Abstract
Background
Structural brain abnormalities associated with delusions in Alzheimer’s disease are poorly understood. In addition, whether the neural substrate underlying the delusions develops before the onset of the delusions is unclear. In this study, we used a voxel-based morphometry approach to examine the existence of regional structural abnormalities at baseline in patients with Alzheimer’s disease who did and who did not develop delusions.
Methods
Using the Neuropsychiatric Inventory, we identified patients with Alzheimer’s disease who exhibited delusions during a 2-year period. All the patients had undergone a magnetic resonance imaging examination at the start of the study period (baseline). We conducted a voxel-based morphometry analysis using statistical parametric mapping (SPM5) software and compared the results of patients with Alzheimer’s disease who did and did not develop delusions.
Results
Compared with the patients who did not develop delusions (n = 35), the patients who did develop delusions (n = 18) had significantly smaller gray matter volumes on both sides of the parahippocampal gyrus, the right posterior cingulate gyrus, the right orbitofrontal cortex, both sides of the inferior frontal cortex, the right anterior cingulate, and the left insula.
Conclusion
Structural brain abnormalities involving both the frontal and medial temporal lobes may be crucial to the expression of delusions in patients with Alzheimer’s disease.
Introduction
Although not all neuropsychiatric diseases manifest psychotic symptoms, some types of brain disorders may be associated with secondary psychosis during the course of illness. Psychotic symptoms often arise because of a general medical illness, such as metabolic disorders without psychotic features. Not all patients with Alzheimer’s disease develop psychotic symptoms during the course of the disorder. However, among a wide variety of neuropsychiatric symptoms in patients with Alzheimer’s disease, psychotic symptoms, such as delusions, are particularly associated with increased caregiver burden,Citation1 a decreased quality of life for both the patient and the caregiver,Citation2 and a relatively poor prognosis for the course of the disease.Citation3 A 2-year, prospective, longitudinal study of patients with Alzheimer’s disease reported that the cumulative incidence of psychotic symptoms (delusions, hallucinations) was 36.9%.Citation4
The examination of possible predictors of the development of psychotic symptoms in patients with Alzheimer’s disease is clinically relevant. Several studies have suggested that greater cognitive impairment predicts an increased risk of the onset of psychosis in patients with Alzheimer’s disease.Citation5.Citation6 Several neuroimaging studies have implicated the frontal lobe, parietal lobe, striatal regions, and insula in the manifestation of delusions in patients with the disease.Citation7–Citation11 In a previous studyCitation12 examining structural brain abnormalities, significant findings indicated an association between low volumes of regional gray matter in several areas and delusions in patients with Alzheimer’s disease. However, whether the neural substrate underlying the delusional symptoms develops before the onset of delusions remains unclear.
Thus, we hypothesized that neuroanatomical abnormalities that predate the onset of delusions may exist in patients with Alzheimer’s disease who develop delusions. Therefore, we examined structural brain abnormalities using baseline data obtained for patients with Alzheimer’s disease without delusions at the time of image acquisition who were enrolled in a 2-year, prospective, longitudinal study. After the 2-year follow-up period, we compared the baseline findings of patients who developed delusions with those who did not using a voxel-based morphometry approach.
Materials and methods
Participants
The baseline sample consisted of Japanese patients with Alzheimer’s disease and mild functional severity who attended the outpatient clinic of Nagoya City University Hospital between June 2009 and December 2010. The diagnostic evaluation included a complete history and physical examination, routine blood tests (including an evaluation of serum vitamin B12 level and thyroid function), either a magnetic resonance imaging (MRI) or a computed tomography scan of the brain, and neuropsychological testing. Study inclusion criteria were a diagnosis of probable Alzheimer’s disease according to the National Institute of Neurological and Communication Disorders and Stroke/Alzheimer Disease and Related Disorders Association criteria,Citation13 no history of treatment with antipsychotic medications, and absence of psychotic symptoms as assessed using the Japanese version of the Neuropsychiatric Inventory (NPI).Citation14,Citation15 The NPI is a semiquantitative assessment based on information provided by the caregiver. The questionnaire consists of ten behavior-related questions concerning delusions, hallucinations, depression, anxiety, agitation, disinhibition, euphoria, irritability, apathy, and aberrant motor activity. The composite score for each item is obtained by multiplying the severity by the frequency, with composite scores ranging between 0 and 12. The maximum total NPI score for the 10 manifestations is 120. In accordance with our previous study,Citation2 psychotic symptoms were defined as delusions, hallucinations, agitation, disinhibition, irritability, and aberrant motor activity.
Patients were excluded if other neurological diseases were present, the patient had a previous history of mental illness or substance abuse before the onset of dementia, either an MRI or a computed tomography scan had revealed focal brain lesions, the patient’s Mini-Mental State Examination (MMSE)Citation16 score was <11, or reliable informed consent could not be obtained from the patient and/or his/her relatives. The study protocol was approved by the ethics committee of Nagoya City University Medical School. Both the subjects and their caregivers were informed of the purpose and procedures of this study and were asked to sign a consent form.
Follow-up assessment
The follow-up assessment was conducted within 2 years of the baseline assessment. The presence of delusions was diagnosed based on the delusion score on the NPI. In agreement with a previous study,Citation4 a score > 3 was regarded as indicating the presence of delusions. An independent psychiatrist who was unaware of the MRI results conducted the NPI evaluation. Both the MMSE and the NPI were assessed at 3-month intervals from the baseline examination.
MRI image acquisition
All the brain images were acquired at baseline using a 1.5-T MRI system (Gyoro Scan Intera; Philips Medical Systems, Best, The Netherlands). The scanning parameters for the three-dimensional T1-weighted turbo field echo sequences were as follows: echo time 3.90 msec; repetition time 8400 msec; flip angle 15 degrees; 256 × 256 matrices; field of view 25 cm; voxel size 1.0 × 1.0 × 1.0 mm; and slice thickness 1.0 mm. The MRI studies were performed in the Department of Radiology at Nagoya City University Hospital.
Voxel-based morphometry protocol
Voxel-based morphometry was performed using the VBM5.1 toolbox (http://dbm.neuro.uni-jena.de/vbm) with Statistical Parametric Mapping 5 (SPM5) running on Matlab 7.5 (Mathworks Inv, Sherborn, MA). Each 3D-MIRAGE image was normalized and segmented into gray matter, white matter, and cerebrospinal fluid components using the unified segmentation model,Citation17 which combines both normalization and segmentation parameters into a single generative model. The Volex values were modulated using Jacobian determinants for affine and nonlinear warping and smoothed using a Gaussian kernel with a full width at half maximum of 12 mm.
Statistical analysis
Comparisons between patients with Alzheimer’s disease who developed delusions and those who did not were conducted for the regional gray matter and white matter volumes using a two-samples t-test as an implement in SPM5. For all the analyses, the total brain volume, patient age, gender, education, duration (in years), and MMSE score were used as covariates of no interest. In addition, a multiple regression analysis was performed to test the relationship between the regional gray matter or white matter volumes at baseline and the change in the delusion score on the NPI between baseline and the time of appearance of delusions in patients with Alzheimer’s disease who developed them. For these analyses, the total brain volume and time between baseline and appearance of delusions (in months) and degree of change in MMSE score over this period were used as nuisance covariates. An absolute gray matter and white matter threshold of 0.1 was used to avoid possible edge effects between different tissue types. In this analysis, the voxel-wise statistical threshold of significance was set at P < 0.05, corrected for multiple comparisons using the false discovery rate approach.Citation18 The Montreal Neurologic Institute coordinates were transformed into Talairach coordinates and were then identified using the Talairach Daemon Client. Differences in the demographic and clinical variables between the two groups were examined using the t-test. The male to female ratio was compared using the Chi-square test.
Results
Demographic and clinical characteristics
Sixty-two patients with Alzheimer’s disease were enrolled in this study. Nine patients had been lost to follow-up at the end of the 2-year period, including six patients who had been transferred to another hospital and three patients who had been institutionalized. As a result, the remaining 53 patients participated in this study throughout the 2-year study period. Of these patients, 18 developed delusions and the remaining 35 did not develop delusions during the follow-up period. The types of delusions experienced by the patients, as identified by the NPI, were persecutory delusions (n = 13), misidentification delusions (n = 4), and both types (n = 1). Other types of delusions were not identified in this study. The mean time until development of delusions from the baseline assessment was 15.6 months (minimum of 6 months, maximum of 21 months).
Baseline demographic data for the patients are summarized in . No significant differences in demographic variables were found between the patients who developed delusions and those who did not. Regarding the NPI subscale scores, with the exception of depression/dysphoria and apathy, the two groups of patients both scored 0. Regarding the depression/dysphoria and apathy subscale, no significant differences were found between the two groups of patients ().
Table 1 Demographic data for patients with Alzheimer’s disease and delusions and those without delusions
Results of voxel-based morphometric analysis
and show the gray matter volume differences between the patients with Alzheimer’s disease who developed delusions and those who did not. At the time of the baseline assessments, the patients who developed delusions had significantly smaller gray matter volumes on both sides of the parahippocampal gyrus (Brodmann 19, 30), the right posterior cingulate gyrus (Brodmann 30), the right orbitofrontal cortex (Brodmann 11), both sides of the inferior frontal cortex (Brodmann 44, 47), the right anterior cingulate (Brodmann 24), the left claustrum, and the left insula (Brodmann 13), compared with the patients who did not develop delusions. No significantly smaller white matter volumes were observed in any brain region between the patients who developed delusions and those who did not. In addition, no significant correlation between regional gray matter or white matter volumes at baseline and change in the NPI delusions score at the time of appearance of delusions was observed among the patients who developed them.
Figure 1 (A) Smaller gray matter volumes in patients with Alzheimer’s disease and delusions (n = 18) than in those without delusions (n = 35) on both sides of the parahippocampal gyrus, both sides of the orbitofrontal cortex, and both sides of the medial frontal gyrus ventromedial prefrontal cortex. (B) Smaller gray matter volumes in patients with Alzheimer’s disease without delusions (n = 35) than in those with delusions (n = 18) in the left inferior temporal gyrus and the right cerebellum.
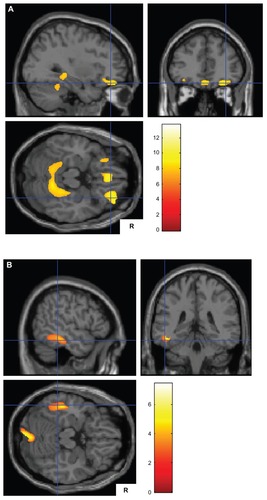
Table 2 Smaller gray matter volumes in patients with Alzheimer’s disease and delusions (n = 18) than in those without delusions (n = 35)
Table 3 Smaller gray matter volumes in patients with Alzheimer’s disease and without delusions (n = 35) than in those with delusions (n = 18)
At the time of the baseline assessments, the patients with Alzheimer’s disease who did not develop delusions showed significantly smaller gray matter volumes, as shown in (), in the right cerebellum, the left lingual gyrus (Brodmann 20), the left inferior temporal cortex (Brodmann 20, 37), and the left occipital cortex (Brodmann 18), compared with the patients who developed delusions. No significantly smaller white matter volumes were observed in any brain region among the patients who did not develop delusions compared with those who did develop delusions. In addition, we could not observe any significant correlations between regional gray matter or white matter volumes at baseline and reduction in delusion score on the NPI between baseline and the time of appearance of the delusions among the patients who developed delusions.
Discussion
To our knowledge, this is the first MRI study to examine baseline structural differences using a voxel-based morphometry approach in patients with Alzheimer’s disease who developed delusions and in those who did not. Compared with the patients who did not develop delusions, the patients who did develop delusions showed significantly smaller gray matter volumes in clinically important areas, including both sides of the parahippocampal gyrus (Brodmann 19, 30), the right orbitofrontal cortex (Brodmann 11), both sides of the inferior frontal gyrus (Brodmann 44, 47), the right anterior cingulate (Brodmann 11), and the left insula (Brodmann 13). These areas may be associated with the pathogenesis of delusion in patients with Alzheimer’s disease.
Previous neuroimaging studies have implicated frontal lobe dysfunction in the manifestation of delusions in patients with Alzheimer’s disease. The most consistent findings among previous functional neuroimaging studies were that delusions are associated with hypoperfusion and hypometabolism, primarily in the frontal lobe. These findings suggest that cortical dysfunction in the frontal lobe may be expressed as delusions during the course of Alzheimer’s disease.Citation19 Consistent with these findings, we observed a smaller gray matter volume in several areas of the frontal lobe in the patients with Alzheimer’s disease who developed delusions, compared with the patients who did not. Bruen et alCitation12 identified an association between reduced gray matter volumes on both sides of the inferior frontal gyrus and the left medial frontal gyrus and the experience of delusions in patients with Alzheimer’s disease. Alterations in other regions, such as the right orbitofrontal region and the anterior cingulate, have been reported in several studies using either single photon emission computed tomography or positron emission tomography.Citation9,Citation10,Citation20 These areas are thought to play an important role in attention and executive function associated with errors of logic, self-monitoring, and regulation of attention.Citation9,Citation10 Supporting this hypothesis, Tsoi et alCitation6 demonstrated that frontal executive impairments predict an increased risk of the onset of psychosis in patients with Alzheimer’s disease. Thus, structural abnormalities in these areas within the frontal lobe may result in dysfunction of attention and executive function, contributing to development of delusions in patients with the disease.
During the earliest stage of Alzheimer’s disease and mild cognitive impairment, apathy, depression, irritability, and anxiety, rather than delusions, are typically the most prominent symptoms among neuropsychiatric symptoms.Citation21–Citation23 Also, a recent studyCitation24 based on data from the Alzheimer’s Disease Neuroimaging Initiative database suggested that anxiety at baseline was associated with an increased hazard of progression from mild cognitive impairment to Alzheimer’s disease. Unlike in schizophrenia, delusions are not a core symptom of Alzheimer’s disease. Thus, while a cognitive decline may occur before the onset of delusions during the early stages of Alzheimer’s disease,Citation5,Citation6 symptoms of delusion are rarely a significant predictor of dementia associated with Alzheimer’s disease.
We also observed a reduced gray matter volume on both sides of the parahippocampal gyrus in patients with Alzheimer’s disease who developed delusions compared with patients who did not. Previous neuroimaging studies have suggested that medial temporal involvement is associated with delusions in patients with Alzheimer’s disease.Citation25,Citation26 Recently, Serra et alCitation27 demonstrated that delusions in patients with the disease were associated with the gray matter volume in the tail of the right hippocampus, which is involved in memory retrieval. Considering these findings, structural brain abnormalities in both the frontal and the medial temporal lobes may increase the likelihood that patients with Alzheimer’s disease will experience delusions. In addition, both the claustrum and the insula are reported to be associated with delusions in patients with the disease.Citation11,Citation12 Matsuoka et alCitation11 suggested that insular dysfunction might be responsible for exacerbation of delusions.
With regard to the smaller gray matter volumes observed in patients with Alzheimer’s disease who did not develop delusions compared with those who did, these findings are difficult to interpret. Although the cerebellum is not considered to be a primary area of pathological involvement in Alzheimer’s disease, the cerebellum may play an important role in coordination of motor and cognitive information.Citation28 However, we did not examine tasks associated with cerebellar function. Other areas, such as the lingual gyrus, inferior temporal gyrus, and occipital cortex, are known to be markers of progression of Alzheimer’s disease.Citation29,Citation30 Whether the patients with Alzheimer’s disease with gray matter reductions in these areas who did not develop delusions may experience a faster cognitive decline relative to patients with Alzheimer’s disease who develop delusions remains unclear. Further investigations of a long-term cohort study are needed to clarify the implications of the smaller gray matter volumes in patients who do not develop delusions.
Finally, we must address several limitations of this study. First, we observed a predominance of women among our patients with Alzheimer’s disease, as the prevalence of the disease is reportedly higher in women than in men.Citation31 Ikeda et alCitation32 also reported that a female predominance was evident among patients with delusion. Thus, the patients with Alzheimer’s disease enrolled in this study may have had a predisposition to delusions because of their gender. However, we could not identify any significant difference in gender between the patients with Alzheimer’s disease who developed delusions and those who did not. Second, the distinct neural basis underlying each of the various types of delusions needs to be examined. The limited number of patients with Alzheimer’s disease with misidentification delusions (n = 4) did not allow such an analysis in the present study. Third, our study included a relatively small number of patients. However, the rate of dropout (14%; n = 9) was relatively small. The results of this study will contribute to new findings regarding the neural basis for the expression of delusions in patients with Alzheimer’s disease. A larger cohort study is needed to allow multiple topics to be studied. Fourth, apolipoprotein E is known to influence the development of specific neuropsychiatric symptoms.Citation33,Citation34 Unfortunately, in this study, we did not examine the apolipoprotein E genotypes in the patients with Alzheimer’s disease. Further studies are needed to clarify the effect of apolipoprotein E on the development of delusions in patients with the disease. Fifth, although individual differences in brain volume exist among patients with Alzheimer’s disease, the voxel-based morphometry technique involves spatial normalization to remove inter-individual variations in brain size and shape.Citation35 However, we analyzed the MRI data only at baseline to compare brain abnormalities that predated the onset of delusions. We could not longitudinally assess the structural changes in patients with Alzheimer’s disease who developed delusions with those who did not using the MRI data. Thus, in this study, we could not detect dynamic changes in the brain structures of patients with Alzheimer’s disease during the 2-year follow-up period. However, some of the neuroanatomical abnormalities might have predated the expression of delusions in these patients.
Despite these limitations, the current study implies that structural brain abnormalities in the frontal and medial temporal lobes may be linked with the subsequent onset of delusions in patients with Alzheimer’s disease. The ability to predict the onset of delusions in patients with the disease based on MRI findings is clinically relevant for early intervention in those who develop delusions.
Acknowledgment
The authors gratefully acknowledge funding from a Grant-in-Aid for Scientific Research (22530750, 22591293) from the Ministry of Education, Culture, Sports, Sciences, and Technology in Japan.
Disclosure
The authors report no conflicts of interest in this work.
References
- MatsumotoNIkedaMFukuharaRCaregiver burden associated with behavioral and psychological symptoms of dementia in elderly people in the local communityDement Geriatr Cogn Disord200723421922417299264
- MatsuiTNakaakiSMurataYDeterminants of the quality of life in Alzheimer’s disease patients as assessed by the Japanese version of the Quality of Life-Alzheimer’s disease scaleDement Geriatr Cogn Disord200621318219116401890
- ScarmeasNBrandtJAlbertMDelusions and hallucinations are associated with worse outcome in Alzheimer diseaseArch Neurol200562101601160816216946
- AaltenPde VugtMELousbergRBehavioral problems in dementia: a factor analysis of the neuropsychiatric inventoryDement Geriatr Cogn Disord20031529910512566599
- WilkoszPAMiyaharaSLopezOLDekoskySTSweetRAPrediction of psychosis onset in Alzheimer disease: the role of cognitive impairment, depressive symptoms, and further evidence for psychosis subtypesAm J Geriatr Psychiatry200614435236016582044
- TsoiTBaillonSLindesayJEarly frontal executive impairment as a predictor of subsequent behavior disturbance in dementiaAm J Geriatr Psychiatry200816210210818239195
- HironoNMoriEIshiiKAlteration of regional cerebral glucose utilization with delusions in Alzheimer’s diseaseJ Neuropsychiatry Clin Neurosci19981044334399813789
- FukuharaRIkedaMNebuAAlteration of rCBF in Alzheimer’s disease patients with delusions of theftNeuroreport200112112473247611496132
- SultzerDLBrownCVMandelkernMADelusional thoughts and regional frontal/temporal cortex metabolism in Alzheimer’s diseaseAm J Psychiatry2003160234134912562582
- NakanoSYamashitaFMatsudaHKodamaCYamadaTRelationship between delusions and regional cerebral blood flow in Alzheimer’s diseaseDement Geriatr Cogn Disord2006211162116254426
- MatsuokaTNarumotoJShibataKInsular hypoperfusion correlates with the severity of delusions in individuals with Alzheimer’s diseaseDement Geriatr Cogn Disord201029428729320375510
- BruenPDMcGeownWJShanksMFVenneriANeuroanatomical correlates of neuropsychiatric symptoms in Alzheimer’s diseaseBrain200813192455246318669506
- McKhannGDrachmanDFolsteinMKatzmanRPriceDStadlanEMClinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services. Task Force on Alzheimer’s DiseaseNeurology19843479399446610841
- CummingsJLMegaMGrayKRosenberg-ThompsonSCarusiDAGornbeinJThe Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementiaNeurology19944412230823147991117
- HironoNMoriEIkejiriYJapanese version of the Neuropsychiatric Inventory – a scoring system for neuropsychiatric disturbance in dementia patientsNo to shinkei = Brain and nerve1997493266271 Japanese9125732
- FolsteinMFFolsteinSEMcHughPR“Mini-mental state”. A practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res19751231891981202204
- AshburnerJFristonKJUnified segmentationNeuroImage200526383985115955494
- GenoveseCRLazarNANicholsTThresholding of statistical maps in functional neuroimaging using the false discovery rateNeuroImage200215487087811906227
- IsmailZNguyenMQFischerCESchweizerTAMulsantBHNeuroimaging of delusions in Alzheimer’s diseasePsychiatry Res20122022899522703622
- MegaMSLeeLDinovIDMishkinFTogaAWCummingsJLCerebral correlates of psychotic symptoms in Alzheimer’s diseaseJ Neurol Neurosurg Psychiatry200069216717110896687
- MegaMSCummingsJLFiorelloTGornbeinJThe spectrum of behavioral changes in Alzheimer’s diseaseNeurology19964611301358559361
- LyketsosCGLopezOJonesBFitzpatrickALBreitnerJDeKoskySPrevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the cardiovascular health studyJAMA2002288121475148312243634
- HwangTJMastermanDLOrtizFFairbanksLACummingsJLMild cognitive impairment is associated with characteristic neuropsychiatric symptomsAlzheimer Dis Assoc Disord2004181172115195459
- WadsworthLPLoriusNDonovanNJNeuropsychiatric symptoms and global functional impairment along the Alzheimer’s continuumDement Geriatr Cogn Disord20123429611122922821
- MentisMJWeinsteinEAHorwitzBAbnormal brain glucose metabolism in the delusional misidentification syndromes: a positron emission tomography study in Alzheimer diseaseBiol Psychiatry19953874384498672604
- StaffRTShanksMFMacintoshLPestellSJGemmellHGVenneriADelusions in Alzheimer’s disease: spet evidence of right hemispheric dysfunctionCortex199935454956010574080
- SerraLPerriRCercignaniMAre the behavioral symptoms of Alzheimer’s disease directly associated with neurodegeneration?J Alzheimers Dis201021262763920555138
- KusbeciOYBasOGocmen-MasNEvaluation of cerebellar asymmetry in Alzheimer’s disease: a stereological studyDement Geriatr Cogn Disord20092811519602887
- ChetelatGLandeauBEustacheFUsing voxel-based morphometry to map the structural changes associated with rapid conversion in MCI: a longitudinal MRI studyNeuroImage200527493494615979341
- KinkingnehunSSarazinMLehericySGuichart-GomezEHerguetaTDuboisBVBM anticipates the rate of progression of Alzheimer disease: a 3-year longitudinal studyNeurology200870232201221118448872
- HironoNMoriETanimukaiSDistinctive neurobehavioral features among neurodegenerative dementiasJ Neuropsychiatry Clin Neurosci199911449850310570764
- IkedaMShigenobuKFukuharaRDelusions of Japanese patients with Alzheimer’s diseaseInt J Geriatr Psychiatry200318652753212789674
- Van der FlierWMStaekenborgSPijnenburgYAApolipoprotein E genotype influences presence and severity of delusions and aggressive behavior in Alzheimer diseaseDement Geriatr Cogn Disord2007231424617077632
- ChenCSOuyangPYehYCApolipoprotein E polymorphism and behavioral and psychological symptoms of dementia in patients with Alzheimer diseaseAlzheimer Dis Assoc Disord201226213513921617520
- BusattoGFDinizBSZanettiMVVoxel-based morphometry in Alzheimer’s diseaseExpert Rev Neurother20088111691170218986240