
Abstract
Background
This study investigated the treatment effects of calligraphy therapy on childhood survivors of the 2008 Sichuan earthquakes in the People’s Republic of China.
Methods
In experiment 1, 129 children participated in a 30-day calligraphic training, and 81 children were controls. The Children’s Revised Impact of Event Scale was adopted to assess behavioral effects. Experiment 2 involved 41 treatment subjects and 39 controls, with the same procedure as in experiment 1 except that salivary cortisol level was also measured as a physiological indicator.
Results
After 30 days of calligraphy treatment, the arousal symptoms and salivary cortisol levels in the experimental group decreased from 5.72±0.31 and 13.34±2.88 to 4.98±0.31 and 9.99±2.81, respectively. In the control group, there was not a significant decrease from pretest to post-test. In addition, the arousal scores in posttest (4.98±4.39) were significantly lower than midtest (5.71±4.14) for girls; in contrast, for boys, posttest (4.90±4.24) showed little change compared with midtest (5.04±4.36), but both were significantly lower than pretest (6.42±4.59).
Conclusions
Calligraphy therapy was effective in reducing hyperarousal symptoms among child survivors.
Introduction
On May 12, 2008, an earthquake measuring 8.0 on the Richter scale hit Wenchuan, People’s Republic of China. The earthquake was considered the most devastating natural disaster in the People’s Republic of China since the 1976 Tangshan earthquake. According to official state statistics, the Wenchuan earthquake caused 69,277 deaths and 374,643 injuries and left 17,923 listed as missing and about 4.8 million homeless.Citation1 Post-traumatic stress disorder (PTSD) is often considered the most frequently reported adverse psychological sequelae among survivors of natural disasters. PTSD is an anxiety disorder caused by exposure to a life-threatening situation or situations accompanied by feelings or fear, helplessness, or horror.Citation2 The symptoms of PTSD listed in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, include intrusion and reexperience, avoidance and emotional numbing, and hyperarousal.Citation3 Children, compared with adults, are a particularly vulnerable populationCitation4 because of their limited cognitive schema and behavioral repertoire.Citation5 The prevalence of PTSD among child and adolescent survivors of earthquakes ranged from 4.5%–60%.Citation6–Citation10
Cortisol, a stress hormone secreted by the adrenal cortex, is considered an informative biomarker of PTSD.Citation11 Psychological stress increases the synthesis and release of cortisol. Cortisol mobilizes and replenishes energy and contributes to increased arousal, vigilance, focused attention, and memory formation.Citation12 Acute exposure to stress leads to a rapid increase in cortisol level; a prolonged status of hypervigilance in PTSD may lead to dysregulation of cortisol.Citation13 The relationship between cortisol level and PTSD is inconsistent, partly because of its comorbidity with major depression, severity of PTSD symptoms, time since the trauma, and duration of trauma exposure.Citation14 Sex difference in cortisol level is also found among adults with PTSD,Citation15 and the reactive change in cortisol level varies with age among dysphoric children, who exhibit age-related difference in cortisol changes in the face of a stressor.Citation16
Chinese calligraphic handwriting entails an integration of the mind, body, and character, interwoven in a dynamic process. It involves visual perception of the character, spatial structuring of the character, cognitive planning, and maneuvering of the brush to follow specific character configurations.Citation17 Research in recent years has gradually established calligraphy therapy as an indigenous and complementary practice that is capable of improving aspects of people’s behavioral and psychosomatic conditions,Citation18,Citation19 enhancing their attention and concentration as well as facilitating their physical relaxation and emotional stabilization.Citation20 The theoretical framework for calligraphy as a treatment is threefold:Citation21 first, sensory and biomotional feedback: the individual receives sensory feedback from the graphic record while practicing calligraphy; second, biomotional feedback: the calligraphy involves the movement of the arms and the whole body as the individuals guide and regulate their movement; and finally, cognitive feedback: the subjective experiences of heighted attention, alertness, and quickened responses during the writing.
Via this feedback, calligraphy practice increases the ability of patients to self-monitor and may modify the cognitive deficits, as well as alter the arousal level. Brush writing in calligraphy requires intensive attention and concentration and involves highly controlled moves and well-coordinated movements. The writer has to reduce external and internal disturbances and focus on the present moment. This high level of attention is evidenced when the heart rate decelerates.Citation20 Calligraphy therapy shares some fundamental elements with mindfulness practice: both involve paying attention to and being aware of the present experiences,Citation22 and both have the same effect on attention regulation and relaxation.Citation23
A recent study has shown the appearance of theta waves in frontal midline during brush writing, which underlines the power of calligraphy training in contributing to facilitated attention, concentration, and focusing at the neurocognitive level. This reflects the relaxed and concentrated state evoked by the act of brush writing, with the brush writer’s body being in a relaxed state while his mind is in an apprehensive and intensive state.Citation22,Citation24 When long-term practitioners of meditation engage in mental training, it involves temporal integrative mechanisms, which may induce short-term and long-term neural changes through the generation of gamma waves.Citation25 This is also what the act of calligraphy entails, showing both the fast gamma waves and the deep relaxing theta waves simultaneously. This indicates a sharing of similar neural cognitive experience between these two practices.Citation24 In fact, some mindfulness practitioners have adapted calligraphy as a method of mindfulness meditation,Citation26 as well as relaxation training.Citation27
Hypervigilance and concentration difficulty are two central characteristics of PTSD hyperarousal symptoms that play an important role in the maintenance of chronic PTSD.Citation28,Citation29 On the basis of previously reviewed clinical evidence of the enhanced attention and relaxation resulting from calligraphy treatment, we believed the treatment may also have the same benefits for PTSD, by reducing hyperarousal symptoms. Stress management intervention has long been adapted as a treatment for post-trauma adjustment,Citation30 and a positive outcome includes reduced cortisol levels and increased relaxation.Citation31 In addition, some behavioral treatment techniques (such as mind–body therapy) have shown moderating effects on salivary cortisol (SC).Citation32 Although no study has accessed the effectiveness of calligraphy treatment for PTSD, mindfulness-base relaxation training has been recently used for treating PTSD and showed clinical effectiveness among military veterans,Citation33 cancer patients,Citation34 firefighters,Citation35 and mental health workers after a natural disaster.Citation36 Mindfulness-based therapy is suggested to be especially useful in reducing rumination symptoms,Citation37 which are associated with increased basal cortisol levels.Citation38 Mindful exercise enhanced the quality of life among women with breast cancer who exhibited a reduction in cortisol level after the treatment.Citation39
Of particular note is the therapeutic effectiveness of calligraphy treatment among children with behavioral and cognitive disorders. Calligraphy treatment has had an effect on enhanced attention, sensory-perceptual sharpness, cognitive and reasoning ability, emotional stability, and self-control among children with attention-deficit/hyperactivity disorder (ADHD) and autism.Citation40–Citation43 The results indicate that this training facilitates cognitive functioning, calms emotions, and improves some clinical and mental health conditions of children with ADHD.Citation40 Significant improvement in all these areas of child behavior was seen after calligraphy training. In general, the results indicate that the practice has an especially positive effect on improving the attentiveness and emotional stability of ADHD children.
For autistic children, postcalligraphy training resulted in significant improvement in the measures of attention, social behavior, communication, volition, ability to adapt to the environment, and emotional and instinctual responses,Citation41 as well as in a significant reduction in negative and group behaviors and in negative behavior in general and in family gatherings in particular,Citation42,Citation43 thus echoing the findings of similar reports on ADHD children.Citation40 Both studiesCitation42,Citation43 have offered evidence on the positive effects of calligraphy training on children with activity, conduct, and attention problems. This summary of our empirical research and of the clinical applications of calligraphy therapy, all involving children with various common disorders, serves as a summative review of the foundations and rationale that underlined the present study on PTSD intervention and treatment.
The current study aimed to investigate the effectiveness of calligraphy treatment among a sample of youth 1 year after exposure to natural disaster (ie, an earthquake). According to previous evidence revealing the psychological benefits (ie, enhanced attention, relaxation) of calligraphy treatment with regard to various mental health problems, we hypothesized that calligraphy treatment would reduce PTSD symptoms, especially hyperarousal symptoms, in the present sample. Second, on the basis of the theoretical and empirical evidence of the relationships between cortisol and stress reduction management, we hypothesized there would be a significant decline in cortisol level in the calligraphy treatment group compared with in the control group. In addition, because sex is a moderator of both PTSD symptomsCitation44 and cortisol reaction to stress,Citation15 we expected that sex may moderate the effect of calligraphy treatment.
Experiment 1: behavioral changes in Children’s Revised Impact of Event Scale
Method
Participants
A total of 210 children in the fourth and fifth grades, 105 boys and 105 girls, participated in our study. They were selected randomly from the five classrooms of two farm village and township schools in the disaster areas. Three of the classes were randomly selected as treatment groups, and the other two were control groups. The treatment group consisted of 129 pupils, 65 boys and 64 girls, and had a mean age of 10.51±1.15 years. They were given calligraphy training for 1 hour a day for 30 consecutive days. The control group had 81 children (41 boys and 40 girls) and a mean age of 10.52±1.13 years. These children were similarly assessed before and after the same period as the treatment group, but without calligraphy training. The demographic characteristics of experiment 1 and experiment 2 are outlined in .
Table 1 Numbers of boys and girls and their ages (mean ± standard deviation) in experiment 1 and experiment 2
Instruments
The Children’s Revised Impact of Event Scale (CRIES-13) was adopted to assess the behavioral effects of the participants before and after training.Citation45 This scale was validated for use in the disaster areas by the Institute of Psychology, Chinese Academy of Sciences. It had three subscales: Intrusion, Avoidance, and Arousal.
Procedure
The experiment procedure followed a validated system of treatment protocols.Citation41 The participants in the experimental group were each required to brush write 40 medium-sized characters from five copybook pages by the tracing mode of writing. The copybook, ink, and writing bush were allocated to these children by the experimenters. The treatment took 1 hour a day, 5 days a week, for a total of 30 days under the supervision of a teacher while the child was in the school or a parent if the child was at home. The controls carried on their regular school activities throughout the study duration, without any writing tasks. The study was conducted a year after the Sichuan earthquakes.
The Chinese version of CRIES-13 was administered to all subjects once before the experiment, again at the halfway point after 15 days, and one more time after 30 days of treatment. Caution was exercised with respect to balancing the geographic regions, age of the pupils, and assignment of groups, as well as potential intervening variables.
Results
Data were submitted to a 3×2×2 repeated measures analysis of variance in which test (three levels: pretest, midtest, and post-test) served as the within-subjects variable and group (two levels: experimental group and control group) and sex (two levels: boys and girls) was the between-subjects variable.
Intrusion and avoidance as dependent variable
The main effect of test [F(2,412)=8.10; P=0.000; η2=0.053] reached a significant level (P<0.05). Further analysis showed that compared with the pretest (mean =5.37, standard deviation =4.05) and midtest (mean =5.28, standard deviation =4.15), there was a significant decrease in Intrusion scores in post-test (mean =4.35, standard deviation =3.71). For Avoidance, neither main effects nor interaction effect reached a significant level ().
Table 2 Average (standard deviation) scores on intrusion, avoidance, and arousal by condition
Arousal as a dependent variable
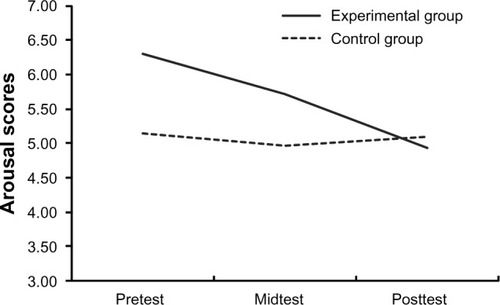
When Arousal scores were analyzed, the main effect of test [F(2,410)=3.44; P=0.033; η2=0.016] reached a significant level (P<0.05). After further multiple comparisons, it was found that the Arousal scores at post-test (mean =4.98, standard deviation =0.31) were significantly lower than at pretest (mean =5.72, standard deviation =0.31; ). More important, there was a significant interaction between test and group [F(2,410)=3.29; P=0.038; η2=0.016]. Further analysis showed that compared with the pretest (mean =6.30, standard deviation =4.78) and midtest (mean =5.64, standard deviation =4.38) results, there was a significant decrease in Arousal scores in post-test (mean =4.84, standard deviation =4.25) for the experimental group, whereas the control group showed no significant change ().
Figure 1 Arousal scores of posttraumatic stress disorder change with the course of test across group.
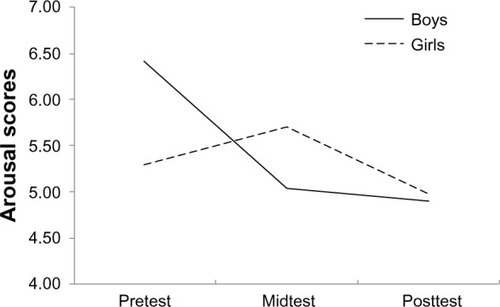
Similarly, a significant interaction between test and sex was found [F(2,410)=6.13; P=0.002; η2=0.019], and the Arousal scores in post-test (mean =4.98, standard deviation =4.39) were significantly lower than in midtest (mean =5.71, standard deviation =4.14) for girls, whereas for boys, post-test (mean =4.90, standard deviation =4.24) showed little change compared with midtest (mean =5.04, standard deviation =4.36); both were significantly lower than pretest (mean =6.42, standard deviation =4.59) in boys ().
Figure 2 Arousal scores of posttraumatic stress disorder change with the course of test across sex.
Summary
It is noted therefore that after 30 days of calligraphy treatment, the experimental group’s stress reduction was highly significantly different from that of the control group, bringing these children’s Intrusion and Arousal scores much lower than their baseline measures. The control group showed some decrease as well, possibly because of a natural mental readjustment of the participants in the aftermath of the tragic event. We also found that among the Arousal scores, which is an important symptom of PTSD, there was significant interaction between test and sex, indicating that sex differences may exist for calligraphy treatment.
In sum, this experiment has provided the first evidence of the promising application of calligraphy therapy as an indigenous and effective means of alleviating PTSD symptoms and behavioral conditions of earthquake victims.
Experiment 2: SC and a second CRIES-13 assessment
Method
Participants
Eighty fourth- and fifth-grade primary children participated in the second experiment. They were screened and selected from an initial pool of 700 children in two district primary schools in the earthquake regions. The participants were balanced for age, sex, and random assignment of groups. The experimental group had 41 children with a mean age of 10.52±1.16 years and was given calligraphy training 1 hour a day for a consecutive 30 days. CRIES-13 (r=0.79; P<0.001) was adopted to assess the treatment effects before, at halfway through, and after the training course. The control group had 39 children with a mean age of 10.54±1.15 years and was similarly assessed, but without calligraphy training. Both groups also had Salivary Collection assessment. The instrument, the CRIES-13, and other experimental conditions were the same as in experiment 1. The description of the participants is presented in .
Salivary collection
The salivary cortical measurement was taken for both the experimental and control groups as a new dependent variable. The procedure entailed inserting a cotton ball under the subject’s tongue for 5 minutes, followed by taking a 2 mL saliva sample by syringe and storing it in a −20°C refrigerator. The sample was refrozen for 24 hours and centrifuged at 3,000 rpm for final collection of the specimen. The specimen was analyzed with a Gamma Coat™ Cortisol I RIA Kit (R&D Systems, Minneapolis, MN, USA) at the State Key Laboratory of Brain and Cognitive Science, Chinese Academy of Sciences, Beijing, People’s Republic of China. The treatment duration was 30 consecutive days, with the SC sample taken 3 times: before the experiment for the pretest, 2 weeks later for midtest, and within 3 days after the treatment for the posttest. The timing of SC sample collection was set at 4 pm on Fridays. The CRIES-13 was administered before the treatment and 3 days after the conclusion of the treatment for both groups. The children in the control group participated in the regular calligraphy class.
Results
Data were submitted to a 3×2×2 repeated measures analysis of variance, in which the test (three levels: pretest, midtest, and post-test) served as the within-subjects variable, whereas the group (two levels: experimental group and control group) and sex (two levels: boys and girls) were the between-subjects variables.
When SC measures were analyzed, we observed that SC measures revealed a significant main effect of test [F(2,196)=17.76; P=0.000] as well as group [F(1, 98)=14.17; P=0.000; η2=0.153]. Further analysis showed that the SC level in post-test (mean =10.99, standard deviation =2.53) is much lower than in pretest (mean =11.99, standard deviation =2.48) and midtest (mean =13.29, standard deviation =2.90) and that the SC level in the experiment group (mean =11.64, standard deviation =0.21) is significantly lower than in the control group (mean =12.97, standard deviation =0.28; ). This main effect is qualified by a significant test × group interaction [F(2,196)=8.47; P=0.029; η2=0.080]. In comparison with pretest (mean =13.34, standard deviation =2.88) and midtest (mean =11.61, standard deviation =2.17), there was a significant decrease of total scores in post-test (mean =9.99, standard deviation =1.81) for the experimental group, whereas the control group showed no significant change ().
Figure 3 Salivary cortisol (SC) measures change with the course of test across group.
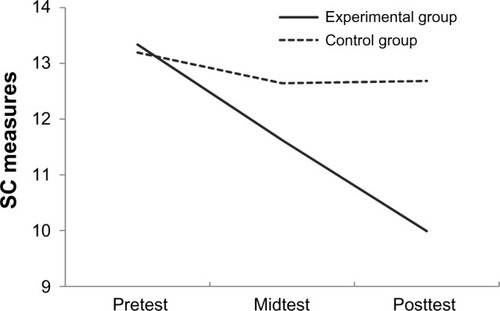
Table 3 Average (standard deviation) measures on salivary cortisol by condition
Summary
The results from this experiment have not only lent support and confirmed the validity of the treatment effect of calli graphy practice in the area of CRIES-13 behaviors in children but have also broken new ground in its therapeutic application at a deeper level (ie, the SC changes as an index of severe stress disorder because of the earthquake experiences). These double, simultaneous outcomes mark a significant new step for calligraphy therapy as a complementary approach of clinical and rehabilitative psychology. The SC findings are most welcoming in showing the progressive nature of this graphonomic treatment as a function of the progress of the training. This observation adds to the rigor and scientific strength of the treatment. Some discussion of the theoretical and empirical foundations of calligraphy treatment deserves closer attention and analysis.
Discussion
The findings of these two experiments are highly illuminating, showing the effectiveness of calligraphy treatment for the PTSD hyperarousal symptoms of the trauma-exposed children from China’s major 2008 earthquakes. A significant decrease in both the CRIES-13 scores, and the SC as a result, has been disclosed. The significance of this result lies in observing, for the first time, the positive effect of calligraphy training in reducing the PTSD symptoms of natural disaster child survivors.
Findings from both self-reported PTSD symptoms and physiological data indicate a consistent lowering of physical arousal conditions as a result of brush writing. We attribute these observed states of emotional stabilization, relaxed alertness, and mindful quiescence to the fundamental changes embedded in the act of brush writing. The physical changes reported are similar to those obtained in studies on meditation.Citation46 Because of this, we regard calligraphic writing as a graphic form of meditation involving rich cognitive and linguistic processing, which is not part of other forms of meditation practice. The latest confirmation of this effect is the Heart Rate Variability study, showing a progressive coherence of the subject’s heart rate with respiration through calligraphy training.Citation47 The finding of a reduction in hyperarousal symptoms among trauma-exposed children echoed past results of calligraphy treatment for facilitating visual attention, as well as a reduced state of hyperactivity among ADHD and autistic children.Citation20,Citation48 In examining the physiological effects of calligraphy training, we have found that the practitioner’s heart rate, blood, blood pressure, and respiration are generally reduced as a result of this practiceCitation49 in various practitioner categories. The associated emotional stability and relaxation have been observed with patients of mental disorders, hypertension and diabetes students, executives and administrators, and children with autism and ADHD.Citation50 The studies presented here have highlighted an alternative model of behavioral treatment of children with various mental problems.
No sex difference was found in either pre- or post-training self-report PTSD symptoms, which suggests the calligraphy treatment has an equivalent effect on boys and girls. This finding is consistent with the result from a meta-analysis on sex differences in treatment effectiveness for PTSD patients.Citation51 However, the studies in the meta-analysis were primarily focused on adult patients, and the trauma type and treatments were heterogeneous. Much remained unknown for childhood victims of natural disaster. In the present study, a significant sex–time interaction was found at the second measurement: a significant decline in symptom severity was reported in boys but not girls during the treatment. This indicated a sex difference in the trajectory of recovering from PTSD symptoms, suggesting that girls would benefit from treatment more slowly than boys but that they would reach the same outcome if the treatment persists. Although no study has reported sex difference in treatment trajectory among children, some researchers found a slower decline in post-traumatic stress symptoms associated with physical injury in girls than in boys in the natural recovery,Citation52 and a lower rate of resilience in girls than boys.Citation53 However, that no sex difference was found in the cortisol changes over time suggests a consistent decline of stress level accompanying the course of calligraphy treatment. This inconsistency between self-report data and physiological data may suggest that factors other than stress-related hormonal changes may contribute to the sex difference in resilience to trauma.
The calligraphy treatment showed no effect on Intrusion and Avoidance symptoms, which reflect the cognitive aspects of PTSD. According to cognitive theories, intrusion is the result of trauma memory that has not been integrated into the cognitive schema.Citation54 In contrast, trauma-exposed individuals are hypervigilant to threat and trauma-related cues in the environmentCitation55 but strategically avoid the cues as a coping mechanism.Citation56 However, persistently avoiding trauma-related triggers may prevent the trauma memory from integrating into the schema, which leads to maintenance of PTSD symptoms. Thus, one of the main purposes of cognitive treatments of PTSD is to integrate the fragments of trauma memory into the cognitive schema.Citation57 Because the emphasis of calligraphy treatment is attention and relaxation, the traumatic memory and cognitive modification have not been processed. To make the most of calligraphy treatment, a combined cognitive therapy is recommended.
In a summary, our past research has been conducted in the context of a general system of perceptual motor control behavior,Citation58 as well as a cybernetic theory of handwriting and feedback regulation.Citation59 This body of work, along with our recent principles of character geometric specificity for calligraphy production, has given credence to calligraphy therapy as an evidence-based system of treatment and rehabilitation. In addition, this body of work offers valid support to the theoretical, empirical, and treatment foundations of calligraphy therapy. This research, as a whole, predicted positive and effective treatment benefits for trauma-exposed pupils, in the case of the present study, in reducing hyper-arousal symptoms. The results arising from this study have indeed supported our stated predictions. The demonstration of changes in SC as a direct effect of calligraphy training makes its first contribution toward the relief of the children’s symptoms in a neurochemical level of analysis.
The overall results of this study have lent convincing support to the predictions of calligraphy treatment in improving and changing the common post-traumatic hyperarousal symptoms in a sample of trauma-exposed children. This global outcome is further backed and confirmed by the measure of the progressive change and reduction of SC throughout the treatment. This main finding indicates a strengthening and enhancement of the participants’ immunity system as a positive response to calligraphy treatment. Overall, we recognize successful calligraphy treatment as an effective, validated, and culturally congruent system of intervention.
Acknowledgments
Our work was supported by the Knowledge Innovation Program of the Chinese Academy of Sciences (KSCX2-EW-J-8-j).
Disclosure
The authors report no conflicts of interest in this work.
References
- Chinese Information Office of the State CouncilWenchuan earthquake has confirmed 69,227 people were killed2008 http://news.sina.com.cn/c/2008-09-25/183514499939s.shtmlAccessed August 1, 2010
- ViewegWVJuliusDAFernandezABeatty-BrooksMHettemaJMPandurangiAKPosttraumatic stress disorder: clinical features, pathophysiology, and treatmentAm J Med2006119538339016651048
- American Psychiatry AssociationDiagnostic and Statistical Manual of Mental Disorders4th edWashington, DCAmerican Psychiatric Association1994
- SalmonKBryantRAPosttraumatic stress disorder in children. The influence of developmental factorsClin Psychol Rev200222216318811806018
- KirschVWilhelmFHGoldbeckLPsychophysiological characteristics of PTSD in children and adolescents: a review of the literatureJ Trauma Stress201124214615421438015
- EksiABraunKLOver-time changes in PTSD and depression among children surviving the 1999 Istanbul earthquakeEur Child Adolesc Psychiatry200918638439119221855
- GoenjianAKPynoosRSSteinbergAMPsychiatric comorbidity in children after the 1988 earthquake in ArmeniaJ Am Acad Child Adolesc Psychiatry1995349117411847559312
- GiannopoulouIStrouthosMSmithPDikaiakouAGalanopoulouVYuleWPost-traumatic stress reactions of children and adolescents exposed to the Athens 1999 earthquakeEur Psychiatry200621316016616529912
- HsuCCChongMYYangPYenCFPosttraumatic stress disorder among adolescent earthquake victims in TaiwanJ Am Acad Child Adolesc Psychiatry200241787588112108814
- WangLLongDLiZArmourCPosttraumatic stress disorder symptom structure in Chinese adolescents exposed to a deadly earthquakeJ Abnorm Child Psychol201139574975821484333
- SriramKRodriguez-FernandezMDoyleFJ3rdModeling cortisol dynamics in the neuro-endocrine axis distinguishes normal, depression, and post-traumatic stress disorder (PTSD) in humansPLoS Comput Biol201282e100237922359492
- CharneyDSPsychobiological mechanisms of resilience and vulnerability: implications for successful adaptation to extreme stressAm J Psychiatry2004161219521614754765
- MorrisMCCompasBEGarberJRelations among posttraumatic stress disorder, comorbid major depression, and HPA function: a systematic review and meta-analysisClin Psychol Rev201232430131522459791
- MeewisseMLReitsmaJBde VriesGJGersonsBPOlffMCortisol and post-traumatic stress disorder in adults: systematic review and meta-analysisBr J Psychiatry200719138739217978317
- ParisJJFrancoCSodanoRSex differences in salivary cortisol in response to acute stressors among healthy participants, in recreational or pathological gamblers, and in those with posttraumatic stress disorderHorm Behav2010571354519538960
- HankinBLBadanesLSAbelaJRWatamuraSEHypothalamic-pituitary-adrenal axis dysregulation in dysphoric children and adolescents: cortisol reactivity to psychosocial stress from preschool through middle adolescenceBiol Psychiatry201068548449020497900
- KaoHSRThe visual-spatial features of Chinese characters and a psychogeometric theory of Chinese character writingKaoHSRChinese Calligraphy TherapyHong KongHong Kong University Press2000 Chinese
- GuoNFKaoHSRLiuXCalligraphy, hypertension and the type-A personalityAnn Behav Med200123S159
- KaoHSRDingBKChengSWBrush handwriting treatment of emotional problems in patients with Type II diabetesInt J Behav Med20007S150
- KaoHSRShufa: Chinese calligraphic handwriting (CCH) for health and behavioural therapyInt J Psychol2006414282286
- XuMKaoHSZhangMLamSPWangWCognitive-neural effects of brush writing of chinese characters: cortical excitation of theta rhythmEvid Based Complement Alternat Med2013201397519023533532
- BrownKWRyanRMThe benefits of being present: mindfulness and its role in psychological well-beingJ Pers Soc Psychol200384482284812703651
- LutzASlagterHADunneJDDavidsonRJAttention regulation and monitoring in meditationTrends Cogn Sci200812416316918329323
- KaoHSRZhuLChaoAAChenHYLiuICYZhangMLCalligraphy and meditation for stress reduction: an experimental comparisonPsychol Res Behav Manag20147475224611024
- LutzAGreischarLLRawlingsNBRicardMDavidsonRJLong-term meditators self-induce high-amplitude gamma synchrony during mental practiceProc Natl Acad Sci U S A200410146163691637315534199
- TerayamaTZen Brushwork: Focusing the Mind with Calligraphy and PaintingTokyoKodansha2004
- YangXLLiHHHongMHKaoHSThe effects of Chinese calligraphy handwriting and relaxation training in Chinese Nasopharyngeal Carcinoma patients: a randomized controlled trialInt J Nurs Stud201047555055919945106
- SchellTLMarshallGNJaycoxLHAll symptoms are not created equal: the prominent role of hyperarousal in the natural course of posttraumatic psychological distressJ Abnorm Psychol2004113218919715122939
- MarshallGNSchellTLGlynnSMShettyVThe role of hyperarousal in the manifestation of posttraumatic psychological distress following injuryJ Abnorm Psychol2006115362462816866603
- BrooksJSScaranoTTranscendental meditation in the treatment of post-Vietnam adjustmentJ Counsel Dev1985643212215
- PhillipsKMAntoniMHLechnerSCStress management intervention reduces serum cortisol and increases relaxation during treatment for nonmetastatic breast cancerPsychosom Med20087091044104918842742
- FanYQTangYFengSModerating effects of mind-body therapy on PTSD victims’s changes in heart rate and salivary cortisolChina J Clin Rehab2006463133 Chinese
- VujanovicAANilesBPietrefesaASchmertzSKPotterCMMindfulness in the treatment of posttraumatic stress disorder among military veteransProf Psychol: Res Pract20114224
- MatchimYArmerJMStewartBREffects of mindfulness-based stress reduction (MBSR) on health among breast cancer survivorsWest J Nurs Res2011338996101620956583
- SmithBWOrtizJASteffenLEMindfulness is associated with fewer PTSD symptoms, depressive symptoms, physical symptoms, and alcohol problems in urban firefightersJ Consult Clin Psychol201179561361721875175
- WaeldeLCUddoMMarquettRA pilot study of meditation for mental health workers following Hurricane KatrinaJ Trauma Stress200821549750018956453
- SpeckensAEEhlersAHackmannARuthsFAClarkDMIntrusive memories and rumination in patients with post-traumatic stress disorder: a phenomenological comparisonMemory200715324925717454662
- ZoccolaPMDickersonSSAssessing the relationship between rumination and cortisol: a reviewJ Psychosom Res20127311922691553
- TacónAMMcCombJMindful exercise, quality of life, and survival: a mindfulness-based exercise program for women with breast cancerJ Altern Complement Med2009151414619769475
- KaoHSRGaoDGWangMQCheungHYChiuJChinese calligraphic handwriting: treatment of cognitive deficiencies of Alzheimer’s disease patientsAlzheimer’s Rep20003281287
- KwokTCBaiXKaoHSLiJCHoFKCognitive effects of calligraphy therapy for older people: a randomized controlled trial in Hong KongClin Interv Aging201126927322087066
- ChiuMLKaoHSRHoSMYThe efficacy of Chinese calligraphic handwriting of stroke patients: A multiple cases studyKorczynADProceedings of the 2nd International Congress on Vascular DementiaSalzburg, Austria2002
- LeungGTFungAWTamCWExamining the association between late-life leisure activity participation and global cognitive decline in community-dwelling elderly Chinese in Hong KongInt J Geriatr Psychiatry2011261394721157849
- TrickeyDSiddawayAPMeiser-StedmanRSerpellLFieldAPA meta-analysis of risk factors for post-traumatic stress disorder in children and adolescentsClin Psychol Rev2012322122138 Chinese22245560
- WuKKZhangYQDevelopment and Application of PTSD and IES in survivors after disastersAdv Psychol Sci2009173495498
- KaoHSRZhuLChaoAAChenHYLiuICYZhangMLCalligraphy and meditation for stress reduction: an experimental comparisonPsychol Res Behav Manag20147475224611024
- LamSPWKaoHSRFungMCalligraphy-Guqin for Brain Health and Emotion33rd Annual Meeting and Scientific Sessions of the Society of Behavioral MedicineNew Orleans2012
- KaoHSRCalligraphy therapy: A complementary approach to psychotherapyAsia Pac J Couns Psychother2010115566
- KaoHSRLamP-WRobinsonLYenNSPsychophysiological changes associated with Chinese calligraphyPlamondonRSuenCYSimnerMLComputer Recognition and Human Production of HandwritingSingaporeWorld Scientific1989349381
- KaoHSRChinese Calligraphy TherapyHong KongUniversity of Hong Kong Press2000
- BlainLMGalovskiTERobinsonTGender differences in recovery from posttraumatic stress disorder: A critical reviewAggression Violent Behav201015463474
- Doron-LaMarcaSVogtDSKingDWKingLASaxeGNPretrauma problems, prior stressor exposure, and gender as predictors of change in posttraumatic stress symptoms among physically injured children and adolescentsJ Consult Clin Psychol201078678179321114341
- AlisicEJongmansMJvan WeselFKleberRJBuilding child trauma theory from longitudinal studies: a meta-analysisClin Psychol Rev201131573674721501581
- DalgleishTCognitive approaches to posttraumatic stress disorder: the evolution of multirepresentational theorizingPsychol Bull2004130222826014979771
- McNallyRJCognitive abnormalities in post-traumatic stress disorderTrends Cogn Sci200610627127716697695
- ToddRMCunninghamWAAndersonAKThompsonEAffect-biased attention as emotion regulationTrends Cogn Sci201216736537222717469
- GreyNYoungKHolmesECognitive restructuring within reliving: a treatment for peritraumatic emotional “hotspots” in posttraumatic stress disorderBehav Cogn Psychother2002303756
- KaoHSSmithKUCybernetic television methods applied to feedback analysis of automobile safetyNature196922251902993005778410
- KaoHSRSmithKUKnutsonRAn experimental cybernetic analysis of handwriting and penpoint designErgonomics196917453458