
Abstract
Background: The goal of this study was to identify the physiological factors related to the blood concentration of lithium in Chinese Han patients with bipolar disorder (BD).
Materials and methods: A total of 186 Chinese Han patients with BD were assessed. Patients were recruited from the Anhui Mental Health Center. The concentrations of serum lithium were measured by a Dimension RxL Max biochemistry analyzer. Physiological factors, including body weight, body mass index (BMI), and routine laboratory parameters, were collected. Relationships between the serum lithium concentration and relevant clinical data were analyzed by Pearson correlation tests, and the independent relationships were determined by multivariate linear regression analysis.
Results: Pearson correlation analysis showed that serum lithium concentrations were positively correlated with creatinine concentrations (r=0.147, P=0.046), Mg2+ concentrations (r=0.151, P=0.04), and the percentage of neutrophils (r=0.178, P=0.015) and negatively correlated with high-density lipoprotein (HDL) concentrations (r=−0.142, P=0.05), apolipoprotein A1 concentrations (r=−0.169, P=0.02), and Na+ concentrations (r=−0.148, P=0.046) in 186 patients with BD. Furthermore, multivariate linear regression analysis showed that serum lithium concentrations were negatively associated with Na+ concentrations and positively associated with the percentage of neutrophils.
Conclusion: These results suggest that physiological factors, including creatinine, HDL, apolipoprotein A1, Na+, and Mg2+ concentrations and percentage of neutrophils, might be related to serum lithium concentrations and provide a basis for parameter selection of lithium population pharmacokinetics in Chinese Han patients with BD.
Introduction
Bipolar disorder (BD), a chronic, severe, and highly disabling psychiatric illness, is among the leading causes of disability, giving rise to tremendous health-care costs and affecting more than 1% of the general population irrespective of nationality, ethnic origin, or socioeconomic status.Citation1 Lithium is still a first-line treatment for BD,Citation2 even though individual response is variable. Given that lithium has a narrow therapeutic index, therapeutic drug monitoring for determining serum lithium concentrations and exploring factors related to lithium blood concentrations remain the key components of clinical surveillance.Citation3
Over the past two decades, China has experienced rapid socio-economic changes, accompanied by social problems, such as the rapid rise in health care costs, the rise in divorce rates, the weakening of family relations, the massive migration of temporary jobs to urban areas and the widening poverty gap.Citation4 These problems generally affect mental health, especially emotional disorders including BD. It has been reported that the 12-month and lifetime prevalence of Chinese BD were 0.17% and 0.11%, respectively.Citation5 Chinese populations make up around one fifth of the total world and the Han nationality accounts for 92% of the total population. Taken together the fact that lithium is a first-line treatment for BD in China and the study on relative factors of blood lithium has not been widely reported in Chinese Han population, it was important and necessary to investigate the factors related to lithium blood concentrations in Chinese Han patients with BD.
The current study has suggested that body size, age and renal function are associated with lithium clearance.Citation6 Further study showed that lower lithium clearance could be attributed to the loss of fluid and sodiumions (Na+).Citation7 Additionally, most drug interactions with lithium are associated with changes in fluid or Na+ balance.Citation8 However, the factors relating the concentration of blood lithium are still incompletely understood and remain controversial, especially in Chinese Han patients with BD.
Pharmacokinetic studies showed that lithium is mainly excreted by glomerular filtration,Citation9 and it is speculated that the significant predictors of lithium clearance identified in most studies were related to renal function, such as glomerular filtration rate (GFR).Citation6,Citation10 However, there are few studies on the relationship between blood lithium concentration and renal function. Therefore, correlations between endogenous markers of GFR (urea nitrogen and creatinine) and serum lithium concentration were observed in the present study.
There is growing evidence that lipid alterations play an important role in the pathophysiology of BD.Citation11 As a valuable first-line treatment for BD, lithium was considered to affect lipid alterations. In agreement with this notion, it has been reported that the serum levels of apolipoprotein A1, a major component of the high-density lipoprotein (HDL) complex, were decreased in patients with BD but can be restored to control levels under lithium treatment.Citation12 Moreover, animal experiments showed that serum enzyme levels of HDL were reduced significantly in lithium-treated rats, depicting the disturbed general physiological status.Citation13 These findings suggest that concentrations of serum lithium may be related to lipid metabolism.
Recent studies have shown a link between blood lithium and electrolyte imbalance. The results of a case report demonstrated that blood lithium concentrations may be increased by a high-sodium diet.Citation14 Nephrogenic diabetes insipidus, the most common adverse effect of lithium, occurs in up to 40% of patients receiving lithium treatment.Citation15 Renal lithium toxicity, characterized by increased water and sodium diuresis, can result in insufficient blood volume, hypernatremia, hyperchloremic metabolic acidosis and distal tubular acidosis.Citation15 Thus, whether the concentration of electrolytes in the blood could relate the lithium concentration was investigated in the present study.
Lithium carbonate was successfully used to treat drug (including paliperidoneCitation16 and clozapineCitation17)-induced leukopenia and neutropenia, indicating a correlation between lithium and changes in the hemogram. Therefore, the association between the concentration of lithium and the hemogram was also investigated.
Considering the potential relationships between blood lithium and renal function, lipid alterations, electrolyte imbalance, and hemogram changes, the current retrospective study sought to identify whether the above physiological factors could influence the serum lithium concentration in Chinese Han patients with BD.
Materials and methods
Subjects
This study was conducted at Hefei Fourth People’s Hospital, Anhui Mental Health Center, between May 2018 and January 2019. Psychiatric diagnosis was established through an International Classification of Diseases 10th Revision (ICD-10) criteria-based structured clinical interview by skilled clinicians. A total of 610 subjects with BD were screened by an experienced researcher, and 186 patients were selected from the above patients. The criteria for joining the group were as follows: (1) age 18–65 years; (2) no use of antipsychotic, antimanic, antidepressant or antianxiety drugs for at least two weeks before admission or not undergone a washout period of at least five half-lives of the above drugs; (3) no serious physical diseases, such as acute or chronic nephritis, cardiovascular disease, acute infection, or central nervous system diseases; and (4) written informed consent to participate in the study. Evidence of clinically significant medical problems through medical history, laboratory workup, and physical examination that evaluated for serious physical diseases, such as acute or chronic nephritis, cardiovascular disease, acute infection, or central nervous system diseases was exclusionary for participation. summarizes the recruitment process. In accordance with the principles of the Declaration of Helsinki, all subjects provided informed written consent prior to participation. The Ethics Committee of Hefei Fourth People’s Hospital, Anhui Mental Health Center, approved this study.
Figure 1 Flowchart of the recruitment of participants.

Collection of relevant clinical data
A demographics questionnaire was used to collect general information about participants, such as sex, body weight, body mass index (BMI), and routine laboratory parameters, including biochemical indexes and clinical parameters. The biochemical indexes and clinical parameters were measured by a COBAS 8000 modular analyzer (Roche Diagnostics) and a Siemens ADVIA 2120i hematology analyzer (Siemens Healthcare Diagnostics Inc., Dublin, Ireland), respectively.
The biochemistry indexes were as follows: total bilirubin (TBIL), direct bilirubin (DBIL), total protein (TP), albumin,globulin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), γ-glutamyl transpeptidase (γ-GT), total bile acid (TBA), total cholesterol (TC), HDL, triglyceride (TG), apolipoprotein A1, apolipoprotein B, blood urea nitrogen (BUN), creatinine (CRE), uric acid, K+, Na+, Cl−, Ca2+, creatine kinase (CK), glucose, and Mg2+.
The clinical parameters were as follows: white blood cell (WBC) count, neutrophil percentage, lymphocyte percentage, monocyte percentage, basophilic percentage, eosinophil percentage, number of neutrophils, number of lymphocytes, number of monocytes, number of eosinophils, number of basophils, number of red blood cells (RBCs), hemoglobin (HB) concentration, packed cell volume (PCV), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), red cell distribution width coefficient of variation (RDW-CV), number of platelets, mean platelet volume (MPV), platelet distribution width (PDW), and platelet crit (PCT).
Detection of blood lithium concentration
The elimination half-life of lithium averages approximately 20–24 hrs, and steady-state concentrationsare reached after 5–7 days.Citation6,Citation18 Therefore, the steady-state blood lithium concentration was measured after administration of oral lithium carbonate 1.0 g/d for 1 week. Blood samples were taken from the participants’ veins at 5:00 a.m. All subjects were fasted prior to blood collection. Dry tubes without any additives were used for collecting the samples. The blood samples were immediately centrifuged at 3,000 rpm for 5 min at 4 °C. The extracted supernatant was collected as a serum sample. The concentration of lithium in the serum was measured using a biochemical analyzer (Dimension RxL Max, SIEMENS Company, Germany) according to the manufacturer’s instructions. Reagents (Lithium Flex reagent cartridge, lot: BA9101) were supplied by SIEMENS Company.
Statistical analysis
Data were analyzed using SPSS version 17.0 statistical analysis software (SPSS, Chicago, IL). Distribution of the data was determined by the Kolmogorov-Smirnov test. Relationships between the serum lithium concentration and relevant clinical data were analyzed using Pearson correlation tests, and multiple linear regression analysis was utilized to identify the factors including the creatinine, HDL, apolipoprotein A1, Na+, Mg2+ concentrations, and percentage of neutrophils related to the serum lithium concentrations. Quantitative data are reported as the means ± standard deviation (SD). A P-value of <0.05 was considered indicative of statistical significance.
Results
One hundred and eighty-six Chinese Han patients with BD were enrolled. The demographic characteristics and routine laboratory parameters of all the subjects are shown in .
Table 1 Distribution of independent variables measured from 186 patients with BD
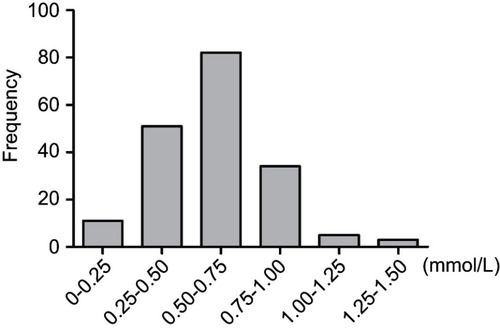
shows the distribution of the serum lithium concentration in patients with BD. These data ranged from 0.11 to 1.34 (mean =0.60, SD=0.23) mmol/L.
Figure 2 Histogram of resulting lithium concentration in 186 patients with bipolar disorder.
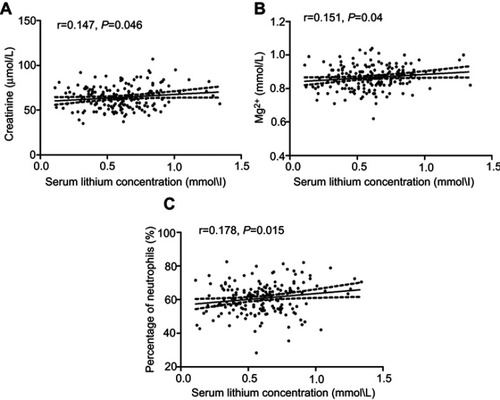
As shown in , the results of the Pearson correlation analysis showed that serum lithium concentrations were positively correlated with creatinine concentrations (r=0.147, P=0.046; ), Mg2+ concentrations (r=0.151, P=0.04; ), and the percentage of neutrophils (r=0.178, P=0.015; ) in 186 patients with BD.
Figure 3 Positive correlations between serum lithium concentration and creatinine (A), Mg2+ (B) concentrations, and percentage of neutrophils (C) in 186 patients with bipolar disorder.
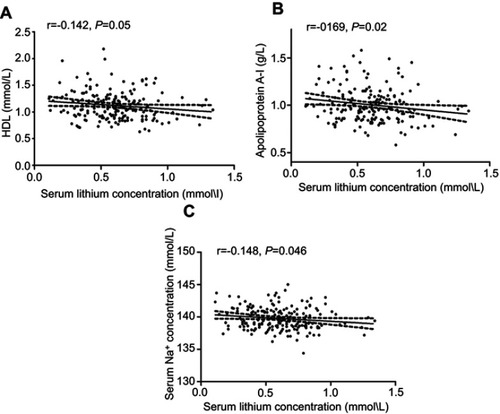
As shown in , the results of the Pearson correlation analysis showed that serum lithium concentrations were negatively correlated with HDL concentrations (r=−0.142, P=0.05; ), apolipoprotein A1 concentrations (r=−0.169, P=0.02; ), and Na+ concentrations (r=−0.148, P=0.046; ) in 186 patients with BD.
Figure 4 Negative correlations between the serum lithium concentration and HDL (A), apolipoprotein A1 (B), and Na+ concentrations (C) in186 patients with bipolar disorder.
Multivariate linear regression analysis showed that serum lithium concentrations were positively associated with the percentage of neutrophils and negatively associated with Na+ concentration ().
Table 2 Multiple linear regression analysis between the serum lithium concentrations (dependent variable) and the creatinine, HDL, apolipoprotein A1, Na+, Mg2+ concentrations, and percentage of neutrophils (independent variables)
Discussion
In the present study, we demonstrated that serum lithium concentrations were positively correlated with creatinine concentrations, Mg2+ concentrations, and the percentage of neutrophils and negatively correlated with HDL concentrations, apolipoprotein A1 concentrations, and Na+ concentrations by Pearson’s correlation test. Multivariate linear regression analysis indicated that serum lithium concentrations were positively associated with the percentage of neutrophils and negatively associated with Na+ concentrations in Chinese Han patients with BD.
Lithium preparations have been successfully used to treat BD and remain the best established long-term treatment for the disorder.Citation19 Because lithium is an agent with a low therapeutic index and as such requires careful monitoring for adverse effects, especially in long-term treatment, identification of factors influencing blood lithium concentration, achievement of a safe and stable blood concentration, and a reduction in adverse reactions of lithium are of great clinical value.
Serum creatinine measurement is a fast, effective and reliable measurement method for accurate estimation of GFR and is therefore considered the gold standard for measuring changes in kidney function and identifying acute kidney injury (AKI).Citation20 As renal insufficiency is clearly a very important potential clinical side effect of lithium,Citation21 a statistically significant increase in blood creatinine was found to be associated with short-termCitation22,Citation23 and long-termCitation24,Citation25 lithium treatment. In a population pharmacokinetic analysis, lithium measurements were described using a two-compartment model, and the most significant covariate for lithium clearance was found to be creatinine clearance.Citation9 More recently, long-term lithium treatment was reported to be associated with a decline in renal function as expressed by significant decreases in estimated GFR over time.Citation25 Consistently, a positive relationship was observed between serum lithium concentrations and creatinine concentrations in the present study, indicating that renal insufficiency might increase serum lithium concentrations. Taken together, these studies suggest that lithium treatment requires continuous monitoring of renal function, particularly when antihypertensive drugs, such as diuretics and renin-aldosterone system inhibitors, are utilized.Citation19
Recent studies support the notion that mood-stabilizing drugs (valproate or lithium) play an important role in lipid homeostasis and can be used as a prospective research target for the mechanism of action of these drugs.Citation12,Citation26 A previous study demonstrated that lithium inhibited the serum enzyme levels of HDL significantly and dose-dependently.Citation13 Similarly, the results of our study indicated that serum lithium concentrations were negatively correlated with HDL concentrations. Apolipoprotein A1 is the major protein component of HDL particles in blood.Citation27 It has been suggested that apolipoprotein A1 is a candidate marker for showing the response to lithium treatment at the serum protein level.Citation10 Consistent with these findings, the results of the present study have indicated a negative relationship between serum lithium concentrations and apolipoprotein A1 concentrations. However, the specific mechanism of these correlations remains unclear and requires further research.
Numerous studies have shown that there is a close relationship between blood lithium and Na+, the mechanism of which might be due to the expression of Na+/K+-ATPase,Citation28 a solute pump that pumps Na+ out of cells while pumping K+ into cells, both against their concentration gradients.Citation29 An in vitro study demonstrated the adaptation of live HEK293 cell metabolism to prolonged exposure to a therapeutic concentration of lithium manifested as the upregulation of Na+/K+-ATPase expression and extracellular Na+,Citation30 which might lead to increased excretion of extracellular Na+ through the kidney and eventually lead to a decrease in blood Na+. Considering the fact that a negative relationship between serum lithium concentrations and Na+ concentrations was observed by both Pearson correlation tests and multivariate linear regression analysis in the present study, it is rational to assume that Na+ concentrations may be an indicator for serum lithium concentrations. Additionally, a positive relationship between serum lithium concentrations and Mg2+ was also found in the present study, the mechanism of which remains unclear and might be related to the fact that lithium could compete with Mg2+and thereby inhibit vasopressin-sensitive adenylyl cyclase.Citation31 Due to the fact that several factors associated with electrolytes were not controlled for in the present study, more studies are clearly required to validate the cause-and-effect relationship between serum lithium concentrations and electrolytes.
Accumulating evidence supports an association between lithium and the number of cells in the blood. Lithium can increase WBC and neutrophil counts in both acutelyCitation32 and long term.Citation33 This lithium-induced increase in WBCs has been used to successfully treat neutropenia during carbamazepine therapy.Citation34,Citation35 The mechanism of lithium increasing neutrophil count and total WBC is not fully understood, and its effect is difficult to quantify. However, various suggestions, including demargination, stimulation of granulocyte-macrophage colony-stimulating factor, and stimulation of cytokines, have been proposed.Citation36,Citation37 The results of the present study first indicated that serum lithium concentrations were positively correlated with the percentage of neutrophils in186 Chinese Han patients with BD, further suggesting a close relationship between the concentration of blood lithium and the number of neutrophils and providing a theoretical basis for clinicians to treat neutropenia with lithium.
There are several limitations of this study that should be noted. First, the sample size is relatively small and all subjects were recruited from a single hospital. Second, the data regarding thyroid function of the patients at sample collection should be included because lithium has many effects on thyroid physiology.Citation38 Third, the causal relationship between the factors and blood lithium concentrations cannot be determined by the current research results and need to be investigated in future studies. Fourth, although all of the patients were drug free for at least 2 weeks, we were unable to take into account the probable long-term effects of previous drugs on kidney function. Fifth, the data regarding urine osmolality of the patients at sample collection should be included, for the reason that urine osmolality is an important indicator of renal function. Sixth, the baseline levels of factors related to blood lithium concentrations before medication was not observed.
At the end of this study, we reached the conclusion that the physiological factors, including creatinine, HDL, apolipoprotein A1, Na+, and Mg2+ concentrations and percentage of neutrophils, might be related to the serum lithium concentrations in Chinese Han patients with BD. Multicentric and longitudinal studies are clearly required to validate the relationship between serum lithium concentrations and physiological factors in patients with BD.
Disclosure
The authors report no conflicts of interest in this work.
References
- Grande I, Berk M, Birmaher B, Vieta E. Bipolar disorder. Lancet. 2016;387(10027):1561–1572. doi:10.1016/S0140-6736(15)00241-X26388529
- Hou L, Heilbronner U, Degenhardt F, et al. Genetic variants associated with response to lithium treatment in bipolar disorder: a genome-wide association study. Lancet. 2016;387(10023):1085–1093. doi:10.1016/S0140-6736(16)00143-426806518
- Pisanu C, Melis C, Squassina A. Lithium pharmacogenetics: where do we stand? Drug Develop Res. 2016;77(7):368–373. doi:10.1002/ddr.21341
- Yan Z, Yang X, Wang L, Zhao Y, Yu L. Social change and birth cohort increase in loneliness among Chinese older adults: a cross-temporal meta-analysis, 1995–2011. Int Psychogeriatr. 2014;26(11):1773–1781. doi:10.1017/S104161021400092124887197
- Zhang L, Cao X-L, Wang S-B, et al. The prevalence of bipolar disorder in China: a meta-analysis. J Affect Disord. 2017;207:413–421. doi:10.1016/j.jad.2016.08.06227771597
- Methaneethorn J. Population pharmacokinetic analyses of lithium: a systematic review. Eur J Drug Metab Pharmacokinet. 2018;43(1):25–34. doi:10.1007/s13318-017-0421-228555320
- Eldesoky ES, Kumar V, Alorainy MS, Hamdi MM, Derendorf H. Estimation of lithium clearance from routine clinical data in Egyptian bipolar patients. A population pharmacokinetic approach. Int J Clin Pharm Th. 2008;46(12):617–626.
- Finley PR. Drug interactions with lithium: an update. Clin Pharmacokinet. 2016;55(8):925–941.26936045
- Perez-Castello I, Mangas-Sanjuan V, Gonzalez-Garcia I, et al. Population pharmacokinetic model of lithium and drug compliance assessment. Eur Neuropsychopharmacol. 2016;26(12):1868–1876.27865605
- Rej S, Beaulieu S, Segal M, et al. Lithium dosing and serum concentrations across the age spectrum: from early adulthood to the tenth decade of life. Drugs Aging. 2014;31(12):911–916. doi:10.1007/s40266-014-0221-125331906
- Brown NC, Andreazza AC, Young LT. An updated meta-analysis of oxidative stress markers in bipolar disorder. Psychiat Res. 2014;218(1–2):61–68. doi:10.1016/j.psychres.2014.04.005
- Sussulini A, Dihazi H, Banzato CE, et al. Apolipoprotein A-I as a candidate serum marker for the response to lithium treatment in bipolar disorder. Proteomics. 2011;11(2):261–269. doi:10.1002/pmic.20100037121204253
- Ahmad M, Elnakady Y, Farooq M, Wadaan M. Lithium induced toxicity in rats: blood serum chemistry, antioxidative enzymes in red blood cells and histopathological studies. Biol Pharm Bull. 2011;34(2):272–277.21415540
- Shen HC, Li JY, Lo YK. Lithium intoxication-induced acute parkinsonism complicated with hyperparathyroidism and nephrogenic diabetes insipidus: report of a case. Acta Neurol Taiwan. 2007;16(4):231–233.18220017
- Grunfeld JP, Rossier BC. Lithium nephrotoxicity revisited. Nat Rev Nephrol. 2009;5(5):270–276. doi:10.1038/nrneph.2009.4319384328
- Matsuura H, Kimoto S, Harada I, Naemura S, Yamamuro K, Kishimoto T. Lithium carbonate as a treatment for paliperidone extended-release-induced leukopenia and neutropenia in a patient with schizoaffective disorder; a case report. BMC Psychiatry. 2016;16:161. doi:10.1186/s12888-016-0874-x27229149
- Sporn A, Gogtay N, Ortiz-Aguayo R, et al. Clozapine-induced neutropenia in children: management with lithium carbonate. J Child Adol Psychop. 2003;13(3):401–404. doi:10.1089/104454603322572697
- Yu W, Sun X, Li Y, Li M, Wang K, Li H. Population pharmacokinetics of lithium carbonate in young male healthy Chinese volunteers. Pharmacopsychiatry. 2016;49(5):177–181. doi:10.1055/s-0042-10332927124003
- Sani G, Perugi G, Tondo L. Treatment of bipolar disorder in a lifetime perspective: is lithium still the best choice? Clin Drug Invest. 2017;37(3):713–727. doi:10.1007/s40261-017-0531-2
- Pottel H, Delanaye P, Schaeffner E, et al. Estimating glomerular filtration rate for the full age spectrum from serum creatinine and cystatin C. Nephrol Dial Transplant. 2017;32(3):497–507. doi:10.1093/ndt/gfw42528089986
- Castro VM, Roberson AM, McCoy TH, et al. Stratifying risk for renal insufficiency among lithium-treated patients: an electronic health record study. Neuropsychopharmacology. 2016;41(4):1138–1143. doi:10.1038/npp.2015.25426294109
- Paul R, Minay J, Cardwell C, Fogarty D, Kelly C. Meta-analysis of the effects of lithium usage on serum creatinine levels. J Psychopharmacol. 2010;24(10):1425–1431. doi:10.1177/026988110910493019395432
- Amitai M, Zivony A, Kronenberg S, et al. Short-term effects of lithium on white blood cell counts and on levels of serum thyroid-stimulating hormone and creatinine in adolescent inpatients: a retrospective naturalistic study. J Child Adol Psychop. 2014;24(9):494–500. doi:10.1089/cap.2013.0046
- Bozikas V, Xafenias T, Andreou C, et al. Chronic renal insufficiency after long term lithium treatment. Psychiatriki. 2007;18(2):168–172.22466524
- Tondo L, Abramowicz M, Alda M, et al. Long-term lithium treatment in bipolar disorder: effects on glomerular filtration rate and other metabolic parameters. Int J Bipolar Disord. 2017;5(1):27. doi:10.1186/s40345-017-0096-228480485
- Dean B, Digney A, Sundram S, Thomas E, Scarr E. Plasma apolipoprotein E is decreased in schizophrenia spectrum and bipolar disorder. Psychiat Res. 2008;158(1):75–78. doi:10.1016/j.psychres.2007.05.008
- Viktorinova A, Jurkovicova I, Fabryova L, et al. Abnormalities in the relationship of paraoxonase 1 with HDL and apolipoprotein A1 and their possible connection to HDL dysfunctionality in type 2 diabetes. Diabetes Res Clin Pr. 2018;140:174–182. doi:10.1016/j.diabres.2018.03.055
- Banerjee U, Dasgupta A, Rout JK, Singh OP. Effects of lithium therapy on Na+-K+-ATPase activity and lipid peroxidation in bipolar disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2012;37(1):56–61. doi:10.1016/j.pnpbp.2011.12.00622230647
- Cui X, Xie Z. Protein interaction and Na/K-ATPase-mediated signal transduction. Molecules. 2017;22(6):pii: E990.
- Vosahlikova M, Ujcikova H, Chernyavskiy O, et al. Effect of therapeutic concentration of lithium on live HEK293 cells; increase of Na(+)/K(+)-ATPase, change of overall protein composition and alteration of surface layer of plasma membrane. Biochim Biophys Acta Gen Subj. 2017;1861(5 Pt A):1099–1112. doi:10.1016/j.bbagen.2017.02.01128215700
- Gong R, Wang P, Dworkin L. What we need to know about the effect of lithium on the kidney. Am J Physiol Renal Physiol. 2016;311(6):F1168–F1171. doi:10.1152/ajprenal.00145.201627122541
- Lapierre G, Stewart RB. Lithium carbonate and leukocytosis. Am J Hosp Pharm. 1980;37(11):1525–1528.7211857
- Carmen J, Okafor K, Ike E. The effects of lithium therapy on leukocytes: a 1-year follow-up study. J Natl Med Assoc. 1993;85(4):301–303.8478973
- Dumas R, Bardin P, Vedie C. Long-term treatment of clozapine-induced leukopenia with lithium: fast-onset agranulocytosis following lithium discontinuation. Prim Care Companion CNS Disord. 2016;18(1). doi:10.4088/PCC.15l01841
- Suraweera C, Hanwella R, de Silva V. Use of lithium in clozapine-induced neutropenia: a case report. BMC Res Notes. 2014;7:635. doi:10.1186/1756-0500-7-63525214394
- Ghaznavi S, Nakic M, Rao P, et al. Rechallenging with clozapine following neutropenia: treatment options for refractory schizophrenia. Am J Psychiatry. 2008;165(7):813–818. doi:10.1176/appi.ajp.2008.0711182318593787
- Phiel CJ, Klein PS. Molecular targets of lithium action. Annu Rev Pharmacol Toxicol. 2001;41:789–813. doi:10.1146/annurev.pharmtox.41.1.78911264477
- Sethy RR, Sinha VK. Effect of lithium on thyroid function in adolescents with mood disorder. Asian J Psychiatr. 2016;24:41–45. doi:10.1016/j.ajp.2016.08.00427931904