
Abstract
Objective
This study aims to apply the virtual radial arm maze (VRAM) task to find spatial working memory and reference memory impairments in patients of amnestic mild cognitive impairment (aMCI) and Alzheimer’s disease (AD). Spatial memory functions between aMCI converters and nonconverters are also compared using VRAM results.
Methods
We assessed the spatial memory in 20 normal controls, 20 aMCI, and 20 mild AD subjects using VRAM. The Mini-Mental State Examination, Clinical Dementia Rating scale, and other neuropsychological tests were given to the subjects in conjunction with the VRAM test. Scores in working memory errors and reference memory errors were compared among the three groups using repeated measures analysis of variance. In addition, aMCI patients were followed-up after 5 years and surveyed for AD conversion rate.
Results
In AD patients, both spatial working and reference memory were impaired. However, in aMCI subjects, only spatial reference memory was impaired. Significant spatial reference memory impairment was found in the aMCI converter group when compared to the nonconverter group.
Conclusion
Spatial working memory is less impaired in aMCI while reference memory is similarly damaged in AD. In aMCI patients, more severe spatial reference memory deficit is a neuropsychological marker for AD conversion. VRAM may be well utilized in humans to assess spatial memory in normal aging, in aMCI, and in AD.
Introduction
In most cases, Alzheimer’s disease (AD) is preceded by a prodromal stage and amnestic mild cognitive impairment (aMCI) in which an individual’s memory is impaired to a greater degree than expected given the individual’s age, sex, and educational background, while the individual’s ability to perform the activities of daily living is preserved and the criteria for dementia are not met. A previous study reported that the conversion rate of aMCI to AD is 10%–15% annually, compared with 1%–2% among normal elderly individuals.Citation1
Structural and functional abnormalities in the hippocampus have been documented in patients with aMCI and AD.Citation2,Citation3 Atrophy of hippocampal formation is a strong risk factor of AD progress.Citation4 As the hippocampus plays a crucial role in spatial memory and navigation,Citation5 it is generally accepted that patients with aMCI or AD show impairments in spatial orientation,Citation6 navigation,Citation7 and visuospatial short-term memory.Citation8 Such deficits may lead to failure in navigating and remembering places.
However, it is difficult to measure spatial memory deficits in real situations with a classic neuropsychological battery. Several studies utilized virtual reality systems to assess cognitive impairments related to degenerative changes to improve ecological validity.Citation7,Citation9–Citation12 Previous studies reported that virtual navigation performance was impaired in aMCI and AD and that virtual environments provide valid assessments of navigation skills that are comparable to those required in real world navigation.Citation9,Citation13 Moreover, examination of spatial memory can be effectively performed using virtual systems, resulting in enhanced diagnostic power compared with classic neuropsychological testing.Citation14
The virtual radial arm maze (VRAM), virtual Morris water maze, and virtual route learning are tools commonly used in assessments of spatial memory.Citation15–Citation17 The VRAM, a human analogue of the radial arm maze (RAM) test used extensively to test spatial memory in small animals such as rodents,Citation18,Citation19 has two merits to examine spatial working memory and reference memory simultaneously when compared to the virtual Morris water maze and virtual route learning. The current VRAM design uses a computer–human interface, and human subjects use monitors and joysticks to control their movements inside the virtual reality in which the classic design of RAM is implemented. The VRAM has been successfully used in human studies on sex differences in these two types of spatial memory,Citation20 on working memory load in elderly patients,Citation21 and on hippocampal activity.Citation22
The hippocampus and prefrontal cortex of rodents and humans are involved in spatial navigation.Citation22,Citation23 Evidence from experiments with rodents indicates that memory functions involve information processing in the hippocampus and prefrontal cortex.Citation24,Citation25 However, spatial reference and working memory systems use different neuronal networks;Citation26 the prefrontal cortex is involved in working memory, whereas the hippocampal region is involved in reference memory.Citation12 A study in rodents also reported that deficits in the two types of spatial function have different patterns; reference memory deficits are common as a function of aging, but working memory deficits are not.Citation27 As in rodents, spatial reference memory in humans is mediated by the hippocampus,Citation28 whereas spatial working memory is more closely related to the frontal cortex.Citation29,Citation30
This study aimed to identify spatial memory impairment in patients with aMCI and AD using the VRAM and to determine whether the VRAM can differentiate between the two types of memory deficits. Beginning with the onset of aMCI, patients with AD typically show early changes in the hippocampus.Citation31 Thus, we expected that both aMCI and AD patients would have reference memory deficits attributable to hippocampal atrophy.Citation32 AD pathology is also associated with spatial working memory problems as measured by the Spatial Span Backward test.Citation31 This may be related to the fact that prefrontal cortical atrophy is more prominent in AD than in aMCI.Citation33 Therefore, we expected that spatial reference memory deficits would appear in both aMCI and AD patients and working memory loss would be found only in patients with AD. We also followed aMCI participants for 5 years to find a virtual navigation predictor of progression from aMCI to AD.Citation1
Methods
Subjects
Sixty older adults were recruited from the local community. The Institutional Review Board at Boramae Hospital approved the study protocol. All procedures in this study were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 1983. Eligibility criteria for participation were 1) age 60 years or older and 2) no known history of head trauma, brain tumor, stroke, mental retardation, or any severe medical, neurological, or psychiatric illness affecting cognitive functioning other than AD. Patients with mild depression were included only if their scores on the short form of the Geriatric Depression Scale were lower than 10.Citation34 All participants were assigned to one of three groups: normal control (NC) (n=20), aMCI (n=20), or mild AD (n=20). The demographic characteristics of each group are presented in .
Table 1 Mean demographic data and scores (SD) of the Mini-Mental State Examination of the normal control, amnestic mild cognitive impairment, and Alzheimer’s disease groups
The NC group had no memory complaints, scored in the normal range on standardized neuropsychological tests, and had no neurological abnormalities. aMCI patients met the criteria for aMCI initially proposed by Petersen:Citation1 1) memory complaints, preferably corroborated by an informant; 2) memory impairment relative to age- and education-matched healthy individuals (below 1.0 standard deviation); 3) intact general cognitive functioning; 4) largely intact activities of daily living; and 5) absence of dementia. AD was diagnosed according to the National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association criteria for probable AD,Citation35 and subjects were mildly demented, scoring 0.5 or 1 on the Clinical Dementia Rating (CDR) global scale.Citation36
After 5 years, in eleven of the 20 aMCI patients, AD was newly developed (aMCI converters), seven still had aMCI (aMCI nonconverters), and two were lost to follow-up.
Neuropsychological assessments
A trained psychologist administered the Korean Mini-Mental State Examination (MMSE),Citation37,Citation38 CDR, and neuropsychological memory and visuospatial tests to the subjects. Visuospatial construction and memory were assessed with the simplified Rey figure test (SRFT).Citation39 Working memory was examined using the Spatial Span Forward and Backward tasks to validate the VRAM. A trained psychiatrist made the clinical diagnoses in consultation with a consensus conference at which the clinical and neuropsychological data were reviewed.
VRAM task
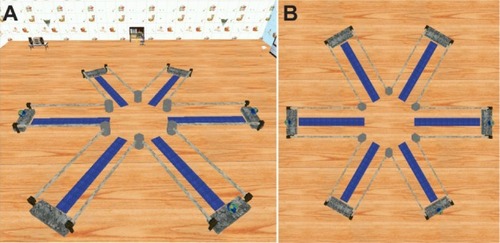
An original virtual maze program, which included a maze with six arms and “treasures” at the distal end of three arms, was used as the VRAM test tool (). Participants were told that they were in a virtual room with six arms extending from a middle area. The virtual room had various colored objects and visual cues to indicate the relative directions, and the room remained unchanged throughout each trial. Although participants were instructed to find the three treasures as quickly as possible, no time limit was imposed. After discovering all three treasures, the trial ended, and participants returned to the center of the maze to begin the next trial. Five trials were conducted, and the intertrial interval was 10 seconds. The same configuration of rewarded arms was used for all participants. This test measured working memory errors by the number of times a subject reentered the same arm; reference memory errors were measured by the number of times a subject reentered the arms with no rewards.Citation22 Distance traveled and time required to find all rewards during each trial were also recorded.
Figure 1 Virtual radial arm maze test.
Test administration
All subjects were visually and verbally informed that the test would occur in a virtual room. The apparatus for the VRAM consisted of a desktop computer with a color monitor and a joystick. All participants were instructed to use the joystick to navigate the virtual environment.
All subjects participated in pretrial training before the task. Trained psychologists who did not participate in neuropsychological tests guided the subjects to ensure they were completely familiar with the virtual environment, the rules of the game, and the manipulation of joysticks. Irrespective of disease severity, all subjects were clearly able to perform the tasks without any problems. The total length of training differed across individuals.
Five years after the VRAM test, the aMCI participants were surveyed and categorized into aMCI converters and aMCI nonconverters. The original VRAM trial results previously gathered were compared between the two groups for any significant group effect.
Statistical analysis
Differences in sex in the three groups were analyzed with chi-square tests. The mean age, years of education, and MMSE scores were compared using analysis of variance (ANOVA) of the three groups. Time latency, distance, number of working memory errors, and number of reference memory errors in the five trials of the VRAM test were compared using repeated measures ANOVA with the Bonferroni adjustment for multiple testing. We used Kendall’s tau-b to analyze the correlation between the VRAM results (working and reference memory errors, time, and distance traveled) and other neuropsychological memory tests to examine the concurrent validity of the VRAM. SPSS for Windows, version 16 (SPSS Inc., Chicago, IL, USA) was used for data analyses. P-values below 0.05 were considered statistically significant.
Results
Subjects
The sample consisted of 60 elderly individuals: 20 with AD, 20 with aMCI, and 20 NC subjects. Demographic data and mean MMSE scores are presented in . The groups had similar mean ages (F=0.6, P=0.53) and sex distributions (P=0.81), but they differed significantly in years of education (F=5.8, P<0.05) and MMSE scores (F=38.6, P<0.05). Post hoc analysis revealed that those in the AD group were less educated and had lower MMSE scores compared with those in the NC and aMCI groups (P<0.05).
VRAM results
Repeated measures ANOVAs () revealed a significant main effect of number of trials on working (F=8.0, df=4, partial η2=0.37, P<0.05) and reference (F=20.0, df=4, partial η2=0.60, P<0.05) memory errors. All three groups committed fewer working and reference memory errors as the trials proceeded. Additionally, we found a significant effect of group on working (F=12.0, df=2, partial η2=0.30, P<0.05) and reference (F=17.7, df=2, partial η2=0.38, P<0.05) memory errors. According to the post hoc analysis, aMCI and NC participants committed a comparable number of working memory errors (P=0.1), but both groups committed fewer working memory errors (P<0.05) than the AD subjects. aMCI subjects committed more reference memory errors than NC subjects (P<0.05) and committed a similar number of reference memory errors (P=0.4) to AD subjects. We observed a significant main effect of trial on distance traveled to find the rewards (F=20.3, df=4, partial η2=0.60, P<0.05); hence, all three groups traveled shorter distances to find the rewards as the trials progressed. A significant main effect of group on distance traveled to find the rewards (F=17.8, df=2, partial η2=0.39, P<0.05) was also observed. Specifically, NC subjects found the rewards after traveling shorter distances than aMCI subjects (P<0.05), and aMCI subjects found the rewards after traveling shorter distances than AD subjects (P<0.05).
Figure 2 Results of virtual radial arm maze test for the normal control, amnestic mild cognitive impairment, and Alzheimer’s disease groups.
Abbreviations: AD, Alzheimer’s disease; aMCI, amnestic mild cognitive impairment; NC, normal control; sec, seconds.
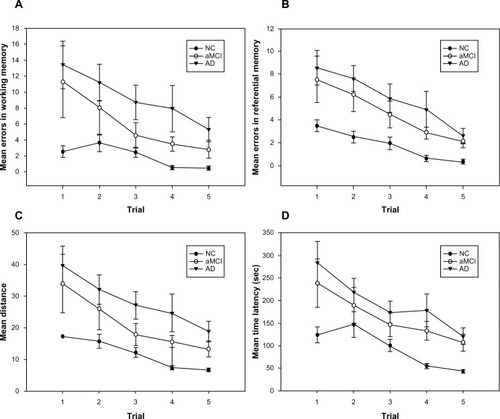
Finally, the data reflected a significant main effect of trial on time latency to find the rewards (F=20.0, df=4, partial η2=0.60, P<0.05). All participants spent less time finding the rewards as the trials proceeded. Moreover, we found a significant group effect of latency (F=15.8, df=2, partial η2=0.36, P<0.05), revealing that NC subjects found the rewards more quickly than aMCI subjects (P<0.05), whereas the time to find the rewards did not differ between aMCI and AD subjects (P=0.18).
VRAM results in the aMCI groups
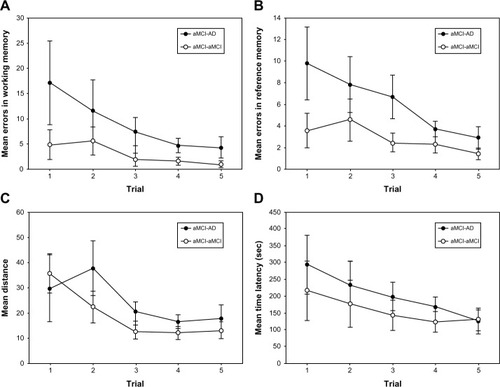
After following patients who were tested 5 years ago, values of the latency, travel distance, and number of working and reference memory errors were compared between the aMCI converter and aMCI nonconverter groups. Despite the small sample, the aMCI converter group made significantly more reference memory errors on the VRAM than the aMCI nonconverter group (, P<0.05). However, the groups did not significantly differ regarding latency (P=0.08), travel distance (P=0.53), and working memory errors (P=0.1).
Figure 3 Results of virtual radial arm maze test for the converted and nonconverted amnestic mild cognitive impaired groups.
Abbreviations: AD, Alzheimer’s disease; aMCI, amnestic mild cognitive impairment; sec, seconds.
Average group differences and relationships to other neuropsychological tests
shows the correlations between number of working and reference memory errors in VRAM trials, and neuropsychological test results of Spatial Span Forward and Backward, SRFT copy, SRFT immediate recall, and SRFT delayed recall. The numbers of working and reference memory errors on the VRAM had significant linear correlations with each other and with scores on all neuropsychological tests except the Spatial Span Forward.
Table 2 Correlations between virtual radial arm maze and neuropsychological tests after controlling for years of education
Discussion
The present study found differences in the spatial memory abilities of NC, aMCI, and AD groups. Participants with aMCI made more spatial reference memory errors than NC subjects, but their spatial working memory seemed intact. AD subjects made more errors in both spatial working and reference memory than did NC subjects. The 5-year follow-up analysis showed that the aMCI converter group made more spatial reference memory errors before developing dementia than the aMCI nonconverter group.
aMCI subjects traveled shorter distances on the VRAM to find the rewards than AD subjects, and were as slow as AD subjects in finding the rewards. presents the results of the VRAM.
Unlike AD, aMCI seems to significantly affect reference memory, but not working memory. Spatial working memory functions have been found to be controlled by the prefrontal cortical area, which is damaged in the progress of AD,Citation32,Citation33 and that spatial reference memory functions are affected by hippocampal atrophy that emerges early in the prodromal aMCI stage.Citation28,Citation31 A Y-maze study showed that spatial working memory may be preserved longer than spatial reference memory in transgenic mice expressing AD pathology.Citation2 Therefore, our results suggest that the loss in spatial reference memory may happen earlier during the aMCI stage, before the spatial significant working memory loss associated with the progress of AD appears. In addition, the current results () indicate that spatial reference memory is significantly more impaired in aMCI patients who develop AD within 5 years than in those who do not. VRAM test results may be used to detect aMCI which can progress on to AD.
aMCI and AD subjects took significantly longer than NC subjects to find the rewards. This impairment in locomotion is reportedly caused by a general deterioration in visual attention and visual processing speed,Citation40 as well as by deficits in global cognitive ability and perceptual speed.Citation41 Patients with aMCI also show attention deficits and process visual stimuli more slowly, although these impairments are less severe in aMCI than in AD.Citation42 AD and aMCI patients are unable to disengage attention and use a visual cue to produce an alerting effect.Citation43 Consistent with previous studies, aMCI and AD subjects showed increased time latency, reflecting a decline in visual stimulus processing and attention. Interestingly, aMCI subjects traveled shorter distances, but with a similar latency when compared to AD patients. This may be indicative of intact spatial working memory in aMCI which helped to prevent reentry into previously entered rooms despite decline in the ability to process visually the landmarks in the VRAM.
The results of the VRAM had linear correlations with those of the Spatial Span Backward and SRFT tests. The statistical significance suggests that the VRAM’s ability to detect spatial memory deficits may be comparable to that of neuropsychological tests.
However, the spatial working and reference memory errors in the VRAM tests were not significantly correlated with those in the Spatial Span Forward task (P>0.05), which assesses passive short-term memory. Whereas the Spatial Span Backward test involves more active attention processes,Citation44 the Spatial Span Forward test assesses only passive attention processes. Previous studies have indicated that passive short-term memories are more resilient and are less likely to be impaired in aMCI and mild AD,Citation31 which is why the Spatial Span Forward test cannot examine spatial impairments in aMCI and AD, and it was not correlated with the VRAM results.
This study has several limitations. Due to the small number of aMCI patients available for follow-up, significant differences in other spatial memory functions between AD converters and nonconverters may not be observed. In addition, although statistically significant, the linear correlations between VRAM results and the neuropsychological tests () were not strong. A larger sample size will improve the quality of statistical data in future investigations. We also assumed that we could completely separate the two different types of spatial memories by counting the number of reentries into emptied arms and selections of wrong arms. However, to test this hypothesis, future research should provide brain imaging analyses to find different brain activation during the occurrence of reference memory and working memory errors.
Conclusion
aMCI subjects differed from AD subjects in their intact spatial working memory, whereas both aMCI and AD subjects demonstrated impaired spatial reference memory, suggesting that the VRAM can help to distinguish among deficits associated with normal aging, aMCI, and AD. Additionally, the VRAM results regarding reference memory errors may be useful as a clinical marker of possible future development of AD among current aMCI subjects, as shown in the 5-year follow-up. Our study shows that the VRAM can be used to examine impairments in spatial working and reference memories in the early stage of AD.
Author contributions
Dr Jun-Young Lee conceived the study, acquired, and interpreted the data. Ms Sooyeon Kho and Ms Hye Bin Yoo analyzed the data and edited the article. Ms Soowon Park made major revisions to the Introduction section. Dr Jung-Seok Choi and Jun Soo Kwon acquired the patients and their clinical reports. The corresponding authors Dr Kyung Ryeol Cha and Dr Hee-Yeon Jung designed the research and the experiments. All authors made substantial contributions to conception and design of the paper, acquisition of data, or analysis and interpretation of data, and drafted the article or revised it for critically important content.
Acknowledgments
The English in this document has been checked by at least two professional editors, both native speakers of English (http://textcheck.com). This study was supported by a grant from the Korea Healthcare technology R&D Project, Ministry for Health and Welfare, Republic of Korea (A070001). The study was conducted at the Seoul National University and Seoul Metropolitan Government – Seoul National University Boramae Medical Center.
Disclosure
The authors report no conflict of interest in this work. No competing financial interests exist.
References
- PetersenRCSmithGEWaringSCIvnikRJTangalosEGKokmenEMild cognitive impairment: clinical characterization and outcomeArch Neurol199956330330810190820
- PennanenCKivipeltoMTuomainenSHippocampus and entorhinal cortex in mild cognitive impairment and early ADNeurobiol Aging200425330331015123335
- MosconiLTsuiWHDe SantiSReduced hippocampal metabolism in MCI and AD Automated FDG-PET image analysisNeurology200564111860186715955934
- KorfESWahlundLOVisserPJScheltensPMedial temporal lobe atrophy on MRI predicts dementia in patients with mild cognitive impairmentNeurology20046319410015249617
- MaguireEABurgessNDonnettJGFrackowiakRSFrithCDO’KeefeJKnowing where and getting there: a human navigation networkScience199828053659219249572740
- PaiMCJacobsWJTopographical disorientation in community-residing patients with Alzheimer’s diseaseInt J Geriatr Psychiatry200419325025515027040
- HortJLaczoJVyhnalekMBojarMBuresJVlcekKSpatial navigation deficit in amnestic mild cognitive impairmentProc Natl Acad Sci U S A2007104104042404717360474
- Alescio-LautierBMichelBFHerreraCVisual and visuospatial short-term memory in mild cognitive impairment and Alzheimer disease: role of attentionNeuropsychologia20074581948196017275041
- PlancherGTirardAGyselinckVNicolasSPiolinoPUsing virtual reality to characterize episodic memory profiles in amnestic mild cognitive impairment and Alzheimer’s disease: Influence of active and passive encodingNeuropsychologia201250559260222261400
- CushmanLASteinKDuffyCJDetecting navigational deficits in cognitive aging and Alzheimer disease using virtual realityNeurology2008711288889518794491
- TippettWJLeeJHZakzanisKKBlackSEMrazRGrahamSJVisually navigating a virtual world with real-world impairments: a study of visually and spatially guided performance in individuals with mild cognitive impairmentsJ Clin Exp Neuropsychol200931444745418686114
- SpiekerEAAsturRSWestJTGriegoJARowlandLMSpatial memory deficits in a virtual reality eight-arm radial maze in schizophreniaSchizophrenia Res20121351–38489
- ZakzanisKKQuintinGGrahamSJMrazRAge and dementia related differences in spatial navigation within an immersive virtual environmentMed Sci Monit2009154CR140CR15019333197
- BellassenVIglóiKde SouzaLCDuboisBRondi-ReigLTemporal order memory assessed during spatiotemporal navigation as a behavioral cognitive marker for differential Alzheimer’s disease diagnosisJ Neurosci20123261942195222323707
- MoffatSDZondermanABResnickSMAge differences in spatial memory in a virtual environment navigation taskNeurobiol Aging200122578779611705638
- AsturRSTaylorLBMamelakANPhilpottLSutherlandRJHumans with hippocampus damage display severe spatial memory impairments in a virtual Morris water taskBehav Brain Res20021321778411853860
- MoffatSDResnickSMEffects of age on virtual environment place navigation and allocentric cognitive mappingBehav Neurosci2002116585185912369805
- GresackJEFrickKMMale mice exhibit better spatial working and reference memory than females in a water-escape radial arm maze taskBrain Res200398219810712915244
- LevinEDKimPMerayRChronic nicotine working and reference memory effects in the 16-arm radial maze: interactions with D1 agonist and antagonist drugsPsychopharmacology (Berl)1996127125308880940
- AsturRSTroppJSavaSConstableRTMarkusEJSex differences and correlations in a virtual Morris water task, a virtual radial arm maze, and mental rotationBehav Brain Res20041511–210311515084426
- BimonteHANelsonMEGranholmACAge-related deficits as working memory load increases: relationships with growth factorsNeurobiol Aging2003241374812493549
- AsturRSSt GermainSABakerEKCalhounVPearlsonGDConstableRTfMRI hippocampal activity during a virtual radial arm mazeAppl Psychophysiol Biofeedback200530330731716167193
- BeckerJTWalkerJAOltonDSNeuroanatomical bases of spatial memoryBrain Res198020023073207417818
- FlorescoSBSeamansJKPhillipsAGSelective roles for hippocampal, prefrontal cortical, and ventral striatal circuits in radial-arm maze tasks with or without a delayJ Neurosci1997175188018909030646
- HasselmoMEA model of prefrontal cortical mechanisms for goal-directed behaviorJ Cogn Neursci200517711151129
- PriorHSchweglerHDuckerGDissociation of spatial reference memory, spatial working memory, and hippocampal mossy fiber distribution in two rat strains differing in emotionalityBehav Brain Res19978721831949331486
- FrickKMBaxterMGMarkowskaALOltonDSPriceDLAge-related spatial reference and working memory deficits assessed in the water mazeNeurobiol Aging19951621491607777133
- BurgessNMaguireEAO’KeefeJThe human hippocampus and spatial and episodic memoryNeuron200235462564112194864
- CourtneySMPetitLMaisogJMUngerleiderLGHaxbyJVAn area specialized for spatial working memory in human frontal cortexScience19982795355134713519478894
- CourtneySMUngerleiderLGKeilKHaxbyJVTransient and sustained activity in a distributed neural system for human working memoryNature199738666256086119121584
- IachiniIIavaroneASeneseVPRuotoloFRuggieroGVisuospatial memory in healthy elderly, AD and MCI: a reviewCurr Aging Sci200921435920021398
- deIpolyiARRankinKPMuckeLMillerBLGorno-TempiniMLSpatial cognition and the human navigation network in AD and MCINeurology2007691098699717785667
- DickersonBCBakkourASalatDHThe cortical signature of Alzheimer’s disease: regionally specific cortical thinning relates to symptom severity in very mild to mild AD dementia and is detectable in asymptomatic amyloid-positive individualsCereb Cortex200919349751018632739
- LesherELBerryhillJSValidation of the Geriatric Depression Scale – Short Form among inpatientsJ Clin Psychol19945022562608014251
- McKhannGDrachmanDFolsteinMKatzmanRPriceDStadlanEMClinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s DiseaseNeurology19843479399446610841
- MorrisJCThe Clinical Dementia Rating (CDR): current version and scoring rulesNeurology19934311241224148232972
- FolsteinMFFolsteinSEMcHughPR“Mini-mental state”. A practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res19751231891981202204
- LeeDYLeeKWLeeJHA normative study of Mini-mental state examination in the Korean elderlyJ Korean Neuropsychiatr Assoc2002413508525
- MilbergWPHebbenNKaplanEThe Boston Process Approach to Neuropsychological AssessmentGrantIAdamsKNeuropsychological Assessment of Neuropsychiatric DisordersNew YorkOxford University Press19965880
- RizzoMAndersonSWDawsonJMyersRBallKVisual attention impairments in Alzheimer’s diseaseNeurology200054101954195910822436
- BackmanLJonesSBergerAKLaukkaEJSmallBJCognitive impairment in preclinical Alzheimer’s disease: a meta-analysisNeuropsychology200519452053116060827
- GorusEDe RaedtRLambertMLemperJCMetsTReaction times and performance variability in normal aging, mild cognitive impairment, and Alzheimer’s diseaseJ Geriatr Psychiatry Neurol200821320421818838743
- TalesASnowdenRJHaworthJWilcockGAbnormal spatial and non-spatial cueing effects in mild cognitive impairment and Alzheimer’s diseaseNeurocase2005111859215804929
- CornoldiCMammarellaICA comparison of backward and forward spatial spansQ J Exp Psychol (Hove)200861567468218421642