
Abstract
Purpose
Few studies have assessed the individual and joint effects of the mother’s, father’s and teacher’s mental health symptoms on schoolchildren’s behavior and emotional well-being simultaneously in the same study.
Patients and Methods
A cross-sectional survey was conducted among 8488 Chinese schoolchildren aged 6–17 years in northeast China. The Strengths and Difficulties Questionnaire (SDQ) and General Health Questionnaire (GHQ) were used to measure the mental health of the students, their parents and the teacher in charge of the class, respectively. A total of 6173 students (72.73%) with full mental health information from all three caretakers were included in the final analysis.
Results
We found a significantly elevated risk of mental health symptoms in children when their mothers (odds ratios (OR)=2.30, 95% CI=1.93–2.73), fathers (OR=2.08, 95% CI=1.73–2.50) and teachers (OR=1.18, 95% CI=1.01–1.39) reported poorer mental health, and the risk increased significantly with the number of the caretakers with mental symptoms. A father with poor mental health has both direct and indirect effects on a child’s emotional health, by worsening the influence of a mother’s poor mental health.
Conclusion
All three caretakers have a significant negative influence on schoolchildren’s emotional well-being, in the order of mother > father > teacher. It is desirable to assess and manage students’ mental health in the both the family and school contexts.
Background
It’s estimated that 10–20% of children and adolescents worldwide have mental health problems.Citation1,Citation2 During child development, the family and school, where children spend most of their time, play crucial roles. Mother, father and teacher are the three caretakers who may have the largest influence on children’s physical and moral development. Many studies have confirmed the strong and lasting impact of a mother’s mental health problems or psychiatric disorders on her children’s poor emotional, behavioral, social, and academic outcomes.Citation3–Citation6 A meta-analysis of 193 studies showed that maternal depression was significantly related to higher levels of internalizing, externalizing, and general psychopathology and negative affect/behavior.Citation3 A study of 2326 mothers and their infants showed that children of mothers with depressive symptoms performed more poorly in cognitive-linguistic functioning, were less cooperative and more problematic compared to children of less depressed mothers.Citation4 A follow-up study showed that the rate of depressive disorders in offspring of depressed parents was 2–3 times that of their counterpart of non-depressed parents, and they had more serious depressive symptoms.Citation5 Maternal depression is also associated with worse treatment outcomes for children with psychological disorders, even when children receive evidence-based care.Citation6 There is ample research on explanatory theories of the link between the mental health problems of caregivers and those of children and adolescents, such as the attachment theory,Citation7 developmental systems model,Citation8 allostatic load modelCitation9 and ‘context-process-outcomes’ model.Citation10 Children regard parents and teacher as a safe haven and seek proximity when they feel threatened or hurt in family or school contexts; lack of a sensitive response because of the caregiver’s poor mental health could damage the children’s capability to become socially and emotionally competent and cope with various allostatic loads.Citation7–Citation10 Although clinical psychology historically has been dominated by an attitude of mother-blaming, researchers and clinicians have gradually recognized that fathers are an important source of risk for children as well. Some studies have found that the associations were stronger between maternal than paternal psychological distress and the presence of internalizing problems in children,Citation11–Citation14 but there are also studies showing that the estimated associations are largely comparable between mothers and fathers.Citation15 A father may help attenuate the adverse effects of maternal psychopathology on child health by increasing his role as a caretaker of the child and by providing additional support to the child’s mother.Citation12,Citation16 Alternatively, if both parents are in poor mental health, the child may be at particularly high risk for poor mental health.Citation17 However, few studies in China have compared the influence of the mother’s and father’s mental health problems, as well as their interactions, on children’s mental health.
Schoolchildren spend more time in school than in any other formal institutional structure, and teachers often provide similar guidance and emotional support to that provided by parents, especially in the early years of a child’s education.Citation17,Citation18 The impacts of teachers’ mental health on students’ cognitive and social development may be more noteworthy in the context of China compared with western countries because Chinese students usually have a head teacher who is in charge of academic activities and other daily affairs over several years.Citation19 Previous studies have also shown that Chinese students experience higher levels of closeness with their teachers than their American and Dutch counterparts, implying that students in collectivistic cultures tend to experience more closeness in their relationship with teachers than students in individualistic cultures.Citation20 The Chinese context will provide us with unique opportunities to understand how a teacher’s mental health could influence their students’ mental health when they remain in a relatively stable environment over time. However, only a few studies have assessed the associations between teachers’ psychological distress and schoolchildren’s mental health problems, in a similar way to parental psychological distress, although there is mounting evidence that student–teacher relationships of poor quality, characterized by a lack of supportive interactions and high conflict, damage children’s academic and emotional development.Citation18,Citation21–Citation24 It is reasonable to hypothesize that the teachers’ psychological distress may have similar, although perhaps smaller, effects on schoolchildren’s mental health to that of their parents, and the combined effects of psychological distress in the three caretakers may have the greatest influence. China has the highest population of schoolchildren in the world. The highly competitive education system and high expectations from one-child families have meant that Chinese schoolchildren face increasing stress in both family and school.Citation25 It has been estimated that at least 30 million Chinese children and adolescents under 17 years old are troubled with various emotional or behavioral problems.Citation26 Therefore, it is of significance to assess whether and how a teacher’s mental health status influences a child’s emotional health. According to our knowledge, no study has assessed the combined effects of mental health problems in the three caretakers on schoolchildren simultaneously.
The aim of this study was to examine the following hypotheses: (1) The father’s and teacher’s mental health symptoms may have a smaller influence on Chinese schoolchildren’s mental health problems than the mother’s, with an order of the magnitude of the effect mother > father > teacher; (2) There may be interactions among the effects of mental health problems among the three caretakers, which may modify the associations between the adults’ mental health problems and children’s mental health.
Methods
Sample
The sampling procedure of the study has been described in detail previously.Citation25 Of a total of 9806 students eligible for the study, 9298 students returned the forms, and a qualified SDQ was collected from 8488 students. The study was a cross-sectional survey of Chinese schoolchildren aged 6–17 years, attending primary, junior and senior schools. These children lived in three cities and three rural counties in Liaoning province, located in northeast China. Two-stage sampling was conducted separately at each site by randomly selecting a sample of schools and then by obtaining a random sample of individuals at each selected school.
Procedure
We assessed the mental health status of children using three informants (the mother or father, the teacher, and students over 11 years old). An informant-rated version of the Strengths and Difficulties Questionnaire (SDQ)Citation26 was independently completed by the parent (either mother or father) and teachers of the students, while a self-reported version of the SDQ was completed by each student aged 11–17 years, but not by students aged 6–10 years. SDQ was selected because of its good validity and reliability, and used as a screening instrument for the two-phase survey to assess the prevalence of psychological disorder in Chinese children and adolescent.Citation25 To measure the mental health status of the three caretakers of the students, a 12-item General Health Questionnaire (GHQ-12)Citation27 was completed independently by the student’s mother, father and the teacher in charge of their class. The study protocol was reviewed and approved by the Institutional Review Board of the Liaoning Provincial Center for Disease Control and Prevention. The study was conducted in accordance with the Declaration of Helsinki on ethical principles for medical research involving human subjects. The ethics committee of Liaoning Provincial Center for Disease Control and Prevention (LNCDCP) approved the study. Parents and teachers were informed about the study and given an information sheet describing the study. Children were included if their parents had given written informed consent. This was considered to be the most appropriate mode as the study was of a simple, observational design with minimal risk. For the purpose of the present study, the students were included only if mental health information was available from all three caretakers, that is, the mother’s, father’s and teacher’s GHQs for all children. By these criteria, a total of 6173 students (72.73%) had all three GHQs from their mother, father and teacher, and were included in the analysis.
Instruments
Strengths and Difficulties Questionnaire (SDQ)
The SDQ is a screening questionnaire for mental health problems consisting of 25 items referring to the past 6 months (with 0 = not true, 1 = somewhat true, 2 = certainly true), comprising the following dimensions: emotional problems, conduct problems, hyperactivity/inattention, peer relationship problems and prosocial behavior. The items on the first four subscales generate the total difficulties score (0–40). The SDQ impact score is generated by the sum of five items: one item about distress, plus four items on social impairment in a) family life, b) friendships, c) learning and d) leisure activities.Citation26 The Chinese version of the SDQ has been validated in China.Citation28
General Health Questionnaire (GHQ)
The 12-item General Health Questionnaire (GHQ) was administrated to measure mental health problems.Citation21 The GHQ includes 12 items describing mood states over the previous 4 weeks. The original GHQ rating method (0–0–1-1) was used in the questionnaire. The total score ranged from 0 to 12 points, with higher scores indicating poor psychological well-being, which we defined as GHQ≥3. Research suggests that the GHQ-12 is appropriate for use with the Chinese population.Citation29 The Cronbach’s alpha in this study was 0.76.
Statistical Analysis
Analyses were performed using Statistical Package for the Social Sciences (SPSS), version 19.0 (SPSS Inc., Chicago, IL, USA) and structural equation modeling (SEM) was performed using SPSS Amos 19.0 (SPSS Inc.). Because Chinese norms for these scales have not yet been established, we used the cut-off points of “abnormal” SDQ scores from the UK to define the students with mental health problems.Citation30 We defined a student as having the “presence of a mental health problem” if anyone (parent, teacher, and/or students aged ≥11 years) classified the child as “abnormal” according to the corresponding cut-off values of the informantCitation31 and impact scores ≥1. The studies conducted both in TaiwanCitation32 and in mainland China showed that the optimum cut-off point obtained from the ROC curves was 3/4 for the Chinese version of GHQ-12, to support the choice of GHQ score ≥3. Therefore, we defined an adult as “positive for mental health problems” if the GHQ score was ≥3.Citation29
A standardized partial correlation coefficient was calculated to assess bivariate relationships between the GHQ scores of the mother, father, teacher and the SDQ scores rated by parents, teacher, and the students themselves, after adjusting for potential confounding variables (age, living area, gender, parental education, income, single child). We conducted bivariate and multivariate logistic regression analyses to identify factors associated with mental health problems, with calculation of odds ratios (ORs) and 95% confidence intervals (CIs). To assess the processes through which the three adults’ GHQ scores affected the average SDQ scores of the student as rated by parents, teacher and themselves (age ≥11). We assessed data model fitness of SEMs with the goodness-of-fit index (GFI), comparative fit index (CFI), and the root mean square error of approximation (RMSA). The goodness-of-fit was evaluated by the following criteria: GFI >0.90, CFI >0.90, and RMSEA <0.05.Citation33 Results of comparisons with a p-value of 0.05 or lower were considered to represent statistically significant differences.
Results
shows that 7629 (89.88%) fathers, 7636 (89.96%) mothers and 269 (86.50%) teachers returned a qualified GHQ for 8488 students with a completed SDQ; 6173 students had all three GHQs, from their mother, father and teacher, and were included in the analysis of the combined effects of the three caretakers’ psychological distress on the schoolchildren’s mental health symptoms. The percentage of students with 2, 1 and 0 completed GHQs was 21.28%, 5.04% and 0.99%, respectively. Of the 6173 students with completed GHQs from all three caretakers, the percentage of students with abnormal symptom scores and impact scores ≥1 was 12.39%.
Table 1 Number of GHQs Completed by the Mothers, Fathers and Teachers of 8488 Schoolchildren
As shown in , of the 6173 schoolchildren aged 11–17, males accounted for 48.60%, 50.25% lived in an urban area, 23.44% were over 15 years old, 6.90% lived in a divorce-affected family, 72.27% were the only one child in the family, 14.74% did not live together with their mother or father, and 4.94% had parents with psychiatric disorder. The percentage with GHQ ≥3 was 14.74%, 17.14% and 31.83% for the father, mother and teacher, respectively. The percentage of children with 1, 2 and 3 adults with GHQ ≥3 was 37.62%, 9.48% and 2.38%, respectively; 49.47% students had at least one adult with GHQ ≥3.
Table 2 Relationships of Demographic Characteristics with Mental Health Among 6173 Schoolchildren
We observed that the risk of mental health problems in the students was significantly elevated with increasing age and the number of adults with GHQ ≥3, and with decreasing maternal education level. The risk was also significantly increased for males (OR=1.56, 95% CI=1.34–1.82), divorced-affected families (OR=2.49, 95% CI=1.91–3.18), not living together with mother or father (OR=1.22, 95% CI=0.99–1.50), and parents with psychiatric disorder (OR=1.94, 95% CI=1.1.45–2.60). The risk for mothers with GHQ ≥3 (OR=2.30, 95% CI=1.93–2.73) was higher than that of the father (OR=2.08, 95% CI=1.73–2.50) and the teacher (OR=1.18, 95% CI=1.01–1.39).
shows the significant correlations between the mother’s GHQ scores and the SDQ scores rated by parents (r=0.28, p<0.01), teacher (r=0.05, p<0.01) and the students themselves (r=0.15, p<0.01); between the father’s GHQ scores and the SDQ scores rated by parents (r=0.19, p<0.01), teacher (r=0.06, p<0.01) and the students themselves (r=0.12, p<0.01); and between the teacher’s GHQ scores and the SDQ scores rated by the teacher (r=0.07, p<0.01). The mother’s GHQ scores were significantly correlated with the father’s GHQ scores (r=0.38, p<0.01).
Table 3 Standardized Partial Correlation Coefficients Between the GHQ Scores
shows that older age, male sex, urban area, family history of psychiatric disorder, divorce-affected family, and lower maternal education were risk factors for students’ mental health problems. The risks increased significantly with the number of the three caretakers with mental health problems, and mother remained in the multiple analysis model (OR=1.46, 95% CI=1.14–1.87).
Table 4 Multiple Regression Analysis of Factors Associated with Mental Health Problems Among Chinese Schoolchildren (n = 6173)
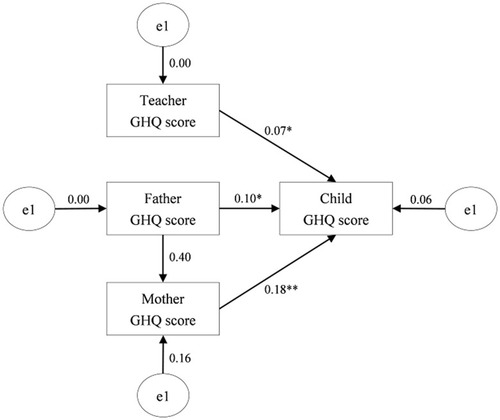
shows the inter-relationships among the GHQ scores of the three adults and the average SDQ score of the child using SEM. The statistical goodness-of-fit of the hypothesized model, denoted by the χ2 value, was 0.705 (df=2, p=0.703). The GFI was 1.000, the CFI was 1.000, and the RMSEA was p<0.001. The GHQ scores of the mother (path coefficient =0.18, p<0.001), father (path coefficient =0.10, p<0.001) and teacher (path coefficient =0.07, p<0.001) had significant positive influences on school children’s SDQ scores. In addition, the father’s GHQ score also had a significant indirect effect on children’s SDQ scores via the mother (path coefficient =0.40, p<0.001).
Figure 1 Hypothesized model for the interactions among the GHQ scores of three caretakers and the SDQ score of the student.
Discussion
The prevalence of mental health problems (GHQ ≥3) for the father and mother of the students was close to the levels previously reported in Chinese adults using the same GHQ criteria (12.8–21.8%).Citation34–Citation36 The higher prevalence of mental health problems in the teachers was consistent with the average levels of 12 studies on Chinese teachers using the Symptom Checklist-90 (SCL-90 (38.2%, range from 28.70 to 51.23%),Citation37 which could be related to burnout caused by the professional environment, serious competition, and a predominance of females, particularly in primary and secondary schools.Citation38 About one in two students faces at least one adult with mental health problems among the three caretakers in their daily life, and 9.48% and 2.38% face two or three adults with mental distress simultaneously, showing the troubling environment of the students in the family and school.
According to the authors’ knowledge, this is the first study to assess the combined influence of the mental health problems of the three important caretakers on schoolchildren’s psychological problems simultaneously in the same study. As expected, we found a significantly elevated risk of children’s mental health problems for not only mothers, but also fathers and teachers who reported poor mental health, which supports that the idea that mental problems in fathers and teachers also have independent effects on children’s mental health problems.Citation8,Citation16
The order (mother > father > teacher) in the odds ratios () and path coefficients (), the correlation coefficients between GHQ scores and SDQ scores (), and the significantly elevated risk associated with a mother with poorer mental health remaining in the multiple analysis supports the stronger influence of the presence of psychological distress in mothers than in fathers and in teachersCitation7–Citation10 and confirmed our hypothesis, which may be due to mothers’ dominant role as a primary caregiver. Some studies have suggested that paternal psychopathology becomes more important than maternal psychopathology in adolescence because there is less primary caretaking and fathers serve as important role models for socialization tasks,Citation16 but our results supported the more important influence of the mother than the father on children’s mental health in Chinese families.
The SEM results, however, showed that a father in poor mental health had not only a direct effect, but also an indirect effect via increasing the influence of a mother’s poor mental health, on a child’s emotional health. These findings are consistent with a theoretical model proposed by Goodman and Gotlib,Citation10 in which the degree of fathers’ depressive symptoms could moderate the relationship between depressive symptoms in mothers and children. They suggested that depressed fathers could amplify the association between depressive symptoms in mothers and those in their children by increasing genetic and environmental risk factors. Such risk factors in mothers and fathers can either have additive effects on their children or interact with each other. Our results also support the findings among American children that a father in better mental health may buffer the influence of a mother’s poorer mental health on a child’s behavior and emotional problems,Citation8 and that problems become most severe for children who have two or three caretakers with poor mental health.Citation8,Citation17 It was suggested that the father’s buffering effects resulted from: (1) being a healthy role model, (2) providing necessary parental care for the child, or (3) supporting depressed mothers in their caregiving of the child.Citation8,Citation10
Although the risk associated with teachers’ psychiatric problems was smaller than for parents, the small significantly increased risk associated with distressed teachers should not be overlooked, considering the long time spent in school and the huge numbers of Chinese students. In contrast to the significant correlations between parents’ GHQ scores and the SDQ scores rated by all three informants (parents, teachers and students themselves), the teacher’s GHQ score was only significantly correlated with the SDQ scores rated by the teacher (r=0.07, p<0.01), suggesting the important role of the teacher as observer/informant of the schoolchildren in the school environment; therefore, informant discrepancies should be considered when assessing their weaker influence on the student.Citation39 The specific role of the head teacher in the class and the closer relationship between students and teachers in China than in Western countries may also contribute to the significant associations,Citation19,Citation20 and highlight the specific influence of the head teacher in the unique Chinese school context. The significantly increasing risk associated with an increase in the number of the three caretakers with mental health problems () confirmed our hypothesis that the coexistence of two or three distressed adults significantly worsens the mental health of students, in line with the explanatory theories that lack of a sensitive response and necessary proximity from the parents and teachers because of their psychological distress could result in poor mental health among children, because they could not get expected support to cope with various allostatic loads when they face difficulties in family or school contexts,Citation11–Citation14 suggesting that the mental health of mother, father and teacher, as well as their interactions, should be addressed simultaneously. More attention should be given to establishing a healthy emotional environment in both the family and the school in order to improve schoolchildren’s mental health. A few studies have demonstrated positive effects of the treatment of parental psychopathology on children’s psychiatric symptoms,Citation40,Citation41 supporting the necessity for early screening and dealing with the mental health problems of both parents and teachers of the students.
The present results should be viewed in the context of several limitations of the study. First, the cross-sectional design limited our ability to make inferences about directionality or causality in the associations between three caretaker’s mental health problems and child mental health. Second, the analysis was conducted among schoolchildren with full information from all three adults completing the GHQ questionnaire; those children who could not get information from a parent or teacher were not included, and this may have led to a biased estimation of the prevalence of mental health problems because these children had a significantly lower rate of divorce in the family and significantly higher levels of maternal education level, family income, single children, and GHQ score ≥3 for mother, father and teacher compared with the 2315 students without complete GHQ information. Third, the use of UK criteria and cutoff values could be criticized. However, because the purpose of the present study was to assess the influence of the three caretakers’ GHQ scores on students’ mental health problems, we believe that the internal comparisons were valid. Fourth, mental health status was measured only for the teacher in charge of the class of the student, not all teachers of the students, which may have underestimated the influence of other teachers. Fifth, we cannot rule out the alternative explanation that the students’ mental health problems also influence the mental health of the three caretakers, and the symptomatology of parent or teacher may influence their report of student’s mental health symptoms, we believe the influence could be bidirectional.
Conclusions
The present paper confirmed that mental health problems in both fathers and teachers have similar, but smaller in magnitude, effects on students’ mental health to those in mothers. In addition, a father’s mental health is a powerful modifier of the influences of the mother’s mental health problems on their children, and the coexistence of two or three distressed adults significantly worsens the mental health of students. Our findings emphasize that a focus on mothers’ mental health will seriously limit our understanding of how the mental health of the three important caretakers affects children’s mental health. It is preferable to conduct a comprehensive assessment in both the family and school contexts when evaluating the risk factors related to mental health problems in schoolchildren. For future study, it will be of significance to assess whether and how screening for and managing mental health problems in mothers, fathers and teachers simultaneously will improve the emotional well-being of schoolchildren with mental health problems.
Abbreviations
SDQ, the Strengths and Difficulties Questionnaire; GHQ, General Health Questionnaire; SEM, structural equation model; GFI, goodness-of-fit index; CFI, comparative fit index; RMSA, root mean square error of approximation; LNCDCP, Liaoning Provincial Center for Disease Control and Prevention.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available because of our agreement with the parents of the schoolchildren, but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The manuscript does not contain clinical studies or patient data.
Author Contributions
Dr. Yan LJ, Li S, and Pan GW participated in the design of the study, performed the statistical analysis and wrote the paper. Dr. Na J, Mu HJ, Li YX, Zhang R, Sun JY, and Sun W carried out the questionnaire investigation. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Acknowledgments
The authors thank the schoolmasters, school teachers and parents of schoolchildren for their cooperation and support.
Disclosure
The authors have declared that no competing interests exist.
Additional information
Funding
References
- Kieling C, Baker-Henningham H, Belfer M, et al. Child and adolescent mental health worldwide: evidence for action. Lancet. 2011;378(9801):1515–1525. doi:10.1016/S0140-6736(11)60827-122008427
- Kato N, Yanagawa T, Fujiwara T, et al. Prevalence of children’s mental health problems and the effectiveness of population-level family interventions. J Epidemiol. 2015;25(8):507–516. doi:10.2188/jea.JE2014019826250791
- Goodman SH, Rouse MH, Connell AM, Broth MR, Hall CM, Heyward D. Maternal depression and child psychopathology: a meta-analytic review. Clin Child Fam Psychol Rev. 2011;14:1–27. doi:10.1007/s10567-010-0080-121052833
- Appelbaum M, Batten D, Belsky J, et al. Chronicity of maternal depressive symptoms, maternal sensitivity, and child functioning at 36 months. Dev Psychol. 1999;35:1297–1310.10493655
- Weissman MM, Warner V, Wickramaratne P, et al. Offspring of depressed parents: 10 years later. Arch Gen Psychiat. 1997;54(10):932–940. doi:10.1001/archpsyc.1997.018302200540099337774
- Swartz HA, Cyranowski JM, Cheng Y, Amole M. Moderators and mediators of a maternal depression treatment study: impact of maternal trauma and parenting on child outcomes. Compr Psychiatry. 2018;86:123–130. doi:10.1016/j.comppsych.2018.08.00130118995
- Bowlby J. Attachment and Loss: Vol.3. Loss: Sadness and Depression. NewYork: BasicBook; 1980.
- Pianta RC, Hamre B, Stuhlman M. Relationships between teachers and children. In: Reynolds W and Miller G, editors. Handbook of Psychology Vol. 7. Educational Psychology. Hoboken, NJ: John Wiley & Sons, Inc. 2003:199–234. doi:10.1002/0471264385.wei0710
- Roeser RW, Midgley C, Urdan TC. Perceptions of the school psychological environment and early adolescents’ psychological and behavioral functioning in school: the mediating role of goals and belonging. J Educ Psychol. 1996;88(3):408–422. doi:10.1037/0022-0663.88.3.408
- McEwen BS. Stress, adaptation, and disease. Allostasis and allostatic load. Ann N Y Acad Sci. 1998;840(1):33–44. doi:10.1111/j.1749-6632.1998.tb09546.x9629234
- Olfson M, Marcus SC, Druss B, et al. Parental depression, child mental health problems, and health care utilization. Med Care. 2003;41(6):716–721. doi:10.1097/01.MLR.0000064642.41278.4812773837
- Robert SK, Dominique B, Robert CW. Combined effect of mothers’ and fathers’ mental health symptoms on children’s behavioral and emotional well-being. Arch Pediat Adol Med. 2004;158(8):721–729. doi:10.1001/archpedi.158.8.721
- Gao F, Ling W. [Association between students’ and teachers’ mental health in middle and primary schools of Shanghai city]. Chin Ment Health J. 1999;13:44. [Chinese]
- Goodman SH, Gotlib IH. Risk for psychopathology in the children of depressed mothers: a developmental model for understanding mechanisms of transmission. Psychol Rev. 1999;106(3):458–490. doi:10.1037/0033-295X.106.3.45810467895
- Stratton KJ, Edwards AC, Overstreet C, et al. Caretaker mental health and family environment factors are associated with adolescent psychiatric problems in a Vietnamese sample. Psychiat Res. 2014;220(1–2):453–460. doi:10.1016/j.psychres.2014.08.033
- Connell AM, Goodman SH. The association between psychological distress in fathers versus mothers and children’s internalizing and externalizing behavior problems: a meta-analysis. Psychol Bull. 2002;128(5):746–773. doi:10.1037/0033-2909.128.5.74612206193
- Foley DL, Pickles A, Simonoff E, et al. Parental concordance and comorbidity for psychiatric disorder and associate risks for current psychiatric symptoms and disorders in a community sample of juvenile twins. J Child Psychol Psyc. 2001;42(3):381–394. doi:10.1111/1469-7610.00731
- Hamre BK, Pianta RC. Early teacher-child relationships and the trajectory of children’s school outcomes through eighth grade. Child Dev. 2001;72(2):625–638. doi:10.1111/1467-8624.0030111333089
- Li J. The characteristic of Chinese class instruction and its contribution to the world. Mod Teach Z. 2015;2:35–40.
- Chen M, Zee M, Koomen HMY, Roorda DL. Understanding cross-cultural differences in affective teacher-student relationships: a comparison between Dutch and Chinese primary school teachers and students. Sch Psychol. 2019;76:89–106. doi:10.1016/j.jsp.2019.07.011
- Zhang X, Sun J. The reciprocal relations between teachers’ perceptions of children’s behavior problems and teacher-child relationships in the first preschool year. J Genet Psychol. 2011;172(2):176–198. doi:10.1080/00221325.2010.52807721675546
- Miller-Lewis LR, Sawyer AC, Searle AK, et al. Student-teacher relationship trajectories and mental health problems in young children. BMC Psychol. 2014;2(1):27. doi:10.1186/s40359-014-0027-225685350
- Mashburn AJ, Pianta RC. Social relationships and school readiness. Early Educ Dev. 2006;17(1):151–176. doi:10.1207/s15566935eed1701_7
- Myers SS, Pianta RC. Developmental commentary: individual and contextual influences on student-teacher relationships and children’s early problem behaviors. J Clin Child Adolesc. 2008;37(3):600–608. doi:10.1080/15374410802148160
- Yang XL, Jiang C, Pan W, et al. Prevalence of psychiatric disorders among children and adolescents in northeast China. PLoS One. 2014;9(10):e111223. doi:10.1371/journal.pone.011122325360718
- Goodman R. The extended version of the strengths and difficulties questionnaire as a guide to child psychiatric caseness and consequent burden. J Child Psychol Psyc. 1999;40(5):791–799. doi:10.1111/1469-7610.00494
- Goldberg DP, Hillier VF. A scaled version of the general health questionnaire. Psychol Med. 1979;9(1):139–145. doi:10.1017/S0033291700021644424481
- Du Y, Kou J, Coghill D. The validity, reliability and normative scores of the parent, teacher and self report versions of the strengths and difficulties questionnaire in China. Child Adol Psych Men. 2008;29(2):8.
- Yang TZ, Huang L, Wu Z. [The application of Chinese health questionnaire for mental disorder screening in community settings in mainland China]. Zhonghua Liu Xing Being Xue Za Zhi. 2003;24(9):769–773. [Chinese]
- SDQ: Information for researchers and professionals about the strengths & difficulties questionnaires; 2008. Available from: http://www.sdqinfo.com. Accessed 204, 2020.
- Goodman R. The strengths and difficulties questionnaire: a research note. J Child Psychol Psyc. 1997;38(5):581–586. doi:10.1111/j.1469-7610.1997.tb01545.x
- Chong MY, Wikinson G. Validation of 30- and 12-item versions of the Chinese Health Questionnaire (CHQ) in patients admitted for general health screening. Psychol Med. 1989;19(2):495–505. doi:10.1017/S00332917000125262788292
- Byrne BM. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming (1st ed.). Psychology Press. 2000. doi:10.4324/9781410600219
- Xu Y, Li J. Analysis of psychological health of registered permanent residents in Songjiang. Med J Chin People Health. 2014;26:54–56.
- Yuan JZ, Zu WB, Li XH, et al. [Mental health survey with General Health Questionnaire (GHQ) among 2749 adults in the community]. Shanghai Arch Psychiatry. 2005;17:27–28. [Chinese]
- Han C. [Study on the currents status and risk factors of mental health among Chinese farmers in four counties]. Master’s Thesis, Shandong University. 2011. [Chinese]
- Gao MS. [Study on the findings of survey into teachers’ psychological health]. J Beijing Inst Educ. 2009;4:10–13. [Chinese]
- Zhang LL, Zhao JP, Xiao HQ, et al. Mental health and burnout in primary and secondary school teachers in the remote mountain areas of Guangdong Province in the People’s Republic of China. Neuropsych Dis Treat. 2014;10:123–130. doi:10.2147/NDT.S56020
- De Los Reyes A, Kazdin AE. Informant discrepancies in the assessment of childhood psychopathology: a critical review, theoretical framework, and recommendations for further study. Psychol Bull. 2005;131(4):483–509. doi:10.1037/0033-2909.131.4.48316060799
- Weissman MM, Pilowsky DJ, Wickramaratne PJ, Talati A, Wisniewski SR, Fava M. Remissions in maternal depression and child psychopathology: a STAR*D-child report. JAMA. 2006;295(12):1389–1398. doi:10.1001/jama.295.12.138916551710
- Garber J, Clarke GN, Weersing VR, et al. Prevention of depression in at-risk adolescents: a randomized controlled trial. JAMA. 2009;301(21):2215–2224. doi:10.1001/jama.2009.78819491183