
Abstract
Recent evidence indicates that the nature of interactions between the nervous system and immune system is important in the pathogenesis of depression. Specifically, alterations in pro-inflammatory cytokines have been related to the development of several psychological and neurobiological manifestations of depressive disorder, as well as to stress exposure. A number of findings point to tumor necrosis factor alpha (TNF-α) as one of the central factors in these processes. Accordingly, in the present study, we test the hypothesis that specific influences of chronic stressors related to traumatic stress and dissociation are related to alterations in TNF-α levels. We performed psychometric measurement of depression (Beck Depression Inventory [BDI]-II), traumatic stress symptoms (Trauma Symptom Checklist [TSC]-40), and psychological and somatoform dissociation (Dissociative Experiences Scale [DES] and Somatoform Dissociation Questionnaire [SDQ]-20, respectively), and immunochemical measure of serum TNF-α in 66 inpatients with unipolar depression (mean age 43.1 ± 7.3 years). The results show that TNF-α is significantly related to DES (Spearman R=−0.42, P<0.01), SDQ-20 (Spearman R=−0.38, P<0.01), and TSC-40 (Spearman R=−0.41, P<0.01), but not to BDI-II. Results of the present study suggest that TNF-α levels are related to dissociative symptoms and stress exposure in depressed patients.
Introduction
Advances in psychoneuroimmunological research suggest that the activation of pro-inflammatory mechanisms plays an important role in the pathophysiology of depression.Citation1–Citation4 Pro-inflammatory cytokines are substantially involved in this process and it has been proposed that, at least for a sub-group of depressed patients, they may represent a causal factor.Citation5
Tumor necrosis factor alpha (TNF-α), one of the prominent pro-inflammatory cytokines, has been studied largely in this context.Citation5 It has been associated with depressive disorder in a number of cross-sectional studies,Citation6–Citation8 as well as one longitudinal study.Citation9 The research, however, has extended beyond a simple association with depression; TNF-α has been related to different aspects of depressive symptomatologyCitation10,Citation11 and specific emotional and cognitive disturbances.Citation12 Moreover, TNF-α has been studied in relation to stress response and stressor-specific findingsCitation13 together with a moderating influence of depressionCitation14 have been identified. However, association to specific trauma-related phenomena in a depressed population, namely trauma-related and dissociative symptoms, has yet to be explored.
Based on these data, it was postulated that serum TNF-α levels, measured in depressed inpatients, would be related to the assessment of both depressive symptomatology and trauma-related and dissociative symptomatology.
Methods
Participants
In order to examine the above hypothesis, assessment of basal serum TNF-α levels during rest conditions and psychometric measures were performed in 66 consecutive inpatients with unipolar depression on the same day. At the time of recruitment, patients were treated at the Department of Psychiatry (Charles University, Prague). The assessments were performed within 2 weeks from the admission. The patients had a diagnosis of unipolar depressive disorder (ie, patients with recurrent depression or depressive period) in relapse without posttraumatic stress disorder (PTSD) and other comorbid diagnoses confirmed according to Diagnostic and Statistical Manual of Mental Disorders (DSM) version IV criteria by clinical interview.Citation15 In order to re-examine diagnosis and to exclude patients with PTSD or other comorbidities all patients were also screened using structured psychiatric interview The Mini-International Neuropsychiatric Interview (MINI) version 5.0.0.Citation16 Patients’ treatment at the time of recruitment was based only on antidepressant medication according to national guidelines.Citation17 Exclusion criteria were organic illnesses involving the central nervous system, psychotic disorders, PTSD, bipolar disorder, alcohol and/or drug abuse, any form of epilepsy, and mental retardation (Raven intelligent quotient test result higher than 90 in all included patients), inflammatory, neuroendocrine, and metabolic disorders, any hormonal or antipsychotic medication, methyldopa, prednisolone and cimetidine medication, electroconvulsive therapy or repetitive transcranial magnetic stimulation, and pregnancy or lactation in women. All the patients gave written informed consent and the clinical study was approved by the ethical committee of Charles University, Prague.
Psychometric measures
For the assessment of depressive symptoms, the Beck Depression Inventory (BDI)-II,Citation18 which is a 21-item questionnaire for assessing depression (Cronbach’s alpha 0.89, test-retest reliability after a week =0.85), was used. Subjects indicated the degree of their experience of depressive symptoms on a 4-point Likert scale.
Psychic dissociative symptoms were assessed by Dissociative Experiences Scale (DES).Citation19 DES represents a 28 item self-reported questionnaire examining main dissociative phenomena such as absorption, amnesia, depersonalization, derealization, reality distortion, and others. Subjects indicate a degree of their experience on the continuum from 0% to 100%. In the present study, we used the Czech version of the DES that, similar to the original English version, displays high reliability and internal consistency (Cronbach’s alpha 0.92, test-retest reliability after a week =0.91).
Somatoform dissociative symptoms were assessed using the 20-item self-reported Somatoform Dissociation Questionnaire (SDQ-20).Citation20 Somatoform dissociative symptoms represent alterations in sensations of pain (analgesia, kinesthetic anesthesia), alterations of perception, loss of motor control, gastrointestinal symptoms, etc. Subjects indicate the degree of their experience on a 5-point Likert scale. We used the Czech version of the SDQ-20 that displays high reliability and internal consistency (Cronbach’s alpha 0.91, test-retest reliability after a week =0.90).
For investigation of traumatic symptoms, the Trauma Symptom Checklist (TSC)-40Citation21 was used. TSC-40 is a self-reported 40-item questionnaire done on a 4-point Likert scale. TSC-40 evaluates symptomatology in adults associated with childhood or adult traumatic experiences and measures aspects of posttraumatic stress and other symptom clusters found in some traumatized individuals. The Czech version of the TSC-40 has high reliability and internal consistency (Cronbach’s alpha 0.91, test-retest reliability after a week =0.88).
Immunochemical measures
For biochemical assessment, blood samples of 5 mL volumes were collected in rest conditions according to common procedures between 7:30 am and 8:00 am in the laboratory of the psychiatry department. The blood samples were carefully transferred (about 10 minutes) in an icebox at 4°C to the Central Laboratories of the Institute of Medical Biochemistry and Laboratory Diagnostics, 1st Faculty of Medicine Charles University and General University Hospital in Prague where they were immediately centrifuged (4°C, 3,000 rpm, 10 minutes), pipetted into vials 2 × 0.5 mL each, and stored at −20°C until the time of analysis. TNF-α serum levels were measured using a commercial immunoradiometric assay (IRMA) provided by DRG Instruments GmbH (Marburg, Germany). Principles of the TNF-α IRMA assay were based on coated-tube separation. The capture antibodies were attached to the lower and inner surface of the plastic tube. Standards or samples added to the tubes at first showed low affinity for antibodies. The signal antibody labeled with 125I triggered the immunological reaction. After washing, the remaining radioactivity bound to the tube reflected the antigen concentration. Precision of the TNF-α IRMA corresponded to intra-assay coefficients of variation <7.0%. Sensitivity of the TNF-α concentration corresponding to the mean counts per minute +2 standard deviations (SD) was 5 pg/mL.
Statistical methods
Statistical description of the studied population included means and SD. In order to assess the relationship between TNF-α levels and psychometric measures, the Spearman rank correlation coefficient were determined. The Spearman rank correlation coefficient represents a robust nonparametric measure of correlation, resistant to the presence of outliers.Citation22
All the methods of statistical evaluation were performed using the software package Statistica version 6 (StatSoft Inc., Tulsa, OH, USA). The statistical significance was presumed at a P-value <0.05.
Results
presents the demographic and biometric characteristics of the studied population. summarizes the drug treatment in the studied population.
Table 1 Demographic and biometric characteristics of the studied population
Table 2 Drug treatment in the studied population
The results indicate that TNF-α is significantly correlated to DES (Spearman R=−0.42, P<0.01) (), SDQ-20 (Spearman R=−0.38, P<0.01) (), and TSC-40 (Spear-man R=−0.41, P<0.01), but not to BDI-II (). These correlations show that TNF-α exhibits a significant relationship with psychological and somatoform dissociation and the symptoms related to traumatic stress. Other statistically significant correlations were also found between psychometric measures of depression, traumatic stress, and dissociation ().
Figure 1 Dependency graph of TNF-α (pg/mL) and DES (Spearman R=−0.36, P<0.01).
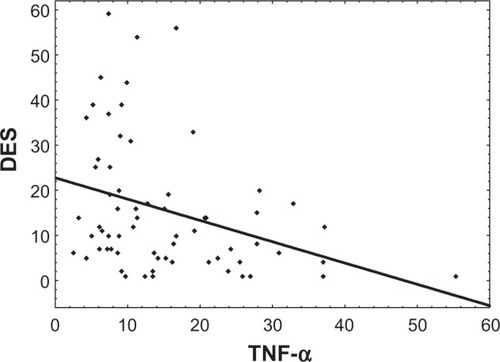
Figure 2 Dependency graph of TNF-α (pg/mL) and SDQ-20 (Spearman R=−0.30, P<0.05).
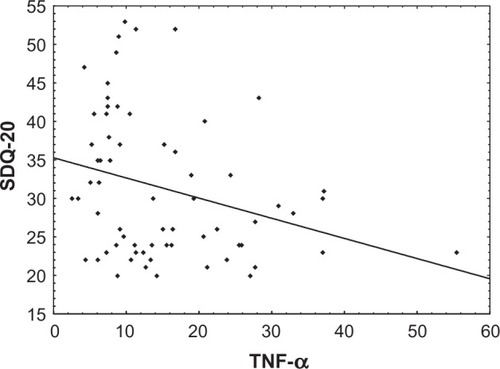
Table 3 Spearman correlations of TNF-α and results of psychometric measures
Statistical comparison between men and women did not show significant differences in TNF-α or psychometric measures. No significant correlation was found between BMI and age and TNF-α and psychometric parameters.
Discussion
In accordance with our hypothesis, results of the present study confirm a statistically significant relationship between TNF-α levels and the symptoms linked to chronic stressful experiences in depressed patients. However, the fact that the correlation is negative, is surprising and seems to be in contrast to both the theoretical framework and our previous research focused on interleukin (IL)-6, another pro-inflammatory cytokine. Moreover, unexpectedly, no significant relationship is revealed between TNF-α and depressive symptoms.
In order to understand the observed relationship between TNF-α and dissociative symptoms, studies on the hypothalamo-pituitary axis (HPA) activation in depression appear relevant. Importantly, a negative correlation was found between cortisol and somatoform dissociation in a population of depressed patients.Citation23 On the other hand, TNF-α was reported to increase the HPA activity in depression.Citation5 The present finding is in line with these results pointing to the fact that somatoform dissociation may moderate the interplay between TNF-α and HPA activity in depression. Noteworthy, our previous work reported a positive correlation between IL-6 and somatoform dissociation.Citation24 Interestingly, taken together, both findings are consistent with the reported inhibition between TNF-α by IL-6Citation25 and they indicate that a complex interaction between the two pro-inflammatory cytokines and their neurobiological effect may exist.
Similarly, the negative correlation between TNF-α and trauma-related symptoms is in an apparent contradiction with the theoretical framework. Notably, acute stress conditions are associated with an increase in TNF-α in depressed patients.Citation26 Nevertheless, when focusing specifically on chronic stress conditions, the result corresponds to the work by Bartolomucci et alCitation27 who observed that chronic psychosocial stress down-regulated TNF-α messenger ribonucleic acid (mRNA) levels in the striatum and hippocampus.
Finally, as stated previously, finding no relevant association between TNF-α and depressive symptoms was unexpected. Mean serum TNF-α level for the whole group (25.4 pg/mL ± 5.1 SD) appears higher than the TNF-α serum values reported in healthy volunteers (1–10 pg/mL).Citation8 Nevertheless, TNF-α assessment was not performed in healthy controls in our study and only a single self-reported test was used to assess the depressive symptoms (BDI-II). Therefore, it is not possible to decide if the lack of correlation between TNF-α and depressive symptoms is due to low TNF-α levels in the depressed group, a low sensitivity of psychometric instrument, or another reason.
The present study has several limitations. First, since the scope of the study is to describe the nature of the relationship between TFN-α and specific psychometric characteristics in depressive disorders, no healthy or other control group was included in the analysis. The interpretation of the findings is therefore limited to this clinical condition. Second, the main focus on trauma-related psychopathology determined largely the choice of psychometric test, preferring reliable and widely used self-reported tests such as DES, SDQ-20, and TSC-40. As a result, the findings may be set in the context with the large body of research performed using these instruments while further interpretation must be done with precaution, taking into account the limitation imposed by the self-reported nature of the testing. This precaution is relevant even more for the interpretation of results related to depressive symptoms, as already mentioned. Third, while patient recruitment led to a quite naturalist clinical cohort, the characteristics of the studied group (inpatients, heterogeneous antidepressant treatment) limit the findings. In particular, the effect of antidepressant treatment may vary considerably between different substances and therapeutic regimens.Citation28–Citation30 A larger clinical group and a longitudinal study design is needed to address this issue. Lastly, the study is limited to only one of a large group of pro-inflammatory cytokines. In order to have a complex insight into the role of immune processes in emotional regulation and the development of affective disorders, other pro- and anti-inflammatory cytokines together with stress axis activity have to be explored.Citation2,Citation13
Altogether, TNF-α has been intensively studied as one of the prominent candidates in the cytokine model of depression. The role of TNF-α within depressive disorder seems, however, rather complex; specific emotional and stress system regulations may play an important role. The findings of the present study reveal a tiny piece in this puzzle, encouraging further efforts to describe in more detail the interplay of TNF-α regulations and chronic stress and dissociative processes in the development and clinical manifestation of depression.
Acknowledgments
The study was supported by the grant GACR P407/12/1957, project MSM0021620849 provided by the Czech Ministry of education and the project “CEITEC – Central European Institute of Technology” (CZ.1.05/1.1.00/02.0068) from the European Regional Development Fund.
Disclosure
The authors report no conflicts of interest in this work.
References
- WichersMMaesMThe psychoneuroimmuno-pathophysiology of cytokine-induced depression in humansInt J Neuropsychopharmacol20025437538812466036
- SchiepersOJWichersMCMaesMCytokines and major depressionProg Neuropsychopharmacol Biol Psychiatry200529220121715694227
- RaisonCLCapuronLMillerAHCytokines sing the blues: inflammation and the pathogenesis of depressionTrends Immunol2006271243116316783
- BlumeJDouglasSDEvansDLImmune suppression and immune activation in depressionBrain Behav Immun201125222122920955778
- HimmerichHFuldaSLinseisenJDepression, comorbidities and the TNF-alpha systemEur Psychiatry200823642142918504118
- ZorrillaEPLuborskyLMcKayJRThe relationship of depression and stressors to immunological assays: a meta-analytic reviewBrain Behav Immun200115319922611566046
- HowrenMBLamkinDMSulsJAssociations of depression with C-reactive protein, IL-1, and IL-6: a meta-analysisPsychosom Med200971217118619188531
- DowlatiYHerrmannNSwardfagerWA meta-analysis of cytokines in major depressionBiol Psychiatry201067544645720015486
- van ZuidenMHeijnenCJvan de SchootRCytokine production by leukocytes of military personnel with depressive symptoms after deployment to a combat-zone: a prospective, longitudinal studyPLoS ONE2011612e2914222195009
- HauserPKhoslaJAuroraHA prospective study of the incidence and open-label treatment of interferon-induced major depressive disorder in patients with hepatitis CMol Psychiatry20027994294712399946
- KrausMRSchäferAFallerHCsefHScheurlenMPsychiatric symptoms in patients with chronic hepatitis C receiving interferon alfa-2b therapyJ Clin Psychiatry200364670871412823087
- ReichenbergAYirmiyaRSchuldACytokine-associated emotional and cognitive disturbances in humansArch Gen Psychiatry200158544545211343523
- García-BuenoBCasoJRLezaJCStress as a neuroinflammatory condition in brain: damaging and protective mechanismsNeurosci Biobehav Rev20083261136115118468686
- WeinsteinAADeusterPAFrancisJLBonsallRWTracyRPKopWJNeurohormonal and inflammatory hyper-responsiveness to acute mental stress in depressionBiol Psychol201084222823420117167
- American Psychiatric AssociationDSM IV, Diagnostic and Statistical Manual of Mental DisordersWashingtonAmerican Psychiatric Association1994
- SheehanDVLecrubierYSheehanKHThe Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10J Clin Psychiatry199859Suppl 202233 quiz 349881538
- RabochJAndersMPraskoJHellerovaPDoporučené postupy psychiatrické péče II [Recommended procedures in psychiatric care]PrahaInfopharm2006 Czech
- BeckATSteerRABrownGKManual for Beck Depression Inventory – IISan AntonioPsychological Corporation1996
- BernsteinEMPutnamFWDevelopment, reliability, and validity of a dissociation scaleJ Nerv Ment Dis1986174127277353783140
- NijenhuisERSpinhovenPVan DyckRVan der HartOVanderlindenJThe development and psychometric characteristics of the Somatoform Dissociation Questionnaire (SDQ-20)J Nerv Ment Dis1996184116886948955682
- BriereJPsychometric review of the Trauma Symptom Checklist-40StammBHMeasurement of Stress, Trauma, and AdaptationLuthervilleSidran Press1996381383
- AbdullahMBOn a robust correlation coefficientStatistician1990394455460
- BobPFreyberghPFJasovaDDepression, cortisol and somatoform dissociative symptomsNeuro Endocrinol Lett200829223523918404142
- BobPRabochJMaesMDepression, traumatic stress and interleukin-6J Affect Disord20101201–323123419359044
- HiranoTAkiraSTagaTKishimotoTBiological and clinical aspects of interleukin 6Immunol Today199011124434492127356
- PepysMBHirschfieldGMC-reactive protein: a critical updateJ Clin Invest2003111121805181212813013
- BartolomucciAPalanzaPParmigianiSChronic psychosocial stress down-regulates central cytokines mRNABrain Res Bull200362317317814698350
- KrausTHaackMSchuldAHinze-SelchDKoetheDPollmächerTBody weight, the tumor necrosis factor system, and leptin production during treatment with mirtazapine or venlafaxinePharmacopsychiatry200235622022512518269
- BrustolimDRibeiro-dos-SantosRKastREAltschulerELSoaresMBA new chapter opens in anti-inflammatory treatments: the antidepressant bupropion lowers production of tumor necrosis factor-alpha and interferon-gamma in miceInt Immunopharmacol20066690390716644475
- JanssenDGCaniatoRNVersterJCBauneBTA psychoneuroimmunological review on cytokines involved in antidepressant treatment responseHum Psychopharmacol201025320121520373471