Abstract
Objective
Depression illnesses are commonly observed in hemodialysis (HD) patients, which can influence the quality of life of end-stage renal disease patients. We evaluate the prevalence and predictive risk factors of depression in the Arab population undergoing HD in Nazareth, Israel.
Methods
We conducted a prospective study that included 71 patients in the HD unit with a mean age of 61.9 ± 14.13 years who had undergone HD and 26 healthy control subjects with a mean age of 59.3 ± 7.3. Beck’s Depression Inventory and Hamilton Depression Scale assessments were administered. Blood analysis for hematological and biochemical parameters was obtained. Diagnosis was made using the Diagnostic and Statistical Manual of Mental Disorders scale to correlate psychological variables with clinical, hematological, and biochemical parameters. Statistical analysis was carried out using analysis of variance followed by Tukey post-hoc multiple comparison tests.
Results
The prevalence of depression was 43.7% in HD patients. Between HD patients and controls, cortisol values were 16.96 ± 0.5476 and 11.96 ± 1.116, respectively (P < 0.0001; 95% confidence intervals [CI]: 2.416–6.825). Between depressed HD patients versus control subjects, cortisol values were 16.48 ± 0.72 and 11.96 ± 1.116, respectively (P = 0.0013; 95% CI: 1.878–7.184). Hematological and biochemical parameters were compared between depressed HD and nondepressed patients, but differences between the two groups were found to be insignificant (P > 0.05).
Conclusion
Our HD patients were severely depressed. Studies of glucocorticoid turnover activity such as cortisol, a potent chemical stress hormone, may be used as a model and marker for early diagnosis of depression among HD patients. The strong familial support system in Arabic traditions has failed to decrease depression among these patients.
Introduction
Depression is the most common psychological problem encountered in patients with end-stage renal disease (ESRD)Citation1–Citation3 and hemodialysis (HD) patients. HD is the most prevalent form of renal replacement therapy, with over 75% of ESRD patients treated using this modality.Citation4,Citation5 HD drastically and negatively affects the quality of life and life expectancy, with both physical and psychological effects.Citation6,Citation7 The experience of multiple losses, including kidney function, the global influence on family roles, work competence, sexual function, time, and mobility, significantly and negatively impact the lives of sufferers.Citation6–Citation9 Further stressors, including medication effectsCitation9 dietary constraints, fear of death, and dependency upon treatmentCitation10–Citation12 may affect quality of life and exacerbate feelings of a loss of control. Depression is widely believed to be the most common psychopathological condition among patients with ESRD.Citation9,Citation13–Citation15
While prevalent, depression is still often unrecognized,Citation16 reflecting a lack of routine psychological evaluation among this patient population.Citation17 The consequences of unidentified depression management among dialysis patients may be significant. Co-morbid depressive illnesses amplify the impact of chronic illnesses and increase functional disability and the use of health care services.Citation18 Nephrologists are well-aware that the most common psychopathological conditions occurring in patients with HD are depression and depressive symptoms.Citation9,Citation13–Citation15,Citation19–Citation21
Recent studies that employed Beck’s Depression Inventory (BDI) have reported remarkably similar findings.Citation2,Citation21,Citation22 The BDI is one of the most commonly used screening tools for depression in the dialysis population and is a self-rating tool that measures cognitive–affective symptoms and attitudes, impaired performance, and somatic symptoms. Furthermore, Wuerth et alCitation23 observed that when these patients were subsequently evaluated by a trained psychiatric interviewer for the presence of clinical depression, 85% of dialysis patients with BDI scores of 11 or greater met the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria for the diagnosis of major depression and had scores of 17 or more on the 21-item Hamilton Depression Scale.Citation23
The BDI is a commonly employed tool for identifying depression, has been extensively validated in various studies,Citation24–Citation26 and has been compared with the Hamilton Depression Rating Scale and the Montgomery-Asburg Depression Rating Scale, which are both expert-administered scales.Citation27–Citation32 In identifying depression, the BDI has been reported to exhibit discriminative validity.Citation26 Our results suggest that there is fair to good interpreter agreement in terms of presence of a depressed mood between patients and controls; agreement was highest among patients with the most intact cognition.
Even after years of study, researchers estimate that the prevalence of depression among dialysis patients varies widely from 5%–50%.Citation19,Citation33–Citation36 These differences have been attributed to varying criteria, methodology, and screening tools used to diagnose depression.Citation1,Citation3 The best estimates of prevalence are between 20% and 30%,Citation17,Citation6 but the reported variations vary significantly due in part to the type of assessment tool employed.Citation35,Citation37
The prevalence of major depression in the general population is approximately 1.1%–15% for men and 1.8%–23% for women.Citation6,Citation38 However, the prevalence of major depression among ESRD patients is approximately 20%–30%, and it may be as high as 47%.Citation13,Citation14,Citation38,Citation39 Some studies have indicated that moderate depressive syndromes are common in approximately 25% of ESRD patients, and that major depression is common in 5%–22% of ESRD patients.Citation40,Citation41
As described above, the prevalence of depression in patients with HD varies according to the test being used. It has been found to be 50% in patients with HD using screening tools such as BDI, 10% using the Multiple Affect Adjective Check List, but in only 5% when a diagnosis was made by psychiatric interview using the American Psychiatric Association standards published in the DSM. Postulated explanations for these wide-ranging estimates vary among medical professionals; for example, in a British study, a primary nurse diagnosed depression in 41.9% of patients, but the nephrology team diagnosed depression in only 24.2%. According to BDI scores, the rate was 38.7%.Citation37
Additional reasons such as different cultural values influence estimated prevalence data of depression; for example, the Dialysis Outcomes and Practice Patterns Study data show that physician-diagnosed depression rates ranged from 2.0% in Japan to 21.7% in the United States, but the rate of self-reported depression in these countries using the Center for Epidemiological Studies Depression Screening Index (CES-D) was similar and much higher: 40.0% in Japan and 39.2% in the US.Citation19 Additionally, timing of screen depression screening is important. Experts have cautioned that the first 3–6 months of dialysis is an unstable and critical period, and that levels of depression may change over time.Citation17 Indeed, screening during the first 6 months of a patient’s dialysis treatment is complicated because it is a very traumatic time. There is powerful, pervasive grief, and symptoms of uremia that must to be considered. Patients should be reassessed every 3–4 months to determine whether changes have occurred.
The etiology of dialysis-related depression is multifactorial and is related to biological, psychological, and social mechanisms. Biological mechanisms include increased cytokine levelsCitation6 and possible genetic predisposition.Citation42,Citation43 Psychological and social factors include feelings of hopelessness, perceptions of loss and lack of control, job loss, and altered family and social relationships.Citation46 Another trigger of depression among HD patients is fatigue, which is a subjective symptom characterized by tiredness, weakness, and lack of energy. Approximately 60%–97% of patients on HD experience some fatigue, which is negatively correlated with quality of life.Citation44,Citation45
Relationship between depression and cortisol
Depression is a very heterogeneous disorder with many different etiologies. By understanding the underlying causes of depression, progress towards effective treatment can be made.
Studies have demonstrated a connection between cortisol levels and depression. However, the results of many studies continue to both contradict each other as well as add to the current understanding.
Cortisol, a glucocorticoid hormone, is essential to human brain functioning. Produced by the adrenal glands, cortisol helps cells to create energy. When a body experiences stress, whether physical, mental, or emotional, cortisol production by the adrenals is upregulated in order to protect the body. This increase in cortisol is part of what is known as the “fight-or-flight” response, which occurs when a body prepares itself to combat a stressful event. This response is critical to an individual’s ability to act quickly in emergency situations.
Rather than an “on–off ” causation effect, studies continue to allude to a broad middle ground of impact between cortisol levels and depression. Balanced hormone levels, particularly regarding quantity and timing, appear to be important for mental health. Theories regarding the connection between cortisol and depression continue to be proposed.
In a study of 1588 participants, Vreeburg et alCitation46 showed a possible increased biological propensity for depression when higher cortisol awakening responses were observed. This large cohort study showed significant, although modest, associations between major depressive disorder (MDD) and specific hypothalamic–pituitary–adrenal (HPA) axis indicators. Because a higher cortisol awakening response was observed among both subjects with current MDD and subjects with remitted MDD, an increased biological vulnerability for depression was indicated.Citation46
It is known that in normal people, cortisol level in the bloodstream peaks in the morning, and then decreases as the day progresses. In depressed people, however, cortisol peaks earlier in the morning and does not level off or decrease in the afternoon or evening. Although the exact mechanism that causes depression is unknown, clinical studies suggest that chronically elevated cortisol may induce clinical depression by affecting central serotonergic neurotransmission.Citation47,Citation48
Because patients with major depression exhibit decreased brain serotonin (5-hydroxytryptamine [5-HT]) function and elevated cortisol secretion, it is generally accepted that changes in serotonin and cortisol are related to depression. A more recent study suggested that elevated cortisol levels, likely caused by stressful life events, may lower brain 5-HT function, leading to a depressive state.Citation49 This study ties abnormalities in cortisol secretion and 5-HT function into a causal chain in which cortisol is the key biological mediator through which life stress lowers brain 5-HT function, causing depression in vulnerable individuals.Citation49
Du’s research teamCitation50 concluded not only that cortisol is necessary for coping, but also that chronically elevated glucocorticoids, as can occur during ongoing stressful situations, work against the body at a cellular level. Their article suggests that this chronic stress-related cell damage may cause physical and mental illness such as depression.Citation50
Additionally, growing evidence suggests that specific types of chronic difficulty, such as caring for a relative with dementia, can be associated with increased cortisol secretion, Citation51 indicating that life events and difficulties can result in cortisol hypersecretion, but that this does not necessarily lead to development of a depressive disorder.
However, some animal studies suggest that elevated cortisol levels may enhance 5-HT neurotransmission by decreasing the sensitivity of inhibitory 5-HT1A cell body autoreceptors.Citation52 From this viewpoint, elevated cortisol levels may promote resilience to environmental adversity. Some subjects may respond to ‘stress levels’ of cortisol by developing depression, but in these cases cortisol hypersecretion must interact with other predisposing factors. In most moderately depressed patients in primary care, increased cortisol secretion may not be an important pathophysiological factor.Citation52
In contrast, other studies have shown that mice injected with cortisol developed symptoms of depression. They suggest that high cortisol levels may decrease serotonin function, leading to depression.Citation53,Citation54
Mackin and YoungCitation55 reported that abnormal cortisol levels were first observed in depressed patients in the late 1950s. Connections between endocrine (hormonal system) function and mental health have been explored for decades. As the understanding of the endocrine system has advanced with neurocognitive research, causes and potential treatments for mental illness have become increasingly clear.Citation55
Quality of life domains include physical, psychological, and social functioning and general satisfaction with life.Citation56 This article primarily measures the frequency of MDD and its predictive risk factors among the Arab population, as well as the issues surrounding screening, methodology, and the underlying causes and consequences of depression in the HD population.
Methods
A cross-sectional study was performed from October 1, 2010 to November 30, 2011 and included 71 patients (37 females) and 26 control subjects. Patients were included in the study if they had ESRD, were on maintenance HD for at least 3 months, and were 18 years of age or older. The control group included 26 control volunteers. The control group included HD patients’ relatives, who were employed as caregivers at the same time by their HD relatives, with no history of depressive episodes. The control group was age-matched to HD patients, who were able to communicate easily and who agreed to answer questionnaires. Exclusion criteria included inability to participate in the psychiatric interview, acute renal failure, and delirium, patients with general mood disorders or complaints of cardiovascular disease, severe electrolyte disturbances, anemia, sepsis, and hormonal disturbances. Additionally, patients who were diagnosed with psychiatric disorders other than MDD based on psychiatric interviewing were excluded. All patients fulfilling the inclusion criteria who regularly visited our department for HD were included. A single psychiatric physician interviewed all study subjects. Subjects were screened for mood, anxiety, and somatoform disorders based on the DSM-IV diagnostic criteria. All participants underwent a series of interviews; demographic data and comprehensive clinical records were collected at study entry.
The study included two essential target goals. The first objective was to identify and measure the prevalence of major depressive disorder and its risk factors at the Nephrology Unit, EMMS hospital of Nazareth, Israel, after approval by the ethical committee of the hospital and obtaining signed consent from all participants. The second goal was to explore underlying etiologies and relationships between depression and hormonal disorders such as the glucocorticoid hormone (cortisol).
The Hamilton Depression Scale was administrated, and a score of 18 or greater on Hamilton Depression Scale accompanied by the presence of significant neurovegetative changes were evaluated to confirm the diagnosis. We also used the BDI, a self-administration evaluation including 21 questions, which is known to be reliable and valid, as the main evaluation method in our study. A BDI score of 11 or greater indicates the presence of at least a moderate level of depression symptoms. Patients with a Hamilton score of >18 and/or BDI score of >11 underwent a structured clinical interview by a psychiatrist based on DSM-IV criteria. Diagnosis was made using the DSM-IV to correlate psychological variables with clinical, hematological, and biochemical parameters. Independent variables included depression, socioeconomic situation, including income, education level, cortisol levels and C-reactive protein, albumin, and hospitalization rates. Dependent variables included HD patients, age, sex, and those who were unmarried and young females ().
Table 1 Demographic and other different variables
MDD is defined by the DSM-IV, as the loss of pleasure or interest for at least 2 weeks, accompanied by five or more psychological, somatic, and behavioral symptoms. Several symptoms including anhedonia and feelings of sadness, emotional inhibitions, lack of energy, sleep disturbances, loss of concentration, intense guilt, and thoughts of suicide or death are associated with major depression. Thoughts of suicide and death are symptoms that are of obvious concern.
Blood samples were drawn for routine hematological and biochemical parameters and viral markers (antihepatitis C and HbsAg). Norepinephrine was assayed using high-pressure liquid chromatography with electrochemical detection. Intra- and interassay coefficients of variability were 11.6% and 7.7%. A blood exam for plasma cortisol levels was conducted early in the morning and in the afternoon. Cortisol was tested by using a radioimmunoassay. Intra- and interassay coefficients of variation were 6% and 10%.
Statistical analysis carried out using one-way analyses of variance followed by Tukey’s post-hoc multiple comparison tests were used. Finally, in order to characterize the relationship between depression scoring measures and the startle response, Pearson correlation was calculated.
Results
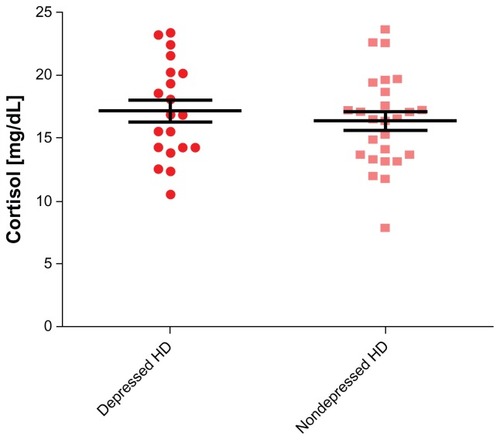
The mean ages of the chronically depressed HD patients and control subjects were 61.92 ± 14.13 and 59.3 ± 7.3 years (P > 0.05), respectively (). The prevalence of severe depression among our HD patients, calculated using BDI, was 43.7%. The frequency of depression was two-fold higher among young female patients (n = 8, age ≤ 27 years) undergoing HD for at least 12 months compared to adulthood female HD patients (n = 29, age > 27 years, P < 0.0001). Depression was twofold higher among unmarried patients (n = 43) versus married patients (n = 28, P = 0.003), and threefold higher among illiterate patients (n = 33) versus literate patients (n = 38, P = 0.001). Depression was also higher among females than among males (61% vs 39%, P = 0.003). The standard of living and socioeconomic status of our patients were examined by a social worker, who concluded that nearly all patients required financial support for their disability after losing employment. A covariant connection was observed between joblessness (n = 66: 93%) and depression. When socioeconomic status deteriorated, the tendency for depression increased (P < 0.001). Hospitalization rates were higher among depressed HD patients compared to controls (61% vs 24%, P < 0.004, respectively) (). Comparing cortisol values between (HD) and control subjects, the levels were statistically significant for HD patients (P < 0.0001, 95% CI: 2.416–6.825; mean cortisol ± SEM of patients; n = 71, 16.96 ± 0.5476; for control subjects, n = 26, 11.96 ± 1.116) (). Comparing cortisol values between depressed HD patients and control subjects, the values were also statistically significant (P = 0.0013, 95% CI: 1.868–7.184; mean ± SEM of depressed patients, 16.48 ± 0.72; for control subjects, 11.96 ± 1.116) (). Comparing cortisol levels among depressed HD patients and nondepressed HD patients, the results were statistically insignificant (). Additionally, the levels of norepinephrine between depressed patients and control subjects were insignificant. C-reactive protein, albumin, hemoglobin, calcium, and phosphor values were compared between depressed HD patients and nondepressed HD patients, and the results were statistically insignificant (P > 0.05) ().
Figure 1 Cortisol levels among hemodialysis (HD) patients vs control.
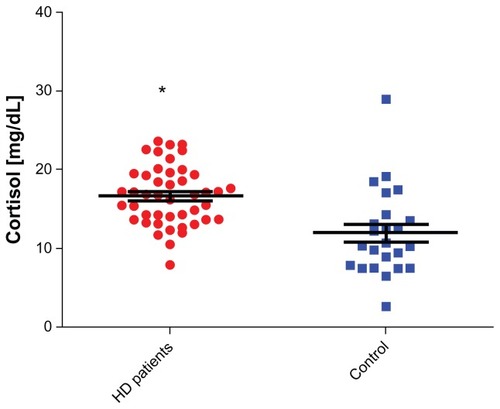
Figure 2 Cortisol levels among depressed hemodialysis (HD) patients vs controls.
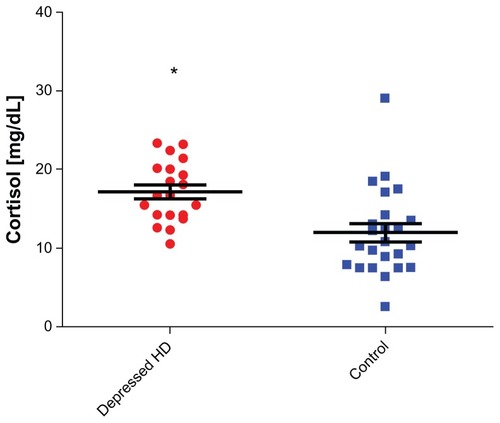
Figure 3 Cortisol levels among depressed hemodialysis (HD) vs nondepressed hemodialysis patients.
Despite strong familial ties present among Arabic traditions, this factor failed to decrease the depression among our patients.
Discussion
Depression has been identified as a complicating comorbid diagnosis in a variety of medical conditions, including ESRD.
Depression is a common psychopathological inconvenience experienced by patients undergoing dialysis which can affect quality of life, morbidity, and mortality of this population, yet its detection and management are typically not documented as part of the routine care of this population. Nevertheless, increasing awareness of psychiatric problems for both patients and physicians, which are often overlooked by patients, their families, and physicians, may increase the early diagnosis and treatment of depressive disorders and may be important for successful care and adherence outcomes. Additionally, awareness of psychiatric problems helps to facilitate psychosocial adaptation of patients, reduce treatment-related costs by increasing treatment success, and decreasing hospitalizations.
In our study, patient and control groups, which had similar age and sex distributions, were compared by evaluating social, economic, and psychological factors. The high unmarried and illiteracy rates observed in our patient group can be coupled with the detrimental effects of depression. The frequency of depression was two-fold higher among unmarried patients compared to married patients, and three-fold more frequent among illiterate patients compared to literate patients. These findings agree with those of previous studies that also reported that a lack of social and familial support increases mortality.Citation57,Citation58 Indeed, being married and having a high-quality marriage are associated with lower depression scores compared to being single or widowed.Citation59,Citation60
In agreement with several previous studies, higher depression scores are associated with low educational level.Citation61,Citation62
The standard of living and the socioeconomic status of nearly all our patients were low and sometimes intolerable, and nearly all required financial supports for their disability after losing employment. The reason for the high rates of unemployment may be due to HD treatment 3 to 4 hours three times per week, which is generally unacceptable to most employers. The patients also had more disease-related disability and more limited work opportunities due to their low-educational levels. This fact fits the covariance with depression, and has a negative impact on patient illness. According to previous studies, as socioeconomic status deteriorates, depression generally increases.Citation63
We also observed a high rate of hospitalization among our depressed HD patients compared to control subjects. This is related to the negative effect of depression in this group, and previous studies have extensively discussed this issue.Citation63–Citation65
Our results also showed a relatively high prevalence of severe depression in nearly half (43.7%) of HD patients compared to control group subjects (15%). Similar results were reported by Watnick et al.Citation33 Additionally, depression frequency was high among females (61%) compared with males (39%); this difference may due to the sensitivity of females to stressors and their greater concern about the future. A female’s obligations to adopt several social roles, such as a mother, wife, housewife, and business woman, may also contribute to this increased stress. In previous studies, both depression and anxiety were reported to be more frequent in females than in males.Citation66,Citation67
To be young, female, unemployed, on dialysis for less than 2 years, and living alone are suggested as risk factors for depression as reported by Craven et al.Citation68
Another interesting finding of our study was the high level of serum cortisol among HP patients compared to that in control subjects (P < 0.0001), and the high cortisol levels among depressed HD patients versus control subjects (P = 0.0013). It is well-known that in normal physiology, the end product of the HPA axis is the glucocorticoid cortisol, secreted from the adrenal gland upon stimulation of adrenocorticotropin (ACTH) from the pituitary gland. ACTH is in turn secreted in response to corticotropin-releasing hormone and vasopressin from the hypothalamus. Cortisol exerts negative feedback control on both corticotropin-releasing hormone and vasopressin in the hypothalamus, and ACTH in the pituitary. In normal individuals, cortisol is secreted in a circadian rhythm; it is the loss of this circadian rhythm, together with loss of the normal feedback mechanism of the HPA axis, which results in chronic exposure to excessive circulating cortisol levels.
Cortisol is widely known to be a stress hormone produced by the human body’s adrenal glands. When the body is under stress, the adrenal gland increases secretion of cortisol. In the short-term, this hormone can aid in survival, for example by mobilizing energy reserves. Long-term elevation of cortisol, however, can have detrimental effects. The timing of cortisol release can cause problems in people who are depressed. It is known that normal plasma cortisol levels fluctuate in a diurnal pattern, with maximal levels of up to (5–25 μg/mL) at 8:00 am and 4:00 pm, and lowest during the night (2.9–13 μg/mL). A depressed individual may have a consistent level of cortisol or high amounts in the middle of the night. In depressed people, however, cortisol peaks earlier in the morning and does not level off or decrease in the afternoon or evening. Although the exact mechanism that causes depression is unclear, clinical studies suggest that chronically elevated cortisol may induce clinical depression by affecting central serotonergic neurotransmission.Citation48,Citation69 In fact, it has long been observed that a significant proportion of depressed patients have elevated plasma cortisol levels,Citation69 possibly due to abnormalities in negative feedback at multiple levels in the HPA axis.Citation70 It is likely that during critical illness, under chronic stress or depression, glucocorticoid secretion and cortisol levels markedly increase.Citation71–Citation73
High circulating cortisol levels may also be related to the kidneys. Indeed, the kidney plays a significant role in degrading many peptides and hormones.Citation74,Citation75 Severe chronic renal failure is associated with a prolonged Tl/2 of serum cortisol, which can be returned to normal or near normal by dialysis. Citation76 However, compared to basal cortisol levels of normal subjects, HD patients were relatively hypercortisolemic. This finding was also confirmed by previous studies.Citation77–Citation79 Since a small percentage of cortisol metabolites can be detected by measuring plasma cortisol, our findings could, in part, be due to high plasma cortisol metabolites which can accumulate in patients with ESRD.Citation80
Other previous findings in HD patients suggested a defect in the hypothalamic reactivity for ACTH secretion, as well as a defect in adrenal cortisol secretion possibly due to a biologically inactive form of ACTH.Citation78–Citation81 Indeed, depressed patients have increased tissue and central nervous system exposure to free, physiologically active glucorticoides. The appearance of severe depressive symptoms which manifests a diurnal rhythm may be due in part by excessive central nervous system exposure to glucocorticoids.Citation82 Whatever the reasons for the increased level of cortisol among our HD patients, measuring serum cortisol concentrations in HD patients with depression may help in the detection of the disease in its early stages and contribute to a quick diagnosis to permit early therapeutic interventions. All of our depressed HD patients were treated using antidepressants. The systematic use of screening instruments for depressive symptoms may help medical personnel identify hemodialysis patients who require special care in order to improve their quality of life, reduce hospitalization, and increase survival.
In our study the BDI, was an easily administered questionnaire and is a useful screen for identifying potentially treatable clinical depression. Employment of BDI, the Hamilton Depression Scale, and the DSM-IV, have reported remarkable accuracy as screening and diagnostic tools for depression among patients with HD. Their specificity and accuracy were justified by the high prevalence of depression observed among HD patients.
Further investigation of the BDI in dialysis populations is required before conclusions can be drawn on the appropriateness of this methodology. We suggest that on-dialysis screening is viable, and that the BDI is a suitable screening tool. Because of the limited sample size of our study, we cannot exclude the possibility that the observed effects are due to confounding factors that could not be fully evaluated due to the limited power of our method (ie, differences between depressed and nondepressed subjects). Further studies examining the turnover activity of glucocorticoids such as cortisol are needed to confirm the effectiveness of glucocorticoids as models or markers for early diagnosis of depression among HP patients.
In summary, our data suggest that most patients undergoing HD are severely depressed and that screening and diagnosis of HD patients for depression is extremely important for successful therapy adherence. We have instituted a program in our dialysis units to screen patients every 6 months to identify those with BDI scores of 11 or greater, or/and with a Hamilton Depression score of 17 or more on the 21 Hamilton Depression Scale. All patients with BDI scores of 11 or greater, or/and with Hamilton Depression Scale of 17 or more are referred to a trained psychiatric interviewer. If the patient meets the DSM-IV criteria for depression, antidepressant medication is prescribed and the patient is carefully monitored. BDI is an easily administered questionnaire that is a useful screen for potentially treatable clinical depression. High level of glucocorticoid hormones such as cortisol turnover may be used as indices for early detection and diagnosis of depression among HD patients.
Disclosure
The authors declare that they have no competing interests. ZH participated in writing part of the conclusion and study design, editing the manuscript, and helped to draft the manuscript. BB carried out the study design and participated in patient recruitment as well as editing of the manuscript and funding the project. AA participated in statistical analysis, study design, and data collection. SS participated in the study design, created tables and figures, and helped with statistical analysis. ZM participated in collection of data and lab analysis. HE participated in lab analysis and patient recruitment. JA was the lab director and participated in data analysis. FJ participated partially in the data collection and helped with study design. BA conceived of the study, and participated in its design and coordination; wrote nearly all of the manuscript (Introduction and Discussion) and helped to draft the manuscript.
References
- FinkelsteinFOFinkelsteinSHPsychological adaptation and quality of life of the patient with end-stage renal diseaseBrownEParfreyPComplications of Long Term DialysisOxford University PressOxford1999168187
- KimmelPLPetersonRAWeihsKLMultiple measurements of depression predict mortality in a longitudinal study of chronic hemodialysis patientsKidney Int20005752093209810792629
- KimmelPLPsychosocial factors in adult end-stage renal disease patients treated with hemodialysis: correlates and outcomesAm J Kid Dis2000351132140
- CollinsAJKasiskeBHerzogCExcerpts from the United States Renal Data System 2006 Annual Data Report: Atlas of End-Stage Renal Disease in the United StatesAm J Kidney Dis200749Suppl 1viviiS1S296
- FoleyRNCollinsAJEnd-stage renal disease in the United States: an update from the United States Renal Data SystemJ Am Soc Nephrol200718102644264817656472
- KimmelPLPsychosocial factors in dialysis patientsKidney Int20015941599161311260433
- ReissDPatient, family, and staff responses to end-stage renal diseaseAm J Kidney Dis19901531942002305759
- ChilcotJWellstedDDa Silva-GaneMFarringtonKDepression on dialysisNephron Clin Pract20081084c256c26418401193
- KimmelPLDepression in patients with chronic renal disease: what we know and what we need to knowJ Psychosom Res200253495195612377308
- De-NourAKShaltielJCzaczkesJWEmotional reactions of patients on chronic hemodialysisPsychosom Med19683055215335725379
- O’BrienMECompliance behavior and long-term maintenance dialysisAm J Kidney Dis19901532092142106260
- De-NourAKSocial adjustment of chronic dialysis patientsAm J Psychiatry19821391971007055285
- KimmelPLWeihsKPetersonRASurvival in hemodialysis patients: the role of depressionJ Am Soc Nephrol19931412278400064
- FinkelsteinFOFinkelsteinSHDepression in chronic dialysis patients: assessment and treatmentNephrol Dial Transplant200015121911191311096130
- LevensonJLGlocheskiSPsychological factors affecting end-stage renal disease: a reviewPsychosomatics19913243823891961849
- WatnickSWangPLDemaduraTGanziniLValidation of 2 depression screening tools in dialysis patientsAm J Kidney Dis200546591992416253733
- KillingworthAvan den AkkerOThe quality of life of renal dialysis patients: trying to find the missing measurementInt J Nurs Stud19963311071208655260
- SteinMBCoxBJAfifiTOBelikSLSareenJDoes co-morbid depressive illness magnify the impact of chronic physical illness? A population-based perspectivePsychol Med200636558759616608557
- LopesAAAlbertJMYoungEWScreening for depression in hemodialysis patients: associations with diagnosis, treatment, and outcomes in the DOPPSKidney Int20046662047205315496178
- CilanHOguzhanNUnalARelationship between depression and proinflammatory cytokine levels in hemodialysis patientsRen Fail201234327527822260097
- SteeleTEBaltimoreDFinkelsteinSHJuergensenPKligerASFinkelsteinFOQuality of life in peritoneal dialysis patientsJ Nerv Ment Dis199618463683748642387
- BeckATSteerRABrownGKBeck Depression Inventory2nd edSan AntonioThe Psychological Corporation1996
- WuerthDBFinkelsteinSHSchwetzOCareyHKligerASFinkelsteinFOPatients’ descriptions of specific factors leading to modality selection of chronic peritoneal dialysis or hemodialysisPerit Dial Int200222218419011990402
- LambertMJHatchDRKingstonMDEdwardsBCZung, Beck, and Hamilton rating scales as measures of treatment outcome: a meta-analytic comparisonJ Consult Clin Psychol198654154593958302
- SnaithRPTaylorCMRating scales for depression and anxiety: a current perspectiveBr J Clin Pharmacol198519Suppl 1S1720
- PlumbMMHollandJComparative studies of psychological function in patients with advanced cancer – I. self-reported depressive symptomsPsychosom Med1977394264276897049
- De SouzaJJonesLARickardsHValidation of self-report depression rating scales in Huntington’s diseaseMov Disord2010251919619908314
- CukorDPetersonRACohenSDKimmelPLDepression in end-stage renal disease hemodialysis patientsNat Clin Pract Nephrol200621267868717124525
- CravenJLRodinGMLittlefieldCThe Beck Depression Inventory as a screening device for major depression in renal dialysis patientsInt J Psychiatry Med19881843653743235282
- CohenSDNorrisLAcquavivaKPetersonRAKimmelPLScreening, diagnosis, and treatment of depression in patients with end-stage renal diseaseClin J Am Soc Nephrol2007261332134217942763
- GençözFTülin GençözTSoykanAPsychometric properties of the Hamilton Depression Rating Scale and other physician-rated psychiatric scales for the assessment of depression in ESRD patients undergoing hemodialysis in TurkeyPsychol Health Med200712445045917620209
- ZimmermanMChelminskiIPosternakMA review of studies of the Hamilton depression rating scale in healthy controls: implications for the definition of remission in treatment studies of depressionJ Nerv Ment Dis2004192959560115348975
- WatnickSKirwinPMahnensmithRConcatoJThe prevalence and treatment of depression among patients starting dialysisAm J Kidney Dis200341110511012500227
- WeisbordSDFriedLFUnruhMLAssociations of race with depression and symptoms in patients on maintenance haemodialysisNephrol Dial Transplant200722120320816998218
- KimmelPLPetersonRADepression in end-stage renal disease patients treated with hemodialysis: tools, correlates, outcomes, and needsSemin Dial2005182919715771651
- WilsonBSpittalJHeidenheimPScreening for depression in chronic hemodialysis patients: comparison of the Beck Depression Inventory, primary nurse, and nephrology teamHemodial Int2006101354116441825
- SmithMDHongBARobsonAMDiagnosis of depression in patients with end-stage renal disease. Comparative analysisAm J Med19857921601663895906
- DrayerRAPirainoBReynoldsCF3rdCharacteristics of depression in hemodialysis patients: symptoms, quality of life, and mortality riskGen Hosp Psychiatry200628430631216814629
- KimJALeeYKHuhWSAnalysis of depression in continuous ambulatory peritoneal dialysis patientsJ Korean Med Sci200217679079412483003
- Herrmann-LingenCKlemmeHMeyerTDepressed mood, physician- rated prognosis, and comorbidity as independent predictors of 1-year mortality in consecutive medical inpatientsJ Psychosom Res200150629530111438110
- CohenLMDobschaSKHailsKCPekowPSChochinovHMDepression and suicidal ideation in patients who discontinue the life-support treatment of dialysisPsychosom Med200264688989612461194
- IsraelMDepression in dialysis patients: a review of psychological factorsCan J Psychiatry19863154454513524786
- SmogorzewskiMNiZMassrySGFunction and metabolism of brain synaptosomes in chronic renal failureArtif Organs19951987958008572998
- JhambMWeisbordSDSteelJLUnruhMFatigue in patients receiving maintenance dialysis: a review of definitions, measures, and contributing factorsAm J Kidney Dis200852235336518572290
- LeeBOLinCCChaboyerWChiangCLHungCCThe fatigue experience of haemodialysis patients in TaiwanJ Clin Nurs200716240741317239077
- VreeburgSAHoogendijkWJGvan PeltJMajor depressive disorder and hypothalamic-pituitary-adrenal axis activityArch Gen Psychiatry200966661762619487626
- HeinzAJonesDWBissetteGRelationship between cortisol and serotonin metabolites and transporters in alcoholism (correction of alcolholism)Pharmacopsychiatry200235412713412163982
- TafetGEIdoyaga-vargasVPDenisePCorrelation between cortisol level and serotonin uptake in patients with chronic stress and depressionCognit Affect Behav Neurosci20011438839312467090
- DinanTGGlucocorticoids and the genesis of depressive illness. A psychobiological modelBr J Psychiatry199416433653717832833
- DuJWangYHunterRDynamic regulation of mitochondrial functions by glucocorticoidsProc Natl Acad Sci U S A200910693543354819202080
- BauerMEVedharaKPerksPWilcockGKLightmanSLShanksNChronic stress in caregivers of dementia patients is associated with reduced lymphocyte sensitivity to glucocorticoidsJ Neuroimmunol20001031849210674993
- McAllister-WilliamsRHAndersonRJYoungAHCorticosterone selectively attenuates 8-OH-DPAT-mediated hypothermia in miceInt J Neuropsychopharmacol2001411811343623
- ArdayfioPKimKSAnxiogenic-like effect of chronic corticosterone in the light-dark emergence task in miceBehav Neurosci2006120224925616719689
- CowenPJCortisol, serotonin and depression: all stressed out?Br J Psychiatry20021809910011823315
- MackinPYoungAHThe role of cortisol and depression: exploring new opportunities for treatmentsPsychiatr Times20042169295
- TsaySLHealsteadMSelf-care, self-efficacy, depression, and quality of life among patients receiving hemodialysis in TaiwanInt J Nurs Stud200239324525111864647
- ChristensenAJWiebeJSSmithTWTurnerCWPredictors of survival among hemodialysis patients: effect of perceived family supportHealth Psychol19941365215257889907
- KimmelPLPetersonRAWeihsKLPsychosocial factors, behavioral compliance and survival in urban hemodialysis patientsKidney Int19985412859742023
- OslerMMcGueMLundRChristensenKMarital status and twins’ health and behavior: an analysis of middle-aged Danish twinsPsychosom Med200870448248718480194
- Holt-LunstadJBirminghamWJonesBQIs there something unique about marriage? The relative impact of marital status, relationship quality, and network social support on ambulatory blood pressure and mental healthAnn Behav Med200835223924418347896
- HamadRFernaldLCKarlanDSZinmanJSocial and economic correlates of depressive symptoms and perceived stress in South African adultsJ Epidemiol Community Health200862653854418477753
- Di CorradoDDi NuovoSIannettiEQuality of life in hemodialyis patients: the effect of educational statusClin Ter2000151423523911107671
- MurataCKondoKHiraiHIchidaYOjimaTAssociation between depression and socio-economic status among community-dwelling elderly in Japan: the Aichi Gerontological Evaluation Study (AGES)Health Place200814340641417913562
- LopesAABraggJYoungEDepression as a predictor of mortality and hospitalization among hemodialysis patients in the United States and EuropeKidney Int200262119920712081579
- ChristensenAJEhlersSLPsychological factors in end-stage renal disease: an emerging context for behavioral medicine researchJ Consult Clin Psychol200270371272412090378
- TorosFBilginNGBugdayciRSasmazTKurtOCamdevirenHPrevalence of depression as measured by the CBDI in a predominantly adolescent school population in TurkeyEur Psychiatry200419526427115276658
- SchmausBJLaubmeierKKBoquirenVMHerzerMZakowskiSGGender and stress: differential psychophysiological reactivity to stress reexposure in the laboratoryInt J Psychophysiol200869210110618453025
- CravenJLRodinGMJohnsonLKennedySHThe diagnosis of major depression in renal dialysis patientsPsychosom Med19874954824923671637
- GibbonsJLCortisol secretion rate in depressive illnessArch Gen Psychiatry19641057257514159257
- HolsboerFLauerCJSchreiberWKriegJCAltered hypothalamic– pituitary–adrenocortical regulation in healthy subjects at high familial risk for affective disordersNeuroendocrinology19956243403478544947
- EpelESPsychological and metabolic stress: a recipe for accelerated cellular aging?Hormones (Athens)20098172219269917
- SonikianMMetaxakiPPapavasileiouDEffects of interleukin-6 on depression risk in dialysis patientsAm J Nephrol201031430330820160434
- HamrahianAHOseniTSArafahBMMeasurements of serum free cortisol in critically ill patientsN Engl J Med2004350161629163815084695
- FeldmanHASingerIEndocrinology and metabolism in uremia and dialysis: a clinical reviewMedicine1974545345376808679
- EmmanouelDSLindheimerMDKatzAIPathogenesis of endocrine abnormalities in uremiaEndocr Rev19801128446785085
- BaconGEKennyFMMardaughHVRichardsCProlonged serum half-life of cortisol in renal failureJohns Hopkins Med J197313221271314684170
- SiamopoulosKCEleftheriadisEPappasMSferopoulosGTsolasOOvine corticotropin-releasing hormone stimulation test in patients with chronic renal failure: pharmacokinetic properties, and plasma adrenocorticotropic hormone and serum cortisol responsesHorm Res198830117212851525
- McDonaldWJGolperTAMassRDAdrenocorticotropin-cortisol axis abnormalities in hemodialysis patientsJ Clin Endocr Metab19794819295217891
- WallaceEZRosmanPToshavNSacerdoteABalthazarAPituitary-adrenocortical function in chronic renal failure: studies of episodic secretion of cortisol and dexamethasone suppressabilityJ Clin Endocr Metab198050146517350187
- EnglertEJrBrownHWillardsonDGWallachSSimonsELMetabolism of free and conjugated 17-hydroxycorticosteroids in subjects with uremiaJ Clin Endocr Metab1958181364813491682
- RamirezGGomez-SanchezCMeikleWAJubizWEvaluation of the hypothalamic hypophyseal adrenal axis in patients receiving long term hemodialysisArch Intern Med19821428144814526285845
- BernardJCGeorgeCCMendelsJCerebrospinal fluid and plasma free cortisol concentrations in depressionPsychol Med1976622352441005564