levels in patients with schizophrenia treated on monotherapy with five second-generation antipsychoticsSchizophr Res20131451–311611923375624
- SawamuraKSuzukiYFukuiNSugaiTSomeyaTGender differences in prolactin elevation induced by olanzapine in Japanese drug-naïve schizophrenic patientsProg Neuropsychopharmacol Biol Psychiatry20063081511151416824658
- SmithSWheelerMJMurrayRO’KeaneVThe effects of antipsychotic-induced hyperprolactinaemia on the hypothalamic-pituitary-gonadal axisJ Clin Psychopharmacol200222210911411910254
- MargariLMateraEPetruzzelliMGProlactin variations during risperidone therapy in a sample of drug-naive children and adolescentsInt Clin Psychopharmacol201530210310825514607
- SkredeSGonzález-GarcíaIMartinsLLack of ovarian secretions reverts the anabolic action of olanzapine in female ratsInt J Neuropsychopharmacol201720121005101229020342
- ZhuYKrauseMHuhnMAntipsychotic drugs for the acute treatment of patients with a first episode of schizophrenia: a systematic review with pairwise and network meta-analysesLancet Psychiatry20174969470528736102
- DayabandaraMHanwellaRRatnatungaSSeneviratneSSuraweeraCde SilvaVAAntipsychotic-associated weight gain: management strategies and impact on treatment adherenceNeuropsychiatr Dis Treat2017132231224128883731
- SongXFanXZhangJProlactin serum levels correlate with inflammatory status in drug-naïve first-episode schizophreniaWorld J Biol Psychiatry201415754655224959913
- DruytsEEapenSWuPThorlundKThe risk of elevated prolactin levels in pediatric patients exposed to antipsychotics for the treatment of schizophrenia and schizophrenia spectrum disorders: protocol for a systematic review and meta-analysisSyst Rev2014311625312992
- PetrikisPTigasSTzallasATArchimandritiDTSkapinakisPMavreasVProlactin levels in drug-naïve patients with schizophrenia and other psychotic disordersInt J Psychiatry Clin Pract201620316516927334805
- SuzukiYOnoSSugaiTDose-dependent effects of olanzapine on QT intervals and plasma prolactin levels in Japanese patients with stable schizophreniaHum Psychopharmacol201126644044321823168
- NoelMBWoodsideBEffects of systemic and central prolactin injections on food intake, weight gain, and estrous cyclicity in female ratsPhysiol Behav19935411511548327594
- Gerardo-GettensTMooreBJSternJSHorwitzBAProlactin stimulates food intake in a dose-dependent mannerAm J Physiol19892561 Pt 2R276R2802912221
- GreenmanYTordjmanKSternNIncreased body weight associated with prolactin secreting pituitary adenomas: weight loss with normalization of prolactin levelsClin Endocrinol1998485547553
- NunesMCSobrinhoLGCalhaz-JorgeCSantosMAMauricioJCSousaMFPsychosomatic factors in patients with hyperprolactinemia and/or galactorrheaObstet Gynecol19805555915957189268
- TekCKucukgoncuSGuloksuzSWoodsSWSrihariVHAnnamalaiAAntipsychotic-induced weight gain in first-episode psychosis patients: a meta-analysis of differential effects of antipsychotic medicationsEarly Interv Psychiatry201610319320225962699
- LeuchtSCiprianiASpineliLComparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysisLancet2013382989695196223810019
- LordCCWylerSCWanRThe atypical antipsychotic olanzapine causes weight gain by targeting serotonin receptor 2CJ Clin Invest201712793402340628805659
- AlbayrakYBeyazyüzMBeyazyüzEKuloğluMIncreased serum prolactin levels in drug-naive first-episode male patients with schizophreniaNord J Psychiatry201468534134624094029
- ShrivastavaAJohnstonMBureauYShahNBaseline serum prolactin in drug-naïve, first-episode schizophrenia and outcome at five years: Is it a predictive factor?Innovat Clin Neurosci2012941721
- AstonJRechsteinerEBullNBorgwardtSGschwandtnerURiecher-RösslerAHyperprolactinaemia in early psychosis-not only due to antipsychoticsProg Neuropsychopharmacol Biol Psychiatry20103471342134420188136
- ShrivastavaATamhaneMSerum prolactin level and severity of psychopathology in patients of schizophreniaIndian J Psychiatry2000421485121407907
- RoelfsemaFPijlHKeenanDMVeldhuisJDProlactin secretion in healthy adults is determined by gender, age and body mass indexPLoS One201272e3130522363612
- HuangMYuLPanFA randomized, 13-week study assessing the efficacy and metabolic effects of paliperidone palmitate injection and olanzapine in first-episode schizophrenia patientsProg Neuropsychopharmacol Biol Psychiatry20188112213029097257