
Abstract
Fragile X syndrome (FXS) is the most common genetic cause of intellectual disability and the most common single-gene cause of autism. It is caused by mutations on the fragile X mental retardation gene (FMR1) and lack of fragile X mental retardation protein, which in turn, leads to decreased inhibition of translation of many synaptic proteins. The metabotropic glutamate receptor (mGluR) hypothesis states that the neurological deficits in individuals with FXS are due mainly to downstream consequences of overstimulation of the mGluR pathway. The main efforts have focused on mGluR5 targeted treatments; however, investigation on the gamma-aminobutyric acid (GABA) system and its potential as a targeted treatment is less emphasized. The fragile X mouse models (Fmr1-knock out) show decreased GABA subunit receptors, decreased synthesis of GABA, increased catabolism of GABA, and overall decreased GABAergic input in many regions of the brain. Consequences of the reduced GABAergic input in FXS include oversensitivity to sensory stimuli, seizures, and anxiety. Deficits in the GABA receptors in different regions of the brain are associated with behavioral and attentional processing deficits linked to anxiety and autistic behaviors. The understanding of the neurobiology of FXS has led to the development of targeted treatments for the core behavioral features of FXS, which include social deficits, inattention, and anxiety. These symptoms are also observed in individuals with autism and other neurodevelopmental disorders, therefore the targeted treatments for FXS are leading the way in the treatment of other neurodevelopmental syndromes and autism. The GABAergic system in FXS represents a target for new treatments. Herein, we discuss the animal and human trials of GABAergic treatment in FXS. Arbaclofen and ganaxolone have been used in individuals with FXS. Other potential GABAergic treatments, such as riluzole, gaboxadol, tiagabine, and vigabatrin, will be also discussed. Further studies are needed to determine the safety and efficacy of GABAergic treatments for FXS.
Introduction
Fragile X syndrome (FXS) is the most common cause of inherited intellectual disability and largest single-gene cause of autism.Citation1 The fragile X mental retardation gene (FMR1) located on the X chromosome at band q27.3 typically has 5–44 CGG repeats; however, this trinucleotide repeat length can expand to an unstable repeat length. 45–54 CGG repeats is considered a gray zone and may have some clinical involvement, including a higher rate of primary ovarian insufficiency compared to controls.Citation2 Premutation carriers have trinucleotide repeats ranging from 55–200 CGG in length. These are usually healthy individuals who are at risk of developing fragile X-associated tremor/ataxia syndrome, a neurodegenerative disorder seen in aging carriers.Citation3 They are also at an increased risk for anxiety and mood disorders,Citation4 immune-mediated disorders,Citation5 migraine headaches,Citation6 hypertension,Citation7 and primary ovarian insufficiency,Citation8 all of which range in severity and prevalence. Adult female carriers have evidence of gamma-aminobutyric acid (GABA) dysfunction.Citation9
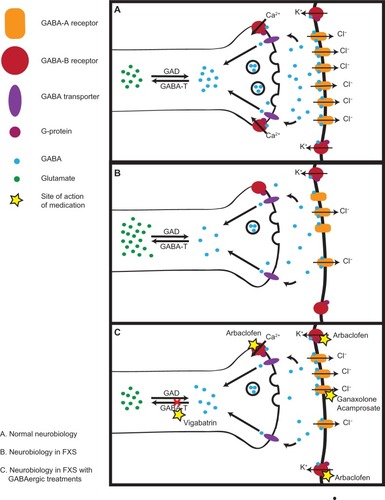
Figure 1 Neurobiology in FXS.
Abbreviations: FMRP, fragile X mental retardation protein; FXS, fragile X syndrome; GABA, gamma-aminobutyric acid; GABA-T, gamma-aminobutyric acid transaminase; GAD, glutamic acid decarboxylase.
There are some carriers who may show an attention-deficit hyperactivity disorder (ADHD) and autism spectrum disorders (ASDs);Citation10 however, the prevalence of those traits is far more common in individuals with the full mutation whose trinucleotide expansion is greater than 200 CGG repeats. The full mutation presents with a range of clinical features, including ADHD, ASDs, anxiety, intellectual disability, social avoidance, aggression, stereotyped behaviors, disrupted sleep patterns, epilepsy, macroorchidism, prominent ears, long faces, soft skin, and hyperextensible joints.Citation11 Males with the full mutation are typically more severely affected than females due to the compensatory nature of the second X chromosome, which still translates the FMR1 gene leading to more normal fragile X mental retardation protein (FMRP) production. The prevalence of the full mutation is approximately one in 5,000 malesCitation12 and one in 8,000 females,Citation13 whereas the premutation is far more common, at one in 130–250 females and one in 250–810 males.Citation14
The expansion of the trinucleotide sequence results in lowered FMRP levels. The premutation expansion results in a two- to eightfold increase in FMR1 mRNA levels, which leads to RNA toxicity accounting for phenotypic features; however, the FMRP levels often stay normal or become somewhat decreased, particularly after 120 CGG repeats.Citation15,Citation16 The full mutation results in reduced or no FMRP production, which is found primarily in the brain and testes. In the brain, FMRP is crucial to synaptic development and refinement thus accounting for the psychiatric features of FXS, while its presence in the testes is needed for normal testicular size. The primary function of FMRP is to negatively regulate protein translation at the synapse,Citation17 and it is estimated that FMRP binds up to 4%–8% of mRNA within the brain.Citation18 This regulation is crucial in the metabotropic glutamate receptors (mGluRs) 1 and 5, which become upregulated, leading to exaggerated long-term depression (LTD). This concept is the basis of the mGluR theory of FXSCitation19 and the focus of many targeted treatments for FXS, such as the mGluR5 antagonists AFQ056 (mavoglurant; Novartis Pharmaceuticals, Basel, Switzerland) and RO4917523 (F Hoffmann-La Roche AG, Basel, Switzerland).
Additionally implicated in the dysregulation at the synapse is the GABA system, which is important in synaptic inhibition. An imbalance between the excitatory glutamatergic and the inhibitory GABAergic neurotrans-mission is proposed to cause the cognitive impartments, anxiety, and autism of FXS and other neuropsychiatric and neurodevelopmental disorders.Citation1,Citation20,Citation21 While two medications have been developed specifically for GABAergic modulation – arbaclofen (Seaside Therapeutics, Cambridge, MA, USA) and ganaxolone (Marinus Pharmaceuticals, Inc., New Haven, CT, USA) – this paper will also address GABAergic medications such as riluzole, gaboxadol, tiagabine, and vigabatrin. Before discussing the medications, a more in-depth focus on the GABA system and its dysregulation in FXS will follow.
Neurobiology
More than 3 decades of molecular research have led to a better understanding of the neurobiology of FXS and related disorders. FXS is caused by a dynamic mutation of more than 200 CGG trinucleotide repeats in the 5’ untranslated region on the FMR1 gene, which results in an absence of expression of FMRP. FMRP is a selective RNA-binding protein, found most abundantly in the CNS and testes, which regulates the expression of many mRNAs through inhibitory control at the synapse.Citation22 The crucial role of FMRP in regulating the synthesis of synaptic proteins extends beyond the phenotype of FXS to other neurodevelopmental and neuropsychiatric disorders, in which FMRP may also be deficient.Citation23
FMRP contains three main RNA-binding domains: two hnRNP K-homology domains and one arginine- and glycine-rich region of FMRP. In vitro FMRP is part of messenger ribonucleoparticles (structures that are involved in protein synthesis) and regulates dendritic transport of associated mRNAs.Citation22 FMRP interacts with several cytoplasmic and nuclear proteins and has been found in granules containing translationally silent preinitiation complexes. In summary, FMRP regulates RNA transportation, stabilization, and translation, mainly at the synapse in neurons.
The activation of mGluR5 induces protein synthesis in the soma, axons, dendrites, and postsynaptic sites, as well as degradation and recycling of somatic and axonic proteins through the MAPK/ERK and mTOR pathways, which is required for LTD, a form of hippocampal synaptic plasticity that develops and consolidates long-term memories. In the Fmr1-knock out [KO] mice, LTD is significantly increased, and this leads to deficits in synaptic plasticity and weakening of synaptic connections.Citation22 The mGluR theory, which suggests that psychiatric and neurological aspects of the syndrome are due to exaggerated downstream consequences of mGluR5 upregulation, was validated by genetic mouse studies in which rescue of several symptoms occurred when the Fmr1-KO mouse was crossed with the mGluR heterozygous mouse.Citation24 The Fmr1-KO also shows hypothalamic excess of many synaptic proteins from increased protein translation rate and protein synthesis, whereas the GABA system is downregulated in the absence of FMRP, as described in the GABA neurobiology section.Citation25
GABA neurobiology
The GABA system is the main inhibitory system in the brain. It works through two classes of GABA receptors: GABAA and GABAB. GABAA receptors are ligand-gated ion channels, whereas GABAB receptors are G protein-coupled receptors. GABAA receptors allow the flow of chloride ions across the membrane, which hyperpolarizes the neuron’s postsynaptic membrane and minimizes the effect of any coincident synaptic input. GABAB receptors hyperpolarize the neuron’s membrane by activating G-protein-coupled inwardly rectifying potassium channels.Citation26 The GABA receptors are very diverse in their subunit composition and localization at the synapse and in regions of the brain; their effects are fast or slow persistent-tonic inhibition, depending on their localization and grade of stimulation.Citation27
The GABA system is required for a balanced neuronal activation and network oscillations, direct flow of information, neural synchrony, and facilitating the movement of information in and between multiple brain areas involved in cognition.Citation28–Citation30 Since FXS is characterized by anxiety, hyperarousal, and epilepsy,Citation31,Citation32 recent studiesCitation33–Citation36 have aimed to identify the defects in the inhibitory GABA system in the Fmr1-KO mouse.
GABAA
FMRP targets the mRNAs encoding eight different GABAA receptor subunits (α1, α3, α4, β1, β2, γ1, γ2, and δ), which were significantly reduced in the neocortex and cerebellum of Fmr1-KO mice, particularly the γ subunit, which represents extrasynaptic (perisynaptic) GABAA receptors.Citation37,Citation38 The Fmr1-KO mouse confirms a deficit in the production of GABAA receptors. Proteins required for GABA transport (eg, GABA transporter) and catabolism (eg, GABA transaminase [GABA-T], succinic semialdehyde [SSADH]) are also reduced.Citation33,Citation34 In addition, FMRP in the presynaptic side also regulates the expression of glutamic acid decarboxylase, which is the rate-limiting GABA-synthesis enzyme.Citation33,Citation35,Citation37 Therefore, FMRP regulates the expression, metabolism, and catabolism of the GABAA receptors, and in its absence, there is a decreased GABAergic input. The Fmr1-KO mouse exhibits reduced inhibitory postsynaptic currents in the amygdalaCitation35 and subicular neurons.Citation36 Although FMRP inhibits the translation of many messages, it can also stimulate the translation of mRNAs, and the GABA system is downregulated in the absence of FMRP. Consequences of the reduced GABAA receptor expression in FXS likely include oversensitivity to sensory stimuli, seizures, and anxiety.
GABAB
GABAB is a metabotropic G protein-coupled receptor that regulates voltage-gated Ca2+ channels, G protein inwardly rectifying K+ channels, and adenylyl cyclase.Citation26 Activation of the receptor triggers slow inhibitory postsynaptic currents, which reduce the neuronal excitability.Citation26 Presynaptic GABAB receptors inhibit glutamate release, which further exacerbates the upregulation of the mGluR5 system; therefore, treatment with GABAB modulators has the potential to correct phenotypic deficits in FXS. When treated with a double-knockout of FMR1 and RGS4, male Fmr1-KO mice showed reduced susceptibility to audiogenic seizures.Citation39 Since RGS4 is a regulator of G protein signaling and associated with GABAB receptors and inward-rectifying K+ channels, it has a therapeutic potential to regulate GABAB subunits in the treatment of FXS.Citation39
Impacted regions of the brain
The amygdala, a component of the limbic system involved in emotional recognition and reaction, as well as fear processing, is one part of the brain considerably impacted by GABAergic dysregulation. Socioemotional impairments are prevalent in both premutation and full mutation patients, which warrants study of the amygdala as a basis for this impairment. Numerous studies have been performed assessing amygdala volume, activation in relation to gaze processing, and facial-emotional processing, which yield contradictory and inconsistent results due to varied protocols and populations (as summarized in Kim et al).Citation40 Fear-specific activation of the amygdala was significantly reduced in patients with FXS compared to neurotypical controls, despite no differences in amygdala volume,Citation40 which suggests biological impairment possibly at the synaptic level instead of altered brain size leading to emotional dysregulation. The amygdala’s phasic inhibitory postsynaptic currents, tonic inhibitory currents, reduced GABA release, and inhibitory synapses are considerably reduced in frequency and amplitude in the amygdala of Fmr1-KO mice.Citation35 Due to the phenotypic socioemotional impairments seen in both the premutation and full mutation individuals alongside the biological impairments seen in the Fmr1-KO mouse, the amygdala is a point of study for gauging improvement with new treatments.
Further modifications in GABAergic activity are found in the cortex of the brain in FXS and, while monosynaptic GABAergic transmission is unaffected, there is a substantial deficit in local excitatory drive targeting fast-spiking inhibitory neurons in layer 4 of the somatosensory (barrel) cortex, which partially accounts for seizures, cognitive dysfunction, and sensory hypersensitivity of the FXS phenotype.Citation41
A study assessing GABA-mediated cerebellar inhibition comparing healthy, asymptomatic women with and without the premutation found that women with the premutation show an absence of cerebellar inhibition over primary motor cortex as well as reduced GABAA-mediated intracortical and afferent inhibition.Citation9 Even in asymptomatic carriers, there is still GABA dysregulation, which warrants the need for compounds with GABAergic modulation properties in premutation carriers. The available compounds are limited and mostly focus on antiepileptic properties; however, other mechanisms of action modified by such treatments may provide additional outlets for improving the phenotype in both carriers and individuals affected by the full mutation.
GABAergic treatments
After a better understanding of the neurobiology and neuropathogenesis of FXS, many compounds have been used as targeted treatments for FXS. Research has focused mainly on the development of mGluR5 antagonists, but better understanding of the GABAergic system in FXS has led to a new GABAergic approach and relevant targeted treatment. The GABA receptors in different regions of the brain are associated with some behavioral phenotypes in individuals with FXS. Particular attention has been devoted to correcting the amygdala-based symptoms. GABAergic agonists can be used for specific phenotypes including anxiety, autistic behavior, epilepsy, and cognitive impairment. GABA agonists have shown very limited efficacy in preliminary studies for these symptoms, but they have been well tolerated.Citation42,Citation43 The GABAergic treatments are a relatively new area and basic and translational research is limited in spite of their potential to treat FXS based on animal and small clinical studies.
Acamprosate
Acamprosate is a GABAA agonist approved for treatment of alcohol withdrawal. Excessive alcohol consumption over a long period of time changes the balance between the excitatory and inhibitory systems. Acamprosate helps people who have consumed large amounts of alcohol by stabilizing the excitatory/inhibitory balance in the brain, mainly by enhancing the function of GABAA receptors and, possibly, by its inhibitory effects on the mGluRs.Citation44 Acamprosate does not prevent the withdrawal symptoms that people may experience when they stop drinking alcohol.
Clinically, a short report of three patients with FXS treated with acamprosate showed improvements in language and behavior,Citation44 which led to other GABAergic targeted treatments and a second open-label 10-week trial of acamprosate (mean dose 1,054±422 mg/day) in 12 children and adolescents ages 6 to 17 years with FXS. The study showed improvements in social behavior and inattention/hyperactivity using multiple standard behavioral outcome measures. A Clinical Global Impressions-Improvement (CGI-I) scale score of “very much improved” or “much improved” was rated in nine of 12 (75%) subjects. No significant adverse effects were reported. Additionally, pre- and posttreatment blood biomarker analyses were performed by measuring brain-derived neurotrophic factor (BDNF) levels. A significant increase in the BDNF levels with treatment was described. However, treatment response did not correlate with change in the BDNF level.Citation44
Ganaxolone
Ganaxolone (3a-hydroxy-3B-methyl analog of allopregnanolone) is a GABAA receptor agonist through allosteric modulation that has anticonvulsant, anxiolytic, and sedative effects.Citation45 It is orally active and does not have hormonal effects. Neuroactive steroids like ganaxolone act most potently and effectively on GABAA receptors containing δ subunits. Ganaxolone is under development for treatment of seizure disorders and posttraumatic stress disorder. This pharmaceutical has been well tolerated, is safe in adults, children, and infants,Citation46 and has been found to improve symptoms in humans and mouse models.Citation46,Citation47
Although many GABAA receptor subtypes are diminished in the Fmr1-KO mouse, there is evidence that extrasynaptic γ subunit containing GABAA receptors are especially affected.Citation48 In the Fmr1-KO, ganaxolone has been shown to decrease audiogenic seizures.Citation47 Similarly, studies in the dfmr mutant fly showed that GABAA agonists ameliorate the lethality phenotype of glutamate-containing food, neuropathology, excessive protein translation, and abnormal courtship behavior.Citation49 The most frequently reported adverse events with ganaxolone in seizure studies are somnolence, convulsion, agitation, pharyngitis, otitis media, diarrhea, vomiting, cough, and pyrexia.Citation50 A randomized, Phase II, double-blind, placebo-controlled crossover trial to investigate the efficacy of ganaxolone for the treatment of anxiety and attention deficits in children with FXS aged 6 to 17 years (http://www.ClinicalTrials.gov; NCT01725152)Citation51 is currently under way. Ganaxolone should increase and normalize GABAA-mediated signaling – by boosting the signaling capacity of existing receptors – and improve behavior, particularly anxiety and attention.
Gaboxadol (THIP)
Tonic GABAA inhibition is associated with specific receptor subunits, particularly the relatively rare α4, α6, and δ subunits. The δ subunit-containing receptors are insensitive to benzodiazepine agonists,Citation52,Citation53 but highly sensitive to gaboxadol.Citation54,Citation55 Gaboxadol, the selective δ-GABAA super-agonist receptor, 4,5,6,7-tetrahydroisoxazolo(5,4-c) pyridin-3-ol (also known as THIP), has properties to generate tonic inhibition, namely activation by low concentrations of GABA through the activation of the extrasynaptic δ subunit-containing receptors.Citation54,Citation56
As previously mentioned, Fmr1-KO mouse studies have showed deficits in inhibitory transmission in the amygdala of the Fmr1-KO mouse, including reduction in the frequency and amplitude of phasic inhibitory postsynaptic currents and of tonic inhibitory currents, as well as a reduction in the number of inhibitory synapses and in neuronal hyperexcitability in principal neurons.Citation35
A neuronal study has also shown significant increases in the action potential threshold in both wild-type and Fmr1-KO mice.Citation57 Strikingly, the action potential threshold in Fmr1-KO mice in amygdala slices was restored to wild-type levels by THIP application. Thus, the electrophysiological abnormalities of neuronal hyperexcitability in the Fmr1-KO amygdala can be dramatically rescued by augmenting tonic inhibitory tone.Citation35 A behavioral study in Fmr1-KO mice have shown that THIP significantly attenuated hyperactivity and reduced prepulse inhibition in a volume-dependent manner. However, THIP did not reverse the deficits in cued fear or startle response.Citation58 Current studies show that enhancing GABAergic transmission can correct specific behavioral phenotypes of the Fmr1-KO mouse, further supporting focus on the GABAergic system and, specifically, tonic inhibition, which might be important for correcting or ameliorating specific behaviors in FXS.Citation47,Citation49,Citation58
Gaboxadol reached a Phase III trial before its cessation because of side effects, such as hallucination and disorientation. Due to these safety concerns and lack of efficacy, work on the drug was discontinued in 2007; however, recent studies in animal models of ASD have shown that gaboxadol is effective in rescuing neurophysiological and behavioral deficits.Citation58,Citation59 Further studies in fragile X animal models are necessary to provide cumulative evidence in the efficacy and safety of gaboxadol. Currently, there are no studies in individuals with FXS.
Vigabatrin
Vigabatrin is an antiepileptic and analog of GABA (although not an agonist) that inhibits the catabolism of GABA by irreversibly inhibiting GABA transaminase. It has been found that the half-life of biologic activity is far longer than the elimination half-life,Citation60,Citation61 and there is no range of target concentrations because there was no difference between the serum concentration levels of responders and those of nonresponders.Citation61 In addition, the duration of action is more a function of the GABA transaminase resynthesis rate.Citation62 Vigabatrin has been approved by the US Food and Drug Administration (FDA) for use in patients with refractory complex partial seizures, but the rentinal toxicity of the medication limits it’s use to those who have not responded to other treatments.Citation63 However, it is recommended when the benefits outweigh the side effects in individuals with intractable seizures. There are no studies in FXS animal models or clinical trials in individuals with FXS.
Arbaclofen
One compound shown to influence GABA regulation in the Fmr1-KO mouse is arbaclofen, a GABAB agonist developed by Seaside Therapeutics. Arbaclofen is a receptor agonist and active enantiomer of racemic baclofen, which presynaptically blocks glutamate release, thereby decreasing the overactivation of the glutamatergic pathways. In Fmr1-KO mice, arbaclofen corrected elevated protein synthesis in the hippocampus; reduced elevated AMPA (α-Amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid) receptor internalization to wild-type values; decreased mRNA translation in the cortex; and corrected the increased spine density prevalent in the mouse phenotype.Citation64
In pediatric, adolescent, and adult patients with FXS, arbaclofen was administered in a randomized, double-blind, placebo-controlled crossover study. The primary outcome measure, the Aberrant Behavior Checklist-Community Edition, a 58-item behavioral questionnaire, did not show reduction in any of the subscales compared to placeboCitation42 and, due to resource limitations, Seaside Therapeutics had to terminate its arbaclofen program.Citation65 However, a post hoc analysis saw a full study improvement on the Aberrant Behavior Checklist Social Avoidance subscale, which was an algorithm developed specifically to assess behavioral function in patients with FXS.Citation66 In addition, a subgroup of 27 patients with more severe social impairment treated with arbaclofen showed improvement on all global measures, as well as on the Vineland Socialization subscale, which is a semi-structured parent interview that assesses adaptive behavior. There were also trends of improvement seen on parent-nominated problem behaviors in the visual analog scale as well as on multiple global measures.Citation42 This demonstrates the need to use biological subtyping, particularly in a heterogeneous group of patients, such as those with ASD. For the subgroup of patients with FXS who did very well with arbaclofen, it became a problem to obtain the drug once the company folded, and the withdrawal from arbaclofen was very difficult for many families. Overall, arbaclofen was well tolerated, with sedation and headache being the most commonly reported side effects.Citation42
Riluzole
Riluzole is a medication approved for the treatment of amyotrophic lateral sclerosis, which blocks voltage-gated Na+ channels and selectively depresses glutamate over GABA release and which, at higher concentrations, can potently increase postsynaptic GABAA response in hippocampal neurons.Citation67 Due to the GABAergic dysregulation and epilepsy shown in patients with FXS, it was proposed that riluzole could act as a beneficial treatment for FXS. An open-label study of riluzole in patients with FXS showed a clinical response in only one of six patients, with significant improvement as measured on the ADHD Rating Scale-IV.Citation43 Riluzole administration was also associated with significant correction of ERK activation time in all subjects. Overall, the medication was well tolerated and showed non-clinically significant increases in liver function tests,Citation43 a notable side effect of the medication.
Tiagabine
Tiagabine, a nipecotic acid derivative, is another antiepileptic that reduces neuronal and astrocytic uptake of GABA.Citation68 Sound-induced convulsions in DBA/2 mice – which, notably, had no sedation or motor debilitationCitation70 – were corrected when tiagabine was administered;Citation69 however, there have not been any studies assessing the efficacy of tiagabine in treating FXS. While it may be used to control epilepsy in patients with FXS, other antiepileptic medications seem to have more potent treatment responses.Citation71
Conclusion
Numerous GABAergic compounds are potential treatments for FXS; however, considerably more basic and translational research is needed. The current studies are mostly open-label treatment options with small sample sizes of patients in a wide age range. Larger, double-blind, placebo-controlled trials are needed to assess the efficacy of these treatments against the placebo in order to better establish the treatment profile of each medication. The largest double-blind, placebo-controlled study using a GABAergic compound in FXS used arbaclofen. Despite trends in a positive treatment response on secondary outcome measures, Seaside Therapeutics could not continue with additional studies focusing on the secondary outcome measures due to limited resources. This outcome brings to light the difficulty of establishing efficacy of targeted treatments in this population.Citation42,Citation72
A number of new treatments are also being studied in clinical trials after promising efficacy studies in the animal models of FXS.Citation73 These include lovastatin, which lowers ERK phosphorylation in the mTOR pathway, and an insulin-like growth factor 1 analog made by Neuren (Neuren Pharmaceuticals Limited, Camberwell, VIC, Australia). Other treatment trials are in the pipeline but have yet to come to clinical trials.Citation74
There are a number of barriers to new treatments, including the time and expense of carrying out the toxicity studies in animals and humans and subsequent multicenter human trials to demonstrate efficacy. Although FXS is a single-gene disorder, there is significant heterogeneity in clinical involvement and response to treatment. For many trials, approximately 30% respond well, but this may not be adequate to demonstrate overall efficacy, which prohibits FDA approval for marketing. The lack of biomarkers that would predict efficacy is greatly needed so that a “likely to respond subgroup” could be identified.
For example, the AFQ056 compound by Novartis appears to be most effective for those who are fully methylated, but additional biomarkers are needed.Citation75 In addition, outcome measures that are quantitative and relate to central nervous system function or molecular changes and do not depend on questionnaires from the family would be useful to decreasing the placebo effect. Event-related potential paradigms of cognitive processing would also be useful, and we have seen a positive effect using the oddball paradigm and habituation task in children treated with minocycline in a controlled trial.Citation76
The placebo effect is high, owing to the overwhelming need for effective interventions, which is further impacted by the difficulty of obtaining objective outcome measures that accurately assess a behavioral treatment response. A majority of the improvement measures were based on parent or caregiver response,Citation42,Citation66 which is subjective. More objective outcome measures are needed, not only for GABAergic medications, but for all clinical trials that focus on neurodevelopmental indications. Biomarkers relating specifically to GABA upregulation in patients who did improve on the arbaclofen medication would be a vital tool for establishing efficacy against placebo.
Combined clinical trials using two drugs or a drug with an intervention program may show positive outcomes for FDA approval. A combined clinical trial of lovastatin with language intervention for individuals with FXS has been supported by the National Institute of Child Health and Human Development.Citation77 GABA downregulation and mGluR5 upregulation are thought to be the major problems in FXS, so interventions in both of these pathways will be critical for an overall treatment program. Ganaxolone is currently undergoing a clinical trial in FXS and is considered to have the best potential as a GABA agent because it specifically targets the GABAA pathway, which is most dysregulated in FXS. If efficacy in FXS is demonstrated and there is FDA approval for an FXS indication, then it will be studied in ASD and related disorders. Research needs to start focusing on multifaceted treatment options that combine multiple pharmacological agents and/or behavioral interventions due to the complex nature of the disease, but this may be difficult prior to FDA approval for each compound. Studies looking at behavioral and pharmacological interventions are planned for other targeted treatment options in FXS, including the mGluR5 antagonists and lovastatin. No studies are currently planned for multiple GABAergic medications or GABAergic medications with behavioral interventions, which would be highly useful and may provide more outcome measures with which to gauge treatment response.
In addition to difficulties in outcome measures, it should also be noted that reversing the behavioral and intellectual abilities in FXS is more difficult in adults because they are not typically in a learning program and because the neurobiological abnormalities may be less reversible over time. More intensive learning programs are required, although the improvements seen in the adult mouse with FXS after treatment with a long-acting mGluR5 antagonist were remarkableCitation78 and gave hope to many of the families that have adult offspring with FXS. Owing to the process involved in obtaining FDA approval for medications, companies must establish safety and efficacy in the adult population prior to moving into younger age groups; as such, the low efficacy of adult studies prevents the medication from moving to the younger age groups, who are more likely to see more robust treatment responses.
It is important to remember that synaptic connections that are strengthened by either a GABA agonist or an mGluR5 antagonist also require an intensive learning environment to strengthen these connections. Although most school-aged children with FXS are receiving special education support in addition to speech and language therapy and occupational therapy, their programs can usually be enhanced by the use of digital learning programs that can be accessed on a tablet device. There are a variety of software applications that have been developed for individuals with ASD, and these programs are likely to also be helpful for those with FXS.Citation79
There are many currently used medications that are helpful in FXS that will likely continue to be helpful even after GABA agonists and mGluR5 antagonists are more widely used clinically. These medications include sertraline, a selective serotonin reuptake inhibitor, that can be started at a young age and has been helpful in improving the language trajectory of toddlers with FXS.Citation80 Another targeted treatment that can be effective at an early age is minocycline, which is an antibiotic that lowers the level of matrix metalloproteinase 9 which is elevated in FXS.Citation81,Citation82 High levels of matrix metalloproteinase 9 interfere with the development of synaptic connections, and a controlled trial of minocycline in children between the ages of 3 and 17 years (doses ranging from 25 to 100 mg per day) recently demonstrated efficacy on the CGI-I in improving overall behavior and on the visual analog scale for improving mood and anxiety.Citation81 Side effects of minocycline include graying of the permanent teeth if given before 8 years of age, and graying or darkening of tissue such as in the gums and nail beds at any age. On rare occasions, minocycline can cause a lupus-like syndrome with a rash or swollen joints or pseudotumor cerebri leading to a severe headache; if these problems occur, minocycline should be discontinued immediately.Citation81 Once children with FXS reach 5 years of age, they usually have a positive response to a stimulant for their ADHD symptoms; for those who do not respond to a stimulant, then an alpha agonist such as guanfacine can be very helpful.Citation32 Lastly, melatonin has also been helpful for sleep disturbances in FXS, particularly in young children.Citation83 Overall, a GABA agonist will add significantly to the treatment regimen in children and adults with FXS, although we do not yet know if improvements will be seen only in behavior or if cognitive deficits will also improve with long-term use.
Acknowledgments
Funding for this chapter includes NICHD grant HD 036071, the Autism Research Training Program (MH073124), Department of Defense grant PR101054, support from the Health and Human Services Administration on Developmental Disabilities (grant 90DD05969), and the National Center for Advancing Translational Research (UL1 TR000002).
Disclosure
Dr Hagerman has received funding from Novartis Pharmaceuticals, F Hoffmann-La Roche, Seaside Therapeutics and Neuren Pharmaceuticals Limited to carry out treatment trials in fragile X syndrome and autism. She has also consulted with F Hoffmann-La Roche/Genentech, and Novartis Pharmaceuticals regarding treatment studies in fragile X syndrome. All authors have participated in clinical trials of ganaxolone and arbaclofen for fragile X syndrome.
References
- BelmonteMKBourgeronTFragile X syndrome and autism at the intersection of genetic and neural networksNat Neurosci20069101221122517001341
- BretherickKLFlukerMRRobinsonWPFMR1 repeat sizes in the gray zone and high end of the normal range are associated with premature ovarian failureHum Genet2005117437638216078053
- HagermanRHagermanPAdvances in clinical and molecular understanding of the FMR1 premutation and fragile X-associated tremor/ataxia syndromeLancet Neurol201312878679823867198
- BourgeoisJASeritanALCasillasEMLifetime prevalence of mood and anxiety disorders in fragile X premutation carriersJ Clin Psychiatry201172217518220816038
- WinarniTIChonchaiyaWSumekarTAImmune-mediated disorders among women carriers of fragile X premutation allelesAm J Med Genet A2012158a102473248122903889
- AuJAkinsRSBerkowitz-SutherlandLPrevalence and risk of migraine headaches in adult fragile X premutation carriersClin Genet201384654655123373759
- HamlinAASukharevDCamposLHypertension in FMR1 premutation males with and without fragile X-associated tremor/ataxia syndrome (FXTAS)Am J Med Genet A2012158A61304130922528549
- SullivanSDWeltCShermanSFMR1 and the continuum of primary ovarian insufficiencySemin Reprod Med2011290429930721969264
- CondeVPalomarFJLamaMJAbnormal GABA-mediated and cerebellar inhibition in women with the fragile X premutationJ Neurophysiol201310951315132223236003
- FarzinFPerryHHesslDAutism spectrum disorders and attention-deficit/hyperactivity disorder in boys with the fragile X premutationJ Dev Behav Pediatr200627Suppl 2S137S14416685180
- LeighMJSHagermanRJHesslDFragile X SyndromeHansenRLRogersSJAutism and Other Neurodevelopmental DisordersArlingtonAmerican Psychiatric Publishing20135776
- CoffeeBKeithKAlbizuaIIncidence of fragile X syndrome by newborn screening for methylated FMR1 DNAAm J Hum Genet200985450351419804849
- CrawfordDCAcuñaJMShermanSLFMR1 and the fragile X syndrome: human genome epidemiology reviewGenet Med20013535937111545690
- SorensenPLGaneLWYarboroughMHagermanRJTassoneFNewborn screening and cascade testing for FMR1 mutationsAm J Med Genet A20131611596923239591
- AllenEGHeWYadav-ShahMShermanSLA study of the distributional characteristics of FMR1 transcript levels in 238 individualsHum Genet2004114543944714758538
- LudwigALEspinalGMPrettoDICNS expression of murine fragile X protein (FMRP) as a function of CGG-repeat sizeHum Mol Genet Epub2112014
- BhakarALDölenGBearMFThe pathophysiology of fragile X (and what it teaches us about synapses)Annu Rev Neurosci20123541744322483044
- BrownVJinPCemanSMicroarray identification of FMRP-associated brain mRNAs and altered mRNA translational profiles in fragile X syndromeCell2001107447748711719188
- BearMFHuberKMWarrenSTThe mGluR theory of fragile X mental retardationTrends Neurosci200427737037715219735
- MoySSNadlerJJAdvances in behavioral genetics: mouse models of autismMol Psychiatry200813142617848915
- RubensteinJMerzenichMModel of autism: increased ratio of excitation/inhibition in key neural systemsGenes Brain Behav20032525526714606691
- BagniCTassoneFNeriGHagermanRFragile X syndrome: causes, diagnosis, mechanisms, and therapeuticsJ Clin Invest2012122124314432223202739
- FatemiSFolsomTRooneyRThurasPmRNA and protein expression for novel GABAA receptors θ and ρ2 are altered in schizophrenia and mood disorders; relevance to FMRP-mGluR5 signaling pathwayTransl Psychiatry201336e27123778581
- DölenGCarpenterRLOcainTDBearMFMechanism-based approaches to treating fragile XPharmacol Ther20101271789320303363
- Berry-KravisEKnoxAHerveyCTargeted treatments for fragile X syndromeJ Neurodev Disord20113319321021484200
- PadgettCLSlesingerPAGABAB receptor coupling to G-proteins and ion channelsAdv Pharmacol20105812314720655481
- FarrantMNusserZVariations on an inhibitory theme: phasic and tonic activation of GABA(A) receptorsNat Rev Neurosci20056321522915738957
- CardinJACarlénMMeletisKDriving fast-spiking cells induces gamma rhythm and controls sensory responsesNature2009459724766366719396156
- WangLWBerry-KravisEHagermanRJFragile X: leading the way for targeted treatments in autismNeurotherapeutics20107326427420643379
- SohalVSZhangFYizharODeisserothKParvalbumin neurons and gamma rhythms enhance cortical circuit performanceNature2009459724769870219396159
- Berry-KravisEGrossmanAWCrnicLSGreenoughWTUnderstanding fragile X syndromeCurrent Paediatrics2002124316324
- HagermanRJBerry-KravisEKaufmannWEAdvances in the treatment of fragile X syndromePediatrics2009123137839019117905
- AduseiDCPaceyLKChenDHampsonDREarly developmental alterations in GABAergic protein expression in fragile X knockout miceNeuropharmacology201059316717120470805
- LiaoCWLienCEstimating intracellular Ca2+ concentrations and buffering in a dendritic inhibitory hippocampal interneuronNeuroscience200916441701171119782725
- Olmos-SerranoJLPaluszkiewiczSMMartinBSKaufmannWECorbinJGHuntsmanMMDefective GABAergic neurotransmission and pharmacological rescue of neuronal hyperexcitability in the amygdala in a mouse model of fragile X syndromeJ Neurosci201030299929993820660275
- CuriaGPapouinTSéguélaPAvoliMDownregulation of tonic GABAergic inhibition in a mouse model of fragile X syndromeCereb Cortex20091971515152018787232
- D’HulstCHeulensIBrouwerJRExpression of the GABAergic system in animal models for fragile X syndrome and fragile X associated tremor/ataxia syndrome (FXTAS)Brain Res2009125317618319070606
- GantoisIVandesompeleJSpelemanFExpression profiling suggests underexpression of the GABAA receptor subunit delta in the fragile X knockout mouse modelNeurobiol Dis200621234635716199166
- PaceyLKKHeximerSPHampsonDRIncreased GABA(B) receptor-mediated signaling reduces the susceptibility of fragile x knockout mice to audiogenic seizuresMol Pharmacol2009761182419351745
- KimSYBurrisJBassalFFear-specific amygdala function in children and adolescents on the fragile x spectrum: a dosage response of the FMR1 geneCereb. Cortex201424360061323146966
- GibsonJRBartleyAFHaysSAHuberKMImbalance of neocortical excitation and inhibition and altered UP states reflect network hyperexcitability in the mouse model of fragile X syndromeJ Neurophysiol200810052615262618784272
- Berry-KravisEMHesslDRathmellBEffects of STX209 (arbaclofen) on neurobehavioral function in children and adults with fragile X syndrome: a randomized, controlled, phase 2 trialSci Transl Med20124152152ra127
- EricksonCAWengNWeilerIJOpen-label riluzole in fragile X syndromeBrain Res2011138026427021059347
- EricksonCAWinkLARayBImpact of acamprosate on behavior and brain-derived neurotrophic factor: an open-label study in youth with fragile X syndromePsychopharmacology (Berl)20132281758423436129
- CarterRBWoodPLWielandSCharacterization of the anticonvulsant properties of ganaxolone (CCD 1042; 3β-hydroxy-3β-methyl-5α-pregnan-20-one), a selective, high-affinity, steroid modulator of the γ-aminobutyric acidA receptorJ Pharmacol Exp Ther19972803128412959067315
- KerriganJFShieldsWDNelsonTYGanaxolone for treating intractable infantile spasms: a multicenter, open-label, add-on trialEpilepsy Res200042213313911074186
- HeulensID’HulstCVan DamDDe DeynPPKooyRFPharmacological treatment of fragile X syndrome with GABAergic drugs in a knockout mouse modelBehav Brain Res2012229124424922285772
- D’HulstCDe GeestNReeveSPDecreased expression of the GABAA receptor in fragile X syndromeBrain Res20061121123824517046729
- ChangSBraySMLiZIdentification of small molecules rescuing fragile X syndrome phenotypes in DrosophilaNat Chem Biol20084425626318327252
- PieriboneVATsaiJSouffletCClinical evaluation of ganaxolone in pediatric and adolescent patients with refractory epilepsyEpilepsia200748101870187417634060
- Marinus PharmaceuticalsGanaxolone Treatment in Children With Fragile X Syndrome Available from: http://clinicaltrials.gov/ct2/show/NCT01725152. NLM identifier: NCT01725152Accessed March 24, 2014
- NusserZModyISelective modulation of tonic and phasic inhibitions in dentate gyrus granule cellsJ Neurophysiol20028752624262811976398
- CopeDWHughesSWCrunelliVGABAA receptor-mediated tonic inhibition in thalamic neuronsJ Neurosci20052550115531156316354913
- BrownNKerbyJBonnertTWhitingPWaffordKPharmacological characterization of a novel cell line expressing human alpha(4)beta(3) delta GABA(A) receptorsBr J Pharmacol2002136796597412145096
- WohlfarthKMBianchiMTMacdonaldRLEnhanced neurosteroid potentiation of ternary GABA(A) receptors containing the delta subunitJ Neurosci20022251541154911880484
- HaasKFMacdonaldRLGABAA receptor subunit gamma2 and delta subtypes confer unique kinetic properties on recombinant GABAA receptor currents in mouse fibroblastsJ Physiol1999514Pt 127459831714
- DengPYRotmanZBlundonJAFMRP regulates neurotransmitter release and synaptic information transmission by modulating action potential duration via BK channelsNeuron201377469671123439122
- Olmos-SerranoJLCorbinJGBurnsMPThe GABA(A) receptor agonist THIP ameliorates specific behavioral deficits in the mouse model of fragile X syndromeDev Neurosci201133539540322067669
- EgawaKKitagawaKInoueKDecreased tonic inhibition in cerebellar granule cells causes motor dysfunction in a mouse model of angelman syndromeSci Transl Med20124163163ra157
- BrowneTRPharmacokinetics of antiepileptic drugsNeurology1998515 Suppl 4S2S79818917
- BrowneTSzaboGNew pharmacokinetic methods for the study of antiepileptic medications of the 1990sEpilepsia199032S66S731743172
- LindbergerMLuhrOJohannessenSILarssonSTomsonTSerum concentrations and effects of gabapentin and vigabatrin: observations from a dose titration studyTher Drug Monit200325445746212883229
- Podboraczynska-JodkoiKLubinskiWHampel-OsipowiczERetinal dysfunction in patients treated with vigabatrinKlin. Oczna20071091–38588 Polish17687922
- HendersonCWijetungeLKinoshitaMNReversal of disease-related pathologies in the fragile X mouse model by selective activation of GABAB receptors with arbaclofenSci Transl Med20124152152ra128
- Thomson ReutersKey trial of Seaside autism drug fails to show benefit [press release]New York, NYThomson Reuters201351 Available from: http://www.reuters.com/article/2013/05/01/us-autism-drug-idUSBRE9400NT20130501Accessed May 05, 2014
- SansoneSMWidamanKFHallSSPsychometric study of the Aberrant Behavior Checklist in Fragile X Syndrome and implications for targeted treatmentJ Autism Dev Disord20124271377139221972117
- HeYBenzAFuTNeuroprotective agent riluzole potentiates postsynaptic GABA(A) receptor functionNeuropharmacology200242219920911804616
- LeachJPBrodieMJNew antiepileptic drugs – an explosion of activitySeizure1995415177788108
- SuzdakPDJansenJAA review of the preclinical pharmacology of tiagabine: a potent and selective anticonvulsant GABA uptake inhibitorEpilepsia19953666126267555976
- NielsenEBSuzdakPDAndersenKEKnutsenLJSonnewaldUBraestrupCCharacterization of tiagabine (NO-328), a new potent and selective GABA uptake inhibitorEur J Pharmacol199119632572661832636
- Berry–KravisEEpilepsy in fragile X syndromeDev Med Child Neurol2002441172472812418611
- National Fragile X FoundationSeaside Therapeutics Announces End of Arbaclofen (STX209) Extension Study [press release]Walnut Creek, CANational Fragile X Foundation2013516 Available from: http://www.fragilex.org/2013/research/news-reports-and-commentaries/seaside-therapeutics-announces-end-of-arbaclofen-stx209-extension-study/Accessed May 06, 2014
- Berry-KravisEMechanism-based treatments in neurodevelopmental disorders: fragile X syndromePediatr Neurol201450429730224518745
- BraatSKooyRFFragile X syndrome neurobiology translates into rational therapyDrug Discovery Today201419451051924508819
- JacquemontSCurieAdes PortesVEpigenetic modification of the FMR1 gene in fragile X syndrome is associated with differential response to the mGluR5 antagonist AFQ056Sci Transl Med201136464ra1
- SchneiderALeighMJAdamsPElectrocortical changes associated with minocycline treatment in fragile X syndromeJ Psychopharmacol2013271095696323981511
- University of California Los AngelesTrial to evaluate the safety of Lovastatin in individuals with neurofibromatosis Type I (NF1) Available from: http://clinicaltrials.gov/show/NCT00352599. NLM identifier: NCT00352599Accessed May 26, 2014
- MichalonASidorovMBallardTMChronic pharmacological mGlu5 inhibition corrects fragile X in adult miceNeuron2012741495622500629
- ChenWMultitouch tabletop technology for people with autism spectrum disorder: a review of the literatureProcedia Comput Sci201214198207
- WinarniTISchneiderABorodyanskaraMHagermanRJEarly intervention combined with targeted treatment promotes cognitive and behavioral improvements in young children with fragile x syndromeCase Rep Genet2012201228081323074686
- LeighMJNguyenDVMuYA randomized double-blind, placebo-controlled trial of minocycline in children and adolescents with fragile x syndromeJ Dev Behav Pediatr201334314715523572165
- DziembowskaMPrettoDIJanuszAHigh MMP-9 activity levels in fragile X syndrome are lowered by minocyclineAm J Med Genet A2013161A81897190323824974
- WirojananJJacquemontSDiazRThe efficacy of melatonin for sleep problems in children with autism, fragile X syndrome, or autism and fragile X syndromeJ Clin Sleep Med20095214515019968048