Abstract
Purpose
The purpose of this report is to demonstrate a rare clinical manifestation of apraxia eyelid opening related to a basal ganglia lesion.
Case report
In this study, we report a 91-year-old woman suffering from difficulty in eyelid opening after being treated for myocardial ischemia with dual antiplatelet medications. She could open her eyelid with fingers touching her forehead. Brain computed tomography revealed a right putamen hemorrhage. Surface electromyography revealed persistent frontalis muscle contraction during relaxation of orbicularis oculi muscles. Apraxia of eyelid opening was diagnosed. Her eyelid symptom resolved 2 months later.
Conclusion
Apraxia of eyelid opening may be caused by subcortical hemorrhage of the basal ganglia. In addition to the primary motor cortex and supplemental motor area, the basal ganglia may also play a role in eyelid opening.
Introduction
Apraxia of eyelid opening (AEO) is a syndrome that manifests as the inability to open the eyes at will. Patients usually try to open their eyes with their hands or by contracting the frontalis muscles in the absence of any significant evidence of orbicularis oculi contraction, such as lowering of the brow beneath the orbital rim (Charcot sign).Citation1,Citation2 This syndrome is often found in patients with progressive supranuclear palsy, Parkinson’s disease, atypical parkinsonism, and blepharospasm,Citation2,Citation3 but is rarely seen as the initial presentation of an acute cerebrovascular event.Citation4–Citation8 Herein, we report the case of a patient with AEO in which the AEO was an initial clinical symptom of right putamen hemorrhage.
Case presentation
A 91-year-old right-handed woman with a history of hypertension was admitted to the medical ward due to pneumonia. She was independent in daily life and without a documented neurological deficit.
One day following admission, a sudden onset of chest discomfort was noted and non-ST elevated myocardial infarction was diagnosed. She was transferred to the intensive care unit, where clopidogrel and aspirin were used continually, followed by heparinization for 3 days. After 7 days of this dual antiplatelet therapy, she was found to have an acute onset of difficulty in opening her eyes. A nasogastric (NG) tube was put in place to avoid choking and because she could not walk steadily. A neurologist was consulted for the eye-opening problem.
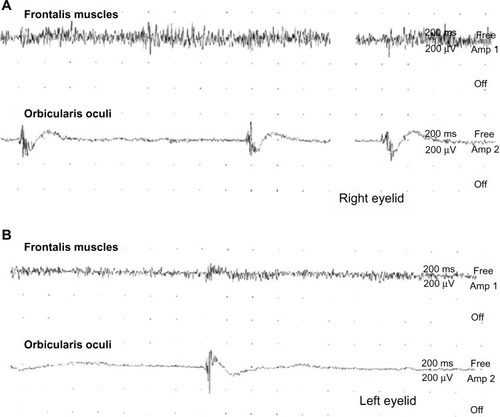
The neurological exam revealed she had difficulty in bilateral eyelid opening, left central facial palsy, mild dysarthria, and left-side hemiparesis. Pursuit and saccadic eye movements were intact. Her eye opening was especially difficult after closing her eyes tight, but she could open her eyelid after a light touch to her forehead. No ptosis or blepharospasm was noted. Brain computed tomography scans revealed an acute hemorrhage at the right putamen () and surface electromyography revealed persistent contraction of the frontalis muscle and relaxation of the orbicularis oculi muscles on trying to open the eyes (). AEO was suspected.
Figure 1 Brain computed tomography scans showing acute hemorrhage at the right putamen.
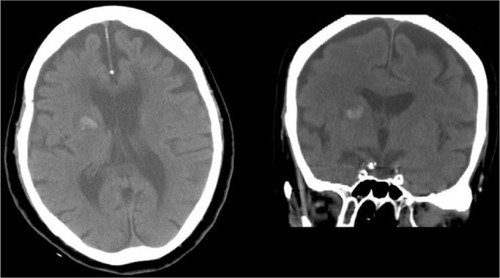
Figure 2 Surface electromyography was recorded at the bilateral eyelids: (A) right frontalis and orbicularis oculi muscles; (B) left frontalis and orbicularis oculi muscles. Persistent contraction of the frontalis muscle was observed, while there was rare contraction of the orbicularis oculi muscle when the patient tried to open her eyes.
Her eyelid opening and dysphagia had not improved 2 weeks after the hemorrhage. Half a Sinemet® (carbidopa-levodopa, 25/100 mg) tablet (Merck & Co., Inc, Whitehouse Station, NJ, USA) was given twice daily for 6 weeks. Her NG tube was removed 1 month later. Her eyelid problem had subsided after 2 months of hemorrhage being identified, while brain computed tomography scans revealed that the hemorrhage had resolved.
Discussion
The case described here had AEO as the initial presentation of right putamen hemorrhage without other extrapyramidal symptoms suggestive of Parkinson’s disease, progressive supranuclear palsy, or cortico-basal degeneration. As it is well known that a unilateral basal ganglia lesion can cause bilateral AEO, here we discuss the possible mechanism of this symptom in our patient.
Voluntary eye opening is controlled by the corticobulbar tract from the primary motor cortex (M1) and motor-related cortical areas, including the supplementary motor area (SMA) or premotor cortex. The basal ganglia may play a role in the regulation of the eye-opening system in the SMA through the thalamus.Citation9 In terms of basal ganglia dysfunction, regulation may be impaired in Parkinson’s disease or other diseases with parkinsonian features and AEO. On the basis of pharmacological evidence, the role of basal ganglia dysfunction in AEO has been further clarified,Citation10 even in Parkinson’s disease patients receiving deep brain stimulation at the bilateral subthalamic nucleus.Citation11 Thus, the AEO in our patient may support the theory of a basal ganglia abnormality producing AEO.
In our case, we suggest that the right hemispheric lesion may have caused the AEO. A few reports have suggested that a right cerebral hemispheric lesion would be more likely to cause AEO because the right cerebral hemisphere controls the bilateral levator palpebrae superioris.Citation5–Citation8 In contrast, other reports have shown that a dominant hemisphere lesion caused AEO.Citation4,Citation7 As for the laterality of AEO, more evidence is still required to reach a conclusion about this.
Dual antiplatelet therapy of aspirin and clopidogrel has been proven to be associated with significantly reduced major atherothrombotic events and an increased risk of moderate and severe bleeding.Citation12 Indeed, gastrointestinal bleeding and intracranial hemorrhage are two of the most common bleeds associated with dual antiplatelet therapy. Since AEO is an uncommon initial presentation of intracranial hemorrhage, special caution should be taken and further brain imaging performed during dual antiplatelet treatment for atherothrombotic events.
Conclusion
Our patient experienced eyelid-opening apraxia secondary to an isolated right putamen hemorrhage, which is suggestive of the essential role of the basal ganglia in eyelid opening.
Disclosure
The authors declare no conflicts of interest in this work.
References
- ZadikoffCLangAEApraxia in movement disordersBrain2005128Pt 71480149715930045
- MillerNRNewmanNJThe Essentials: Walsh and Hoyt’s Clinical Neuro-Ophthalmology5th edBaltimore, MDWilliams & Wilkins1999
- HallettMEvingerCJankovicJStacyMBEBRF International WorkshopUpdate on blepharospasm: report from the BEBRF International WorkshopNeurology200871161275128218852443
- KaiboriboonKOliveiraGRLeiraECApraxia of eyelid opening secondary to a dominant hemispheric infarctionJ Neurol2002249334134211993536
- AlgoedLJanssensJVanhoorenGApraxia of eyelid opening secondary to right frontal infarctionActa Neurol Belg19929242282331441901
- JohnstonJCRosenbaumDMPiconeCMGrottaJCApraxia of eyelid opening secondary to right hemisphere infarctionAnn Neurol19892566226242742362
- HiroseMMochizukiHHonmaMKobayashiTNishizawaMUgawaYApraxia of lid opening due to a small lesion in basal ganglia: two case reportsJ Neurol Neurosurg Psychiatry201081121406140720547609
- LeeSSLeeHSCan subcortical infarction cause apraxia of eyelid opening?J Clin Neurosci201118101399140021778059
- CostaJValls-SoléJValldeoriolaFRumiàJTolosaEMotor responses of muscles supplied by cranial nerves to subthalamic nucleus deep brain stimuliBrain2007130Pt 124525517151002
- LeeKCFinleyRMillerBApraxia of lid opening: dose-dependent response to carbidopa-levodopaPharmacotherapy200424340140315040654
- UmemuraAToyodaTYamamotoKOkaYIshiiFYamadaKApraxia of eyelid opening after subthalamic deep brain stimulation may be caused by reduction of levodopaParkinsonism Relat Disord200814865565718316231
- BhattDLFoxKAHackeWCHARISMA InvestigatorsClopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic eventsN Engl J Med2006354161706171716531616