
Abstract
Background
The multinational, open-label COMPLETE study (NCT03835715) investigated the effectiveness of vortioxetine in alleviating emotional blunting in patients with major depressive disorder (MDD) experiencing inadequate response and emotional blunting while being treated with a selective serotonin reuptake inhibitor (SSRI) or serotonin–noradrenaline reuptake inhibitor (SNRI). This paper presents results for the subgroup of patients enrolled in Spain.
Methods
Patients with MDD (n = 67) experiencing partial response and emotional blunting during monotherapy with an SSRI or SNRI were switched to vortioxetine (10–20 mg/day) for 8 weeks. The primary study outcome was emotional blunting, assessed by the Oxford Depression Questionnaire (ODQ).
Results
After 8 weeks of vortioxetine, the mean (SE) change in ODQ total score from baseline was −26.0 (2.9) (P < 0.001). Respective changes in Montgomery–Åsberg Depression Rating Scale (MADRS), Motivation and Energy Inventory, Digit Symbol Substitution Test, and Sheehan Disability Scale (SDS) total scores were −14.9 (0.8), +34.2 (4.5), +6.3 (1.6), and ‒9.0 (1.3) (all P < 0.001 vs baseline). At week 8, 70.4% of patients no longer reported emotional blunting and 53.7% had achieved remission from their depressive symptoms (defined as a MADRS total score ≤10). Mediation analysis showed 77.1% of the change in SDS total score to be a direct effect of the improvement in ODQ total score after switching to vortioxetine. Adverse events were reported by 35 patients (52.2%), most commonly nausea (14 patients, 20.9%). At week 8, 33/54 patients (61.1%) were receiving vortioxetine 20 mg/day.
Conclusion
In this study investigating the effectiveness of vortioxetine in Spanish patients with MDD who experienced inadequate response and emotional blunting on SSRI/SNRI monotherapy, significant improvements in emotional blunting, core depressive symptoms (including anhedonia), sleep duration, motivation and energy, cognitive performance, and overall patient functioning were observed during the 8 weeks of treatment. Two-thirds of patients no longer reported emotional blunting and over half were in remission from their depressive symptoms at week 8.
Introduction
In Spain, major depressive disorder (MDD) affects approximately 5% of the adult population annually,Citation1,Citation2 accounting for 424,436 years lived with disability in 2015.Citation1 The total annual societal cost of depressive disorders in the Spanish adult population was estimated to be €6145 million in 2017.Citation2 Selective serotonin reuptake inhibitors (SSRIs) and serotonin–noradrenaline reuptake inhibitors (SNRIs) are widely used for the treatment of MDD. However, approximately 50% of patients do not respond adequately to these therapies.Citation3 In addition, 40–60% of patients treated with either SSRIs or SNRIs experience emotional blunting (a debilitating functional syndrome sometimes termed “apathy syndrome”) as a side effect of their antidepressant medication.Citation4–12
Anhedonia, or the inability to anticipate and experience pleasure, is a key aspect of emotional blunting and a core symptom of MDD.Citation13 Emotional blunting is distinguished from anhedonia by flattening of negative as well as positive emotions and the lack of expected emotional responses to specific events or circumstances.Citation7 Patients experiencing emotional blunting may also report personality changes, reduced motivation, apathy, general indifference to people or things that should matter to them, and detrimental impacts on their judgement, ability to make decisions, and personal relationships.Citation4,Citation10,Citation12,Citation14
Emotional blunting is of clinical importance and a considerable burden for patients with MDD. A large online survey undertaken in Brazil, Canada, and Spain found emotional blunting to have a significant detrimental effect on daily functioning, well-being, and quality of life in patients with acute depression and those who had achieved remission.Citation15 Emotional blunting also frequently leads to discontinuation of antidepressant therapy. In the same survey, 45% of patients reported that their antidepressant medication affected their emotions, and 39% were considering stopping or reported that they had already stopped antidepressant use because of the emotional side effects experienced.Citation11 Similarly, another survey found that “blunted emotions” was a cause of treatment discontinuation in 35% of patients with MDD.Citation16 Greater recognition of the symptom and use of appropriate alternative antidepressants are required in patients experiencing emotional blunting during treatment with SSRIs or SNRIs in order to prevent discontinuation of antidepressant treatment resulting in an increased risk for relapse.
A recent systematic review found only limited data on the effectiveness of antidepressant therapy for the treatment of emotional blunting in patients with MDD.Citation12 However, this review omitted the results of the international COMPLETE study that demonstrated the effectiveness of the multimodal antidepressant vortioxetine for improving emotional blunting in patients with MDD experiencing an inadequate response and emotional blunting on SSRI/SNRI monotherapy.Citation17 Vortioxetine has demonstrated broad efficacy across the spectrum of symptoms experienced by patients with MDD,Citation18–26 including both anhedoniaCitation27 and emotional blunting.Citation17 As almost half (45%) of all patients participating in the COMPLETE study were enrolled in Spain,Citation17 it is of scientific interest to further explore the study findings in this large subgroup of patients.
Methods
Study Design and Participants
COMPLETE was an international, multicenter, open-label study conducted at 23 sites in France, Spain, Italy, and Lithuania between February 2019 and February 2020 (NCT03835715). The design and overall findings of the COMPLETE study have been reported in detail previously.Citation17 In brief, participants were adult outpatients (18–65 years) who had a primary diagnosis of MDD (Diagnostic and Statistical Manual of Mental Disorders, 5th edition criteria; duration of current depressive episode <12 months). Eligible patients were experiencing partial response to monotherapy with an SSRI or SNRI at an adequate dose for ≥6 weeks, a Montgomery–Åsberg Depression Rating Scale (MADRS) total score of >21 and <29 (ie moderate to severe depressive symptoms), and had emotional blunting, defined as an Oxford Depression Questionnaire (ODQ) total score of ≥50 and a response of “Yes” to the following standardized screening question:Citation28
Emotional effects vary, but may include, for example, feeling emotionally ‘numbed’ or ‘blunted’ in some way; lacking positive emotions or negative emotions; feeling detached from the world around you; or ‘just not caring’ about things that you used to care about. Have you experienced such emotional effects during the last 6 weeks?
Additionally, all patients were, in their own and the investigator’s opinion, suitable candidates for switching to another antidepressant. The key exclusion criteria were: an inadequate response to two or more previous courses of antidepressant therapy of adequate dosage and duration; any other current psychiatric diagnosis; a history of substance abuse within the previous 6 months; and a risk for suicide.Citation17
Patients were switched directly from SSRI/SNRI therapy and received treatment with vortioxetine for 8 weeks. All patients initiated treatment with vortioxetine at a dose of 10 mg/day for 1 week. After the first week of treatment, vortioxetine dosage could be adjusted between 10 and 20 mg/day at the investigator’s discretion. The standardized screening question on emotional blunting was repeated at the end of the 8 weeks of vortioxetine treatment.
Study Assessments
Patients were assessed at baseline and weeks 1, 4, and 8. The primary study outcome was emotional blunting, assessed using the ODQ.Citation28 The ODQ is a patient-reported questionnaire eliciting information concerning emotional experiences during the past week across five domains: general reduction in emotions, reduction in positive emotions, emotional detachment from others, not caring, and antidepressant as cause. The “antidepressant as cause” domain, which is only completed by patients receiving antidepressant therapy, explores the patient’s perception of any potential link between their current treatment for depression and their experience of emotional blunting. Each item is rated on a scale of 1 (disagree) to 5 (agree). The ODQ total score ranges from 26 to 130, with higher scores indicating more severe emotional symptoms. The suggested minimum clinically important difference for change from baseline in the ODQ total score after 8 weeks of antidepressant treatment is 20 points.Citation29
Overall severity of depressive symptoms was assessed using the clinician-reported MADRS total and individual item scores. Sleep was assessed using MADRS item 4; this item assesses the patient’s experience of reduced duration or depth of sleep compared with their normal sleep pattern. Severity of anhedonia was assessed using the MADRS 5-item anhedonia subscale score, comprising the sum of MADRS items 1 (apparent sadness), 2 (reported sadness),6 (concentration difficulty), 7 (lassitude), and 8 (inability to feel).Citation30 Overall disease severity and worsening/improvement during treatment were also assessed by means of the Clinical Global Impressions–Severity of Illness (CGI-S) and CGI–Improvement (CGI-I) scales.
Motivation and energy were assessed using the Motivation and Energy Inventory (MEI), a patient-reported outcome for evaluation of the impact of motivation and energy levels over the past 4 weeks on their ability to perform daily activities and engage in social interactions.Citation31 Questions cover three domains: mental/cognitive energy, social motivation, and physical energy. The MEI total score ranges from 0 to 144 points, with higher scores indicating higher levels of motivation and energy. The suggested minimum clinically important difference for change in MEI total score from baseline after 8 weeks of antidepressant treatment is 15 points.Citation32
Patient functioning was assessed using the Sheehan Disability Scale (SDS).Citation33,Citation34 This brief self-reported scale assesses the severity of depression-associated functional impairment experienced by the patient over the past 7 days across three domains: work/school, social life/leisure, and family life/home responsibilities. Domain scores range from 0 (unimpaired) to 10 (highly impaired) and the SDS total score ranges from 0 to 30, with higher scores indicating greater impairment. A change in SDS total score of ≥4 points is considered meaningful for patients.Citation34 The SDS also reports on the number of underproductive and lost work days during the preceding week. Cognitive functioning was assessed using the Digit Symbol Substitution Test (DSST).
Treatment-emergent adverse events (TEAEs) were recorded using Medical Dictionary for Regulatory Activities (MedDRA) version 14.0 preferred terms. After recording of TEAEs at baseline and at week 1, discontinuation-emergent events were also evaluated using the Discontinuation-Emergent Signs and Symptoms (DESS) scale. This 43-item clinician-rated checklist is designed to evaluate symptoms that may be associated with discontinuation of antidepressant therapy, such as agitation, insomnia, fatigue, and dizziness.Citation35 The DESS total score represents the total number of discontinuation-emergent events (either reported for the first time or worsening events if previously reported); higher scores indicate more pronounced discontinuation symptoms.
Statistical Analysis
This was a subgroup analysis of patients enrolled in Spain. Effectiveness was analyzed in all eligible patients who received at least one dose of vortioxetine and had a minimum of one valid post-baseline ODQ assessment (full analysis set). Analyses were conducted on observed cases and missing data were not replaced. Safety was analyzed in all patients who received at least one dose of vortioxetine (all patients treated set).
Continuous effectiveness endpoints (including all individual MADRS items) were analyzed using a mixed model for repeated measures, including site and analysis timepoint (week) as fixed effects, the relevant baseline score as a continuous covariate (except for the analysis of CGI-I, for which baseline CGI-S score was used in the model), and the baseline score-by-week interaction, based on all available observations. Missing SDS work/school domain scores were imputed for the calculation of the total score as the mean of the social life/leisure and family life/home responsibilities domain scores.Citation21 To assess the change from baseline in ODQ total score that was not explained by the corresponding change in MADRS total score, the primary analysis was repeated with the additional inclusion of baseline MADRS total score and change from baseline as covariates, and with/without adjustment for change in MADRS total score.
The proportions of patients who achieved MADRS response and remission were also calculated. Response was defined as ≥50% reduction in MADRS total score from baseline, with remission defined as a MADRS total score of ≤10.
Partial correlation analyses were performed to investigate the relationship between change from baseline to week 8 in ODQ total score and MEI and SDS total scores. Pairwise associations were described using partial correlation coefficients that controlled for site and baseline scores. To assess the extent to which these associations might be explained by improvement in MADRS total score from baseline, analyses were repeated with removal of the effects of MADRS total score at baseline and change from baseline to week 8.
A mediation analysis was undertaken to estimate the extent to which the change in MADRS total score mediated the change from baseline to week 8 in SDS total score explained by the change in ODQ total score. Three models were fitted in the analysis: (i) estimating the total effect of the change in ODQ total score on the change in SDS total score; (ii) confirming a relationship (total effect) between ODQ and MADRS total scores; and (iii) estimating the direct and indirect (mediated) effects of ODQ total score and MADRS total score, respectively, on SDS total score. All models included site and SDS, ODQ, and MADRS total scores at baseline.
Safety endpoints were summarized descriptively. All statistical analyses were performed using SAS statistical software (version 9.4 or later). Reported P-values are nominal and multiplicity was not controlled; significance was set at P < 0.05.
Results
Patient Characteristics
A total of 68 patients were enrolled at seven psychiatric outpatient sites in Spain, 67 of whom received at least one dose of study medication (all patients treated set). Of these, 62 patients were eligible for inclusion in the full analysis set. Fifty-four patients completed the study. Primary reasons for withdrawal from the study were adverse events (4 patients, 6.0%), protocol violation (3 patients, 4.5%), lost to follow-up (3 patients, 4.5%), withdrawal of consent (1 patient, 1.5%), lack of efficacy (1 patient, 1.5%), and other (1 patient, 1.5%).
Baseline demographics and clinical characteristics are shown in . No clinically relevant differences were seen compared with the overall COMPLETE study population (data not shown). Patients enrolled in Spain were mostly female (64.2%), with a mean (SD) age of 47.2 (10.5) years. Mean (SD) duration of the current depressive episode was 20.6 (11.8) weeks. Most patients (51 patients, 76.1%) were switching to vortioxetine from an SSRI, most commonly escitalopram (29 patients, 43.3%).
Table 1 Baseline Demographics and Clinical Characteristics
Per protocol, all patients reported experiencing emotional blunting at baseline. The mean (SD) ODQ total score was 87.6 (15.6), indicating a population with moderately severe emotional blunting. Mean (SD) baseline MADRS total score and CGI-S score at baseline were 25.6 (1.6) and 4.4 (0.5), respectively, indicative of moderate to severe depression. Mean (SD) SDS total score at baseline was 20.0 (4.9), implying severely impaired patient functioning.
Vortioxetine Dosing
All patients initiated vortioxetine at a dose of 10 mg/day. After 1 week, the vortioxetine dosage was increased to 20 mg/day in 23 (37.1%) of the 62 patients included in the full analysis set. At week 4, 18 of these 23 patients remained on vortioxetine 20 mg/day, three had had their dose reduced to 10 mg/day, and two had withdrawn from the study. At this visit, the vortioxetine dose was increased from 10 to 20 mg/day in a further 17 patients. Of the 54 patients who completed the study, 33 (61.1%) were receiving vortioxetine 20 mg/day at week 8.
Effectiveness
Emotional Blunting
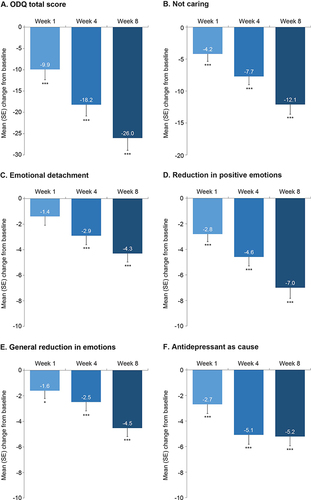
A rapid and sustained reduction in the severity of emotional blunting was seen over the 8 weeks of vortioxetine treatment ( and ). Mean (SE) change in ODQ total score from baseline was −9.9 (2.4) after 1 week of vortioxetine treatment, increasing to −18.2 (2.7) after 4 weeks and −26.0 (2.9) after 8 weeks (all P ≤ 0.0001 vs baseline). Significant improvements were seen across all ODQ domains, with mean (SE) change from baseline at week 8 ranging from −4.3 (0.7) for the emotional detachment domain to −12.1 (1.5) for the not caring domain (P < 0.001 for change from baseline at week 8 for all ODQ domains). At week 8, 38/54 (70.4%) patients who responded to the ODQ screening question reported that they were no longer experiencing emotional blunting.
Table 2 Effect of Vortioxetine on Emotional Blunting, Depressive Symptoms, Anhedonia, Motivation and Energy, and Overall Patient Functioning (FAS, MMRM)
Figure 1 Mean (SE) change from baseline over the 8 weeks of vortioxetine treatment for (A) ODQ total score and (B–F) ODQ domain scores: (B) not caring, (C) emotional detachment, (D) reduction in positive emotions, (E) general reduction in emotions, and (F) antidepressant as cause (FAS, MMRM analysis).
Repeating the primary analysis with additional correction for MADRS total score at baseline and change from baseline in MADRS total score showed that only 16.6% of the total variation in change in ODQ total score from baseline to week 8 could be explained by the corresponding change in MADRS total score.
Other Clinical Assessments
Statistically significant improvements in the severity of core depressive symptoms (including anhedonia), motivation and energy, cognitive performance, and patient functioning were also seen over the 8 weeks of vortioxetine treatment (). The mean (SE) reduction in MADRS total score from baseline was −3.1 (0.6) after 1 week of vortioxetine treatment, −9.5 (0.7) after 4 weeks, and −14.9 (0.8) after 8 weeks (all P < 0.001 vs baseline). The mean MADRS anhedonia subscale score also improved significantly from week 1 onwards (P < 0.001 vs baseline at all timepoints). As shown in , improvements were seen from week 1 onwards for all individual MADRS item scores (P < 0.001 vs baseline for all items at week 8). The mean (SE) reduction in the MADRS sleep item score from baseline was −0.28 (0.14) after 1 week of vortioxetine treatment, −0.76 (0.14) after 4 weeks, and −1.24 (0.15) after 8 weeks (P = 0.052 at week 1 and P < 0.001 vs baseline at weeks 4 and 8). At week 8, 36/54 (66.7%) patients had achieved a MADRS response (ie ≥50% reduction in MADRS total score from baseline), and 29/54 (53.7%) had achieved remission (ie MADRS total score ≤10).
Table 3 Change from Baseline in Individual MADRS Item Scores Over the 8 Weeks of Vortioxetine Treatment (FAS, MMRM)
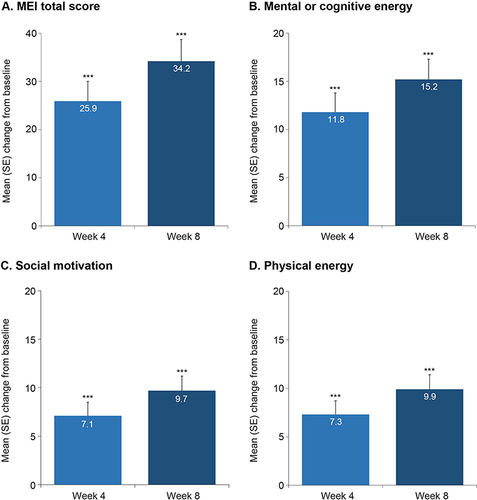
Significant improvements in overall disease severity were observed, as assessed by CGI-S and CGI-I scores (). Substantial and significant improvements in levels of motivation and energy assessed using the MEI were seen from week 4 onwards (ie the first post-baseline MEI assessment) (). The mean (SE) increase in MEI total score from baseline after 8 weeks of vortioxetine treatment was 34.2 (4.5) points (P < 0.001). Significant improvements were also seen across all MEI domains (). Significant improvement in cognitive performance, as assessed using the DSST, was seen after 1 week of vortioxetine treatment (mean [SE] change from baseline, 3.3 [1.5]; P < 0.05) and this was further improved at week 8 (mean [SE] change from baseline, 6.3 [1.6]; P < 0.001).
Figure 2 Mean (SE) change from baseline over the 8 weeks of vortioxetine treatment for (A) MEI total score and (B–D) MEI domain scores: (B) MEI mental or cognitive energy, (C) social motivation, and (D) physical energy (FAS, MMRM analysis).
A clinically relevant improvement in overall patient functioning, as assessed by SDS total score, was seen after 8 weeks of vortioxetine treatment (mean [SE] change from baseline, −9.0 [1.3]; P < 0.001), with significant improvements seen across all SDS domains (). Significant reductions in the number of working days lost to absenteeism (work days lost) and presenteeism (work days underproductive) were also seen after 8 weeks of vortioxetine treatment (both P < 0.001): at week 8, the mean (SE) reduction from baseline over the past 7 days in work days lost was −2.0 (0.2) days and in work days underproductive was −2.5 (0.4) days.
Partial Correlation Analyses
Results of the partial correlation analyses are shown in . In the unadjusted analysis, a strong negative correlation was seen for the change from baseline to week 8 in ODQ total score and MEI total score (r = −0.779; P < 0.001). A strong positive correlation was seen between the change from baseline to week 8 in ODQ and SDS total score (r = 0.725; P < 0.001). Strong positive correlations were also seen for the improvement in ODQ total score and all SDS domain scores (r values ranging from 0.684 for the SDS social life/leisure score to 0.809 for the SDS work/school score; P < 0.001 for all domains). All associations remained moderately strong after adjustment for improvement in MADRS total score ().
Table 4 Partial Correlation Analysis of Improvements in Emotional Blunting with Motivation and Energy, and Patient Functioning After 8 Weeks of Vortioxetine Treatment, Unadjusted and Adjusted for Depressive Symptom Severity
Mediation Analysis
Results of the mediation analysis showed that 77.1% of the change in SDS total score was a direct effect of the improvement in ODQ total score after switching to vortioxetine (ie it could be explained by the change in ODQ total score from baseline and not by the change in MADRS total score, which accounted for 22.9% of the effect on SDS total score).
Safety
A total of 35 patients (52.2%) reported at least one TEAE during the 8 weeks of vortioxetine treatment (). The most common TEAE was nausea, which was reported by 14 patients (20.9%). Other common TEAEs (ie reported by >5% of patients) were dizziness, headache, pruritus, diarrhea, and vomiting. Insomnia was reported as a TEAE by only one patient. No serious TEAEs were reported. Four patients withdrew from the study due to TEAEs. The only TEAEs leading to withdrawal in more than one patient were nausea and vomiting (each in two patients). Mean (SD) DESS total score was 2.0 (3.5) at baseline and 2.6 (4.6) at week 1.
Table 5 Summary of TEAEs Reported Over the8 Weeks of Vortioxetine Treatment
Discussion
COMPLETE was the first study of antidepressant therapy in patients with MDD to include longitudinal assessment of emotional blunting as a primary prespecified endpoint.Citation17 In this large subgroup of patients enrolled in Spain, clinically relevant and statistically significant improvements in emotional blunting, anhedonia, depressive symptoms, duration or depth of sleep, motivation and energy, cognitive performance, patient functioning, and measures of work productivity were seen during treatment with vortioxetine 10–20 mg/day. At week 8, almost two-thirds (61%) of patients were receiving the maximum vortioxetine dosage of 20 mg/day.
The observed mean improvements in ODQ and MEI total scores over the 8-week study period were similar to those seen in the overall study population,Citation17 and exceeded the minimum clinically important differences for change from baseline after 8 weeks of antidepressant treatment of 20 and 15 points, respectively.Citation29,Citation32 After 8 weeks of vortioxetine treatment, 70% of patients reported that they were no longer experiencing emotional blunting. This is substantially higher than the 50% observed in the overall population of patients participating in the COMPLETE study.Citation17 This may at least in part be due to the fact that a greater proportion of patients enrolled in Spain were receiving the maximum vortioxetine dosage of 20 mg/day (61% vs 51% in the overall study population). Vortioxetine has been shown to have dose-dependent efficacy across a broad range of symptoms experienced by patients with MDD, including anhedonia, with the greatest therapeutic benefits seen in patients receiving vortioxetine 20 mg/day.Citation17–27
Although the observed improvement in core depressive symptoms was very similar to that reported in the overall study population,Citation17 the proportion of the total variation in change in ODQ total score from baseline to week 8 that could be explained by the corresponding change in MADRS total score was lower in this analysis (17% vs 23% in the overall analysis). After 8 weeks of treatment with vortioxetine, two-thirds of patients (67%) had achieved a ≥50% reduction in MADRS total score from baseline and over half (54%) were in remission (defined as MADRS total score ≤10). This is slightly higher than the corresponding rates of MADRS response and remission in the overall study population (62% and 47%, respectively).Citation17 Statistically significant improvements were seen for the MADRS anhedonia subscore and across all individual MADRS item scores over the 8 weeks of treatment, demonstrating that patients who received vortioxetine in the study experienced significant improvements across the spectrum of their core depressive symptoms.
The significant improvement in the MADRS sleep item score is of particular interest, as many antidepressants are associated with adverse effects on sleep.Citation36,Citation37 For example, in a recent study, insomnia was found to be one of the most common reasons for treatment discontinuation in patients receiving SSRIs.Citation38 Available data suggest that rates of treatment-emergent insomnia are lower in patients treated with vortioxetine than in those receiving SSRIs and SNRIs.Citation36,Citation37 In a meta-analysis of TEAEs in 11 short-term, randomized, double-blind, placebo-controlled studies of vortioxetine 5–20 mg/day in patients with MDD, the incidence of insomnia was 2.0–5.1% for vortioxetine versus 4.0% for placebo.Citation39 Significant improvements in sleep were seen in patients with MDD receiving treatment with vortioxetine 10–20 mg/day in another open-label 8-week trial, with improved sleep significantly associated with the observed reduction in depressive symptom severity.Citation40 In that study, the proportion of patients with insomnia decreased by approximately 50% over the 8 weeks of follow-up. Results of another observational study found the benefits of vortioxetine on sleep quality and depressive symptoms to be maintained during longer-term therapy.Citation41 Of note, in the present analysis, insomnia was reported as a TEAE in only one patient.
Marked improvement in patient functioning assessed by the SDS was seen over the 8 weeks of vortioxetine treatment. The mean change in SDS total score from baseline was –9 points, which is substantially greater than the reduction of≥4 points that is considered meaningful for patients.Citation34 Significant reductions in the levels of absenteeism (work days lost) and presenteeism (work days underproductive) were also reported. The improvement in emotional blunting was found to be strongly and positively correlated with overall functioning and patients’ motivation and energy levels, even after adjusting for the severity of depressive symptoms. Mediation analysis suggested that more than 75% of the observed improvement in overall patient functioning was directly related to the effect of vortioxetine on emotional blunting; this is higher than reported in the overall study population (63%).Citation17
Treatment with vortioxetine was well tolerated, with no clinically relevant increase in DESS score after switching from SSRI/SNRI therapy. Consistent with reports from randomized controlled clinical trials of vortioxetine,Citation39 nausea was the most common TEAE, occurring in approximately 20% of patients over the 8-week study period. However, only two patients withdrew from treatment due to nausea and no serious TEAEs were reported. Clinical experience has shown that any nausea experienced when initiating vortioxetine mostly occurs during the first week of treatment, tends to be transient, and rarely leads to treatment withdrawal.Citation26
No TEAEs related to sexual dysfunction were reported. Sexual dysfunction is common in patients with MDD and is also frequently reported as a TEAE in patients receiving SSRIs and SNRIs.Citation42–44 In pivotal short-term randomized controlled clinical trials in patients with MDD, rates of treatment-emergent sexual dysfunction in vortioxetine-treated patients were similar to those seen in patients who received placebo.Citation39,Citation45 In patients with MDD and an inadequate response to first-line SSRI therapy, significantly greater improvement in sexual relationships (assessed using the Functioning Assessment Short Test) was seen over the 8 weeks of treatment in patients who switched to vortioxetine compared with those who received desvenlafaxine.Citation46 Other studies have also demonstrated a significant improvement in sexual function in patients switching to vortioxetine after experiencing SSRI-induced sexual dysfunction.Citation47–49
Our findings are consistent with those of studies undertaken to assess the effect of vortioxetine on anhedonia in patients with MDD. In short-term placebo-controlled studies, significant dose-dependent improvements in symptoms of anhedonia assessed by both the Snaith–Hamilton Pleasure Scale total score and the MADRS anhedonia subscale score were reported in patients with MDD treated with vortioxetine for 8 weeks.Citation27,Citation30,Citation50 The effects of vortioxetine on anhedonia were shown to be dose-dependent, with the greatest benefits achieved at a dose of 20 mg/day.Citation27 Post-hoc analysis of the results of a 12-week study in patients with MDD experiencing an inadequate response to SSRI/SNRI monotherapy also demonstrated significantly greater improvements in symptoms of anhedonia following a switch to vortioxetine 10–20 mg/day compared with agomelatine 25–50 mg/day.Citation27 The beneficial effects of vortioxetine on anhedonia in patients with MDD have been shown to be sustained during longer-term treatment. In a post-hoc analysis of two open-label extension studies, the mean reduction in MADRS anhedonia subscale score over 52 weeks of vortioxetine treatment was 3 points in patients receiving vortioxetine 5–10 mg/day and 6 points in those receiving vortioxetine 15–20 mg/day.Citation51
Both anhedonia and emotional blunting have a significant negative impact on functioning in patients with MDD, even when they are deemed to be in remission from their depressive symptoms.Citation15 The current study showed that the subgroup of patients enrolled in Spain had moderately severe emotional blunting and severely impaired patient functioning at baseline. A previously conducted online survey also noted severe emotional blunting and functional impairment in patients in Spain who were diagnosed with depression and were being treated with SSRIs or SNRIs; functional impairments were most notably in “interpersonal relationships”, “cognitive functioning”, and “occupational functioning”.Citation15 Functional impairment may persist after resolution of other symptoms in patients with MDD and has been shown to be a predictor of relapse.Citation52–54 As such, improvement in functioning is a key treatment goal in patients with MDD.Citation55–57 The association observed in the current analysis between improvements in emotional blunting and patient functioning provides further evidence of the need to specifically address emotional blunting in patients with MDD to improve antidepressant treatment outcomes.
Although many antidepressants may help relieve anhedonia in patients with MDD,Citation58 some—notably SSRIs—may also cause emotional blunting.Citation7 Central dopaminergic, mesolimbic, and mesocortical reward pathways are implicated in the development of anhedonia,Citation59,Citation60 while emotional blunting appears to be a consequence of reduced dopaminergic or glutamatergic activity in the prefrontal cortex.Citation5,Citation61
The positive effects of vortioxetine across a wide range of symptoms in MDD, including both anhedonia and emotional blunting, are likely due to its multimodal mechanism of action.Citation62,Citation63 As well as inhibiting the serotonin (5-HT) transporter, vortioxetine has 5-HT1D, 5-HT3, and 5-HT7 receptor antagonist, 5-HT1B receptor partial agonist, and 5-HT1A receptor agonist activity.Citation63–65 Vortioxetine therefore directly and indirectly modulates not only the activity of the serotonergic system, but also the downstream release of other neurotransmitters, including dopamine, acetylcholine, histamine, gamma-aminobutyric acid (GABA), and glutamate.Citation63,Citation66,Citation67 Thus, the beneficial effects of vortioxetine on emotional blunting may be mediated via direct and indirect effects on serotonergic and other neurotransmitter systems, including downstream effects on dopaminergic neurotransmission, modulation of serotonin neuronal connections of glutamate and GABA neurons to the prefrontal cortex and hippocampus, and effects on glutamatergic pyramidal neurons and GABAergic interneurons in the prefrontal cortex and hippocampus.Citation63,Citation66,Citation67 The antagonistic properties of vortioxetine on 5-HT3 receptors may contribute to its favorable effect on sleep architecture compared with SSRIs.Citation68,Citation69
The main limitation of this study is the lack of a placebo or active-comparator arm and the relatively short duration of follow-up. It should also be noted that the COMPLETE study was not specifically powered for this subgroup analysis in patients enrolled in Spain; however, almost half (45%) of all patients participating in the COMPLETE study were enrolled in Spain.
Conclusions
In summary, in patients with an inadequate response and emotional blunting during prior SSRI/SNRI therapy recruited in Spain as part of the COMPLETE study, significant and clinically relevant improvements in emotional blunting, core depressive symptoms (including anhedonia), duration and/or depth of sleep, motivation and energy, cognitive performance, patient functioning, and measures of work productivity were achieved after 8 weeks of vortioxetine treatment. The observed improvement in emotional blunting was directly associated with better patient functioning, independent of the effect of treatment on core depressive symptoms. After 8 weeks of vortioxetine treatment, over two-thirds of patients were no longer experiencing emotional blunting and over half were in remission from their depressive symptoms.
Abbreviations
5-HT, serotonin; CGI-I, Clinical Global Impressions–Improvement; CGI-S, Clinical Global Impressions–Severity of Illness; DESS, Discontinuation-Emergent Signs and Symptoms scale; DSST, Digit Symbol Substitution Test; GABA, gamma-aminobutyric acid; MADRS, Montgomery–Åsberg Depression Rating Scale; MDD, major depressive disorder; MEI, Motivation and Energy Inventory; ODQ, Oxford Depression Questionnaire; SD, standard deviation; SDS, Sheehan Disability Scale; SE, standard error; SNRI, serotonin–noradrenaline reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; TEAE, treatment-emergent adverse event.
Ethics Approval and Informed Consent
The COMPLETE study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines and was approved by the Drug Research Ethics Committee (Comité de Ética de la Investigación con Medicamentos) of the Hospital Universitario La Paz, Madrid. Written informed consent was obtained from all patients prior to study participation.
Consent for Publication
As this manuscript does not contain patient-sensitive material, consent is not required.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
MCC and HL are employees of H. Lundbeck A/S. FC has received consultancy fees or honoraria/research grants in the last 5 years from Exeltis, IdISBa, Janssen Cilag, Lundbeck, Otsuka, Pfizer Angelini, Servier. ALM has received consultancy fees or honoraria/research grants in the last 5 years from Boehringer Ingelheim, Casen Recordati, Eli Lilly, Forum Pharmaceuticals, Instituto de Salud Carlos III, Janssen Cilag, Lundbeck, Otsuka, Pfizer, Roche, ROVI, Servier, and the Junta de Castilla y León. The authors report no other conflicts of interest in this work.
Acknowledgments
The authors would like to thank the following investigators at the COMPLETE study sites in Spain: Salvador Ros Montalbán (Instituto Internacional de Neurociencias Aplicadas, Hospital Plató 21, Barcelona), Manuel Riobo Fernandez (Centro de Especialidades a Doblada, Vigo), Francisco Montañés Rada (Hospital Universitario Fundación Alcorcón, Madrid), Gabriel Selva Vera (Centro de Salud Mental de Foios, Valencia), and Julio Bobes García (Universidad de Oviedo, Oviedo). The overall findings of the COMPLETE study have been published previously (Fagiolini A et al. J Affect Disord. 2021;283:472–479).
Data Sharing Statement
Please visit www.lundbeck.com for more information about our clinical data sharing policy and processes.
Additional information
Funding
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. Geneva: World Health Organization; 2017. Available from: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf. Accessed February 22, 2023.
- Vieta E, Alonso J, Pérez-Sola V, et al. Epidemiology and costs of depressive disorder in Spain: the EPICO study. Eur Neuropsychopharm. 2021;50:93–103. doi:10.1016/j.euroneuro.2021.04.022
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. 2006;163(11):1905–1917. doi:10.1176/ajp.2006.163.11.1905
- Price J, Cole V, Goodwin GM. Emotional side-effects of selective serotonin reuptake inhibitors: qualitative study. Br J Psychiatry. 2009;195(3):211–217. doi:10.1192/bjp.bp.108.051110
- Sansone RA, Sansone LA. SSRI-induced indifference. Psychiatry. 2010;7(10):14–18.
- Read J, Cartwright C, Gibson K. Adverse emotional and interpersonal effects reported by 1829 New Zealanders while taking antidepressants. Psychiatry Res. 2014;216(1):67–73. doi:10.1016/j.psychres.2014.01.042
- Goodwin GM, Price J, De Bodinat C, Laredo J. Emotional blunting with antidepressant treatments: a survey among depressed patients. J Affect Disord. 2017;221:31–35. doi:10.1016/j.jad.2017.05.048
- Read J, Williams J. Adverse effects of antidepressants reported by a large international cohort: emotional blunting, suicidality, and withdrawal effects. Curr Drug Saf. 2018;13(3):176–186. doi:10.2174/1574886313666180605095130
- Marazziti D, Mucci F, Tripodi B, et al. Emotional blunting, cognitive impairment, bone fractures, and bleeding as possible side effects of long-term use of SSRIs. Clin Neuropsychiatry. 2019;16(2):75–85.
- Padala PR, Padala KP, Majagi AS, Garner KK, Dennis RA, Sullivan DH. Selective serotonin reuptake inhibitors-associated apathy syndrome: a cross sectional study. Medicine. 2020;99(33):e21497. doi:10.1097/MD.0000000000021497
- Christensen MC, Ren H, Fagiolini A. Emotional blunting in patients with depression. Part I: clinical characteristics. Ann Gen Psychiatry. 2022;21(1):10. doi:10.1186/s12991-022-00387-1
- Masdrakis VG, Markianos M, Baldwin DS. Apathy associated with antidepressant drugs: a systematic review. Acta Neuropsychiatr. 2023;35(4):189–204. doi:10.1017/neu.2023.6
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed., text revision. Washington, DC: American Psychiatric Association; 2022.
- Sandell K, Bornäs H. Functioning numbness instead of feelings as a direction: young adults’ experiences of antidepressant use. Sociology. 2017;51(3):543–558. doi:10.1177/0038038515591947
- Christensen MC, Ren H, Fagiolini A. Emotional blunting in patients with depression. Part II: relationship with functioning, well-being, and quality of life. Ann Gen Psychiatry. 2022;21(1):20. doi:10.1186/s12991-022-00392-4
- Rosenblat JD, Simon GE, Sachs GS, et al. Treatment effectiveness and tolerability outcomes that are most important to individuals with bipolar and unipolar depression. J Affect Disord. 2019;243:116–120. doi:10.1016/j.jad.2018.09.027
- Fagiolini A, Florea I, Loft H, Christensen MC. Effectiveness of vortioxetine on emotional blunting in patients with major depressive disorder with inadequate response to SSRI/SNRI treatment. J Affect Disord. 2021;283:472–479. doi:10.1016/j.jad.2020.11.106
- Thase ME, Mahableshwarkar AR, Dragheim M, Loft H, Vieta E. A meta-analysis of randomized, placebo-controlled trials of vortioxetine for the treatment of major depressive disorder in adults. Eur Neuropsychopharmacol. 2016;26(6):979–993. doi:10.1016/j.euroneuro.2016.03.007
- Baldwin DS, Florea I, Jacobsen PL, Zhong W, Nomikos GG. A meta-analysis of the efficacy of vortioxetine in patients with major depressive disorder (MDD) and high levels of anxiety symptoms. J Affect Disord. 2016;206:140–150. doi:10.1016/j.jad.2016.07.015
- McIntyre RS, Harrison J, Loft H, Jacobson W, Olsen CK. The effects of vortioxetine on cognitive function in patients with major depressive disorder: a meta-analysis of three randomized controlled trials. Int J Neuropsychopharmacol. 2016;19(10):pyw055. doi:10.1093/ijnp/pyw055
- Florea I, Loft H, Danchenko N, et al. The effect of vortioxetine on overall patient functioning in patients with major depressive disorder. Brain Behav. 2017;7(3):e00622. doi:10.1002/brb3.622
- Christensen MC, Florea I, Lindsten A, Baldwin DS. Efficacy of vortioxetine on the physical symptoms of major depressive disorder. J Psychopharmacol. 2018;32(10):1086–1097. doi:10.1177/0269881118788826
- Iovieno N, Papakostas GI, Feeney A, et al. Vortioxetine versus placebo for major depressive disorder: a comprehensive analysis of the clinical trial dataset. J Clin Psychiatry. 2021;82(4):20r13682. doi:10.4088/JCP.20r13682
- Adair M, Christensen MC, Florea I, Loft H, Fagiolini A. Vortioxetine in patients with major depressive disorder and high levels of anxiety symptoms: an updated analysis of efficacy and tolerability. J Affect Disord. 2023;328:345–354. doi:10.1016/j.jad.2023.01.074
- Christensen MC, McIntyre RS, Florea I, Loft H, Fagiolini A. Vortioxetine 20 mg/day in patients with major depressive disorder: updated analysis of efficacy, safety, and optimal timing of dose adjustment. CNS Spectr. 2023;28(1):90–97. doi:10.1017/S1092852921000936
- Christensen MC, McIntyre RS, Adair M, Florea I, Loft H, Fagiolini A. Clinical benefits of vortioxetine 20 mg/day in patients with major depressive disorder. CNS Spectr. 2023;28(6):693–701. doi:10.1017/S1092852923002249
- McIntyre RS, Loft H, Christensen MC. Efficacy of vortioxetine on anhedonia: results from a pooled analysis of short-term studies in patients with major depressive disorder. Neuropsychiatr Dis Treat. 2021;17:575–585. doi:10.2147/NDT.S296451
- Price J, Cole V, Doll H, Goodwin GM. The Oxford Questionnaire on the Emotional Side-effects of Antidepressants (OQuESA): development, validity, reliability and sensitivity to change. J Affect Disord. 2012;140(1):66–74. doi:10.1016/j.jad.2012.01.030
- Christensen MC, Fagiolini A, Florea I, Loft H, Cuomo A, Goodwin GM. Validation of the Oxford Depression Questionnaire: sensitivity to change, minimal clinically important difference, and response threshold for the assessment of emotional blunting. J Affect Disord. 2021;294:924–931. doi:10.1016/j.jad.2021.07.099
- Cao B, Park C, Subramaniapillai M, et al. The efficacy of vortioxetine on anhedonia in patients with major depressive disorder. Front Psychiatry. 2019;10:17. doi:10.3389/fpsyt.2019.00017
- Fehnel SE, Bann CM, Hogue SL, Kwong WJ, Mahajan SS. The development and psychometric evaluation of the Motivation and Energy Inventory (MEI). Qual Life Res. 2004;13(7):1321–1336. doi:10.1023/B:QURE.0000037502.64077.4d
- Christensen MC, Adair M, Loft H, McIntyre RS. The Motivation and Energy Inventory (MEI): analysis of the clinically relevant response threshold in patients with major depressive disorder and emotional blunting using data from the COMPLETE study. J Affect Disord. 2023;323:547–553. doi:10.1016/j.jad.2022.11.033
- Sheehan DV, Harnett-Sheehan K, Raj BA. The measurement of disability. Int Clin Psychopharmacol. 1996;11(Suppl 3):89–95. doi:10.1097/00004850-199606003-00015
- Sheehan KH, Sheehan DV. Assessing treatment effects in clinical trials with the discan metric of the Sheehan Disability Scale. Int Clin Psychopharmacol. 2008;23(2):70–83. doi:10.1097/YIC.0b013e3282f2b4d6
- Rosenbaum JF, Fava M, Hoog SL, Ascroft RC, Krebs WB. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial. Biol Psychiatry. 1998;44:77–87. doi:10.1016/S0006-3223(98)00126-7
- Wichniak A, Wierzbicka A, Walęcka M, Jernajczyk W. Effects of antidepressants on sleep. Curr Psychiatry Rep. 2017;19(9):63. doi:10.1007/s11920-017-0816-4
- Zhou S, Li P, Lv X, et al. Adverse effects of 21 antidepressants on sleep during acute-phase treatment in major depressive disorder: a systemic review and dose-effect network meta-analysis. Sleep. 2023;46(10):zsad177. doi:10.1093/sleep/zsad177
- Golder S, Medaglio D, O’Connor K, Hennessy S, Gross R, Gonzalez Hernandez G. Reasons for discontinuation or change of selective serotonin reuptake inhibitors in online drug reviews. JAMA Netw Open. 2023;6(7):e2323746. doi:10.1001/jamanetworkopen.2023.23746
- Baldwin DS, Chrones L, Florea I, et al. The safety and tolerability of vortioxetine: analysis of data from randomized placebo-controlled trials and open-label extension studies. J Psychopharmacol. 2016;30(3):242–252. doi:10.1177/0269881116628440
- Cao B, Park C, Rosenblat JD, et al. Changes in sleep predict changes in depressive symptoms in depressed subjects receiving vortioxetine: an open-label clinical trial. J Psychopharmacol. 2019;33(11):1388–1394. doi:10.1177/0269881119874485
- Liguori C, Ferini-Strambi L, Izzi F, et al. Preliminary evidence that vortioxetine may improve sleep quality in depressed patients with insomnia: a retrospective questionnaire analysis. Br J Clin Pharmacol. 2019;85(1):240–244. doi:10.1111/bcp.13772
- Clayton AH, El Haddad S, Iluonakhamhe JP, Ponce Martinez C, Schuck AE. Sexual dysfunction associated with major depressive disorder and antidepressant treatment. Expert Opin Drug Saf. 2014;13(10):1361–1374. doi:10.1517/14740338.2014.951324
- Cartwright C, Gibson K, Read J, Cowan O, Dehar T. Long-term antidepressant use: patient perspectives of benefits and adverse effects. Patient Prefer Adherence. 2016;10:1401–1407. doi:10.2147/PPA.S110632
- Atmaca M. Selective serotonin reuptake inhibitor-induced sexual dysfunction: current management perspectives. Neuropsychiatr Dis Treat. 2020;16:1043–1050. doi:10.2147/NDT.S185757
- Jacobsen PL, Mahableshwarkar AR, Palo WA, Chen Y, Dragheim M, Clayton AH. Treatment-emergent sexual dysfunction in randomized trials of vortioxetine for major depressive disorder or generalized anxiety disorder: a pooled analysis. CNS Spectr. 2016;21(5):367–378. doi:10.1017/S1092852915000553
- McIntyre RS, Florea I, Pedersen MM, Christensen MC. Head-to-head comparison of vortioxetine versus desvenlafaxine in patients with major depressive disorder with partial response to SSRI therapy: results of the VIVRE study. J Clin Psychiatry. 2023;84(4):23m14780. doi:10.4088/JCP.23m14780
- Jacobsen PL, Mahableshwarkar AR, Chen Y, Chrones L, Clayton AH. Effect of vortioxetine vs. escitalopram on sexual functioning in adults with well-treated major depressive disorder experiencing SSRI-induced sexual dysfunction. J Sex Med. 2015;12(10):2036–2048. doi:10.1111/jsm.12980
- Jacobsen PL, Nomikos GG, Zhong W, Cutler AI, Affinito H, Clayton A. Clinical implications of directly switching antidepressants in well-treated depressed patients with treatment-emergent sexual dysfunction: a comparison between vortioxetine and escitalopram. CNS Spectr. 2020;25(1):50–63. doi:10.1017/S1092852919000750
- Montejo AL, Sánchez-Sánchez F, De Alarcón R, et al. Switching to vortioxetine in patients with poorly tolerated antidepressant-related sexual dysfunction in clinical practice: a 3-month prospective real-life study. J Clin Med. 2024;13(2):546. doi:10.3390/jcm13020546
- Subramaniapillai M, Mansur RB, Zuckerman H, et al. Association between cognitive function and performance on effort based decision making in patients with major depressive disorder treated with vortioxetine. Compr Psychiatry. 2019;94:152113. doi:10.1016/j.comppsych.2019.07.006
- Mattingly GW, Necking O, Schmidt SN, Reines E, Ren H. Long-term safety and efficacy, including anhedonia, of vortioxetine for major depressive disorder: findings from two open-label studies. Curr Med Res Opin. 2023;39(4):613–619. doi:10.1080/03007995.2023.2178082
- IsHak WW, Greenberg JM, Cohen RM. Predicting relapse in major depressive disorder using patient-reported outcomes of depressive symptom severity, functioning, and quality of life in the Individual Burden of Illness Index for Depression (IBI-D). J Affect Disord. 2013;151(1):59–65. doi:10.1016/j.jad.2013.05.048
- IsHak WW, James DM, Mirocha J, et al. Patient-reported functioning in major depressive disorder. Ther Adv Chronic Dis. 2016;7(3):160–169. doi:10.1177/2040622316639769
- Papalexi E, Galanopoulos A, Roukas D, et al. Residual cognitive and psychosocial functional impairment in outpatients in Greece who responded to conventional antidepressant monotherapy treatments for major depressive disorder (MDD). J Affect Disord. 2022;314:185–192. doi:10.1016/j.jad.2022.07.009
- Lam RW, McIntosh D, Wang J, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 1. Disease burden and principles of care. Can J Psychiatry. 2016;61:510–523. doi:10.1177/0706743716659416
- Sheehan DV, Nakagome K, Asami Y, Pappadopulos EA, Boucher M. Restoring function in major depressive disorder: a systematic review. J Affect Disord. 2017;215:299–313. doi:10.1016/j.jad.2017.02.029
- Yang H, Gao S, Li J, et al. Remission of symptoms is not equal to functional recovery: psychosocial functioning impairment in major depression. Front Psychiatry. 2022;13:915689. doi:10.3389/fpsyt.2022.915689
- Cao B, Zhu J, Zuckerman H, et al. Pharmacological interventions targeting anhedonia in patients with major depressive disorder: a systematic review. Prog Neuropsychopharmacol Biol Psychiatry. 2019;92:109–117. doi:10.1016/j.pnpbp.2019.01.002
- Pan Z, Rosenblat JD, Swardfager W, McIntyre RS. Role of proinflammatory cytokines in dopaminergic system disturbances, implications for anhedonic features of MDD. Curr Pharm Des. 2017;23(14):2065–2072. doi:10.2174/1381612823666170111144340
- Höflich A, Michenthaler P, Kasper S, Lanzenberger R. Circuit mechanisms of reward, anhedonia, and depression. Int J Neuropsychopharmacol. 2019;22(2):105–118. doi:10.1093/ijnp/pyy081
- Nutt D, Demyttenaere K, Janka Z, et al. The other face of depression, reduced positive affect: the role of catecholamines in causation and cure. J Psychopharmacol. 2007;21(5):461–471. doi:10.1177/0269881106069938
- De Diego-Adeliño J, Crespo JM, Mora F, et al. Vortioxetine in major depressive disorder: from mechanisms of action to clinical studies. An updated review. Exp Opin Drug Saf. 2022;21(5):673–690. doi:10.1080/14740338.2022.2019705
- Sanchez C, Asin KE, Artigas F. Vortioxetine, a novel antidepressant with multimodal activity: review of preclinical and clinical data. Pharmacol Ther. 2015;145:43–57. doi:10.1016/j.pharmthera.2014.07.001
- Bang-Andersen B, Ruhland T, Jørgensen M, et al. Discovery of 1-[2-(2,4-dimethylphenylsulfanyl)phenyl]piperazine (Lu AA21004): a novel multimodal compound for the treatment of major depressive disorder. J Med Chem. 2011;54:3206–3221. doi:10.1021/jm101459g
- Mørk A, Pehrson A, Brennum LT, et al. Pharmacological effects of Lu AA21004: a novel multimodal compound for the treatment of major depressive disorder. J Pharmacol Exp Ther. 2021;340:666–675. doi:10.1124/jpet.111.189068
- Stahl SM. Modes and nodes explain the mechanism of action of vortioxetine, a multimodal agent (MMA): actions at serotonin receptors may enhance downstream release of four pro-cognitive neurotransmitters. CNS Spectr. 2015;20(6):515–519. doi:10.1017/S1092852915000358
- Stahl SM. Modes and nodes explain the mechanism of action of vortioxetine, a multimodal agent (MMA): modifying serotonin’s downstream effects on glutamate and GABA (gamma amino butyric acid) release. CNS Spectr. 2015;20(4):331–336. doi:10.1017/S1092852915000334
- Wilson S, Højer AM, Buchberg J, Areberg J, Nutt DJ. Differentiated effects of the multimodal antidepressant vortioxetine on sleep architecture: part 1, a pharmacokinetic/pharmacodynamic comparison with paroxetine in healthy men. J Psychopharmacol. 2015;29(10):1085–1091. doi:10.1177/0269881115599387
- Leiser SC, Iglesias-Bregna D, Westrich L, Pehrson AL, Sanchez C. Differentiated effects of the multimodal antidepressant vortioxetine on sleep architecture: part 2, pharmacological interactions in rodents suggest a role of serotonin-3 receptor antagonism. J Psychopharmacol. 2015;29(10):1092–1105. doi:10.1177/0269881115592347