
Abstract
Background: The subgroup analysis of a primary study (NCT01051531) evaluated the effect of long-term paliperidone palmitate once-monthly (PP1M) therapy in Chinese patients with recent-onset schizophrenia responding unsatisfactorily to previous oral antipsychotics.
Patients and methods: This 18-month, open-label study consisted of 3 phases – screening (7 days), treatment (18 months) and end-of-study/withdrawal visit. All enrolled patients (18–50 years) received PP1M: 150 mg eq. (day 1), 100 mg eq. (day 8) followed by a once-monthly flexible dose (50, 75, 100 or 150 mg eq.). Efficacy and safety were assessed.
Results: Among the 118 enrolled Chinese patients, 68 completed the treatment (mean age: 25.6 years; male: 54.7%). A clinically meaningful change from baseline to day 548 was observed in Positive and Negative Syndrome scale (primary endpoint, mean [SD]: −15.3 [20.76]), Personal and Social Performance scale (15.9 [19.65]), Clinician Global Impression-schizophrenia score (−1.2 [1.54]) and Medication Satisfaction Questionnaire score (0.9 [1.73]). Commonly reported treatment-emergent adverse events (TEAEs) included insomnia (13.9%), injection-site pain (13.9%), upper respiratory tract infection (13.0%), restlessness (13.0%) and akathisia (13.0%). Serious TEAEs were reported in 9.3% patients with schizophrenia being most common (6.5%) and one death (suicide) was observed.
Conclusion: Efficacy of PP1M corroborate findings from earlier studies and no new safety concerns emerged in this Chinese subgroup of patients with schizophrenia.
Introduction
Schizophrenia, a mentally debilitating disease, is the leading cause of psychiatric disability in adults from China,Citation1 which results in considerable economic burden.Citation2 Approximately 40–60% of patients are partially or totally non-compliant to oral antipsychotic medication in less than a year of treatment.Citation3–Citation5 Although second-generation oral antipsychotics demonstrate lower side-effects as compared with the first-generation, the issue of non-adherence still persists.Citation6,Citation7 Poor medication adherence to oral antipsychotics is a primary predictor of relapse and hospitalizations.Citation8 High relapse rates are commonly observed among schizophrenia patients in the initial five years of diagnosis.Citation8,Citation9 Some factors contributing to inadequate medication adherence include complex medication regimen, irregular daily routine leading to missed doses or clinician’s lack of awareness on adherence.Citation10,Citation11
Long-acting injectables (LAIs) were designed to overcome these issues of non-adherence by decreasing the dosing frequency and signaling the clinician in the event of non-adherence by regular patient contact.Citation12 The LAIs were previously recommended when there was poor medication adherence or symptom exacerbation or in maintenance phase of therapy.Citation13–Citation15 The early phase of schizophrenia (initial 2 years up to 5 years) is an important period for intervention with implications on long-term prognosis to prevent schizophrenia-associated impairments and disabilities including relapse.Citation16 Recent guidelines recommend LAIs in all phases of schizophrenia including first-line therapy as well as the initial 2–5 years.Citation17–Citation19
Paliperidone palmitate once-monthly (PP1M) is an LAI with unique pharmacokinetics, wherein rapid therapeutic concentrations are attained post-initiation and the once-monthly dosing leads to sustained therapeutic effect. PP1M has been approved for the treatment of schizophrenia and schizoaffective disorder in various countries world-wide.Citation20 Studies have demonstrated efficacy and safety of PP1M in acute phase in schizophrenia patients from China,Citation21–Citation23 albeit limited information is present on the long-term maintenance therapy with PP1M in this population.Citation24
Cultural and ethnic variations in patients with schizophrenia have been widely acknowledged and are known to influence epidemiology, diagnosis, symptom expression and treatment outcomes.Citation25–Citation27 Differences in acceptability to antipsychotics and variances in efficacy and tolerability profiles of antipsychotics among Chinese patients with schizophrenia have been corelated with pharmacodynamic and pharmacokinetic inconsistencies and are known to have clinically relevant implications on prescription patterns in China.Citation28,Citation29 In addition, the influence of traditional herbal medicine, a prevalent practice in China and social stigma associated with psychiatric conditions, could potentially influence the course and outcomes of antipsychotic treatments.Citation26,Citation30,Citation31 The Chinese subgroup therefore represents a unique population with a high cultural impact. The primary study of the current subgroup analysis, a long-term, open-label, Phase 3b, Asia-Pacific (AP) study demonstrated significant clinical improvement and reduction in hospitalizations with PP1M therapy in patients who had recent-onset schizophrenia and had failed previous second-generation oral antipsychotics.Citation32 This analysis was carried out in the Chinese subgroup of schizophrenia patients from the primary study to identify long-term efficacy and safety of PP1M in this population.
Methods
Patients
This study included patients 18–50 years (both inclusive) of age, recently diagnosed (≤5 years) with schizophrenia (as per Diagnostic and Statistical Manual of Mental Disorders-4th edition [DSM-IV]). Detailed methodology of this study has been published previously.Citation32 Briefly, the key inclusion criterion was a history of unsuccessful treatment with oral antipsychotics and the key exclusion criterion was suspected psychiatric diagnosis due to drug abuse or medical conditions.
An Independent Ethics Committee or Institutional Review Board (all Independent Ethics Committees from China are listed in the Supplementary material) approved the study protocol at each study site. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. All patients provided written informed consent before study enrollment.
Study drug
The doses of PP1M are expressed as milligram equivalent (mg eq.) wherein pharmacologically active paliperidone: 75, 100 and 150 mg eq. correspond to 117, 156 and 234 mg of paliperidone palmitate, respectively. PP1M injections were supplied as aqueous extended-release suspensions for intramuscular injections in pre-filled syringes.
Study design
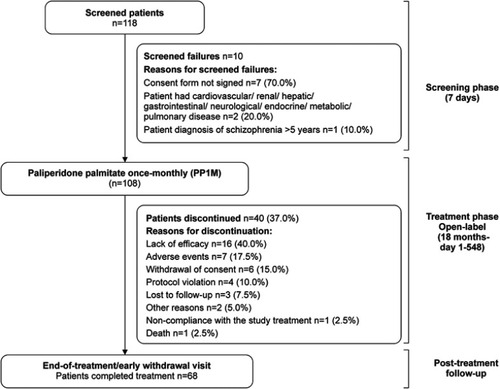
The current study was a subgroup analysis of an 18-month, multicenter, single-arm, open-label study conducted across AP region between April 2010 and May 2013.Citation32 Briefly, the study consisted of a screening phase of up to 7 days, an open-label treatment phase of 18 month (day 1 to day 548) and an end-of-study or early-withdrawal visit. The patients were administered PP1M: 150 mg eq. on day 1, 100 mg eq. on day 8 (both in deltoid muscle) followed by flexible doses of 50, 75, 100 or 150 mg eq. once-monthly (deltoid or gluteal muscle) ().
Figure 1 Study design and patient disposition.
Concomitant medications
Continuation of mood-stabilizing agents, anti-depressants, benzodiazepines (used for at least three months before the study) and lorazepam (0.5 mg up to 6 mg/day) were allowed in an open-label manner. Anti-cholinergic medications could be continued up to 8 weeks before tapering off at the investigator’s discretion.
Study outcomes
Efficacy assessments
The primary efficacy endpoint was change in Positive and Negative Syndrome Scale (PANSS) total score from baseline to the end-of-study (day 548) after switching from oral antipsychotics to PP1M. Secondary endpoints included the changes from baseline to the end of study in Personal and Social Performance (PSP) scale score including evolution of ratio of mild degree of dysfunction (PSP total score 71–100), varying degree of difficulty (31–70) and poor level of function (≤30); PANSS five factor scores; improvement, worsening and stable conditions in PANSS total scores; response rates for PANSS total score; symptom remission; overall score in global severity of illness (Clinical Global Impression-Schizophrenia [CGI-SCH] scale); Medication Satisfaction Questionnaire (MSQ, 7-point categorical scale); rate of patient discontinuation; rate of patients hospitalized during the study; total number of institutionalizations; institutionalizations in the retrospective (12 months before the initiation of PP1M) and prospective period (12 months after the initiation of PP1M); and dosage of injection.
Safety assessments
Safety assessments included continuous monitoring of treatment-emergent adverse events (TEAEs), physical examinations, vital signs measurements, clinical laboratory tests, body weight and evaluation of CGI of Movement Severity scale.
Statistical analysis
Similar to the sample size calculation for the AP study,Citation32 to detect a difference of 3 units in the PANSS total score with 90% power, assuming a drop-out rate of 20%, a total of 587 patients were recruited. Since only 118 patients were expected to be enrolled in China, this subgroup analysis was not sufficiently powered. Hence, statistical tests were not performed, and the data are presented descriptively. The number of institutionalizations in the retrospective and prospective periods (day 1 to 6 months and day 1 to 12 months) were compared using the mirror-analysis method. Both primary and secondary efficacy analyses were performed on the intent-to-treat (ITT) population that included all the patients who received at least one PP1M injection. The safety analysis set comprised of all patients in the ITT population.
Results
Patient disposition and characteristics
A total of 118 patients from China were enrolled in the study. Of the total ITT population (n=108), 68 patients (63.0%) completed the study. Among the discontinued patients (n=40), the most common reason for early termination from the study was the lack of efficacy (n=16) followed by TEAEs (n=7) and withdrawal of consent (n=6) (). Among the patients who withdrew due to lack of efficacy, 68.8% withdrew without a schizophrenia-related TEAE.
Prior to study enrollment, this Chinese subgroup of patients were on oral antipsychotics, with risperidone, olanzapine, paliperidone and sulpiride being most commonly used (). The most frequent diagnosis was paranoid type schizophrenia (61.1%). The mean time since the first diagnosis of disease was 2.0 years and most of the patients (69.4%) were diagnosed within three years prior to study enrollment (). Concomitant medications were used by 75.9% patients and antipsychotics (50.9%) were reported as the most commonly administered agents followed by diazepines, oxazepines, thiazepines, oxepines (combined, 15.7%); indole derivatives (7.4%) and benzamides (5.6%). A mean (SD) of 14.7 (6.41) PP1M doses were administered over a period of 412.2 (196.42) days in this Chinese patient subgroup.
Table 1 Patient demographics and baseline characteristics (intent-to-treat population)
Efficacy findings
Primary efficacy endpoint
At the end of treatment (day 548), a significant and clinically meaningful improvement from baseline in the PANSS total score was observed in these patients (mean [SD]: −15.3 [20.76], 95% CI=−19.3; −11.4) ().
Table 2 Efficacy parameters (LOCF; intent-to-treat population)
Secondary efficacy endpoints
Significant and clinically meaningful improvements in the PSP total score, PANSS five factor scores, CGI-SCH four symptoms and overall severity scores and MSQ score from baseline to the end of treatment (day 548) were observed (). A considerable proportion of patients exhibited an improvement in the PANSS total score and symptom remission from baseline to day 548 (). Only 0.9% of patients who were in remission at baseline did not achieve symptom remission at day 548. Also, the percentage of patients achieving a response (≥30% improvement from baseline in the PANSS total score) increased with each successive visit (). Notably, the percentage of patients with hospitalization in this study was 7.4%. The Kaplan Meier estimates for institutionalization due to psychiatric reasons was 6.5% (). The mirror-analysis revealed that the percentage of patients institutionalized in the 12-month period post PP1M therapy was lower (ie, 6.5% as compared to 37%) than that in the retrospective period ().
Safety findings
In this study, 90.7% of patients experienced at least one TEAE, and 9.3% of patients experienced at least one serious TEAE (). The most common TEAEs (>2% patients) included injection-site pain, insomnia, upper respiratory tract infection, nasopharyngitis and dizziness. The most commonly reported serious TEAE (≥5% patients) was schizophrenia exacerbation. One incidence of death (0.9%, 1/108) due to suicide was also observed in this subgroup and was not considered to be related to PP1M by the investigator. Thirteen patients had TEAEs that led to discontinuation from treatment or premature withdrawal, with the most common reason being worsening of schizophrenia. Also, TEAEs occurred more frequently in the first three months for the patients who tapered off prior antipsychotic medications during the study compared with patients without any concomitant use of antipsychotics (60.2% vs 17.6%). Incidence of depression, muscle rigidity, musculoskeletal stiffness and salivary hypersecretion were not observed in this study.
Table 3 Summary of treatment-emergent adverse events (safety analysis set)
Prolactin-related TEAEs were reported in 15.7% patients and were more commonly reported in women (30.4%) than in men (4.8%). Menstrual disorder was the most common prolactin-related TEAE (9.3%). Glucose-related TEAEs were less frequently reported (0.9%) and extrapyramidal symptom (EPS) TEAEs were observed in 41.7% patients. The most common EPS TEAEs included akathisia, restlessness and tremor. A mean [SD] weight gain of 4.3 [7.30] kg from baseline was observed () and an increase of ≥7% in body weight from baseline was observed in 42.0% patients. A significant reduction in CGI of Movement Severity score (mean [SD]: −0.2 [0.80], 95% CI: −0.4; −0.1) involving Parkinsonism was also observed. No clinically relevant changes in the vital signs were observed in this study.
Discussion
Patients from the AP region with recent-onset schizophrenia, who had failed previous oral antipsychotics, responded favorably to 18 months of PP1M therapy.Citation32 The current subgroup analysis of Chinese patients from the AP study also demonstrated improvements in symptoms (PANSS and PANSS five factor), function (PSP), clinical status (CGI-SCH) and medication satisfaction (MSQ) along with a decrease in the hospitalizations and institutionalizations in this longest study (18 months) carried out in this population. Overall, the efficacy endpoints improved in Chinese subgroup, similar to the total AP group.Citation32
The data on hospitalizations and institutionalizations in the course of PP1M LAI therapy is limited.Citation33 Institutionalizations are also indicators for assessment of health care resource utilization. A mirror-design analysis,Citation32 that closely resembles the real-world scenario, was employed in the current study to understand the changes between institutionalizations in the retrospective period versus the prospective period post PP1M therapy. The institutionalizations reduced considerably in the 12-month period of therapy as compared with the retrospective period (37.0% vs 6.5%) in this study. Observations from the current study combined with data from other recent real-world observations in naturalistic clinical settings revealed very low rates of new hospitalization with 12-month PP1M therapy,Citation34 suggesting that a lowered direct health care cost may be expected as a benefit of long-term PP1M therapy.Citation35
Previously, two separate studies were conducted with PP1M treatment in recent-onset schizophrenia patients from China with a therapy duration of 3 monthsCitation23 and 6 months.Citation24 A reduction in PANSS total score, improvement in PSP score and change in MSQ score from baseline was observed in the 3-month (mean [SD]; −30.9 [19.51], 19.3 [16.30] and 1.1 [1.6]), 6-month (−29.0 [18.77], 14.9 [15.04] and 0.8 [1.42]) and the current 18-month study (−15.3 [20.76], 15.9 [19.65] and 0.9 [1.73]).Citation23,Citation24 This sustained pattern of evidence observed across the different durations of therapy with respect to efficacy and patient satisfaction, support the relevance of PP1M in the initiation and maintenance therapy of recent-onset schizophrenia in Chinese patients.
No new safety signals were observed in the Chinese subgroup. The increase in TEAE instances (32.1%, 51.3% and 90.7%) and weight gain (7.8%, 28.6% and 42.0%) in the 3-, 6- and 18-month study could be attributed possibly to the increased duration of therapy.Citation23,Citation24 The EPS-related TEAEs were noted to have the highest occurrence among all TEAEs in the 3-, 6- and the current 18-month study.Citation22,Citation28 Of note, the prolactin-related TEAEs (11.6% vs 15.7%) and glucose-related TEAEs (0.6% vs 0.9%) were comparable between the 6- and current 18-month study.Citation24 Although there was an increase in the occurrence of TEAEs in the current study, treatment satisfaction for PP1M therapy among patients was similar to the previous studies.Citation23,Citation24 Death due to suicide was reported in one 19-year-old woman in the Chinese subgroup and the incident was not attributed to PP1M treatment by the investigator. It is estimated that 20% to 40% of individuals with schizophrenia have a lifetime risk of attempting suicide and as compared to the general population, individuals afflicted with schizophrenia have an 8.5-fold greater risk of suicide.Citation36–Citation39 The prevalence pattern of schizophrenia and suicides due to schizophrenia has been observed to be unique in China and Chinese women are at a higher risk than men, a reverse of what is observed in other global populations. A high suicide rate of 6.8 per 1000 people per year has been reported among individuals with schizophrenia from China, with a relative risk of 23.8 (95% CI: 18.8; 30.2) in patients with schizophrenia versus those without.Citation26
The current study was limited by the open-label nature of its design in that it may have influenced the patient-reported outcomes and clinician ratings of the patients. Additionally, due to the small sample size, the study was not sufficiently powered to perform statistical analysis. Hence, future studies with a larger sample size including placebo or active comparators (other LAIs or oral antipsychotics) could be conducted to confirm the long-term efficacy and safety findings. Treatment adherence is monitored closely during the course of a clinical trial; however, similar adherence may not be achieved in real world, long-term treatment.
Conclusion
To summarize, PP1M showed a consistent efficacy profile, corroborating the overall AP population and no new safety findings were observed in this subgroup of Chinese patients with schizophrenia who had previously failed oral antipsychotics. The number of patients hospitalized was notably low and the duration of hospitalization in these patients reduced following 18 months of treatment with PP1M.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
Sonia Philipose, PhD and Priya Ganpathy, MPharm, ISMPP CMPP™ (SIRO Clinpharm Pvt. Ltd.) provided writing assistance and Harry Ma, PhD (Janssen Global Services, LLC) provided additional editorial support for this manuscript. The authors also thank the study participants, without whom this study would never have been accomplished, and the investigators for their participation in this study. This study was supported by funding from Janssen-Cilag Asia-Pacific Medical Affairs, Johnson & Johnson Pvt. Ltd.
Disclosure
The study presented in this report is supported by Janssen Research and Development, People’s Republic of China. Dr Si has been a consultant and/or advisor to Janssen Research and Development (Beijing); Pfizer, Lundbeck and Otsuka. She received honoraria and/or grant support from Janssen Research and Development (Beijing), Lundbeck, Pfizer and Otsuka. Drs Zhang, Hong and Lu are employees of Xi’an Janssen Pharmaceuticals, Dr Zhuo is an employee of Johnson & Johnson (China) Investment Ltd., and Dr. Feng is an employee of Janssen Pharmaceutical Companies of Johnson and Johnson, Singapore. The authors report no other conflicts of interest in this work.
Supplementary material
List of institutional review boards and ethics committees from China
Table S1 Antipsychotics taken by patients prior to study enrollment (Chinese subgroup)
References
- Li N, Chen G, Du W, Song X, Zhang L, Zheng X. Population-level prevalence estimate and characteristics of psychiatric disability among Chinese adults. J Psychiatr Res. 2011;45(11):1530–1534. doi:10.1016/j.jpsychires.2011.07.00121794875
- Zhai J, Guo X, Chen M, Zhao J, Su Z. An investigation of economic costs of schizophrenia in two areas of China. Int J Ment Health Syst. 2013;7(1):26. doi:10.1186/1752-4458-7-2624237846
- Miller BJ. A review of second-generation antipsychotic discontinuation in first-episode psychosis. J Psychiatr Pract. 2008;14(5):289–300. doi:10.1097/01.pra.0000336756.65308.8318832960
- Miller BJ, Bodenheimer C, Crittenden K. Second-generation antipsychotic discontinuation in first episode psychosis: an updated review. Clin Psychopharmacol Neurosci. 2011;9(2):45–53. doi:10.9758/cpn.2011.9.2.4523429653
- Novick D, Haro JM, Suarez D, Perez V, Dittmann RW, Haddad PM. Predictors and clinical consequences of non-adherence with antipsychotic medication in the outpatient treatment of schizophrenia. Psychiatry Res. 2010;176(2–3):109–113. doi:10.1016/j.psychres.2009.05.00420185182
- Leucht S, Corves C, Arbter D, Engel RR, Li C, Davis JM. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373(9657):31–41. doi:10.1016/S0140-6736(08)61764-X19058842
- Nakonezny PA, Byerly MJ. Electronically monitored adherence in outpatients with schizophrenia or schizoaffective disorder: a comparison of first- vs. second-generation antipsychotics. Schizophr Res. 2006;82(1):107–114. doi:10.1016/j.schres.2005.10.01516376522
- Ascher-Svanum H, Zhu B, Faries DE, et al. The cost of relapse and the predictors of relapse in the treatment of schizophrenia. BMC Psychiatry. 2010;10:2. doi:10.1186/1471-244X-10-220059765
- Weiden PJ, Olfson M. Cost of relapse in schizophrenia. Schizophr Bull. 1995;21(3):419–429.7481573
- Olivares JM, Pinal B, Cinos C. Comparison of long-acting antipsychotic injection and oral antipsychotics in schizophrenia. Neuropsychiatry. 2011;1(3):275–289. doi:10.2217/npy.11.24
- Patel MX, David AS. Why aren‘t depot antipsychotics prescribed more often and what can be done about it? Adv Psychiatric Treat. 2005;11(3):203–211. doi:10.1192/apt.11.3.203
- Agid O, Foussias G, Remington G. Long-acting injectable antipsychotics in the treatment of schizophrenia: their role in relapse prevention. Expert Opin Pharmacother. 2010;11(14):2301–2317. doi:10.1517/14656566.2010.49912520586707
- Hasan A, Falkai P, Wobrock T, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, part 2: update 2012 on the long-term treatment of schizophrenia and management of antipsychotic-induced side effects. World J Biol Psychiatry. 2013;14(1):2–44. doi:10.3109/15622975.2012.73970823216388
- Kuipers E, Yesufu-Udechuku A, Taylor C, Kendall T. Management of psychosis and schizophrenia in adults: summary of updated NICE guidance. BMJ. 2014;348:g1173. doi:10.1136/bmj.g117324523363
- Takeuchi H, Suzuki T, Uchida H, Watanabe K, Mimura M. Antipsychotic treatment for schizophrenia in the maintenance phase: a systematic review of the guidelines and algorithms. Schizophr Res. 2012;134(2–3):219–225. doi:10.1016/j.schres.2011.11.02122154594
- Birchwood M, Todd P, Jackson C. Early intervention in psychosis. The critical period hypothesis. Br J Psychiatry Suppl. 1998;172(33):53–59.9764127
- Llorca PM, Abbar M, Courtet P, Guillaume S, Lancrenon S, Samalin L. Guidelines for the use and management of long-acting injectable antipsychotics in serious mental illness. BMC Psychiatry. 2013;13:340. doi:10.1186/1471-244X-13-34024359031
- Malla A, Tibbo P, Chue P, et al. Long-acting injectable antipsychotics: recommendations for clinicians. Can J Psychiatry. 2013;58(5Suppl 1):30S–35S.23945065
- Moore TA, Buchanan RW, Buckley PF, et al. The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia: 2006 update. J Clin Psychiatry. 2007;68(11):1751–1762.18052569
- Newton R, Hustig H, Lakshmana R, et al. Practical guidelines on the use of paliperidone palmitate in schizophrenia. Curr Med Res Opin. 2012;28(4):559–567. doi:10.1185/03007995.2012.66536222321007
- Zhang L, Li J, Zhao Y, Su Y, Si T. Critical evaluation of paliperidone in the treatment of schizophrenia in Chinese patients: a systematic literature review. Neuropsychiatr Dis Treat. 2016;12:113–131. doi:10.2147/NDT.S6467226811684
- Li H, Turkoz I, Zhang F. Efficacy and safety of once-monthly injection of paliperidone palmitate in hospitalized Asian patients with acute exacerbated schizophrenia: an open-label, prospective, noncomparative study. Neuropsychiatr Dis Treat. 2016;12:15–24. doi:10.2147/NDT.S8365126730193
- Si T, Zhang K, Tang J, et al. Efficacy and safety of flexibly dosed paliperidone palmitate in Chinese patients with acute schizophrenia: an open-label, single-arm, prospective, interventional study. Neuropsychiatr Dis Treat. 2015;11:1483–1492. doi:10.2147/NDT.S8176026150719
- Zhao J, Li L, Shi J, et al. Safety and efficacy of paliperidone palmitate 1-month formulation in Chinese patients with schizophrenia: a 25-week, open-label, multicenter, phase IV study. Neuropsychiatr Dis Treat. 2017;13:2045–2056. doi:10.2147/NDT.S13122428814873
- Chang N, Newman J, D‘Antonio E, McKelvey J, Serper M. Ethnicity and symptom expression in patients with acute schizophrenia. Psychiatry Res. 2011;185(3):453–455. doi:10.1016/j.psychres.2010.07.01920705345
- Phillips MR, Yang G, Li S, Li Y. Suicide and the unique prevalence pattern of schizophrenia in mainland China: a retrospective observational study. Lancet. 2004;364(9439):1062–1068. doi:10.1016/S0140-6736(04)17061-X15380965
- Robinson DG, Schooler NR, John M, et al. Prescription practices in the treatment of first-episode schizophrenia spectrum disorders: data from the national RAISE-ETP study. Am J Psychiatry. 2015;172(3):237–248. doi:10.1176/appi.ajp.2014.1310135525727536
- Bai Z, Wang G, Cai S, et al. Efficacy, acceptability and tolerability of 8 atypical antipsychotics in Chinese patients with acute schizophrenia: a network meta-analysis. Schizophr Res. 2017;185:73–79. doi:10.1016/j.schres.2017.01.00228108226
- Ng CH, Chong SA, Lambert T, et al. An inter-ethnic comparison study of clozapine dosage, clinical response and plasma levels. Int Clin Psychopharmacol. 2005;20(3):163–168.15812267
- Haraguchi K, Maeda M, Mei YX, Uchimura N. Stigma associated with schizophrenia: cultural comparison of social distance in Japan and China. Psychiatry Clin Neurosci. 2009;63(2):153–160. doi:10.1111/j.1440-1819.2009.01922.x19335384
- Wei YY, Lin WF, Zhang TH, Tang YX, Wang JJ, Zhong MF. Effectiveness of traditional Chinese medicineas as an adjunct therapy for refractory schizophrenia: a systematic review and meta analysis. Sci Rep. 2018;8(1):6230. doi:10.1038/s41598-018-24547-029670200
- Zhang F, Si T, Chiou CF, et al. Efficacy, safety, and impact on hospitalizations of paliperidone palmitate in recent-onset schizophrenia. Neuropsychiatr Dis Treat. 2015;11:657–668. doi:10.2147/NDT.S7777825792835
- Nasrallah HA. The case for long-acting antipsychotic agents in the post-CATIE era. Acta Psychiatr Scand. 2007;115(4):260–267. doi:10.1111/j.1600-0447.2006.00982.x17355516
- Emsley R, Hargarter L, Bergmans P, et al. Once-monthly paliperidone palmitate in early stage schizophrenia – a retrospective, non-interventional 1-year study of patients with newly diagnosed schizophrenia. Neuropsychiatr Dis Treat. 2017;13:2261–2269. doi:10.2147/NDT.S14263428919757
- Chiou CF, Wang BC, Caldwell R, et al. The cost reduction in hospitalization associated with paliperidone palmitate in the People‘s Republic of China, Korea, and Malaysia. Neuropsychiatr Dis Treat. 2015;11:1989–1994. doi:10.2147/NDT.S8672226346330
- Altamura AC, Bassetti R, Bignotti S, Pioli R, Mundo E. Clinical variables related to suicide attempts in schizophrenic patients: a retrospective study. Schizophr Res. 2003;60(1):47–55.12505137
- Kasckow J, Felmet K, Zisook S. Managing suicide risk in patients with schizophrenia. CNS Drugs. 2011;25(2):129–143. doi:10.2165/11586450-000000000-0000021254789
- Pompili M, Amador XF, Girardi P, et al. Suicide risk in schizophrenia: learning from the past to change the future. Ann Gen Psychiatry. 2007;6:10. doi:10.1186/1744-859X-6-1017367524
- Suokas JT, Perala J, Suominen K, Saarni S, Lonnqvist J, Suvisaari JM. Epidemiology of suicide attempts among persons with psychotic disorder in the general population. Schizophr Res. 2010;124(1–3):22–28. doi:10.1016/j.schres.2010.09.00920934306