
Abstract
Autism spectrum disorder (ASD) is a highly complex and heterogeneous developmental disorder that affects how individuals communicate with other people and relate to the world around them. Research and clinical focus on the behavioural and cognitive manifestations of ASD, whilst important, have obscured the recognition that ASD is also commonly associated with a range of physical and mental health conditions. Many physical conditions appear with greater frequency in individuals with ASD compared to non-ASD populations. These can contribute to a worsening of social communication and behaviour, lower quality of life, higher morbidity and premature mortality. We highlight some of the key physical comorbidities affecting the immune and the gastrointestinal systems, metabolism and brain function in ASD. We discuss how healthcare professionals working with individuals with ASD and parents/carers have a duty to recognise their needs in order to improve their overall health and wellbeing, deliver equality in their healthcare experiences and reduce the likelihood of morbidity and early mortality associated with the condition.
Plain Language Summary
A diagnosis of autism spectrum disorder (ASD) is based on the presence of impairments with social communication and repetitive or restricted patterns of behaviour. Much of the scientific interest has focused on the behaviours and cognitive functioning that define ASD and how they can affect a person’s day-to-day quality of life. However, ASD does not typically appear as a stand-alone condition. Various other health conditions affecting physical and mental wellbeing are also commonly reported. These can have an important impact on daily living, social communication and behaviour. We highlight some of the conditions affecting the immune and gastrointestinal systems, metabolism and brain function, and how they can influence a person’s quality of life and increase the risk of early mortality. We discuss how professionals, working with those with ASD and their parents and carers can recognise the impact such conditions may have on individuals with ASD.
Introduction
Autism spectrum disorder (ASD) is a highly heterogeneous and complex neurodevelopmental condition. It is diagnosed by the presence of core deficits in the areas of social communication and restricted and/or repetitive patterns of behaviours that significantly impact on quality of life.Citation1 There is notable heterogeneity in the presentation of core autistic features, such that ASD for some individuals means a life of constant care and supervision with minimal opportunities for independent living. For others, ASD is associated with many lasting challenges but does not hinder the acquisition of independent living skills, meaningful employment and/or the development of close relationships.
ASD is for most people a lifelong disability.Citation2 Whilst developmental trajectories vary across individuals as a result of maturation and interventionsCitation3,Citation4 there is a substantial degree of persistence of core ASD features over a lifetime for many. This means that individualised support provisions are required across the lifespan for most individuals with ASD. The disparities in presentation subsumed under a singular label of ASD have led some to question whether a more plural taxonomy for autism is requiredCitation5 based on differing aetiologies, symptom profiles, responses to intervention and courses.
The current estimated prevalence of ASD is between 1–2%Citation6–Citation8 with a trend towards increasing numbers being diagnosed.Citation9–Citation12 Importantly, evidence of the increasing prevalence of ASD is not confined to one geographic areaCitation13,Citation14 but instead reflects an increasing global trend. Various factors have been put forward to account for the increasing number of cases of ASD including a widening of the diagnostic criteria, better case ascertainment, diagnostic substitution and increasing public awareness of the heterogeneity of ASD.Citation15,Citation16 A true increase in numbers is also possible.Citation17
The aetiologies of ASD are highly complex and vary across individuals. In most cases the emergence of ASD likely involves an interplay between genetic and environmental influences.Citation11 It is estimated that between 40–55% of the variance in ASD is attributed to environmental risk factors.Citation18,Citation19 Some of the environmental factors most strongly associated with the risk of ASD include maternal infections during pregnancy, autoimmune issues, foetal exposure to toxins, pollutants and certain types of medications, pregnancy complications, maternal stress, health and nutrition, and advanced paternal age.Citation20–Citation22 Regarding the genetic predisposition, there are a number of genetic disorders that are known to be associated with higher rates of ASD, such as Rett Syndrome, Fragile X and Down Syndrome, further illustrating the multiple aetiologies associated with this disorder.Citation23 Large scale whole genome analyses have identified additional susceptibility genes and processes involved in host defence and immune adaptive mechanisms that can contribute to ASD in the presence of specific environmental factors.Citation24–Citation28
Individuals with ASD have a significantly higher prevalence of comorbid mental and physical health conditions compared to the general population.Citation29–Citation33 Such comorbidities span a whole range of different conditions affecting various systems of the body including immune conditions, gastrointestinal (GI) disorders, metabolic conditions and seizure disorders. Importantly, physical health problems are persistent over the lifespan and are over-represented in very young children, including newborns who are later diagnosed with ASD, as well as in young people and adults with ASD.Citation34,Citation35 The concordance of ASD in monozygotic twins is significantly higher in those with a history of early physical conditions.Citation36 Early-life physical health problems and infant dysregulation, for example abnormal crying, feeding and sleeping difficulties, have been proposed as reliable early red flags for ASD screening.Citation37
Premature mortality is estimated to be three to ten times higher for individuals with ASD.Citation38–Citation40 Many early deaths are attributed to physical conditions, including seizures, sepsis, cancer as well as immune, respiratory and GI conditions such as constipation, outside of other accidental factors. Post-mortem studies have also revealed an association between ASD and the presence of often undiagnosed physical conditions.Citation41,Citation42 As a result of such comorbidities, those diagnosed with ASD also have much higher health care utilisation and associated costs.Citation33
There is a wealth of scientific data demonstrating the over-representation of various mental and physical health conditions alongside ASD. There is, however, still insufficient recognition amongst healthcare professionals that such symptoms could be related to comorbid physical health conditions rather than being commonly dismissed as “part of autism” or “autistic behaviours”. In this paper, we provide a literature review of the key physical comorbidities identified in people with ASD covering the areas of neuroinflammation and immune dysregulation, GI dysfunction, metabolic abnormalities, as well as seizure disorders such as epilepsy. We also discuss how healthcare professionals, working in partnership with individuals with ASD and their parents/carers, have a duty to be informed about the challenges and considerations in identifying physical comorbidities in this population. Hence, recognising and responding to such additional physical needs will provide equality in their healthcare experiences, and improve their quality of life as well as reducing their morbidity and premature mortality.
Neuroinflammation and Immune Dysregulation in ASD
There is abundant published evidence showing that over half of individuals with ASD present with immune dysregulation and neuroinflammation.Citation43–Citation46 Various clinical trials and experimental animal research have identified abnormal immune function as being central to the pathogenesis of ASD for at least a subset of individuals diagnosed with the condition.Citation47,Citation48 The severity of various types of immune alterations has also been found to correlate with the severity of the core features of ASD.Citation49–Citation52
A connection between immune dysfunction and ASD is continued in studies identifying a range of ASD susceptibility genes known to be involved in inflammatory signalling, immune function and infections.Citation27,Citation53,Citation54 Genetic associations between ASD and autoimmune disease, such as multiple sclerosis, have also been observed.Citation55 Furthermore, several large studies have detailed pro-inflammatory biomarkers indicative of dysfunctional immune responses in mothers and newborns who were later diagnosed with ASD.Citation56 In addition, epidemiological studies have consistently shown an association between prenatal infection/immune activation, maternal/infantile atopic diseases, food allergies/intolerances as well as family history of autoimmunity and risk of ASD.Citation57–Citation62 Repeated investigations have found chronic inflammatory processes in multiple areas of the brain and cerebrospinal fluid of individuals with ASD, including increased inflammatory cytokine and chemokine production and consistent activation of astrocytes and microglia.Citation63–Citation66
It is of particular interest that large doses of interferon-alpha, a pro-inflammatory cytokine given to humans in cancer treatment, can cause symptoms that can mimic ASD. Symptoms include a decline in speech, executive functioning and cognition as well as motor coordination, anxiety and irritability issues.Citation67,Citation68 Animal model studies have similarly shown that exposure to proinflammatory agents can lead to the emergence of ASD-like symptoms.Citation69–Citation72 In addition, offspring of animals exposed to immune stressors such as infections or allergies can also develop ASD-like symptoms, including deficits in social interactions, communicative impairments, and repetitive/stereotyped behaviours as well as sleep disturbances and epileptiform activity that closely mirror those observed in ASD.Citation73–Citation75
Autoimmunity in ASD
Autoimmune disorders are characterised by an abnormal immune response to “self”, where “self” tissues are recognised as foreign by the host immune system, leading to a cascade of adverse events and the dysfunction of these tissues or cell types. A number of studies have shown a high prevalence of autoimmune conditions in families of individuals with ASD compared to the general population. Such autoimmune conditions include coeliac disease, psoriasis, type I diabetes, rheumatoid arthritis, autoimmune thyroid disease and antiphospholipid syndrome.Citation76 In addition, mothers of ASD children have been found to have elevated levels of brain-reactive autoantibodies that are passed to their child in utero and react to foetal proteins.Citation77 This so-called maternal antibody-related (MAR) autism could potentially equate to around 10% of all cases of autism.Citation78
The severity of adaptive functioning and communication impairments in the offspring have been correlated to the levels of maternal autoantibodies.Citation79 Animal studies cast further light on such associations, where IgG antibodies derived from mothers of children with ASD were found to cause abnormal brain development and social functioning when transplanted to primate animals.Citation80
The presentation and the severity of core autistic symptoms and the presence of various autoantibodies have been linked.Citation81,Citation82 Studies have shown that children with ASD and a family history of autoimmunity had significantly higher frequency of systemic serum antinuclear antibodies. These autoantibodies can cause tissue damage via multiple mechanisms, including neurotoxicity.Citation83
Although still the topic of some discussion, research reports have recommended further study on a possible role for PANDAS (Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections) or PANS (Pediatric Acute-onset Neuropsychiatric Syndrome) in relation to ASD.Citation84 PANDAS/PANS represent infection-induced autoimmune conditions that disrupt typical neurological functioning. The conditions manifest as rapid onset obsessive compulsive disorder (OCD) and/or motor tics,Citation85 alongside other behaviours that potentially overlap with the diagnosis of ASD. There are some important clues about the pathophysiology of PANDAS/PANS pertinent to autoimmunity and ASD. Specifically the infection-triggered autoimmune response and/or molecular mimicry that characterise the conditions, targeting brain structures such as the basal ganglia, provide a template for further investigations.
Autistic Regression and Its Association with Infection, Autoimmunity and Inflammation
Autistic regression is characterized as the emergence of ASD symptoms and functional impairments after an initial period of normal or typical development. While many children who are later diagnosed with ASD present with developmental delay from birth, an estimated quarter to a third of all cases demonstrate normal development followed by some regression characterised by a loss of previously achieved language and/or other developmental skills.Citation86 Onset of symptoms of physical distress such as fever, irritability, vomiting, incessant crying, sudden changes in sleep patterns, as well as novel dietary restrictions, sensory dysfunction and the emergence of motor impairments are frequently noted around the time of regression. Changes can be seen as abrupt (occurring within days) or progressive, evolving more gradually over a period of several months. There appears to be a strong correlation between autistic regression and poorer long-term outcomes.Citation87 While the regression usually occurs between the ages of 12–24 months, several studies have reported unusual patterns of regression. This includes regressions involving severe and/or sudden-onset motor dysfunction, recurring regressions and/or regressions after age three years.Citation88,Citation89
Cases of autistic regression in young children are not typically the subject of detailed investigations, and the precise contributing mechanisms are largely unknown. An emerging body of evidence suggests however, that immune dysregulation and autoimmune phenomena could be one potential pathogenic mechanism in at least a subset of cases.Citation88 Cases of autistic regression following viral and bacterial encephalitis have been reported in previously healthy and typically-developing childrenCitation90–Citation93 as well as in adolescents and even adults.Citation94–Citation97
Autistic regression has also been reported in cases following the onset of autoimmune proliferative syndrome, or autoimmune anti-N-methyl-D-aspartate receptor antibodies (NMDAR-Ab) encephalitis.Citation98–Citation100 NMDAR-Ab encephalitis is a well-characterised clinical-immunological syndrome caused by an autoimmune reaction to neuronal NMDA receptors. In adults, the initial symptoms are mostly neuropsychiatric in nature, with an often rapid global health deterioration including the occurrence of hypoventilation, catatonia, cerebellar ataxia and loss of consciousness. The symptoms in children are typically less severe and more difficult to recognise. One of the main presenting features of NMDAR-Ab encephalitis in children is loss of language and social skills and reduced interest in surroundings; some of the hallmarks of ASD. Other presenting features in children can include seizures and/or status epilepticus, sleep disturbances, temper tantrums, lack of appetite, dystonia, abnormal gait, tics, hyperactivity, psychotic episodes, irritability, agitation and aggression.Citation101,Citation102 All of those features, in varying degrees of severity, are commonly present in idiopathic autism. An awareness of a potentially important role for autoantibodies in some cases of ASD is required by healthcare professionals. Such appreciation should particularly extend to those individuals with ASD who have a familial history of autoimmune-related diseases and/or seizure disorder.
Allergic Diseases in ASD
The manifestations of allergic disease, including IgE and non-IgE mediated reactions, are being increasingly recognised to encompass both behavioural and neurological indicators alongside classical somatic markers.Citation103,Citation104 Diagnoses such as anxiety and mood disorders show important relationships with allergic reaction biological markers. Such allergic reactions can contribute to difficulties in focusing, irritability, hyperactivity, daytime fatigue and sleep problems in both young people and adults.Citation105 Treatment of allergy can also positively impact on behaviour, where symptoms of anxiety and mood disorders for some diminish following allergy treatments.Citation106
Atopic disease, asthma and food allergies are common in individuals with ASD.Citation107 The presentation of core ASD symptoms - impaired social communication and repetitive and/or stereotyped behaviours - are seemingly connected to allergic manifestations, alongside other neuropsychiatric symptoms such as anxiety, hyperactivity, and irritability.Citation108–Citation111 The assumption is that the pain and discomfort following allergic conditions exacerbate challenging behaviours and cognitive dysfunction in individuals with ASD. In some cases, the treatment of allergies has been reported to result in improvements in challenging behaviours and cognitive function.Citation112 In addition, some findings suggest shared pathological mechanisms,Citation113–Citation116 and experimental animal studies have even demonstrated a possibility that allergic neuroimmune activation might underlie some of the symptoms and behavioural abnormalities associated with ASD.Citation117
Imbalances in the hypothalamus-pituitary-adrenal axis (HPA) and the sympathetic axes can result from allergic diseases such as atopic dermatitis and allergic rhinitis. Such an imbalance is thought also to affect cognition and behaviour. Whilst still the topic of investigation, adrenaline release via histamine or direct activation by mast cell involvement are likely involved.Citation118 Given the high prevalence of allergic diseases, non-IgE mediated hypersensitivity reactions and mast cell over-activation in ASD, as well as confirmed HPA dysfunction with abnormal stress reactivity and sympathetic over-activation, it is possible that, in at least some individuals with ASD, some aberrant behaviours that are frequently characterised as “autistic behaviour” can be related to preventable allergy and intolerance issues.
Allergic and/or non-IgE hypersensitivity should be ruled out when a young person or adult with ASD presents with agitation, irritability, aggression, anxiety, sleep difficulties, lack of concentration, hyperactivity and daytime fatigue.
Gastrointestinal Dysfunction in ASD
GI disorders are significantly overrepresented in ASD compared with the general population.Citation119 Individuals with ASD present with frequent functional issues of diarrhoea, constipation, and gastroesophageal reflux alongside higher rates of inflammatory bowel diseases.Citation120 Various other clinical findings appear to be overrepresented in ASD, including increased intestinal permeability, various digestive enzyme deficiencies and bacterial dysbiosis.Citation121–Citation123 Children with ASD present with higher rates of lymphoid nodular hyperplasia, esophagitis, gastritis, and duodenitis.Citation124,Citation125 The presence of GI dysfunction in children with ASD is, in most cases, not associated with medication or peculiar dietary habits or medication.Citation126 Importantly, there is a strong correlation between the presence of GI symptoms and the severity of ASD-related symptoms and behaviours, including irritability, aggression, rigid-compulsive behaviours, anxiety, sensory over-responsivity and dysregulated sleep issues.Citation127–Citation129
Analyses of the GI bacterial composition as well as the identification of bacterial metabolic and biochemical markers in the urine of individuals with ASD have demonstrated the presence of atypical microbiota.Citation130,Citation131 Translocation of bacterial species to other parts of the GI tract and indeed, outside of it, has also been described.Citation132 This has led to the proposal that treatment aimed at rebalancing the gut flora could alleviate some symptoms associated with ASD. There is some emerging evidence in support of the use of pre- and probiotics for the management of behavioural issues associated with ASD.Citation133–Citation135
There is existing guidance in the peer-reviewed literature recommending that healthcare professionals consider the possibility of behavioural manifestations of GI disorders in individuals with ASD “as those can be atypical and evident only as a change in behaviour, thus presenting a significant challenge to both parents and healthcare providers”.Citation136 Authors explicitly described how, in young people with ASD, faint and anomalous behavioral symptoms should increase suspicion for the existence of constipation. A routine programme of screening, identification and treatment of constipation and its underlying causes is appropriate. Other authors have similarly urged the need for appropriate investigations,Citation137 again stressing a possible connection between GI symptoms and behaviour as well as acknowledging that issues such as a limited verbal capacity can affect the quality of care received.
Non-Coeliac Gluten Sensitivity (NCGS) and ASD
Dietary changes, predominantly including the adoption of gluten- and casein-free diets, have been a feature of autism research and practice for many years. Early preliminary research,Citation138 published case studiesCitation139,Citation140 and parental reports of beneficial changes in ASD symptoms following such dietary regimes litter the peer-reviewed literature. Despite no universal effect being reported thus far,Citation141 research continues in this area, specifically concentrating on determining potential non- and best-responders to such nutritional changes.Citation142
Debate persists as to the effect and mode of actions of gluten and casein containing foods on individuals with ASD. Insufficiency of numerous digestive enzymes, such as disaccharidases and lactase, has been consistently reported in this population.Citation121 Preferential screening for coeliac disease has been indicated.Citation143 Case reports have noted an improvement in presentation of ASD-related symptoms following a gluten-free and/or casein-free diet in cases of dual ASD and coeliac disease.Citation144
Alongside examples of clinically-indicated coeliac disease, evidence is emerging for non-coeliac gluten sensitivity (NCGS) in some cases of ASD.Citation145–Citation148 While the exact prevalence and clinical manifestations of NCGS in the general population are still the subject of investigation (with continued steps towards definitive description), the existence of NCGS as a new clinical entity has recently been confirmed and classified through large-scale double-blinded studies.Citation149 Identification of NCGS is currently based on exclusion criteria and following the outcome of a gluten-free diet.
Individuals with ASD and a history of allergy and atopic disease are more likely to suffer from NCGS.Citation150 Carrocio et alCitation151 observed that mucosal eosinophil infiltration was a primary histological feature of non-coeliac wheat sensitivity. Such infiltration has been reported in cases of pediatric ASD. Adoption of a gluten-free diet has also been reported to positively affect such clinical findings.Citation152,Citation153
Healthcare professionals need to be familiar with NCGS and its possible appearance in cases of ASD. Those on the autism spectrum displaying symptoms of irritable bowel syndrome or those with potential allergic and other immune-related symptoms may be particular candidates for further screening and inquiry. In this context it is also important to highlight how various neurological dysfunctions can also show a relationship with gluten sensitivity, and can arise independent of noticeable GI symptoms. Familiarity with the various neurological and neuropsychiatric presentations linked to ingestion of foods containing gluten - mood and anxiety disorders, ataxia, migraine, neuropathy and seizure disorders - which may indeed underlie some of the symptoms commonly associated with ASDCitation154,Citation155 is an important requirement.
Seizure Disorders and Epilepsy in ASD
The frequency of seizure disorders including epilepsy is notably greater in individuals with ASD compared to the general population. Estimates suggest that around 20% of individuals with ASD will develop epilepsy at some stage in their lifeCitation156 with a sizable number also presenting with subclinical epileptiform activity in the absence of a clinical seizure disorder.Citation157 While an association between the more severe forms of ASD and epilepsy has been known for many years, recent detailed investigations have also shown a high rate of EEG abnormalities and epilepsy risk in individuals with high-functioning ASD.Citation158 Conversely, the frequency of ASD and related diagnoses is also elevated among individuals with epilepsy compared with the general population.Citation159
Aside from the significant impact that epilepsy can have on a person’s life, it is a leading cause of the elevated premature mortality risk in ASD.Citation39 Accurate and timely diagnosis and treatment of epilepsy is vitally important. Intervention approaches as and when atypical epileptiform activity is present, can lead to a significant abatement of aberrant behaviours and improvements in psychosocial function, alongside decreasing seizure activity.Citation160,Citation161 Such a connection implies that some behaviours commonly attributed to ASD may in some cases be due to epileptic activity itself. In addition to clinical seizures, successful treatment of subclinical epileptiform discharges has also been shown to improve cognitive function and ASD-related symptoms and behaviours.Citation162 Apart from their possible detrimental effects on cognitive and executive function in individuals with ASD, abnormal isolated epileptiform discharges (IEDs) have been observed to convert to clinical seizures in over 20% of the sufferers in a 2-year follow up study.Citation163 Other findings support the diagnostic use of EEG in individuals with ASD.Citation164
For those individuals who have failed prior psychopharmacology attempts, and those who exhibit unusual and challenging behaviours—for example, sudden and unprovoked outbursts of aggression, irritability, crying, screaming or self-harming, unusual facial and body movements and postures, staring spells, covering of ears—an EEG could be helpful for differentiating between seizures and non-epileptic paroxysmal behaviours.Citation165,Citation166
Metabolic Irregularities, Acquired Mitochondrial Dysfunction and Oxidative Stress in ASD
Children and adults with ASD are at significantly greater risk for weight issues and obesity than the general population.Citation167 Compared with those presenting with milder impairments, individuals with severe ASD also show an increased likelihood of obesity alongside various other metabolic disorders including hypertension, diabetes and dyslipidemia.Citation29,Citation32,Citation168 While the reasons for increased obesity rates in ASD are commonly assumed to be due solely to poor eating habits, the lack of physical activity and/or medication, increased weight gain has been recorded during early infancyCitation169 pointing to possible involvement of intrinsic biological factors. Such findings complement other studies observing that maternal obesity may be a significant risk factor for offspring ASD.Citation170,Citation171 Interestingly, and in common with autism, obesity has been found to be associated with a dysregulated gut microbiota,Citation172 offering the possibility of a common underlying cause or pathways. Whether maternal obesity or other conditions more likely to appear alongside obesity (eg hypertension, diabetes, dyslipidemia, alteration of gut microbiota) are causative of such enhanced risk for offspring ASD remains to be elucidated.
Consistent scientific findings point to elevated levels of oxidative stress and perturbed methylation processes, atypical energy metabolism and mitochondrial dysfunction and disruption in sulphur and amino acid biochemistry in ASD compared to the general population.Citation173,Citation174 There is also strong evidence that such processes may have an intricate, and likely pathogenic, connection in at least a subset of ASD.Citation175
While cellular energy production in the brain has been reported as impaired in individuals with ASD, inflated levels of markers of oxidative stress alongside reductions in glutathione and other important cellular antioxidants have been reported in other body regions and in immune cells.Citation176 Atypical detoxification systems present in cases of ASD have also been associated with the severity of cognitive and social impairments.Citation177 Atypical mitochondrial energy metabolism - elevated blood, urine and cerebrospinal fluid levels of pyruvate, lactate and alanine alongside serum carnitine insufficiency - have been reported in cases of ASD.Citation178 In the majority of cases this abnormal energy metabolism cannot be linked to an identifiable genetic cause or another primary inborn error of metabolism.Citation179 The metabolic and chemical changes observed in individuals with ASD are instead suggestive of a dynamic dysfunction process secondary to outside stressors.Citation180 Some authors have proposed that the mitochondrial and metabolic anomalies appearing alongside ASD ensue following immune dysfunctionCitation181 or an abnormal microbiome.Citation182 Inadequate mitochondrial energy production could both result from and add to cellular oxidative stress and chronic inflammation in individuals with ASD. Reactive oxygen species are damaging to cells and organs. Inflated levels of oxidative stress are suspected in various other inflammatory and autoimmune diseases. Chronic inflammation as an important function in various metabolic disorders manifesting behavioural and cognitive features is also likely relevant to ASD.Citation183
Studies investigating metabolic markers in the context of ASD have also revealed a variety of important findings. In one study an inborn error of metabolism was detected in 7% of children.Citation184 Cerebral folate deficiency, together with folate receptors autoantibodies, have also been reported to play a pathological role in cases of ASD.Citation185
Healthcare professionals should have awareness of and screen for metabolic and/or mitochondrial dysfunction as these physical comorbidities can potentially contribute to ASD severity.
Motor Dysfunction, Connective Tissue Disturbance and Movement Disorders in ASD
Motor difficulties are an important facet of many cases of ASD. Some of the earliest descriptions of ASD included discussion of motor deficitsCitation168 although formal diagnostic criteria have so far not included this important area of functioning. Various different types of motor dysfunction and movement disorders have been noted in ASD.Citation187 Such observations cover both fine and gross motor skills. Despite the lack of formal acceptance of such deficits, motor skill dysfunction shows some important correlations with other core ASD features.Citation188 Ehlers-Danlos Syndrome (EDS), a disorder of the connective tissue characterised by joint hypermobility and a wide range of articular and non-articular manifestations including GI symptoms, has also been reported alongside ASD.Citation189
Sensory Dysfunction and Abnormal Pain Reactivity in ASD
Another important feature of ASD is sensory processing and dysfunction. Covering all of the primary senses - auditory, visual, tactile, olfactory and gustatory input - there is a wealth of scientific literature noting differences in the sensation and/or processing of sensory data in ASD.Citation190 Sensory dysfunctions and abnormal processing of pain also seemingly underlie some of the more challenging behaviours associated with ASDCitation191,Citation192 and are a facet of the current diagnostic criteria for ASD. Various studies have highlighted a strong connection between sensory dysfunction and the presentation of other core ASD features.
Identifying Physical Comorbidities in ASD – Challenges and Considerations
In this paper, we have highlighted a number of physical comorbidities that are associated with ASD (see ). Recognising the physical comorbidities in individuals with ASD is challenging. A primary reason is that ASD is not traditionally seen as being related to any physical ailments but solely the result of behavioural and neuropsychiatric dysfunction. We argue that the main barrier to better awareness and recognition is this paradigm within which many healthcare professionals operate. Another reason is that the expression of physical comorbidities in ASD is sometimes atypical.
Figure 1 Physical health comorbidities associated with ASD.
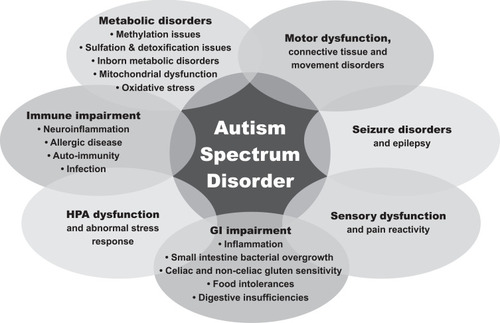
Various factors need to be considered to enable the accurate recognition of physical health comorbidities in individuals with ASD. Challenging behaviours such as aggression or self-injurious behaviour (SIB) in individuals with ASD may be the dominant or exclusive symptom of a hidden physical condition, which can be acute or chronic as well as progressive or static. Individuals with ASD often respond to pain with challenging behaviours. For example common target body areas of SIB include biting of the hands (especially in the area between thumb and index), the head (frontal, temporal and back of the head) and the jaw areas.
Symptoms such as grimacing, appetite disturbances, insomnia and strange postures are not core features of ASD. A considerable volume of scientific evidence points to the possibility of an underlying physical cause to such behaviours. To avert diagnostic overshadowing, screening for physical conditions should be initiated when such behaviours are observed.
A functional analysis of challenging behaviours is warranted to identify the root cause(s) of such behaviours. These could be purely behavioural (ie attention seeking, access to tangibles, escape, sensory) and/or be related to physical health. The sudden onset of challenging behaviour, often described as “out of the blue” by parents and carers, more specifically suggests an underlying physical cause and warrants further evaluation. For example, a sudden occurrence of compulsive behaviour and tics might be associated with infection and/or autoimmune conditions; abnormal, out of context laughter and sudden onset of aggressive behaviour could be related to gut dysbiosis or seizures.
Parents and carers typically provide accurate and valuable information about the symptoms and behavioural changes observed in their children. However, they may be unaware of the possible causes of these changes, especially when they have been advised that these are ‘simply what autism is’.
Individuals with ASD who are perceiving pain and/or discomfort may be unable to report either the pain itself or the physical location within their body. Hence, the use of visual aids and augmentative communication tools may be useful. Equally the use of a non- communicative pain checklist can be helpful.Citation193 In order to tackle morbidity and preventable death in individuals with ASD it is of utmost importance to provide regular physical health checks and to maintain high level of clinical suspicion towards physical health problems in ASD.
Conclusion
Physical health comorbidities occur significantly more frequently in individuals with ASD than in the wider general population. Such comorbidities include neuroinflammation and immune dysregulation, GI dysfunction, metabolic abnormalities, acquired mitochondrial dysfunction and oxidative stress as well as seizure disorders such as epilepsy. Some of the physical symptoms presented by those with ASD have been erroneously attributed to the core behavioural and neurological features of ASD. Impairments in social interaction and communication are, by their definition, central symptoms of ASD. They obscure the recognition of underlying physical comorbidities by clinicians. It is of utmost importance to raise awareness among healthcare professionals and bridge the gap between physical health and the implication of ASD as a whole body disorder. Leaving these physical conditions undiagnosed and untreated clearly results in health inequalities. They can also significantly decrease a person’s quality of life potentially leading to morbidity and/or premature mortality.
Acknowledgments
This paper was derived from the document ‘Medical comorbidities in autism spectrum disorders: a primer for health care professionals and policy makers’ published by Thinking Autism (charity number: 1113628) in 2014. Paul Shattock and Paul Whiteley would like to acknowledge a grant received from the Robert Luff Foundation (charity number: 273810) which enabled their contribution to this paper.
Disclosure
Dr Sala has been an advisor to or has received honoraria from Takeda. Dr Paul Whiteley reports grants from The Robert Luff Foundation, during the preparation of this paper. The authors report no other conflicts of interest in this work.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: Diagnostic and Statistical Manual of Mental Disorders. Fifth Arlington, VA; 2013.
- Whiteley P, Carr K, Shattock P, et al. Is autism inborn and lifelong for everyone? Neuropsychiatr Dis Treat. 2019;15:2885–2891. doi:10.2147/NDT.S22190131632036
- Fein D, Barton M, Eigsti I-M, et al. Optimal outcome in individuals with a history of autism. J Child Psychol Psychiatry. 2003;54:195–205. doi:10.1111/jcpp.12037
- Wise EA, Smith MD, Rabins PV, et al. Aging and autism spectrum disorder: a naturalistic, longitudinal study of the comorbidities and behavioural and neuropsychiatric symptoms in adults with ASD. J Autism Dev Disord. 2017;47(6):1708–1715. doi:10.1007/s10803-017-3095-328303420
- Whiteley P. Nutritional management of (some) autism: a case for gluten- and casein-free diets? Proc Nutr Soc. 2015;74(3):202–207. doi:10.1017/S002966511400147525311313
- Baron-Cohen S, Scott FJ, Allison C, et al. Prevalence of autism-spectrum conditions: UK school-based population study. Br J Psychiatry. 2009;194(6):500–509. doi:10.1192/bjp.bp.108.05934519478287
- Zablotsky B, Black LI, Maenner MJ, et al. Estimated Prevalence of autism and other developmental disabilities following questionnaire changes in the 2014 National Health Interview Survey. Natl Health Stat Rep. 2015;87:1–20.
- Baio J, Wiggins L, Christensen DL, et al. Prevalence of autism spectrum disorder among children aged 8 years — autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014. MMWR Morb Mortal Wkly Rep. 2018;67(6):1–23.29324727
- Xu G, Strathearn L, Liu B, et al. Prevalence of autism spectrum disorder among US children and adolescents, 2014–2016. JAMA. 2018;319(1):81–82. doi:10.1001/jama.2017.1781229297068
- Blumberg SJ, Bramlett MD, Kogan MD, et al. Changes in prevalence of parent-reported autism spectrum disorder in school-aged U.S. children: 2007 to 2011–2012. Natl Health Stat Report. 2013;65:1–11.
- Lyall K, Croen L, Daniels J, et al. The changing epidemiology of autism spectrum disorders. Annu Rev Public Health. 2017;38(1):81–102. doi:10.1146/annurev-publhealth-031816-04431828068486
- Waugh I. The Prevalence of Autism (Including Asperger Syndrome) in School Age Children in Northern Ireland 2019. Northern Ireland Department of Health; 5 2019.
- Sun X, Allison C, Wei L, et al. Autism prevalence in China is comparable to Western prevalence. Mol Autism. 2019;10:7. doi:10.1186/s13229-018-0246-030858963
- Kim YS, Leventhal BL, Koh Y-J, et al. Prevalence of autism spectrum disorders in a total population sample. Am J Psychiatry. 2011;168(9):904–912. doi:10.1176/appi.ajp.2011.1010153221558103
- Rice CE, Rosanoff M, Dawson G, et al. Evaluating changes in the prevalence of the autism spectrum disorders (ASDs). Public Health Rev. 2012;34(2):1–22. doi:10.1007/BF0339168526236074
- Hertz-Picciotto I, Delwiche L. The rise in autism and the role of age at diagnosis. Epidemiology. 2009;2:84–90. doi:10.1097/EDE.0b013e3181902d15
- Russell G, Collishaw S, Golding J, et al. Changes in diagnosis rates and behavioural traits of autism spectrum disorder over time. BJPsych Open. 2015;1(2):110–115. doi:10.1192/bjpo.bp.115.00097627703734
- Sandin S, Lichtenstein P, Kuja-Halkola R, et al. The heritability of autism spectrum disorder. JAMA. 2017;318(12):1182–1184. doi:10.1001/jama.2017.1214128973605
- Hallmayer J, Cleveland S, Torres A, et al. Genetic heritability and shared environmental factors among twin pairs with autism. Arch Gen Psychiatry. 2011;68(11):1095–1102. doi:10.1001/archgenpsychiatry.2011.7621727249
- Modabbernia A, Velthorst E, Reichenberg A, et al. Environmental risk factors for autism: an evidence-based review of systematic reviews and meta-analyses. Mol Autism. 2017;8:13. doi:10.1186/s13229-017-0121-428331572
- Emberti Gialloreti L, Mazzone L, Benvenuto A, et al. Risk and protective environmental factors associated with autism spectrum disorder: evidence-based principles and recommendations. J Clin Med. 2019;8(2):217. doi:10.3390/jcm8020217
- Getahun D, Fassett M, Peltier M, et al. Association of perinatal risk factors with autism spectrum disorder. Am J Perinatol. 2017;34(03):295–304. doi:10.1055/s-0036-159762428099978
- Gilberg C, Coleman M. The Biology of Autistic Disorders. Clinics in Developmental Medicine. 3rd ed. London, United Kingdom: Mac Keith Press; 2000.
- Saffari A, Arno M, Nasser E, et al. RNA sequencing of identical twins discordant for autism reveals blood-based signatures implicating immune and transcriptional dysregulation. Mol Autism. 2019;10:38. doi:10.1186/s13229-019-0285-131719968
- Saxena V, Ramdas S, Ochoa CR, et al. Structural, genetic, and functional signatures of disordered neuro-immunological development in autism spectrum disorder. PLoS One. 2012;7(12):e48835. doi:10.1371/journal.pone.004883523239965
- Castelbaum L, Sylvester CM, Zhang Y, et al. On the nature of monozygotic twin concordance and discordance for autistic trait severity: a quantitative analysis. Behav Genet. 2019. doi:10.1007/s10519-019-09987-2
- Tamouza R, Fernell E, Eriksson MA, et al. HLA polymorphism in regressive and non-regressive autism: a preliminary study. Autism Res. 2019. doi:10.1002/aur.2217
- Nazeen S, Palmer NP, Berger B, et al. Integrative analysis of genetic data sets reveals a shared innate immune component in autism spectrum disorder and its co-morbidities. Genome Biol. 2016;17(1):228. doi:10.1186/s13059-016-1084-z27842596
- Croen L, Zerbo O, Qian Y, et al. The health status of adults on the autism spectrum. Autism. 2015;19(7):814–823. doi:10.1177/136236131557751725911091
- Gurney JG, McPheeters ML, Davis MM, et al. Parental report of health conditions and health care use among children with and without autism: national Survey of Children’s Health. Arch Pediatr Adolesc Med. 2006;160(8):825–830. doi:10.1001/archpedi.160.8.82516894082
- Bishop-Fitzpatrick L, Rubenstein E. The physical and mental health of middle aged and older adults on the autism spectrum and the impact of intellectual disability. Res Autism Spectr Disord. 2019;63:34–41. doi:10.1016/j.rasd.2019.01.00131768189
- Fortuna RJ, Robinson L, Smith TH, et al. Health conditions and functional status in adults with autism: a cross-sectional evaluation. J Gen Intern Med. 2016;31(1):77–84. doi:10.1007/s11606-015-3509-x26361965
- Vohra R, Madhavan S, Sambamoorthi U, et al. Comorbidity prevalence, healthcare utilization, and expenditures of Medicaid enrolled adults with autism spectrum disorders. Autism. 2017;21(8):995–1009. doi:10.1177/136236131666522227875247
- Losh M, Esserman D, Anckarsäter H, et al. Lower birth weight indicates higher risk of autistic traits in discordant twin pairs. Psychol Med. 2012;42(5):1091–1102. doi:10.1017/S003329171100233922132806
- Pan P-Y, Tammimies K, Bölte S, et al. The association between somatic health, autism spectrum disorder, and autistic traits. Behav Genet. 2019. doi:10.1007/s10519-019-09986-3
- Willfors C, Carlsson T, Anderlid B-M, et al. Medical history of discordant twins and environmental etiologies of autism. Transl Psychiatry. 2017;7(1):e1014. doi:10.1038/tp.2016.26928140403
- Dillenburger K, Jordan J-A, McKerr L, et al. The Millennium child with autism: early childhood trajectories for health, education and economic wellbeing. Dev Neurorehabil. 2015;18:37–46. doi:10.3109/17518423.2014.96437825289682
- Smith DaWalt L, Hong J, Greenberg JS, et al. Mortality in individuals with autism spectrum disorder: predictors over a 20-year period. Autism. 2019;23(7):1732–1739. doi:10.1177/136236131982741230818975
- Hwang YI (Jane), Srasuebkul P, Foley K-R, et al. Mortality and cause of death of Australians on the autism spectrum. Autism Res. 2019;12(5):806–815. doi:10.1002/aur.208630802364
- Shavelle RM, Strauss DJ, Pickett J, et al. Causes of death in autism. J Autism Dev Disord. 2001;31(6):569–576. doi:10.1023/A:101324701148311814268
- Datlow Smith M, Graveline PJ, Smith JB, et al. Autism and obstacles to medical diagnosis and treatment. Focus Autism Other Dev Disabl. 2012;27:189–195. doi:10.1177/1088357612450049
- Vargas DL, Nascimbene C, Krishnan C, et al. Neuroglial activation and neuroinflammation in the brain of patients with autism [published correction appears in Ann Neurol. 2005 Feb;57(2):304]. Ann Neurol. 2005;57(1):67–81. doi:10.1002/ana.2031515546155
- Rodriguez JI, Kern JK. Evidence of microglial activation in autism and its possible role in brain underconnectivity. Neuron Glia Biol. 2011;7(2–4):205–213. doi:10.1017/S1740925X1200014222874006
- Young AM, Chakrabarti B, Roberts D, et al. From molecules to neural morphology: understanding neuroinflammation in autism spectrum condition. Mol Autism. 2016;7:9. doi:10.1186/s13229-016-0068-x26793298
- DiStasio MM, Nagakura I, Nadler MJ, et al. T lymphocytes and cytotoxic astrocyte blebs correlate across autism brains. Ann Neurol. 2019;86(6):885–898. doi:10.1002/ana.2561031591744
- Masi A, Glozier N, Dale R, et al. The immune system, cytokines, and biomarkers in autism spectrum disorder. Neurosci Bull. 2017;33(2):194–204. doi:10.1007/s12264-017-0103-828238116
- Carlezon WA Jr., Kim W, Missig G, et al. Maternal and early postnatal immune activation produce sex-specific effects on autism-like behaviors and neuroimmune function in mice. Sci Rep. 2019;9(1):16928. doi:10.1038/s41598-019-53294-z31729416
- Thom RP, Keary CJ, Palumbo ML, et al. Beyond the brain: A multi-system inflammatory subtype of autism spectrum disorder. Psychopharmacology (Berl). 2019;236(10):3045–3061. doi:10.1007/s00213-019-05280-631139876
- Al-Ayadhi LY, Mostafa GA. Elevated serum levels of macrophage-derived chemokine and thymus and activation-regulated chemokine in autistic children. J Neuroinflammation. 2013;10(1):72. doi:10.1186/1742-2094-10-7223782855
- Grigorenko EL, Han SS, Yrigollen CM, et al. Macrophage migration inhibitory factor and autism spectrum disorders. Pediatrics. 2008;122(2):e438–e445. doi:10.1542/peds.2007-360418676531
- Heuer L, Ashwood P, Schauer J, et al. Reduced levels of immunoglobulin in children with autism correlates with behavioral symptoms. Autism Res. 2008;1(5):275–283. doi:10.1002/aur.4219343198
- Onore C, Careaga M, Ashwood P, et al. The role of immune dysfunction in the pathophysiology of autism. Brain Behav Immun. 2012;26(3):383–392. doi:10.1016/j.bbi.2011.08.00721906670
- Gupta S, Ellis SE, Ashar FN, et al. Transcriptome analysis reveals dysregulation of innate immune response genes and neuronal activity-dependent genes in autism. Nat Commun. 2014;5(1):5748. doi:10.1038/ncomms674825494366
- Bennabi M, Gaman A, Delorme R, et al. HLA-class II haplotypes and autism spectrum disorders. Sci Rep. 2018;8(1):7639. doi:10.1038/s41598-018-25974-929769579
- Jung J-Y, Kohane IS, Wall DP, et al. Identification of autoimmune gene signatures in autism. Transl Psychiatry. 2011;1(12):e63. doi:10.1038/tp.2011.6222832355
- Brown AS, Sourander A, Hinkka-Yli-Salomäki S, et al. Elevated maternal C-reactive protein and autism in a national birth cohort. Mol Psychiatry. 2014;19(2):259–264. doi:10.1038/mp.2012.19723337946
- Chess S. Autism in children with congenital rubella. J Autism Child Schizophr. 1971;1(1):33–47. doi:10.1007/BF015377415172438
- Maeyama K, Tomioka K, Nagase H, et al. Congenital cytomegalovirus infection in children with autism spectrum disorder: systematic review and meta-analysis. J Autism Dev Disord. 2018;48(5):1483–1491. doi:10.1007/s10803-017-3412-x29185167
- Atladóttir HO, Pedersen MG, Thorsen P, et al. Association of family history of autoimmune diseases and autism spectrum disorders. Pediatrics. 2009;124(2):687–694. doi:10.1542/peds.2008-244519581261
- Spann MN, Timonen-Soivio L, Suominen A, et al. Proband and familial autoimmune diseases are associated with proband diagnosis of autism spectrum disorders. J Am Acad Child Adolesc Psychiatry. 2019;58(5):496–505. doi:10.1016/j.jaac.2018.09.44430975444
- Vinet E, Pineau CA, Clarke AE, et al. Increased risk of autism spectrum disorders in children born to women with systemic lupus erythematosus: results from a large population-based cohort. Arthritis Rheumatol. 2015;67(12):3201–3208. doi:10.1002/art.3932026315754
- Theoharides TC, Tsilioni I, Patel AB, et al. Atopic diseases and inflammation of the brain in the pathogenesis of autism spectrum disorders. Transl Psychiatry. 2016;6(6):e844. doi:10.1038/tp.2016.7727351598
- Li X, Chauhan A, Sheikh AM, et al. Elevated immune response in the brain of autistic patients. J Neuroimmunol. 2009;207(1–2):111–116. doi:10.1016/j.jneuroim.2008.12.00219157572
- Morgan JT, Chana G, Pardo CA, et al. Microglial activation and increased microglial density observed in the dorsolateral prefrontal cortex in autism. Biol Psychiatry. 2010;68:368–376. doi:10.1016/j.biopsych.2010.05.02420674603
- Suzuki K, Sugihara G, Ouchi Y, et al. Microglial activation in young adults with autism spectrum disorder. JAMA Psychiatry. 2013;70(1):49–58. doi:10.1001/jamapsychiatry.2013.27223404112
- Young AMH, Campbell E, Lynch S, et al. Aberrant NF-kappaB expression in autism spectrum condition: a mechanism for neuroinflammation. Front Psychiatry. 2011;2:27. doi:10.3389/fpsyt.2011.0002721629840
- Adams F, Quesada JR, Gutterman JU, et al. Neuropsychiatric manifestations of human leukocyte interferon therapy in patients with cancer. JAMA. 1984;252(7):938–941. doi:10.1001/jama.1984.033500700560266748198
- Niiranen A, Laaksonen R, livanainen M, et al. Behavioral assessment of patients treated with alpha‐interferon. Acta Psychiatr Scand. 1988;78:622–626. doi:10.1111/j.1600-0447.1988.tb06395.x3232542
- Dada T, Rosenzweig JM, Al Shammary M, et al. Mouse model of intrauterine inflammation: sex-specific differences in long-term neurologic and immune sequelae. Brain Behav Immun. 2014;38:142–150. doi:10.1016/j.bbi.2014.01.01424486323
- Martin LA, Ashwood P, Braunschweig D, et al. Stereotypies and hyperactivity in rhesus monkeys exposed to IgG from mothers of children with autism. Brain Behav Immun. 2008;22(6):806–816. doi:10.1016/j.bbi.2007.12.00718262386
- Filiano AJ, Xu Y, Tustison NJ, et al. Unexpected role of interferon-γ in regulating neuronal connectivity and social behaviour. Nature. 2016;535(7612):425–429. doi:10.1038/nature1862627409813
- Rose DR, Careaga M, Van de Water J, et al. Long-term altered immune responses following fetal priming in a non-human primate model of maternal immune activation. Brain Behav Immun. 2017;63:60–70. doi:10.1016/j.bbi.2016.11.02027876552
- Patterson P. Infectious Behaviour: Brain-Immune Connections in Autism, Schizophrenia, and Depression. MIT Press; 2012.
- Allard M-J, Bergeron JD, Baharnoori M, et al. A sexually dichotomous, autistic‐like phenotype is induced by Group B Streptococcus maternofetal immune activation. Autism Res. 2017;10:233–245. doi:10.1002/aur.164727220806
- Schwartzer JJ, Careaga M, Chang C, et al. Allergic fetal priming leads to developmental, behavioral and neurobiological changes in mice. Transl Psychiatry. 2015;5(4):e543. doi:10.1038/tp.2015.4025849982
- Chen SW, Zhong XS, Jiang LN, et al. Maternal autoimmune diseases and the risk of autism spectrum disorders in offspring: a systematic review and meta-analysis. Behav Brain Res. 2016;296:61–69. doi:10.1016/j.bbr.2015.08.03526327239
- Gata-Garcia A, Diamond B. Maternal antibody and ASD: clinical data and animal models. Front Immunol. 2019;10:1129. doi:10.3389/fimmu.2019.0112931191521
- Brimberg L, Sadiq A, Gregersen PK, et al. Brain-reactive IgG correlates with autoimmunity in mothers of a child with an autism spectrum disorder. Mol Psychiatry. 2013;18(11):1171–1177. doi:10.1038/mp.2013.10123958959
- Piras IS, Haapanen L, Napolioni V, et al. Anti-brain antibodies are associated with more severe cognitive and behavioural profiles in Italian children with Autism Spectrum Disorder. Brain Behav Immun. 2014;38:91–99. doi:10.1016/j.bbi.2013.12.02024389156
- Bauman MD, Iosif A-M, Smith SEP, et al. Activation of the maternal immune system during pregnancy alters behavioural development of rhesus monkey offspring. Biol Psychiatry. 2014;75(4):332–341. doi:10.1016/j.biopsych.2013.06.02524011823
- Mostafa GA, Al-Ayadhi LY. The relationship between the increased frequency of serum antineuronal antibodies and the severity of autism in children. Eur J Paediatr Neurol. 2012;16(5):464–468. doi:10.1016/j.ejpn.2011.12.01022226851
- Frye RE, Sequeira JM, Quadros EV, et al. Cerebral folate receptor autoantibodies in autism spectrum disorder. Mol Psychiatry. 2013;18(3):369–381. doi:10.1038/mp.2011.17522230883
- Mostafa GA, El-Sherif DF, Al-Ayadhi LY, et al. Systemic auto-antibodies in children with autism. J Neuroimmunol. 2014;272(1–2):94–98. doi:10.1016/j.jneuroim.2014.04.01124837704
- Goncalves MVM, Harger R, Braatz V, et al. Pediatric acute-onset neuropsychiatric syndrome (PANS) misdiagnosed as autism spectrum disorder. Immunol Lett. 2018;203:52–53. doi:10.1016/j.imlet.2018.09.00930222991
- Orlovska S, Vestergaard CH, Bech BH, et al. Association of streptococcal throat infection with mental disorders: testing key aspects of the PANDAS hypothesis in a Nationwide Study. JAMA Psychiatry. 2017;74(7):740–746. doi:10.1001/jamapsychiatry.2017.099528538981
- Barger BD, Campbell JM, McDonough JD, et al. Prevalence and onset of regression within autism spectrum disorders: a meta-analytic review. J Autism Dev Disord. 2013;43(4):817–828. doi:10.1007/s10803-012-1621-x22855372
- Goin-Kochel RP, Esler AN, Kanne SM, et al. Developmental regression among children with autism spectrum disorder: onset, duration, and effects on functional outcomes. Res Autism Spectr Disord. 2014;8(7):890–898. doi:10.1016/j.rasd.2014.04.002
- Scott O, Shi D, Andriashek D, et al. Clinical clues for autoimmunity and neuroinflammation in patients with autistic regression. Dev Med Child Neurol. 2017;59(9):947–951. doi:10.1111/dmcn.1343228383115
- Thompson L, Gillberg C, Landberg S, et al. Autism with and without regression: a two-year prospective longitudinal study in two population-derived swedish cohorts. J Autism Dev Disord. 2019;49(6):2281–2290. doi:10.1007/s10803-018-03871-430734177
- DeLong GR, Bean SC, Brown FR, et al. Acquired reversible autistic syndrome in acute encephalopathic illness in children. Arch Neurol. 1981;38(3):191–194. doi:10.1001/archneur.1981.005100300850136162440
- Akcakaya NH, Tekturk P, Cagatay A, et al. Atypical enterovirus encephalitis causing behavioral changes and autism-like clinical manifestations: case report. Acta Neurol Belg. 2016;116(4):679–681. doi:10.1007/s13760-016-0614-526895551
- Marques F, Brito MJ, Conde M, et al. Autism spectrum disorder secondary to enterovirus encephalitis. J Child Neurol. 2014;29(5):708–714. doi:10.1177/088307381350831424782421
- Mankoski RE, Collins M, Ndosi NK, et al. Etiologies of autism in a case-series from Tanzania. J Autism Dev Disord. 2006;36(8):1039. doi:10.1007/s10803-006-0143-916897390
- Gillberg C. Onset at age 14 of a typical autistic syndrome. A case report of a girl with herpes simplex encephalitis. J Autism Dev Disord. 1986;16(3):369–375. doi:10.1007/BF015316653558293
- Gillberg IC. Autistic syndrome with onset at age 31 years: herpes encephalitis as a possible model for childhood autism. Dev Med Child Neurol. 1991;33:920–924. doi:10.1111/j.1469-8749.1991.tb14804.x1743418
- Baldaçara L, Diniz T, Parreira B, et al. Organic mental disorder after pneumococcal meningoencephalitis with autism-like symptoms. Braz J Psychiatry. 2011;33(4):410–411. doi:10.1590/S1516-4446201100040001622189932
- Ghaziuddin M, Al-Khouri I, Ghaziuddin N, et al. Autistic symptoms following herpes encephalitis. Eur Child Adolesc Psychiatry. 2002;11(3):142–146. doi:10.1007/s00787-002-0271-512369775
- Hacohen Y, Wright S, Gadian J, et al. N-methyl-d-aspartate (NMDA) receptor antibodies encephalitis mimicking an autistic regression. Dev Med Child Neurol. 2016;58(10):1092–1094. doi:10.1111/dmcn.1316927255282
- González-Toro MC, Jadraque-Rodríguez R, Sempere-Pérez Á, et al. Encefalitis antirreceptor de NMDA: dos casos pediátricos [Anti-NMDA receptor encephalitis: two paediatric cases]. Rev Neurol. 2013;57(11):504–508.24265144
- Scott O, Richer L, Forbes K, et al. Anti-N-methyl-D-aspartate (NMDA) receptor encephalitis: an unusual cause of autistic regression in a toddler. J Child Neurol. 2014;29(5):691–694. doi:10.1177/088307381350187524092894
- Matoq AA, Rappoport AS, Yang Y, et al. Anti-NMDA-receptor antibody encephalitis in infants. Epilepsy Behav Case Rep. 2015;4:99–101. doi:10.1016/j.ebcr.2015.07.00526744696
- Schieveld JNM. Case reports with a child psychiatric exploration of catatonia, autism, and delirium. Int Rev Neurobiol. 2006;72:195–206.16697299
- Khandaker GM, Zammit S, Lewis G, et al. A population-based study of atopic disorders and inflammatory markers in childhood before psychotic experiences in adolescence. Schizophr Res. 2014;152(1):139–145. doi:10.1016/j.schres.2013.09.02124268471
- Chang HY, Seo J-H, Kim HY, et al. Allergic diseases in preschoolers are associated with psychological and behavioural problems. Allergy Asthma Immunol Res. 2013;5(5):315–321. doi:10.4168/aair.2013.5.5.31524003389
- Dahl RE, Bernhisel-Broadbent J, Scanlon-Holdford S, et al. Sleep disturbances in children with atopic dermatitis. Arch Pediatr Adolesc Med. 1995;149(8):856–860. doi:10.1001/archpedi.1995.021702100300057633537
- Goodwin RD, Galea S, Perzanowski M, et al. Impact of allergy treatment on the association between allergies and mood and anxiety in a population sample. Clin Exp Allergy. 2012;42(12):1765–1771. doi:10.1111/j.1365-2222.2012.04042.x23181792
- Xu G, Snetselaar LG, Jing J, et al. Association of food allergy and other allergic conditions with autism spectrum disorder in children. JAMA Netw Open. 2018;1(2):e180279. doi:10.1001/jamanetworkopen.2018.027930646068
- Mostafa GA, Hamza RT, El-Shahawi HH, et al. Allergic manifestations in autistic children: relation to disease severity. J Paediatr Neurol. 2008;6:115–123.
- Shibata A, Hitomi Y, Kambayashi Y, et al. Epidemiological study on the involvements of environmental factors and allergy in child mental health using the Autism Screening Questionnaire. Res Autism Spectr Disord. 2013;7(1):132–140. doi:10.1016/j.rasd.2012.06.003
- Lyall K, Van de Water J, Ashwood P, et al. Asthma and allergies in children with autism spectrum disorders: results from the CHARGE study. Autism Res. 2015;8(5):567–574. doi:10.1002/aur.147125722050
- Boris M, Goldblatt A. Pollen exposure as a cause for the deterioration of neurobehavioural function in children with autism and attention deficit hyperactive disorder: nasal pollen challenge. J Nutr Environ Med. 2004;14:47–54. doi:10.1080/13590840410001695176
- Jyonouchi H. Autism spectrum disorders and allergy: observation from a pediatric allergy/immunology clinic. Expert Rev Clin Immunol. 2010;6(3):397–411. doi:10.1586/eci.10.1820441426
- Angelidou A, Alysandratos K-D, Asadi S, et al. Brief report: “allergic symptoms” in children with autism spectrum disorders. More than meets the eye? J Autism Dev Disord. 2011;41(11):1579–1585. doi:10.1007/s10803-010-1171-z21210299
- Theoharides TC. Is a subtype of autism an allergy of the brain? Clin Ther. 2013;35(5):584–591. doi:10.1016/j.clinthera.2013.04.00923688533
- Yadama AP, Kelly RS, Lee-Sarwar K, et al. Allergic disease and low ASQ communication score in children. Brain Behav Immun. 2020;83:293–297. doi:10.1016/j.bbi.2019.10.00831606476
- Kordulewska NK, Kostyra E, Chwała B, et al. A novel concept of immunological and allergy interactions in autism spectrum disorders: molecular, anti-inflammatory effect of osthole. Int Immunopharmacol. 2019;72:1–11. doi:10.1016/j.intimp.2019.01.05830953868
- de Theije CGM, Wu J, Koelink PJ, et al. Autistic-like behavioural and neurochemical changes in a mouse model of food allergy. Behav Brain Res. 2014;261:265–274. doi:10.1016/j.bbr.2013.12.00824333575
- Liezmann C, Klapp B, Peters E, et al. Stress, atopy and allergy: A re-evaluation from a psychoneuroimmunologic perspective. Dermatoendocrinol. 2011;3:37–40. doi:10.4161/derm.3.1.1461821519408
- Lefter R, Ciobica A, Timofte D, et al. A descriptive review on the prevalence of gastrointestinal disturbances and their multiple associations in autism spectrum disorder. Medicina (Kaunas). 2019;56(1):E11. doi:10.3390/medicina5601001131892195
- Lee M, Krishnamurthy J, Susi A, et al. Association of autism spectrum disorders and inflammatory bowel disease. J Autism Dev Disord. 2018;48(5):1523–1529. doi:10.1007/s10803-017-3409-529170940
- Kushak RI, Lauwers GY, Winter HS, et al. Intestinal disaccharidase activity in patients with autism: effect of age, gender, and intestinal inflammation. Autism. 2011;15(3):285–294. doi:10.1177/136236131036914221415091
- de Magistris L, Familiari V, Pascotto A, et al. Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives. J Pediatr Gastroenterol Nutr. 2010;51(4):418–424. doi:10.1097/MPG.0b013e3181dcc4a520683204
- Hughes HK, Rose D, Ashwood P, et al. The gut microbiota and dysbiosis in autism spectrum disorders. Curr Neurol Neurosci Rep. 2018;18(11):81. doi:10.1007/s11910-018-0887-630251184
- Torrente F, Anthony A, Heuschkel RB, et al. Focal-enhanced gastritis in regressive autism with features distinct from Crohn’s and Helicobacter pylori gastritis. Am J Gastroenterol. 2004;99(4):598–605. doi:10.1111/j.1572-0241.2004.04142.x15089888
- Walker SJ, Fortunato J, Gonzalez LG, et al. Identification of unique gene expression profile in children with regressive autism spectrum disorder (ASD) and ileocolitis. PLoS One. 2013;8(3):e58058. doi:10.1371/journal.pone.005805823520485
- Gorrindo P, Williams KC, Lee EB, et al. Gastrointestinal dysfunction in autism: parental report, clinical evaluation, and associated factors. Autism Res. 2012;5(2):101–108. doi:10.1002/aur.23722511450
- Chaidez V, Hansen RL, Hertz-Picciotto I, et al. Gastrointestinal problems in children with autism, developmental delays or typical development. J Autism Dev Disord. 2014;44(5):1117–1127. doi:10.1007/s10803-013-1973-x24193577
- Mazurek MO, Vasa RA, Kalb LG, et al. Anxiety, sensory over-responsivity, and gastrointestinal problems in children with autism spectrum disorders. J Abnorm Child Psychol. 2013;41(1):165–176. doi:10.1007/s10802-012-9668-x22850932
- Prosperi M, Santocchi E, Muratori F, et al. Vocal and motor behaviours as a possible expression of gastrointestinal problems in preschoolers with autism spectrum disorder. BMC Pediatr. 2019;19(1):466. doi:10.1186/s12887-019-1841-831779607
- Ding HT, Taur Y, Walkup JT, et al. Gut microbiota and autism: key concepts and findings. J Autism Dev Disord. 2017;47(2):480–489. doi:10.1007/s10803-016-2960-927882443
- Yap IKS, Angley M, Veselkov KA, et al. Urinary metabolic phenotyping differentiates children with autism from their unaffected siblings and age-matched controls. J Proteome Res. 2010;9(6):2996–3004. doi:10.1021/pr901188e20337404
- Williams BL, Hornig M, Parekh T, et al. Application of novel PCR-based methods for detection, quantitation, and phylogenetic characterization of Sutterella species in intestinal biopsy samples from children with autism and gastrointestinal disturbances. MBio. 2012;3(1):e00261–11. doi:10.1128/mBio.00261-1122233678
- Ng QX, Loke W, Venkatanarayanan N, et al. A systematic review of the role of prebiotics and probiotics in autism spectrum disorders. Medicina (Kaunas). 2019;55(5):129. doi:10.3390/medicina55050129
- Kang D-W, Adams JB, Coleman DM, et al. Long-term benefit of microbiota transfer therapy on autism symptoms and gut microbiota. Sci Rep. 2019;9(1):5821. doi:10.1038/s41598-019-42183-030967657
- Mangiola F, Ianiro G, Franceschi F, et al. Gut microbiota in autism and mood disorders. World J Gastroenterol. 2016;22(1):361–368. doi:10.3748/wjg.v22.i1.36126755882
- Furuta GT, Williams K, Kooros K, et al. Management of constipation in children and adolescents with autism spectrum disorders. Pediatrics. 2012;130(Suppl 2):S98–S105. doi:10.1542/peds.2012-0900H23118260
- Coury DL, Ashwood P, Fasano A, et al. Gastrointestinal conditions in children with autism spectrum disorder: developing a research agenda. Pediatrics. 2012;130(Suppl 2):S160–S168. doi:10.1542/peds.2012-0900N23118247
- Goodwin MS, Goodwin TC, Cowen MA. Malabsorption and cerebral dysfunction: a multivariate and comparative study of autistic children. J Autism Child Schizophr. 1971;1(1):48–62. doi:10.1007/BF015377425172439
- Herbert MR, Buckley JA. Autism and dietary therapy: case report and review of the literature. J Child Neurol. 2013;28(8):975–982. doi:10.1177/088307381348866823666039
- El-Rashidy O, El-Baz F, El-Gendy Y, et al. Ketogenic diet versus gluten free casein free diet in autistic children: a case-control study. Metab Brain Dis. 2017;32(6):1935–1941. doi:10.1007/s11011-017-0088-z28808808
- Whiteley P, Shattock P, Knivsberg AM, et al. Gluten- and casein-free dietary intervention for autism spectrum conditions. Front Hum Neurosci. 2013;6:344. doi:10.3389/fnhum.2012.0034423316152
- Pedersen L, Parlar S, Kvist K, et al. Data mining the ScanBrit study of a gluten- and casein-free dietary intervention for children with autism spectrum disorders: behavioural and psychometric measures of dietary response. Nutr Neurosci. 2014;17(5):207–213. doi:10.1179/1476830513Y.000000008224075141
- Calderoni S, Santocchi E, Del Bianco T, et al. Serological screening for celiac disease in 382 pre-schoolers with autism spectrum disorder. Ital J Pediatr. 2016;42(1):98. doi:10.1186/s13052-016-0308-x27852289
- Genuis SJ, Bouchard TP. Celiac disease presenting as autism. J Child Neurol. 2010;25(1):114–119. doi:10.1177/088307380933612719564647
- Sapone A, Bai JC, Ciacci C, et al. Spectrum of gluten-related disorders: consensus on new nomenclature and classification. BMC Med. 2012;10(1):13. doi:10.1186/1741-7015-10-1322313950
- Ludvigsson JF, Reichenberg A, Hultman CM, et al. A nationwide study of the association between celiac disease and the risk of autistic spectrum disorders. JAMA Psychiatry. 2013;70(11):1224–1230. doi:10.1001/jamapsychiatry.2013.204824068245
- Lau NM, Green PHR, Taylor AK, et al. Markers of celiac disease and gluten sensitivity in children with autism. PLoS One. 2013;8(6):e66155. doi:10.1371/journal.pone.006615523823064
- de Magistris L, Picardi A, Siniscalco D, et al. Antibodies against food antigens in patients with autistic spectrum disorders. Biomed Res Int. 2013;2013:729349. doi:10.1155/2013/72934923984403
- Caio G, Volta U, Tovoli F, et al. Effect of gluten free diet on immune response to gliadin in patients with non-celiac gluten sensitivity. BMC Gastroenterol. 2014;14(1):26. doi:10.1186/1471-230X-14-2624524388
- Massari S, Liso M, De Santis L, et al. Occurrence of nonceliac gluten sensitivity in patients with allergic disease. Int Arch Allergy Immunol. 2011;155(4):389–394. doi:10.1159/00032119621346369
- Carroccio A, Mansueto P, Iacono G, et al. Non-celiac wheat sensitivity diagnosed by double-blind placebo-controlled challenge: exploring a new clinical entity. Am J Gastroenterol. 2012;107(12):1898–1907. doi:10.1038/ajg.2012.23622825366
- Ashwood P, Murch SH, Anthony A, et al. Intestinal lymphocyte populations in children with regressive autism: evidence for extensive mucosal immunopathology. J Clin Immunol. 2003;23(6):504–517. doi:10.1023/B:JOCI.0000010427.05143.bb15031638
- Chen B, Girgis S, El-Matary W, et al. Childhood autism and eosinophilic colitis. Digestion. 2010;81(2):127–129. doi:10.1159/00025276520068312
- Hadjivassiliou M, Duker AP, Sanders DS. Gluten-related neurologic dysfunction. Handb Clin Neurol. 2014;120:607–619.24365341
- Peters SL, Biesiekierski JR, Yelland GW, et al. Randomised clinical trial: gluten may cause depression in subjects with non-coeliac gluten sensitivity - an exploratory clinical study. Aliment Pharmacol Ther. 2014;39(10):1104–1112. doi:10.1111/apt.1273024689456
- Besag FM. Epilepsy in patients with autism: links, risks and treatment challenges. Neuropsychiatr Dis Treat. 2017;14:1–10. doi:10.2147/NDT.S12050929296085
- Lewine JD, Andrews R, Chez M, et al. Magnetoencephalographic patterns of epileptiform activity in children with regressive autism spectrum disorders. Pediatrics. 1999;104(3 Pt 1):405–418. doi:10.1542/peds.104.3.40510469763
- Ertürk Çetin Ö, Korkmaz B, Alev G, et al. EEG abnormalities and long term seizure outcome in high functioning autism. Acta Neurol Belg. 2017;117(3):729–732. doi:10.1007/s13760-017-0785-828447214
- Strasser L, Downes M, Kung J, et al. Prevalence and risk factors for autism spectrum disorder in epilepsy: a systematic review and meta-analysis. Dev Med Child Neurol. 2018;60(1):19–29. doi:10.1111/dmcn.1359829119560
- García-Peñas JJ. Tratamiento con fármacos antiepilépticos en los sindromes de regresión autista [Antiepileptic drugs in the treatment of autistic regression syndromes]. Rev Neurol. 2005;40(Suppl 1):S173–S176.15736083
- Ko C, Kim N, Kim E, et al. The effect of epilepsy on autistic symptom severity assessed by the social responsiveness scale in children with autism spectrum disorder. Behav Brain Funct. 2016;12(1):20. doi:10.1186/s12993-016-0105-027350381
- Wang M, Jiang L, Tang X, et al. Levetiracetam is associated with decrease in subclinical epileptiform discharges and improved cognitive functions in pediatric patients with autism spectrum disorder. Neuropsychiatr Dis Treat. 2017;13:2321–2326. doi:10.2147/NDT.S14396628919764
- Veerappan VD, Sweetha B, Kavitha HR, et al. Two-year follow-up of isolated epileptiform discharges in autism: an endophenotypic biomarker? [published correction appears in Indian J Psychol Med. 2018 Nov-Dec;40(6):602]. Indian J Psychol Med. 2018;40(3):219–224. doi:10.4103/IJPSYM.IJPSYM_555_1729875528
- Swatzyna RJ, Tarnow JD, Turner RP, et al. Integration of EEG into psychiatric practice: a step toward precision medicine for autism spectrum disorder. J Clin Neurophysiol. 2017;34(3):230–235. doi:10.1097/WNP.000000000000036527893495
- Kokoszka MA, McGoldrick PE, La Vega-talbott M, et al. Epilepsy surgery in patients with autism. J Neurosurg Pediatr. 2017;19(2):196–207. doi:10.3171/2016.7.PEDS165127885946
- Shuper A, Mimouni M. Problems of differentiation between epilepsy and non-epileptic paroxysmal events in the first year of life. Arch Dis Child. 1995;73(4):342–344. doi:10.1136/adc.73.4.3427492200
- Zheng Z, Zhang L, Li S, et al. Association among obesity, overweight and autism spectrum disorder: a systematic review and meta-analysis. Sci Rep. 2017;7(1):11697. doi:10.1038/s41598-017-12003-428916794
- Kim E-K, Neggers YH, Shin C-S, et al. Alterations in lipid profile of autistic boys: a case control study. Nutr Res. 2010;30(4):255–260. doi:10.1016/j.nutres.2010.04.00220534328
- Hill AP, Zuckerman KE, Fombonne E. Obesity and autism. Pediatrics. 2015;136(6):1051–1061. doi:10.1542/peds.2015-143726527551
- Sanchez CE, Barry C, Sabhlok A, et al. Maternal pre-pregnancy obesity and child neurodevelopmental outcomes: a meta-analysis. Obes Rev. 2018;19(4):464–484. doi:10.1111/obr.1264329164765
- Wang Y, Tang S, Xu S, et al. Maternal body mass index and risk of autism spectrum disorders in offspring: a meta-analysis. Sci Rep. 2016;6(1):34248. doi:10.1038/srep3424827687989
- Delzenne NM, Neyrinck AM, Bäckhed F, et al. Targeting gut microbiota in obesity: effects of prebiotics and probiotics. Nat Rev Endocrinol. 2011;7(11):639–646. doi:10.1038/nrendo.2011.12621826100
- Weissman JR, Kelley RI, Bauman ML, et al. Mitochondrial disease in autism spectrum disorder patients: a cohort analysis. PLoS One. 2008;3(11):e3815. doi:10.1371/journal.pone.000381519043581
- Goh S, Dong Z, Zhang Y, et al. Mitochondrial dysfunction as a neurobiological subtype of autism spectrum disorder: evidence from brain imaging. JAMA Psychiatry. 2014;71(6):665–671. doi:10.1001/jamapsychiatry.2014.17924718932
- Rose S, Niyazov DM, Rossignol DA, et al. Clinical and molecular characteristics of mitochondrial dysfunction in autism spectrum disorder. Mol Diagn Ther. 2018;22(5):571–593. doi:10.1007/s40291-018-0352-x30039193
- Rose S, Frye RE, Slattery J, et al. Oxidative stress induces mitochondrial dysfunction in a subset of autism lymphoblastoid cell lines in a well-matched case control cohort. PLoS One. 2014;9(1):e85436. doi:10.1371/journal.pone.008543624416410
- Alabdali A, Al-Ayadhi L, El-Ansary A, et al. A key role for an impaired detoxification mechanism in the etiology and severity of autism spectrum disorders. Behav Brain Funct. 2014;10(1):14. doi:10.1186/1744-9081-10-1424776096
- Hollis F, Kanellopoulos AK, Bagni C, et al. Mitochondrial dysfunction in autism spectrum disorder: clinical features and perspectives. Curr Opin Neurobiol. 2017;45:178–187. doi:10.1016/j.conb.2017.05.01828628841
- Hadjixenofontos A, Schmidt MA, Whitehead PL, et al. Evaluating mitochondrial DNA variation in autism spectrum disorders. Ann Hum Genet. 2013;77(1):9–21. doi:10.1111/j.1469-1809.2012.00736.x23130936
- Tang G, Rios PG, Kuo SH, et al. Mitochondrial abnormalities in temporal lobe of autistic brain. Neurobiol Dis. 2013;54:349–361. doi:10.1016/j.nbd.2013.01.00623333625
- Palmieri L, Persico AM. Mitochondrial dysfunction in autism spectrum disorders: cause or effect? Biochim Biophys Acta. 2010;1797(6–7):1130–1137. doi:10.1016/j.bbabio.2010.04.01820441769
- Ming X, Stein TP, Barnes V, et al. Metabolic perturbance in autism spectrum disorders: a metabolomics study. J Proteome Res. 2012;11(12):5856–5862. doi:10.1021/pr300910n23106572
- Lasselin J, Capuron L. Chronic low-grade inflammation in metabolic disorders: relevance for behavioural symptoms. Neuroimmunomodulation. 2014;21(2–3):95–101. doi:10.1159/00035653524557041
- Spilioti M, Evangeliou AE, Tramma D, et al. Evidence for treatable inborn errors of metabolism in a cohort of 187 Greek patients with autism spectrum disorder (ASD). Front Hum Neurosci. 2013;7:858. doi:10.3389/fnhum.2013.0085824399946
- Krsička D, Geryk J, Vlčková M, et al. Identification of likely associations between cerebral folate deficiency and complex genetic- and metabolic pathogenesis of autism spectrum disorders by utilization of a pilot interaction modeling approach. Autism Res. 2017;10(8):1424–1435. doi:10.1002/aur.178028339176
- Kanner L. Autistic disturbances of affective contact. Nerv Child. 1943;2:217–250.
- Bell L, Wittkowski A, Hare DJ, et al. Movement disorders and syndromic autism: a systematic review. J Autism Dev Disord. 2019;49(1):54–67. doi:10.1007/s10803-018-3658-y30014250
- Bal VH, Fok M, Lord C, et al. Predictors of longer-term development of expressive language in two independent longitudinal cohorts of language-delayed preschoolers with Autism Spectrum Disorder [published online ahead of print, 2019 Aug 19]. J Child Psychol Psychiatry. 2019. doi:10.1111/jcpp.13117
- Cederlöf M, Larsson H, Lichtenstein P, et al. Nationwide population-based cohort study of psychiatric disorders in individuals with Ehlers-Danlos syndrome or hypermobility syndrome and their siblings. BMC Psychiatry. 2016;16:207. doi:10.1186/s12888-016-0922-627377649
- Baum SH, Stevenson RA, Wallace MT, et al. Behavioral, perceptual, and neural alterations in sensory and multisensory function in autism spectrum disorder. Prog Neurobiol. 2015;134:140–160. doi:10.1016/j.pneurobio.2015.09.00726455789
- O’Nions E, Happé F, Evers K, et al. How do parents manage irritability, challenging behaviour, non-compliance and anxiety in children with autism spectrum disorders? A meta-synthesis. J Autism Dev Disord. 2018;48(4):1272–1286. doi:10.1007/s10803-017-3361-429222612
- Goldschmidt J. What happened to Paul? Manifestation of abnormal pain response for individuals with autism spectrum disorder. Qual Health Res. 2017;27(8):1133–1145. doi:10.1177/104973231664441527117957
- Breau LM, Finley GA, McGrath PJ, et al. Validation of the non-communicating children’s pain checklist-postoperative version [published correction appears in Anesthesiology 2002 Sep;97(3):769]. Anesthesiology. 2002;96(3):528–535. doi:10.1097/00000542-200203000-0000411873023