Abstract
Background
While symptoms of deficient emotional self-regulation (DESR) have been long associated with attention-deficit/hyperactivity disorder (ADHD), there has been limited investigation of this aspect of the clinical picture of the disorder. The main aim of this study was to examine the predictive utility of DESR in moderating the course of ADHD children into adolescence.
Methods
Subjects comprised 177 children with and 204 children without ADHD followed for an average of 4 years (aged 6–18 years at baseline, 54% male). Subjects were assessed with structured diagnostic interviews and measures of psychosocial functioning. DESR was defined by the presence (n = 79) or absence (n = 98) of Child Behavior Checklist (CBCL)-DESR profile (score ≥ 180 < 210 total of Attention, Aggression, and Anxious/Depressed subscales) at the baseline assessment.
Results
Of subjects with DESR at baseline, 57% had DESR at follow-up. Persistent ADHD was significantly associated with DESR at follow-up (χ2 (1) = 15.37, P < 0.001). At follow-up, ADHD + DESR subjects had significantly more comorbidities (z = 2.55, P = 0.01), a higher prevalence of oppositional defiant disorder (z = 3.01, P = 0.003), and more impaired CBCL social problems t-score (t(227) = 2.41, P = 0.02) versus ADHD subjects.
Conclusion
This work suggests that a positive CBCL-DESR profile predicts subsequent psychopathology and functional impairments in children with ADHD suggesting that it has the potential to help identify children with ADHD at high risk for compromised outcomes.
Introduction
Although attention-deficit/hyperactivity disorder (ADHD) has been conceptualized as a disorder of deficient self-regulation,Citation1 the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision)Citation2 symptoms of the disorder have been limited to those of cognitive (inattention) and behavioral (hyperactivity/ impulsivity) deficits, leaving out deficient emotional self-regulation (DESR). DESR refers to: deficits in self-regulating the physiological arousal caused by strong emotions; difficulties inhibiting inappropriate behavior in response to either positive or negative emotions; problems refocusing attention from strong emotions; and disorganization of coordinated behavior in response to emotional activation.Citation3 DESR traits include low tolerance of frustration, impatience, quickness to anger, and being easily excited to emotional reactions. Although these traits may be a source of significant morbidity, there has been a paucity of research on the subject.Citation3–Citation6
The symptoms of DESR should not be confused with the emotional symptoms of mood disorders. DESR differs from the persistent and severe irritability often seen in pediatric mood disorder.Citation7 Unlike DESR, the abnormal mood of mood disorder is not defined by poor self-regulation and includes features that are not part of DESR (eg, the other mood criteria in DSM-IV).
We recently examinedCitation8 whether a unique profile of the Child Behavior Checklist (CBCL) would help identify DESR in children with ADHD. We defined DESR if a child had a sum of t scores of >180 but <210 (between one and two standard deviations [SD] above the mean) on the Anxiety/ Depression, Aggression, and Attention scales of the CBCL (CBCL-DESR). This profile was selected because of its conceptual congruence with the clinical concept of DESR and because its extreme (>210, more than 2 SD above the mean) form had been previously associated with severe forms of mood and behavioral dysregulation in children with ADHD.Citation9 We found that 44% of children with ADHD had a positive CBCL-DESR profile versus 2% of controls (P < 0.001). The CBCL-DESR profile was associated with elevated rates of anxiety and disruptive behavior disorders, as well as significantly more impairment in emotional and interpersonal functioning. These findings suggested that the CBCL-DESR profile helped identify a subgroup of ADHD children with a psychopathological and functional profile consistent with the clinical concept of DESR. DESR remained associated with poorer psychosocial functioning even after controlling for comorbid disorders, suggesting that DESR may represent a burdensome source of morbidity in children with ADHD that is partially independent of comorbid disorders such as oppositional defiant disorder. Others have examined this CBCL-DESR profile but not using the cutoffs defined by our group. Ayer et alCitation10 found that the profile was associated with lower functioning and child suicidal behavior. Althoff et alCitation11 found cross-informant agreement of the profile and describe its association with suicidal thoughts and behaviors. However, more information is needed as to the prognostic significance of this profile.
New insights into the role that DESR plays in the clinical picture of ADHD would have important clinical and scientific implications. Clinically, DESR could account for the frequent social interaction problems and impairments in several domains of major life activities that are commonly seen with ADHD and other disorders. If so, the assessment of DESR could be an important feature of child psychiatric assessment. Scientifically understanding the relationships between ADHD and DESR could provide new insight into the neural basis of emotional regulation separating cortical regulatory regions from limbic ones. It could also help identify genes associated with emotional dysregulation apart from those associated with other behavioral and cognitive features of psychopathology.
The main aim of this study was to assess the longitudinal course of DESR in ADHD children. To this end, we used longitudinal follow-up data from two identically designed large controlled studies of well characterized boys and girls with and without ADHD. We hypothesized that a positive CBCL-DESR profile will predict more psychopathology and poorer psychosocial functioning in children with ADHD at follow-up. To the best of our knowledge, this is the first investigation of this issue.
Materials and methods
Subjects
The methodology used in this study has been previously described.Citation12,Citation13 Briefly, subjects were derived from two identically designed longitudinal case-control family studies of ADHD. These studies recruited male and female subjects aged 6–18 years with (n = 140 boys, n = 140 girls) and without (n = 120 boys, n = 122 girls) DSM-III-R ADHD ascertained from pediatric and psychiatric clinics. Male subjects were assessed at baseline and at four-year follow-up while female subjects were assessed at baseline and at five-year follow-up. Potential subjects were excluded if they had been adopted or if their nuclear family was not available for study. We also excluded potential subjects if they had major sensorimotor handicaps (paralysis, deafness, blindness), psychosis, autism, inadequate command of the English language, or a Full Scale IQ less than 80. Parents and adult offspring provided written informed consent to participate, and parents also provided consent for offspring under the age of 18 years. Children and adolescents provided written assent to participate. The human research committee at Massachusetts General Hospital approved this study.
Measures
Psychiatric assessments of probands younger than 18 years relied on the Kiddie Schedule for Affective Disorders and Schizophrenia - Epidemiological Version (KSADS-E).Citation14,Citation15 Subjects 18 years of age and older were assessed with the Structured Clinical Interview for DSMCitation16,Citation17 (supplemented with modules from the K-SADS-E to assess childhood diagnoses). Diagnoses for this analysis were considered positive if full criteria were met within the past year of the assessment. We interviewed the mothers for all subjects and directly interviewed subjects older than 12 years. We combined data from direct and indirect interviews by considering a diagnostic criterion positive if it was endorsed in either interview. Interviewers blind to all previous information about the child and family assessed mothers and children.
The interviewers had undergraduate degrees in psychology and were extensively trained. Based on 500 assessments from interviews of children and adults, the median kappa coefficient for diagnoses was 0.98. Kappa coefficients for individual diagnoses included ADHD (0.88), cognitive disorder (1.0), major depression (1.0), mania (0.95), separation anxiety (1.0), agoraphobia (1.0), panic (0.95), and substance use disorder (1.0). We considered a disorder positive if DSM diagnostic criteria were unequivocally met.
A committee of board-certified child and adult psychiatrists who were blind to the subject’s ADHD status, referral source, and all other data resolved diagnostic uncertainties. Diagnoses presented for review were considered positive only when the committee determined that diagnostic criteria were met to a clinically meaningful degree. We estimated the reliability of the diagnostic review process by computing kappa coefficients of agreement for clinician reviewers. For these diagnoses, the median reliability between individual clinicians and the review committee assigned diagnoses was 0.87. Kappa coefficients for individual diagnoses included ADHD (1.0), conduct disorder (1.0), major depression (1.0), mania (0.78), separation anxiety (0.89), agoraphobia (0.80), panic (0.77), and substance use disorder (1.0).
All assessment personnel were blind to proband diagnosis (ADHD or control) and ascertainment site (psychiatric or pediatric). The diagnosis of major depression was made only if the depressive episode was associated with severe impairment.Citation18,Citation19 Since there are many anxiety disorders measured by our structured interviews, we aggregated them into a binary measure-coded positive if two or more anxiety disorders were endorsed, and negative otherwise. Two or more anxiety disorders previously provided a reasonable trade-off between case identification and the false positive rate when compared against an independently defined “anxiety standard” in youth with ADHD.Citation20 Psychoactive substance use disorder was defined as any alcohol abuse, alcohol dependence, substance abuse, or substance dependence. Total comorbidities were calculated as the number of up to six psychiatric disorders/categories (bipolar disorder, major depressive disorder, multiple anxiety disorders, oppositional defiant disorder, conduct/antisocial personality disorder, psychoactive substance use disorder) present at any time in the year before the structured interview.
Global functioning was assessed using the Global Assessment of Functioning Scale.Citation21 Psychosocial functioning was assessed using the Social Adjustment Inventory for Children and Adolescents (SAICA).Citation22 The SAICA provides an evaluation of children’s functioning in school, in spare time activities, and with peers, siblings, and parents. A SAICA subscale is an average of 3–11 Likert items (eg, 1 = not a problem, 2 = mild problem, 3 = moderate problem, 4 = severe problem) from an area of social functioning. Family functioning was defined using the Moos Family Environment Scale,Citation23 which uses standard scores with a mean of 50 and SD of 10. Higher family conflict and lower family cohesion and expressiveness scores indicate poorer family functioning. Socioeconomic status was measured using the five-point Hollingshead scale.Citation24
Assessment of deficient emotional self-regulation
Assessment of DESR relied on the CBCL,Citation25 completed at baseline and follow-up. A parent (usually the mother) of each participant completed the 1991 version of the Child Behavior Checklist for children aged 4–18 years. The CBCL is an affordable pencil and paper test completed by the child’s caregiver, requiring no administration by a physician or rater. The CBCL queries the parent about the child’s behavior in the past 6 months and aggregates this data into behavioral problem t scores.Citation25 A computer program calculates the t scores for each scale. Raw scores are converted to genderand age-standardized scores (t scores having a mean of 50 and a SD of 10). A minimum t score of 50 is assigned to scores that fall at midpoint percentiles of ≤50 on the syndrome scales to permit comparison of standardized scores across scales. DESR was defined as positive if the sum of the CBCL Attention Problems, Aggressive Behavior, and Anxious-Depressed t scores was ≥180 and <210. These cutoff scores represent, on average, 1 SD (t score = 60) to 2 SD (t score = 70) on each of the three selected CBCL subscales. Subjects with a sum of >210 on these CBCL subscales were excluded, because we previously showed that these subjects were at risk for developing bipolar disorder and associated impairments.Citation9
Statistical analysis
We compared ADHD probands with and without DESR on baseline demographic characteristics using t-tests, Pearson’s Chi-square, or Wilcoxon rank-sum tests. The one-year prevalence rates of baseline and follow-up psychiatric disorders were compared using logistic regression, and controlling for demographic confounders. Linear regression was used to test continuous variables (eg, Global Assessment of Functioning Scale) and negative binomial regression was used to test count variables (eg, total number of comorbidities). All tests were two-tailed with alpha set at 0.05.
Results
Of 280 subjects with ADHD and 242 subjects without ADHD at baseline, 242 and 229, respectively, had CBCL data (). Of the 242 ADHD subjects, 45 were dropped because they had an attention problems + aggressive behavior + an anxious-depressed (AAA) score of >210 at baseline. Of the 229 control subjects, five were dropped because they met criteria for DESR. Of the remaining 197 ADHD subjects and 224 control subjects, 177 (100 boys, 77 girls) and 204 (105 boys, 99 girls), respectively, had follow-up data. The mean follow-up time was 4.4 years (SD 1.1 years, range 3–9 years).
Figure 1 Participant flow chart.
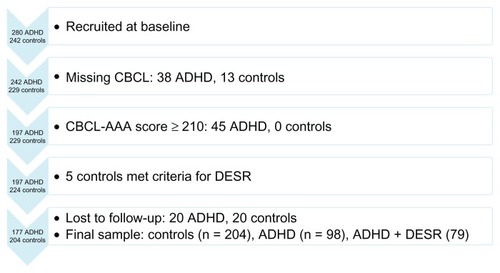
Of the 177 ADHD subjects with follow-up data, 119 subjects had CBCL data at the four-year follow-up. The kappa for DESR between the baseline and four-year followup assessments was 0.29 (P < 0.001), 57% of subjects with DESR at baseline also had DESR at follow-up (sensitivity, 33/58), 72% of subjects without DESR at baseline did not have DESR at follow-up (specificity, 44/61), the positive predictive value was 66% (33/50), and the negative predictive value was 64% (44/69). The intraclass correlation of the continuous AAA score between baseline and follow-up was 0.47 (P < 0.001). Persistent ADHD (full or subthreshold diagnosis in the last month) was significantly associated with DESR at follow-up (0/18 with remittent ADHD had DESR compared with 50/101 with persistent ADHD had DESR, χ2 (1) = 15.37, P < 0.001).
Comparisons were made between controls (n = 204) versus ADHD subjects with (ADHD + DESR, n = 79) and without DESR at baseline (ADHD, n = 98). Subjects used for this analysis (n = 381) did not significantly differ from subjects lost to follow-up (n = 40) on group status (P = 0.64), gender/study (P = 0.65), age (P = 0.58), socioeconomic status (P = 0.16), or ascertainment source (P = 0.69).
Sociodemographic characteristics
There were no differences between groups on gender, socioeconomic status, family intactness, or ascertainment source (). The ADHD + DESR group was significantly younger than controls. Therefore, all analyses controlled for age.
Table 1 Demographics, mean standard deviation or n (%)
Psychopathology at the 4-year follow-up
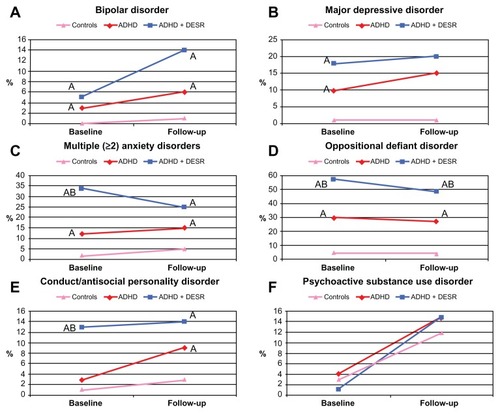
At the adolescent follow-up, both ADHD groups had significantly higher 1-year prevalence rates of bipolar (z = 3.89, P < 0.001), major depressive (z = 4.59, P < 0.001), multiple anxiety (z = 4.27, P < 0.001), and conduct/antisocial personality (z = 3.34, P = 0.001) disorders compared with controls (). In addition, the ADHD + DESR group continued to have significantly more total comorbidities at follow-up compared with the ADHD and control groups (1.4 versus 0.9, z = 2.55, P = 0.01 and 1.4 versus 0.3, z = 8.61, P < 0.001, respectively) as well as a significantly higher one-year prevalence of oppositional defiant disorder (z = 3.01, P = 0.003 and z = 7.28, P < 0.001, respectively, ). DESR was not significantly associated with mood disorders at baseline or follow-up (all P > 0.05).
Figure 2 One-year prevalence rates of disorders at baseline and follow-up by DESR status. (A) bipolar disorder, (B) major depressive disorder, (C) multiple (≥2) anxiety disorders, (D) oppositional defiant disorder, (E) conduct/antisocial personality disorder, and (F) psychoactive substance use disorder.
Abbreviation: ADHD, attention-deficit/hyperactivity disorder; DESR, deficient emotional self-regulation.
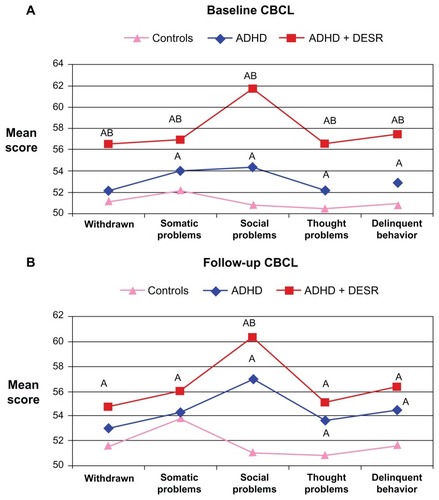
At follow-up, both ADHD groups continued to have higher thought problems and delinquent behavior t scores at follow-up compared with the controls (ADHD + DESR: t(227) = 5.38, ADHD: t(227) = 3.79, both P < 0.001). ADHD + DESR subjects continued to have a more impaired social problems t score compared with the ADHD and control groups (t(227) = 2.41, P = 0.02 and t(227) = 7.68, P < 0.001, respectively, ).
Figure 3 CBCL scales not used in deficient emotional self-regulation definition. (A) Baseline CBCL and (B) follow-up CBCL.
Abbreviation: ADHD, attention-deficit/hyperactivity disorder; CBCL, Child Behavior Checklist; DESR, deficient emotional self-regulation.
Psychosocial functioning
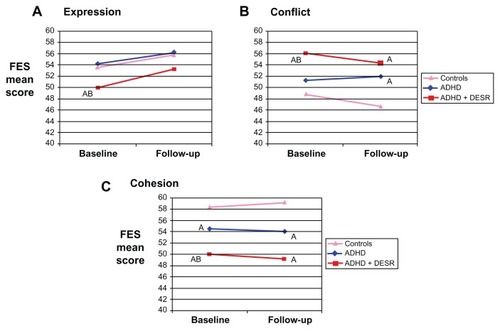
shows that the ADHD + DESR group continued to have poorer global functioning than the ADHD and control groups at follow-up (t(377) = −3.71, P < 0.001 and t(377) = −15.14, P < 0.001, respectively). While DESR was associated with significantly poorer social adjustment at baseline (t(365) = 4.38, P < 0.001), this no longer held true at follow-up due to the more impaired Social adjustment inventory for children and adolescents (SAICA) score in the ADHD group at follow-up (t(166) = 0.75, P = 0.45, ). The ADHD + DESR group had poorer Family Environment Scale scores at baseline (expression: t(372) = 2.35, P = 0.02; conflict: t(372) = 2.62, P = 0.009; cohesion: t(372) = 2.05, P = 0.04) and follow-up (expression: t(241) = 1.33, P = 0.18; conflict: t(241) = 0.96, P = 0.34; cohesion: t(242) = 1.66, P = 0.10) compared with the ADHD group, although the differences attained statistical significance only at baseline (). DESR was not associated with educational functioning (extra tutoring, placement in special class, repeated grade) at baseline or follow-up (all P > 0.30).
Figure 4 Psychosocial functioning by deficient emotional self-regulation. (A) Global Assessment of Functioning and (B) Social Adjustment Inventory for Children and Adolescents.
Abbreviation: ADHD, attention-deficit/hyperactivity disorder; DESR, deficient emotional self-regulation.
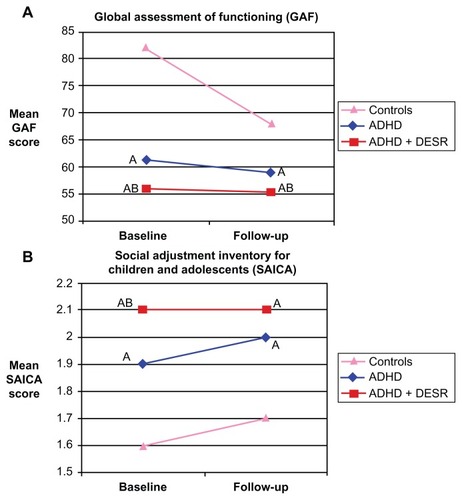
Figure 5 Current (last month) Family Environment Scale. (A) Expression, (B) conflict, and (C) cohesion.
Abbreviation: ADHD, attention-deficit/hyperactivity disorder; DESR, deficient emotional self-regulation; FES, Family Environment Scale.
Discussion
Our a priori definition of DESR based on moderate (>1 and <2 SD) elevations of CBCL-DESR identified a clinically meaningful subgroup of ADHD children at high risk for long-term morbidity and dysfunction consistent with current conceptualizations of DESR. The CBCL-DESR profile was associated at the follow-up assessment into adolescent years with higher rates of persistence of ADHD, more psychiatric comorbidity, more impaired scores on the Social Problems CBCL scale, as well as more impaired ratings of the Global Assessment of Functioning Scale. These findings suggest that the CBCL-DESR profile can help identify a clinically meaningful subgroup of children with ADHD with long-term compromised outcomes.
The finding that 57% of subjects with DESR at baseline also had DESR at follow-up suggests that DESR is a largely persistent trait (intraclass correlation of the continuous AAA score between baseline and follow-up was 0.47). Also noteworthy is the finding that DESR was predictive of a persistent course of ADHD; 50% of ADHD youth with persistent ADHD had DESR versus 0% in those without.
At the adolescent follow-up, ADHD + DESR subjects continued to have significantly more mean number of comorbidities compared with ADHD and control subjects as well as a significantly higher one-year prevalence of oppositional defiant disorder. These findings are congruent with those derived from analysis of the follow-up CBCL data showing more social problems associated with DESR in children with ADHD growing up. Although social functioning as measured by the SAICA was significantly associated with DESR at baseline and not at follow-up, subjects with DESR had the same high overall SAICA score at follow-up as they did at baseline ().
Also congruent with the psychopathological findings are those showing that children with ADHD + DESR continued to have poorer global functioning than the ADHD and control groups at follow-up. These findings are consistent with those of Whalen and Henker,Citation26 who found that emotional dysregulation in ADHD children disrupted the smoothness, reciprocity, and cooperative activities involved in peer relationships and with the suggestion by BarkleyCitation3 that DESR might account for a significant portion of the social dysfunction documented in ADHD. Several diagnostic and functioning measures that were associated with DESR at baseline were no longer significantly different at follow-up, including multiple anxiety disorders, conduct/antisocial personality disorder, several CBCL scales, SAICA, and Family Environment Scale. Therefore, the CBCL-DESR profile appears better at identifying children with ADHD with more extreme concurrent impairments than at identifying children at risk for future impairments. The fact that nearly half (43%) of the children with DESR at baseline no longer had DESR at follow-up may explain the somewhat weaker findings at follow-up. DESR was not associated with substance use disorders at baseline or follow-up. Because a substantial proportion of this sample had not yet entered the age of risk for substance use disorders, future studies should seek to confirm this lack of association.
Our longitudinal findings that children with ADHD with the CBCL-DESR profile were at significantly increased risk for oppositional defiant disorder but not for depression and bipolar disorder stand in contrast with findings of increased risks for these mood disorders associated with the CBCL-Pediatric Bipolar profile.Citation9 This latter profile requires very abnormal (2 SD) scores on the same scales of Anxiety/ Depression, Aggression, and Attention of the CBCL used to define the CBCL-DESR profile. These nonoverlapping profile findings between the high (2 SD) and the intermediate (1 SD) CBCL profiles (used to define DESR) support the hypotheses that these are mutually exclusive profiles that identify different clinical entities, with the severe profile likely identifying the extreme mood dysregulation associated with mood disorder, while the intermediate one is limited to deficient emotional self-regulation.
While both DESR and mood disorders involve emotional dysregulation, these constructs are substantially different clinically. The cardinal feature of mood disorders is the experience of strong emotions, not their self-regulation, the hallmark of DESR. Children who fulfilled the CBCL-DESR criteria were not more likely to have bipolar disorder or major depression or to have been hospitalized than other children with ADHD. In this regard, our data support the utility of the CBCL in defining DESR as a substantially different clinical entity than the CBCL-Juvenile Bipolar profile used to identify children at high risk for pediatric bipolar disorder. In fact, a comprehensive literature reviewCitation2 documents numerous studies in which children and adults with ADHD are highly likely to manifest DESR characterized by “low frustration tolerance, impatience, quickness to anger, and being easily excited to emotional reactions more generally”.
Our findings need to be viewed in light of some methodological limitations. Although our rate of retention was high (90%), our findings may have been affected by attrition bias. The large age range of our sample makes it difficult to assess any developmentally sensitive outcomes.
Our definition of emotional dysregulation relied on elevations in three CBCL clinical scales (A-A-A). Others have used this scale without cutoffs to measure dysregulated mood, attention, and behavior pathology across DSM-IV diagnoses. Citation10 One limitation of our CBCL definition of DESR is that, because it includes the Attention Problems Scale, which is known to be associated with ADHD, it may simply define a more severe form of ADHD, rather than a categorically different form of ADHD. In fact, our previous examinationCitation7 showed that DESR was associated with greater ADHD-associated impairment. On the other hand, our prior family studies of DESR suggest that ADHD + DESR is distinct from a familial perspective.Citation4,Citation27 Although we selected the CBCL-DESR profile from ongoing conceptualizations of DESR in the literature (most fully articulated by BarkleyCitation2) indexing deficits in self-regulating cognition and inhibiting behavior caused by strong emotions, we do not know whether our results would be replicated if other methods were used to define DESR. Investigating continuous measures or measures that do not have symptom overlap with other psychiatric diagnoses may help our understanding of DESR.
For example, Gioia et alCitation28 reported that children with ADHD had higher ratings on the Behavior Rating Inventory of Executive Function (BRIEF) Emotional Control subscale compared with healthy children. However, since these authors did not report correlations of their BRIEF-defined DESR (beyond impulsivity), it is unclear whether the BRIEF-Emotional Control Scale captures the same phenomenology as the CBCL-DESR profile. On the other hand, the validity of our construct of CBCL-DESR is supported by face validity, the consistency of the constituent symptoms with other definitions of DESR, its expression across a wide range of comorbid disorders and elevations of clinical scales, and its association with significant impairments beyond those accounted for by ADHD. Nevertheless, further research is needed to evaluate other definitions of DESR to determine its optimal definition. Because our sample was clinically referred and primarily Caucasian, our findings may not generalize to community samples and other ethnic groups.
Conclusion
Despite these considerations, these longitudinal findings indicate that intermediate (>1 and <2 SD) scores on the Anxiety/Depression, Attention and Aggression CBCL subscales can help identify a clinically meaningful subgroup of children with ADHD at high risk for more psychopathology and poorer functioning than other children with ADHD. These findings suggest that the CBCL-DESR profile may aid in the identification of children with deficient emotional regulation within and without the context of ADHD at high risk for compromised outcomes. Systematic efforts should be undertaken to determine the pharmacological or psychological interventions to best prevent these poor outcomes in children with ADHD and DESR.
Disclosure
JB is currently receiving research support from the following sources: Elminda, Janssen, McNeil, and Shire. In 2011, JB gave a single unpaid talk for Juste Pharmaceutical Spain, received honoraria from the MGH Psychiatry Academy for a tuition-funded continuing medical education course, and received an honorarium for presenting at an international scientific conference on ADHD. He also received an honorarium from Cambridge University Press for a chapter publication. JB received departmental royalties from a copyrighted rating scale used for ADHD diagnoses, paid by Eli Lilly, Shire and AstraZeneca; these royalties are paid to the Department of Psychiatry at MGH. In 2010, JB received a speaker’s fee from a single talk given at Fundación Dr Manuel Camelo AC in Monterrey Mexico. JB provided single consultations for Shionogi Pharma Inc and Cipher Pharmaceuticals Inc; the honoraria for these consultations were paid to the Department of Psychiatry at the MGH. JB received honoraria from the MGH Psychiatry Academy for a tuition-funded continuing medical education course. In 2009, JB received a speaker’s fee from the following sources: Fundacion Areces (Spain), Medice Pharmaceuticals (Germany), and the Spanish Child Psychiatry Association. In previous years, JB has received research support, consultation fees, or speaker’s fees for/ from the following additional sources: Abbott, Alza, AstraZeneca, Boston University, Bristol Myers Squibb, Celltech, Cephalon, Eli Lilly and Co, Esai, Forest, Glaxo, Gliatech, Hastings Center, Janssen, McNeil, Merck, MMC Pediatric, NARSAD, NIDA, New River, NICHD, NIMH, Novartis, Noven, Neurosearch, Organon, Otsuka, Pfizer, Pharmacia, Phase V Communications, Physicians Academy, The Prechter Foundation, Quantia Communications, Reed Exhibitions, Shire, The Stanley Foundation, UCB Pharma Inc, Veritas, and Wyeth.
TS has received research support from the following sources: Shire Laboratories Inc, Cephalon, Eli Lilly and Company, Glaxo-Smith Kline, Janssen, McNeil Pharmaceutical, Novartis Pharmaceuticals, Pfizer, and NIMH. TS has been a speaker or on a speaker’s bureau for the following pharmaceutical companies: Shire Laboratories Inc, Eli Lilly and Company, Glaxo-Smith Kline, Janssen, McNeil Pharmaceutical, and Novartis Pharmaceuticals. TS has been an advisor or on an advisory board for the following pharmaceutical companies: Shire Laboratories Inc, Cephalon, Eli Lilly and Company, Glaxo-Smith Kline, Janssen, McNeil Pharmaceutical, Novartis Pharmaceuticals, and Pfizer. TS receives research support from royalties and licensing fees on copyrighted ADHD scales through MGH Corporate Sponsored Research and Licensing. TS has a US patent application pending (Provisional Number 61/233,686), through MGH corporate licensing, on a method to prevent stimulant abuse.
CBHS has received research support from Abbott, Alza, Cephalon, Eli Lilly, the Hilda and Preston Davis Foundation, McNeil, Merck, New River, National Institutes of Health, Organon, Pfizer, Shire, and Takeda; has received support from Janssen-Ortho, McNeil, Novartis, and Shire for speaking and other educational activities; and has been a consultant/advisor for McNeil, Shire, Somaxon, and Takeda. CBHS has also received honoraria from Reed Medical Education (a logistics collaborator for the MGH Psychiatry Academy). Commercial entities supporting the MGH Psychiatry Academy are listed on the academy’s web site, http://www.mghcme.org.
In the past year, SVF received consulting income and research support from Shire and Alcobra and research support from the National Institutes of Health. In previous years, he received consulting fees or was on advisory boards or participated in continuing medical education programs sponsored by: Shire, McNeil, Janssen, Novartis, Pfizer and Eli Lilly. SVF receives royalties from books published by Guilford Press (Straight Talk about Your Child’s Mental Health) and Oxford University Press (Schizophrenia: The Facts).
CP, LH, and KOC report no conflict of interest in this work. This manuscript was supported in part by grants to JB from the National Institutes of Health (R01 HD36317, R01 MH50657) and to TS from Shire Pharmaceuticals.
References
- BarkleyRABehavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHDPsychol Bull1997121165949000892
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR4th ed text revisionWashington, DCAmerican Psychiatric Association2000
- BarkleyRADeficient emotional self-regulation: a core component of attention-deficit/hyperactivity disorderJournal of ADHD and Related Disorders201012537
- SurmanCBBiedermanJSpencerTDeficient emotional self regulation and adult attention deficit hyperactivity disorder: a family risk analysisAm J Psychiatry2011168661762321498464
- ReimherrFWMarchantBKWilliamsEDStrongREHallsCSoniPPersonality disorders in ADHD Part 3: Personality disorder, social adjustment, and their relation to dimensions of adult ADHDAnn Clin Psychiatry201022210311220445837
- JensenSARosenLAEmotional reactivity in children with attention-deficit/ hyperactivity disorderJ Atten Disord200482536115801335
- WozniakJRecognizing and managing bipolar disorder in childrenJ Clin Psychiatry200566Suppl 1182315693748
- SpencerTJFaraoneSVSurmanCBToward defining deficient emotional self-regulation in children with attention-deficit/ hyperactivity disorder using the Child Behavior Checklist: a controlled studyPostgrad Med20111235505921904086
- BiedermanJPettyCRMonuteauxMCThe child behavior checklist- pediatric bipolar disorder profile predicts a subsequent diagnosis of bipolar disorder and associated impairments in ADHD youth growing up: a longitudinal analysisJ Clin Psychiatry200970573274019389330
- AyerLAlthoffRIvanovaMChild Behavior Checklist Juvenile Bipolar Disorder (CBCL-JBD) and CBCL Posttraumatic Stress Problems (CBCL-PTSP) scales are measures of a single dysregulatory syndromeJ Child Psychol Psychiatry200950101291130019486226
- AlthoffRRRettewDCAyerLAHudziakJJCross-informant agreement of the Dysregulation Profile of the Child Behavior ChecklistPsychiatry Res2010178355055520510462
- BiedermanJFaraoneSVMickEClinical correlates of ADHD in females: findings from a large group of girls ascertained from pediatric and psychiatric referral sourcesJ Am Acad Child Adolesc Psychiatry199938896697510434488
- BiedermanJFaraoneSMilbergerSA prospective 4-year followup study of attention-deficit hyperactivity and related disordersArch Gen Psychiatry19965354374468624187
- OrvaschelHPsychiatric interviews suitable for use in research with children and adolescentsPsychopharmacol Bull19852147377454089105
- OrvaschelHSchedule for Affective Disorder and Schizophrenia for School-Age Children Epidemiologic Version5th edFort Lauderdale, FLNova Southeastern University, Center for Psychological Studies1994
- SpitzerRLWilliamsJBGibbonMFirstMBStructured Clinical Interview for DSM-III-R: Non-Patient Edition (SCID-NP, Version 1.0)Washington, DCAmerican Psychiatric Press1990
- FirstMSpitzerRGibbonMWilliamsJStructured Clinical Interview for DSM-IV Axis I DisordersWashington, DCAmerican Psychiatric Press1997
- GershonESHamovitJGuroffJJA family study of schizoaffective, bipolar I, bipolar II, unipolar, and normal control probandsArch Gen Psychiatry19823910115711677125846
- WeissmanMMLeckmanJFMerikangasKRGammonGDPrusoffBADepression and anxiety disorders in parents and children: Results from the Yale Family StudyArch Gen Psychiatry19844198458526466043
- MenninDBiedermanJMickEFaraoneSVTowards defining a meaningful anxiety phenotpye for research in ADHD childrenJ Atten Disord200034192199
- AssociationAPDSM-IV Sourcebook1Washington, DCAmerican Psychiatric Association1994
- JohnKGammonGDPrusoffBAWarnerVThe Social Adjustment Inventory for Children and Adolescents (SAICA): Testing of a new semistructured interviewJ Am Acad Child Adolesc Psychiatry19872668989113429410
- MoosRHMoosBSManual for the Family Environment ScalePalo Alto, CAConsulting Psychologists Press1974
- HollingsheadABFour Factor Index of Social StatusNew Haven, CTYale Press1975
- AchenbachTMManual for the Child Behavior Checklist/4-18 and the 1991 ProfileBurlington, VTUniversity of Vermont, Department of Psychiatry1991
- WhalenCKHenkerBThe social profile of attention-deficit hyperactivity disorderChild Adolesc Psychiatr Clin N Am199212395410
- BiedermanJSpencerTLomedicoADayHPettyCRFaraoneSVDeficient emotional self-regulation and pediatric attention deficit hyperactivity disorder: a family risk analysisPsychol Med201242363964621861953
- GioiaGAIsquithPKGuySCKenworthyLBrief Behavior Rating Inventory of Executive Function: ManualLutz, FLPsychological Assessment Resources2000