
Abstract
Background
Migraine is a recurrent headache disease that has been identified as a risk factor for subsequent dementia. The present study collected data from Taiwan’s National Health Insurance Research Database (NHIRD) to investigate the incidence of dementia in patients with migraine who did or did not concurrently receive acupuncture treatment.
Methods
A 1:1 propensity score method was used to match an equal number of patients (N = 4813) in the acupuncture and nonacupuncture cohorts based on sex, age, migraine diagnosis year, index year, insurance amount, urbanization level, baseline comorbidities, and medication usage. We employed Cox proportional hazards models to evaluate the risk of dementia.
Results
Patients with migraine who received acupuncture treatment were found to have a lower risk of dementia (adjusted hazard ratio [aHR] = 0.51, 95% CI = 0.40–0.65) than those who did not undergo acupuncture treatment. The cumulative incidence of dementia was significantly lower in the acupuncture cohort than in the nonacupuncture cohort (Log rank test, p < 0.001). This propensity score–matched cohort study demonstrated an association between acupuncture treatment and dementia development in patients with migraine in Taiwan.
Conclusion
The results suggest that acupuncture treatment significantly reduced the development of dementia in patients with migraine.
Introduction
Migraine is one of the most common neurological disorders; the newest edition (third) of the International Classification of Headache Disorders (ICHD-3) defines migraine as a recurrent headache disease, manifesting as a unilateral throbbing headache with moderate to severe pain intensity.Citation1 Common symptoms include headache and accompanying nausea, vomiting, photophobia, and occasional sensitivity to taste and sound.Citation1 According to a survey, the prevalence rate of migraine in the Taipei area for people over 15 years old is approximately 9.1%. Among this group, the prevalence rate is 4.5% for men and 14.4% for women.Citation2 In a study from the United States, the prevalence of migraine was 8.6% in males, 17.5% in females, and 13.2% in the overall population; migraine exhibited a bimodal distribution in both sexes (peaking in those in late adolescence or their 20s and in those approximately 50 years of age).Citation3
Several studies have indicated that migraine is associated with increased risks of stroke,Citation4 depression,Citation5 and dementia.Citation6 In addition, a cross-sectional prevalence study found that patients with migraine with or without aura are at increased risk for subclinical brain lesions.Citation7 Previous studies have revealed that silent brain lesions in the general population double the risk of dementia.Citation8
According to the 2019 Alzheimer’s Disease International (ADI) Global Dementia Report, more than 50 million people worldwide are estimated to have dementia, and this number is expected to grow to 152 million by 2050.Citation9 Dementia is a disease in which brain function is gradually lost. It not only leads to loss of memory but also adversely affects other cognitive functions, including language ability, spatial awareness, computing power, judgment, abstract thinking, and attention span. Acupuncture, traumatology manipulative therapies, and Chinese herbal products (CHPs) are all categorized as forms of traditional Chinese medicine (TCM), which is a popular form of alternative medicine in many countries.Citation10 Several studies have reported that acupuncture or CHPs are often used to treat migraine.Citation11,Citation12 A population-based cohort study indicated a decreased risk of dementia in patients with migraine who used CHPs.Citation13 However, this study investigated the effects of CHPs only, and the potential benefits of acupuncture as preventive treatment for dementia in patients with migraine are yet unknown.
The National Health Insurance Research Database (NHIRD) of Taiwan is used for health policy and management, disease treatment research, drug efficacy and disease risk factor analysis, real-time tracking of epidemics, and medical quality improvement. The National Health Insurance (NHI) program was launched in 1995, and by the end of 2010, more than 99% of people in Taiwan were enrolled in the program.Citation14 A previous study reported that middle-aged people in Taiwan are most likely to receive acupuncture treatment. Other research has revealed that patients most often receive acupuncture to treat physical injury and diseases of the musculoskeletal system and of connective tissue.Citation15 Another study found migraine to be associated with vascular risk factors and reduced cerebral blood flow (CBF) to be a potential cause of dementia.Citation16 One clinical trial indicated that CBF was enhanced through acupuncture.Citation17 In addition, decreased hippocampal volume of newly diagnosed migrainers was discovered,Citation18 and the hippocampal structural and functional changes play a critical role in the pathophysiology of migraine.Citation19 A study found that acupuncture treatment can increase the hippocampal connectivity among patients with Alzheimer Disease (AD).Citation20 In the present study, we hypothesized that acupuncture could reduce the risk of developing dementia among patients with migraine. Therefore, the association between acupuncture treatment and the risk of dementia was evaluated in 9626 patients with migraine between 2000 and 2012 who were identified in the NHIRD.
Materials and Methods
Data Source
The NHIRD, a large-scale health database in Taiwan, has enrolled over 99% of the population of Taiwan. The database contains data on outpatient visits, hospitalizations, medical treatments, and other medical services at each hospital visit.
We conducted the analyses by Longitudinal Health Insurance Database 2000 (LHID 2000), which is a subset of the NHIRD containing 1 million individuals randomly selected from the NHIRD; that the distribution of age and sex is similar to the original database after sampling has been confirmed. For personal information protection, patient identification numbers are encrypted before being released for use.
Each diagnosis was coded based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). The study was approved by the Research Ethics Committee of China Medical University and Hospital in Taiwan [CMUH104-REC2-115 (CR-6)]. All methods were performed in accordance with the relevant guidelines and regulations. The NHIRD encrypts patient personal information to protect privacy and provides researchers with anonymous identification numbers associated with relevant claims information, including sex, date of birth, medical services received, and prescriptions. Therefore, patient consent is not required to access the NHIRD.
Study Population
This study included patients with migraine who had at least two outpatient visits or one hospitalization for migraine (ICD-9-CM: 346). Included patients were then classified into the acupuncture cohort or nonacupuncture-treated cohort.
The index date was set as the date when patients first received acupuncture treatment, and patients were followed until they were newly diagnosed as having dementia (ICD-9-CM: 290, 294.1, 331.0; at least two outpatient visits or one hospitalization after at least one year), withdrew from the NHIRD, or December 31, 2013. The patients with dementia were grouped into those with Alzheimer’s disease (AD) (ICD-9-CM: 331.0), vascular dementia (VaD) (ICD-9-CM: 290.4), or other degenerative dementia (ICD-9-CM: 290.x except 290.4).
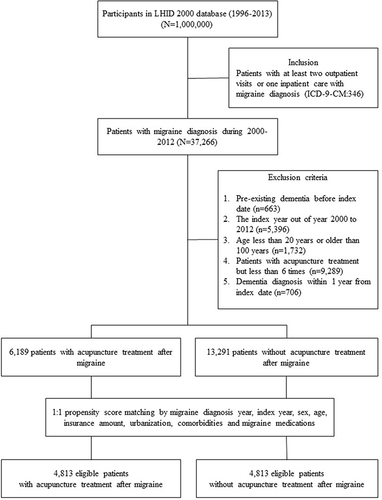
Migraine patients who were diagnosed with dementia before the index date, who were younger than 20 years old, or who were missing demographic information were excluded from this study. Each acupuncture-treated patient was matched with a nonacupuncture-treated patient through propensity score matching. We defined acupuncture cohort based on more than 6 times acupuncture treatments received after diagnosing as migraine during the study period. The matching variables included age, sex, insurance amount, urbanization level, baseline comorbidities, and medication usage ().
Figure 1 Study population flowchart. 37,266 patients with migraine, newly diagnosed between 2000 and 2012, were identified. A 1:1 propensity score was used to match cohorts based on sex, age, baseline comorbidities, and medication usage. The groups of acupuncture users and nonacupuncture users each contained 4813 patients.
Baseline comorbidity was defined as a comorbidity present before the index date and coded in the patient’s medical records for at least two outpatient visits or one hospitalization. Included diseases were diabetes mellitus (ICD-9-CM: 250), hypertension (ICD-9-CM: 401–405), hyperlipidemia (ICD-9-CM: 272), coronary artery disease (ICD-9-CM: 410–414), head injury (ICD-9-CM: 850–854, 959.01), chronic kidney disease (ICD-9-CM: 403–404, 585–589), stroke (ICD-9-CM: 430–438), and depression (ICD-9-CM: 296.2, 296.3, 296.82, 300.4, 309.0, 309.1, 309.28, 311). Medication usage was defined as the first prescribed medication after migraine and included sumatriptan, rizatriptan, ergotamine, naproxen, diclofenac, caffeine, acetaminophen, etoricoxib, celecoxib, and ibuprofen. Patient medication usage was classified into groups taking 0, 1, 2, or 3+ medications.
Statistical Analysis
The differences between categorical and continuous variables of the two cohorts were tested using the chi-square test and t-test, respectively.
The association between acupuncture treatment and the risk of dementia among patients with migraine was evaluated using the Cox proportional hazards model, and hazard ratios (HR), adjusted hazard ratios (aHR), and 95% CIs were employed to estimate the risk of dementia. The incidence rate of dementia was expressed as the number of diagnoses per 1000 person-year. The Kaplan–Meier method was applied to create cumulative incidence curves for the acupuncture-treated and nonacupuncture-treated groups. The difference between two incidence curves was determined using a Log rank test. All statistical analyses were performed using SAS, version 9.4 (SAS Institute, Cary, NC, USA). The cumulative incidence curve was plotted using R software. A two-sided p-value < 0.05 indicated statistical significance.
Results
Of the 4813 patients with migraine who received acupuncture treatment, 75% were female and the overall mean age was 46 years (). The distributions of sex, age, insurance amount, and comorbidities exhibited nonsignificant differences between the groups (p > 0.05). Patients who received acupuncture treatment lived in more urbanized areas (p = 0.0659) and exhibited a higher rate of medication usage for migraine (p = 0.2646).
Table 1 Characteristics of Newly Diagnosed Patients with Migraine Who Did or Did Not Receive Acupuncture
displays the diagnosis distribution for patients who received acupuncture treatment. Most received treatment because of injury or poisoning (83.5%) or receiving a diagnosis of a disease of the musculoskeletal system or connective tissue (83.5%).
Table 2 Distribution of Acupuncture Cohort by Disease Category or Diagnosis in Patients with Migraine
Several stratified analyses were conducted to verify the associations (). Patients who received acupuncture treatment exhibited a decreased risk of overall dementia and acupuncture is more effective for other degenerative dementia; this was true for women (aHR = 0.47, 95% CI = 0.35–0.63); men (aHR = 0.56, 95% CI = 0.37–0.85); patients aged 40 to 65 years (aHR = 0.46, 95% CI = 0.30–0.71); patients aged over 65 years (aHR = 0.45, 95% CI = 0.33–0.59); patients with diabetes (aHR = 0.49, 95% CI = 0.33–0.72), hypertension (aHR = 0.55, 95% CI = 0.42–0.72), hyperlipidemia (aHR = 0.54, 95% CI = 0.40–0.75), coronary artery disease (aHR = 0.55, 95% CI = 0.40–0.75), depression (aHR = 0.43, 95% CI = 0.26–0.71), stroke (aHR = 0.63, 95% CI = 0.44–0.90), or chronic kidney disease (aHR = 0.65, 95% CI = 0.42–0.99); and patients without migraine-related medication usage (aHR = 0.59, 95% CI = 0.39–0.87).
Table 3 Incidence Rates, Hazard Ratios, and Confidence Intervals of Dementia for Patients with Migraine Who Did and Did Not Receive Acupuncture in Different Stratifications
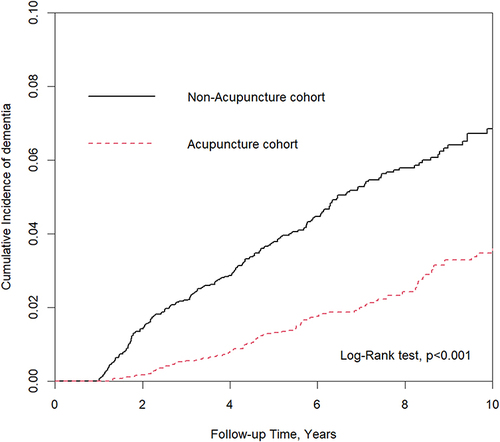
Among patients with migraine, the risk of dementia exhibited a dose-dependent decrease with increasing use of acupuncture treatment (). illustrates the significantly lower incidence of dementia in patients with migraine who underwent acupuncture treatment compared with their nonacupuncture counterparts (p < 0.001).
Table 4 Risk of Dementia and Number of Acupuncture in Migraine Patients
Figure 2 Cumulative incidence of dementia in the acupuncture and nonacupuncture cohorts. Cumulative incidence of dementia in the acupuncture cohort was significantly lower than in the nonacupuncture cohort (Log rank test, p < 0.001).
Discussion
The results of the present study indicated that the incidence of dementia was 49% lower among patients with migraine who received acupuncture treatment than among those who did not receive acupuncture treatment. This suggests that acupuncture treatment may decrease the risk of dementia in patients with migraine. After multiple adjustments for sex, age, insurance amount, urbanization level, baseline comorbidities, and medication usage, acupuncture treatment was found to play a key role in reducing the risk of dementia.
Previous studies have reported that acupuncture can exert preventive effects in populations with several diseases associated with dementia, including traumatic brain injury (TBI),Citation21 stroke,Citation22 and hypertension.Citation23 From this, we inferred that acupuncture may also prevent dementia; for this reason, we conducted this study. The present study indicated that the risk of dementia increases with advancing age. Patients with migraine who were aged 40–65 years or aged over 65 years had a higher risk of dementia than younger individuals. The risk of developing dementia after age 60 was higher among individuals with migraine in midlife than among individuals without.Citation24 Therefore, aging can be identified as a key factor that increases the incidence of dementia.Citation25
Of all the baseline comorbidities associated with migraine, including hypertension, depression, coronary artery disease, and stroke, were found to significantly increase the risk of dementia the most. In previous study, patients at midlife ages with high blood pressure were found to have a higher risk of cognitive decline, including Alzheimer’s disease and dementia.Citation26 Early life depressive symptoms have been revealed to be related to a 2-fold or greater increase in the risk of dementia.Citation27 Heart disease and cardiovascular risk factors in midlife are confirmed to the development of dementia in later life.Citation28 In addition, studies on stroke have revealed that vascular risk factors may also be independent risk factors for developing dementia.Citation29 In this study, acupuncture was found to potentially reduce the incidence of dementia in migraine patients with these comorbidities.
In the current study, patients with migraine who received acupuncture treatment were divided into two groups: those affected by musculoskeletal system or connective tissue disorders (83.5%) and those affected by injury or poisoning (83.5%). Injury and disorders of the musculoskeletal system or connective tissue were the predominant reasons for patients to seek acupuncture treatment.Citation15 A previous study indicated that patients with migraine exhibited significantly more musculoskeletal dysfunction than migraine-free control participants, especially muscle tension in the neck.Citation30 Most patients had cervical musculoskeletal impairments that accompanied their migraine episodes.Citation31,Citation32 In addition, a case report suggested chronic carbon monoxide (CO) intoxication may mimic migraine attacks.Citation33 Therefore, acupuncture is a safe form of intervention and is a feasible option for patients with chronic neck pain or carbon monoxide intoxication.Citation34,Citation35
Acupuncture functions as a neuroprotector because it promotes the recovery of the neuronal deficit resulting from TBI by activating the brain-derived neurotrophic factor (BDNF)/tropomyosin receptor kinase B (TrkB) signaling pathway at specific acupoints (Baihui, Renzhong, Hegu, and Zusanli).Citation36 A population-based database study indicated that TBI is a risk factor for migraine.Citation37 Combining acupuncture with a TBI treatment regimen was reported to reduce the risk of dementia by 35%.Citation21 Therefore, acupuncture can not only reduce TBI symptoms but also prevent subsequent dementia.
An increased risk of dementia caused by migraine can be attributed to several mechanisms such as cerebral hypoperfusion, white matter hyperintensities (WMHs), stress, and depression.Citation38–41 A case report demonstrated that headache was associated with bilateral hypoperfusion starting from the occipital lobes and spreading anteriorly to the temporal and parietal lobes, providing clear evidence of the spreading depression associated with spontaneous migraine.Citation42 Olesen et al,Citation43 after observing changes in CBF, proposed that the mechanism of migraine-induced cerebral ischemia is spreading cortical depression. The fall in CBF can also rapidly increase the deposition of amyloid β (Aβ) and drive cognitive decline that occurs early in the development of AD patients.Citation44 However, this proposition related only to migraines with aura. Another study found that the vascular factors of migraine may be related to the risk of dementia because changes in the brain indicated that cerebral small vessel disease increases the risk of most dementia types and cerebrovascular dysfunction.Citation24 Yet another study determined that acupuncture at the Baihui (GV20) and Yintang (GV29) points increased the CBF of the prefrontal lobe and hippocampus in mouse models of Alzheimer’s disease.Citation45 Moreover, a pilot study demonstrated a significant increase in CBF after true acupuncture in patients with stroke.Citation17 Together, the results of these studies indicate that acupuncture may reduce the risk of dementia in patients with migraine, possibly by increasing CBF.
WMHs in the brain are frequently discovered on MRI scans in older people and are associated with migraine.Citation40,Citation46 High-resolution evidence has indicated that WHMs give rise to cognitive impairment and play a crucial role in the development of dementia.Citation8,Citation40 Acupuncture at the Baihui (GV20) and Zusanli (ST36) points has been found to prevent cognitive function decline in rat models of vascular dementia by ameliorating white matter perfusion and maintaining its integrity.Citation47 In addition, acupuncture at the Yanglingquan (GB34) point was found to potentially enhance the communication between cortices with damaged white matter tracts in patients with ischemic stroke.Citation48 Therefore, we infer that acupuncture modulates these alterations of white matter, thereby preventing the development of dementia.
Stress, which affects the hypothalamus–pituitary–adrenal (HPA) system, may also contribute to dementia.Citation39,Citation49 Chronic stress has been found to enhance an individual’s susceptibility to inflammatory activities in the brain, which affects dementia risk by increasing inflammatory cytokines such as interleukin (IL)-1β, IL-6, tumor necrosis factor–α (TNF-α), or interferon-γ (INF-γ).Citation39 Oxidative stress, which induces excessive production of free radical species, could lead to oxidative biomolecules and expedite aging.Citation50 Electroacupuncture (EA) was found to decrease the serum levels of IL-1β, IL-6, and TNF-α in a rat model of migraine.Citation51 In addition, acupuncture was found to attenuate cognitive impairment and neuronal death by downregulating hippocampal thioredoxin-interaction proteins (TXNIPs) to inhibit oxidative stress and inflammation in a rat model of vascular dementia.Citation52 These studies illustrate the potential of acupuncture to protect against dementia. However, further investigation is required to determine whether these mechanisms are applicable to humans.
A national cohort study indicated that severe depression also increased the risk of dementia, with some patients being diagnosed with dementia two decades after their depressive episode.Citation38 Several mechanisms may link depression and dementia, including 1) vascular disease, 2) increased deposition of β-amyloid, 3) inflammatory changes, and 4) small hippocampal volumes.Citation27,Citation53 Acupuncture has been identified as having potential to enhance CBF in both animals and humans.Citation17,Citation45 Moreover, manual acupuncture or EA at specific acupoints has been found to improve cognitive impairment and suppress the generation of amyloid beta (Aβ) in several rat models of AD.Citation54 Acupuncture also significantly decreased the serum levels of IL-1β, IL-6, and TNF-α in a chronic stress model of depression in rats.Citation55 In addition, a fMRI study revealed that acupuncture treatment strengthen the hippocampal connectivity in AD patients.Citation20 A previous rat study found that acupuncture improved cognition and hippocampal synaptic plasticity through activation of D1/D5 receptors.Citation56 Acupuncture, through multiple depression-associated pathways, could therefore reduce the risk of dementia in patients with migraine by increasing CBF, decreasing Aβ generation, decreasing the contents of proinflammatory cytokines, and increasing neuron density of the hippocampus in the brain.
The present study leaves open one key question: the mean number of acupuncture visits was 19.9 during the study period, which may not be enough to prevent the development of dementia (). However, compared with standard pharmacological agents, acupuncture is a safe and beneficial treatment for chronic migraine.Citation57 Acupuncture not only decreases migraine recurrence for an extended period but also reduces the need for rescue medication.Citation58 Therefore, acupuncture may be used to improve the quality of life of and increase physical activity in patients with migraine. Moderate-intensity physical exercise, such as aerobic activity, is often prescribed as a means of decreasing cognitive impairment and reducing the risk of dementia by attenuating the progression of neurodegenerative processes and age-related loss of synapses and neuropil.Citation59 Notably, no more than 15 visits for acupuncture treatment are covered through Taiwan’s NHI program per month. Patients may have received additional, self-paid acupuncture treatments. However, these treatments are not included in the NHIRD and were, therefore, not included in this study.
Limitations
The present study had other limitations that should be addressed. First, the data file from LHID 2000 we used was provided by Taiwan National Health Research Institutes (NHRI), which had been authorized by the Ministry of Health and Welfare to manage the claims data of the national health insurance. The latest update database by NHRI is not available now. Second, the NHIRD does not indicate the severity and duration of migraine. Accordingly, we performed 1:1 propensity score matching, which was useful in minimizing the difference between the two cohorts. Third, information regarding several aspects of treatment is not recorded in the NHIRD, including the acupoints used and the frequency and duration of treatment. Therefore, we were unable to clearly identify which acupoints may treat both migraine and dementia. Fourth, the NHIRD does not contain laboratory data or brain images; therefore, no empirical evidence could be evaluated to understand the mechanism through which acupuncture reduces the incidence of dementia in patients with migraine. Fifth, because some cases of dementia are late onset, the duration of the current study’s follow-up period was insufficient to capture these.
Conclusions
Patients with migraine may receive complementary therapies in Taiwan, and most of them would like to choose acupuncture treatment. The results of the present study indicate that the incidence of dementia was lower among patients with migraine who received acupuncture treatment than among patients with migraine who did not, suggesting that acupuncture is associated with a reduced risk of dementia. Our study emphasizes the need for additional clinical trials that include laboratory data and brain imaging to identify potential preventive mechanisms.
Data Sharing Statement
Data are available from the National Health Insurance Research Database (NHIRD), published by the Taiwan National Health Insurance (NHI) Bureau. The use of the NHIRD is limited to research purposes only. Due to the legal restrictions imposed by the government of Taiwan in relation to the Personal Information Protection Act, the data used for this study cannot be made publicly available. Request for data can be sent as a formal proposal to the NHIRD (http://nhird.nhri.org.tw).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This study was conducted using data from the NHIRD, which was provided by the National Health Insurance Administration and the Ministry of Health and Welfare, and supervised by the National Health Research Institutes. We would like to thank the management of the office for health data of China Medical University Hospital for collecting and analyzing the data used in this study.
Additional information
Funding
References
- Olesen J, Bes A, Kunkel R, et al. The international classification of headache disorders, 3rd edition (beta version). Cephalalgia. 2013;33(9):629–808.
- Wang SJ, Fuh JL, Young YH, Lu SR, Shia BC. Prevalence of migraine in Taipei, Taiwan: a population-based survey. Cephalalgia. 2000;20(6):566–572. doi:10.1046/j.1468-2982.2000.00085.x
- Victor TW, Hu X, Campbell JC, Buse DC, Lipton RB. Migraine prevalence by age and sex in the United States: a life-span study. Cephalalgia. 2010;30(9):1065–1072. doi:10.1177/0333102409355601
- Peng KP, Chen YT, Fuh JL, Tang CH, Wang SJ. Migraine and incidence of ischemic stroke: a nationwide population-based study. Cephalalgia. 2017;37(4):327–335. doi:10.1177/0333102416642602
- Amoozegar F. Depression comorbidity in migraine. Int Rev Psychiatry. 2017;29(5):504–515. doi:10.1080/09540261.2017.1326882
- Chuang CS, Lin CL, Lin MC, Sung FC, Kao CH. Migraine and risk of dementia: a nationwide retrospective cohort study. Neuroepidemiology. 2013;41(3–4):139–145. doi:10.1159/000353559
- Kruit MC, van Buchem MA, Hofman PA, et al. Migraine as a risk factor for subclinical brain lesions. JAMA. 2004;291(4):427–434. doi:10.1001/jama.291.4.427
- Vermeer SE, Prins ND, den Heijer T, Hofman A, Koudstaal PJ, Breteler MM. Silent brain infarcts and the risk of dementia and cognitive decline. N Engl J Med. 2003;348(13):1215–1222. doi:10.1056/NEJMoa022066
- Bhatt J, Comas Herrera A, Amico F, et al. The World Alzheimer Report 2019: attitudes to dementia; 2019.
- Wang HM, Lin SK, Yeh CH, Lai JN. Prescription pattern of Chinese herbal products for adult-onset asthma in Taiwan: a population-based study. Ann Allergy Asthma Immunol. 2014;112(5):465–470. doi:10.1016/j.anai.2014.02.012
- Chang YY, Tsai YT, Lai JN, Yeh CH, Lin SK. The traditional Chinese medicine prescription patterns for migraine patients in Taiwan: a population-based study. J Ethnopharmacol. 2014;151(3):1209–1217. doi:10.1016/j.jep.2013.12.040
- Hsieh C-L. Acupuncture as treatment for nervous system diseases. BioMedicine. 2012;2(2):51–57. doi:10.1016/j.biomed.2012.04.004
- Liu CT, Wu BY, Hung YC, et al. Decreased risk of dementia in migraine patients with traditional Chinese medicine use: a population-based cohort study. Oncotarget. 2017;8(45):79680–79692. doi:10.18632/oncotarget.19094
- Yeh YH, Chou YJ, Huang N, Pu C, Chou P. The trends of utilization in traditional Chinese medicine in Taiwan from 2000 to 2010: a population-based study. Medicine. 2016;95(27):e4115. doi:10.1097/MD.0000000000004115
- Wu MY, Lee YC, Lin CL, Huang MC, Sun MF, Yen HR. Trends in use of acupuncture among adults in Taiwan from 2002 to 2011: a nationwide population-based study. PLoS One. 2018;13(4):e0195490. doi:10.1371/journal.pone.0195490
- Morton RE, St John PD, Tyas SL. Migraine and the risk of all-cause dementia, Alzheimer’s disease, and vascular dementia: a prospective cohort study in community-dwelling older adults. Int J Geriatr Psychiatry. 2019;34(11):1667–1676. doi:10.1002/gps.5180
- Ratmansky M, Levy A, Messinger A, Birg A, Front L, Treger I. The effects of acupuncture on cerebral blood flow in post-stroke patients: a randomized controlled trial. J Altern Complement Med. 2016;22(1):33–37. doi:10.1089/acm.2015.0066
- Liu HY, Chou KH, Chen WT. Migraine and the Hippocampus. Curr Pain Headache Rep. 2018;22(2):13. doi:10.1007/s11916-018-0668-6
- Qu H, Yang S, Yao Z, Sun X, Chen H. Association of headache disorders and the risk of dementia: meta-analysis of cohort studies. Front Aging Neurosci. 2022;14:804341. doi:10.3389/fnagi.2022.804341
- Wang Z, Liang P, Zhao Z, et al. Acupuncture modulates resting state hippocampal functional connectivity in Alzheimer disease. PLoS One. 2014;9(3):e91160. doi:10.1371/journal.pone.0091160
- Juan YH, Livneh H, Huang HJ, Lu MC, Yeh CC, Tsai TY. Decreased risk of dementia among patients with traumatic brain injury receiving acupuncture treatment: a population-based retrospective cohort study. J Head Trauma Rehabil. 2019;34(5):E17–e23. doi:10.1097/HTR.0000000000000464
- Chu SA, Chen TY, Chen PY, et al. Acupuncture may decrease the incidence of post-stroke dementia: a Taiwan nationwide retrospective cohort study. Front Neurol. 2021;12:657048. doi:10.3389/fneur.2021.657048
- Sun J, Ashley J, Kellawan JM. Can acupuncture treatment of hypertension improve brain health? A mini review. Front Aging Neurosci. 2019;11:240. doi:10.3389/fnagi.2019.00240
- Islamoska S, Hansen ÅM, Wang HX, et al. Mid- to late-life migraine diagnoses and risk of dementia: a national register-based follow-up study. J Headache Pain. 2020;21(1):98. doi:10.1186/s10194-020-01166-7
- Ryan L, Hay M, Huentelman MJ, et al. Precision aging: applying precision medicine to the field of cognitive aging. Front Aging Neurosci. 2019;11:128. doi:10.3389/fnagi.2019.00128
- Sierra C. Hypertension and the risk of dementia. Front Cardiovasc Med. 2020;7:5. doi:10.3389/fcvm.2020.00005
- Byers AL, Yaffe K. Depression and risk of developing dementia. Nat Rev Neurol. 2011;7(6):323–331. doi:10.1038/nrneurol.2011.60
- Justin BN, Turek M, Hakim AM. Heart disease as a risk factor for dementia. Clin Epidemiol. 2013;5:135–145. doi:10.2147/CLEP.S30621
- Sahathevan R, Brodtmann A, Donnan GA. Dementia, stroke, and vascular risk factors; a review. Int J Stroke. 2012;7(1):61–73. doi:10.1111/j.1747-4949.2011.00731.x
- Luedtke K, Starke W, May A. Musculoskeletal dysfunction in migraine patients. Cephalalgia. 2018;38(5):865–875. doi:10.1177/0333102417716934
- Dodick DW. Migraine. Lancet. 2018;391(10127):1315–1330. doi:10.1016/S0140-6736(18)30478-1
- Liang Z, Galea O, Thomas L, Jull G, Treleaven J. Cervical musculoskeletal impairments in migraine and tension type headache: a systematic review and meta-analysis. Musculoskelet Sci Pract. 2019;42:67–83. doi:10.1016/j.msksp.2019.04.007
- Kanburoglu MK, Cizmeci MN, Akelma AZ, Rare A. Cause of chronic headache that may be misdiagnosed as migraine: chronic carbon monoxide poisoning. Turk J Emerg Med. 2014;14(3):132–134. doi:10.5505/1304.7361.2014.00868
- Witt CM, Jena S, Brinkhaus B, Liecker B, Wegscheider K, Willich SN. Acupuncture for patients with chronic neck pain. Pain. 2006;125(1–2):98–106. doi:10.1016/j.pain.2006.05.013
- Sheu SY, Yao CH, Fu YT, Wang WL. Acupuncture as complementary therapy for hypoxic encephalopathy: a case study. Complement Ther Med. 2010;18(6):265–268. doi:10.1016/j.ctim.2010.08.001
- Li X, Chen C, Yang X, et al. Acupuncture improved neurological recovery after traumatic brain injury by activating BDNF/TrkB pathway. eCAM. 2017;2017:8460145. doi:10.1155/2017/8460145
- Wang QR, Lu YY, Su YJ, et al. Migraine and traumatic brain injury: a cohort study in Taiwan. BMJ Open. 2019;9(7):e027251. doi:10.1136/bmjopen-2018-027251
- Holmquist S, Nordström A, Nordström P. The association of depression with subsequent dementia diagnosis: a Swedish nationwide cohort study from 1964 to 2016. PLoS Med. 2020;17(1):e1003016. doi:10.1371/journal.pmed.1003016
- Machado A, Herrera AJ, de Pablos RM, et al. Chronic stress as a risk factor for Alzheimer’s disease. Rev Neurosci. 2014;25(6):785–804. doi:10.1515/revneuro-2014-0035
- Prins ND, Scheltens P. White matter hyperintensities, cognitive impairment and dementia: an update. Nat Rev Neurol. 2015;11(3):157–165. doi:10.1038/nrneurol.2015.10
- Wolters FJ, Zonneveld HI, Hofman A, et al. Cerebral perfusion and the risk of dementia: a population-based study. Circulation. 2017;136(8):719–728. doi:10.1161/CIRCULATIONAHA.117.027448
- Woods RP, Iacoboni M, Mazziotta JC. Brief report: bilateral spreading cerebral hypoperfusion during spontaneous migraine headache. N Engl J Med. 1994;331(25):1689–1692. doi:10.1056/NEJM199412223312505
- Olesen J, Friberg L, Olsen TS, et al. Ischaemia-induced (symptomatic) migraine attacks may be more frequent than migraine-induced ischaemic insults. Brain. 1993;116(Pt 1):187–202. doi:10.1093/brain/116.1.187
- Duncombe J, Kitamura A, Hase Y, Ihara M, Kalaria RN, Horsburgh K. Chronic cerebral hypoperfusion: a key mechanism leading to vascular cognitive impairment and dementia. Closing the translational gap between rodent models and human vascular cognitive impairment and dementia. Clin Sci. 2017;131(19):2451–2468. doi:10.1042/CS20160727
- Ding N, Jiang J, Xu A, Tang Y, Li Z. Manual acupuncture regulates behavior and cerebral blood flow in the samp8 mouse model of alzheimer’s disease. Front Neurosci. 2019;13:37. doi:10.3389/fnins.2019.00037
- Hamedani AG, Rose KM, Peterlin BL, et al. Migraine and white matter hyperintensities: the ARIC MRI study. Neurology. 2013;81(15):1308–1313. doi:10.1212/WNL.0b013e3182a8235b
- Ma SM, Wang L, Su XT, et al. Acupuncture improves white matter perfusion and integrity in rat model of vascular dementia: an MRI-based imaging study. Front Aging Neurosci. 2020;12:582904. doi:10.3389/fnagi.2020.582904
- Han X, Bai L, Sun C, et al. Acupuncture enhances communication between cortices with damaged white matters in poststroke motor impairment. eCAM. 2019;2019:4245753. doi:10.1155/2019/4245753
- Gradus JL, Horváth-Puhó E, Lash TL, et al. Stress disorders and dementia in the Danish population. Am J Epidemiol. 2019;188(3):493–499. doi:10.1093/aje/kwy269
- Bennett S, Grant MM, Aldred S. Oxidative stress in vascular dementia and Alzheimer’s disease: a common pathology. JAD. 2009;17(2):245–257. doi:10.3233/JAD-2009-1041
- Zhao L, Liu L, Xu X, et al. Electroacupuncture inhibits hyperalgesia by alleviating inflammatory factors in a rat model of migraine. J Pain Res. 2020;13:75–86. doi:10.2147/JPR.S225431
- Du SQ, Wang XR, Zhu W, et al. Acupuncture inhibits TXNIP-associated oxidative stress and inflammation to attenuate cognitive impairment in vascular dementia rats. CNS Neurosci Ther. 2018;24(1):39–46. doi:10.1111/cns.12773
- MacQueen G, Frodl T. The hippocampus in major depression: evidence for the convergence of the bench and bedside in psychiatric research? Mol Psychiatry. 2011;16(3):252–264. doi:10.1038/mp.2010.80
- Park S, Lee JH, Yang EJ. Effects of acupuncture on Alzheimer’s disease in animal-based research. eCAM. 2017;2017:6512520. doi:10.1155/2017/6512520
- Lu J, Shao RH, Hu L, Tu Y, Guo JY. Potential antiinflammatory effects of acupuncture in a chronic stress model of depression in rats. Neurosci Lett. 2016;618:31–38. doi:10.1016/j.neulet.2016.02.040
- Ye Y, Li H, Yang JW, et al. Acupuncture attenuated vascular dementia-induced hippocampal long-term potentiation impairments via activation of D1/D5 receptors. Stroke. 2017;48(4):1044–1051. doi:10.1161/STROKEAHA.116.014696
- Zhang N, Houle T, Hindiyeh N, Aurora SK. Systematic review: acupuncture vs standard pharmacological therapy for migraine prevention. Headache. 2020;60(2):309–317. doi:10.1111/head.13723
- Zhao L, Chen J, Li Y, et al. The long-term effect of acupuncture for migraine prophylaxis: a randomized clinical trial. JAMA Intern Med. 2017;177(4):508–515. doi:10.1001/jamainternmed.2016.9378
- Ahlskog JE, Geda YE, Graff-Radford NR, Petersen RC. Physical exercise as a preventive or disease-modifying treatment of dementia and brain aging. Mayo Clin Proc. 2011;86(9):876–884. doi:10.4065/mcp.2011.0252