
Abstract
Untreated attention-deficit/hyperactivity disorder (ADHD) can lead to substantial adverse social, economic, and emotional outcomes for patients. The effectiveness of current pharmacologic treatments is often reduced, due to low treatment adherence and medication discontinuation. This current systematic literature review analyzes the current state of knowledge surrounding ADHD medication discontinuation, focusing on: 1) the extent of patient persistence; 2) adherence; and 3) the underlying reasons for patients’ treatment discontinuation and how discontinuation rates and reasons vary across patient subgroups. We selected 91 original studies (67 with persistence/discontinuation results, 26 with adherence results, and 41 with reasons for discontinuation, switching, or nonadherence) and 36 expert opinion reviews on ADHD medication discontinuation, published from 1990 to 2013. Treatment persistence on stimulants, measured by treatment duration during the 12-month follow-up periods, averaged 136 days for children and adolescents and 230 days for adults. Owing to substantial study heterogeneity, comparisons across age or medication type subgroups were generally inconclusive; however, long-acting formulations and amphetamines were associated with longer treatment duration than short-acting formulations and methylphenidates. The medication possession ratio, used to measure adherence, was <0.7 for all age groups and medication classes during a 12-month period. Adverse effects were the most commonly cited reason for discontinuation in all studies. Original research studies reported the lack of symptom control as a common discontinuation reason, followed by dosing inconvenience, social stigma associated with ADHD medication, and the patient’s attitude. In summary, although there was a lack of consistency in the measurement of adherence and persistence, these findings indicate that drug adherence and persistence are generally poor among patients with ADHD. Clinicians may be able to help improve adherence and persistence to ADHD treatment by educating caregivers and patients on treatment goals, administering long-acting medications, and following-up with patients to verify if medication is still effective and well-tolerated.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common psychiatric disorder characterized by hyperactivity, impulsivity, and difficulty maintaining sustained attention.Citation1 Approximately 5.3% of children and adolescents are affected by ADHD worldwide,Citation2 of whom 60% continue to demonstrate notable ADHD symptoms throughout life.Citation3
Pharmacologic treatment is a key component of evidence-based care for patients with ADHD and has been shown to be a cost-effective therapeutic option.Citation4 Currently, there are two main classes of medications with proven efficacy for ADHD – stimulants and nonstimulants. Stimulants, such as amphetamines (AMPHs) and methylphenidates (MPHs), have been the mainstay of ADHD pharmacotherapy.Citation5 For patients with contraindications, or those who are averse or nonresponsive to stimulants, nonstimulants, such as guanfacine extended release (GXR), atomoxetine (ATX), and clonidine hydrochloride extended release, are alternative treatment options.
Owing to the chronic nature of ADHD symptoms, patients with ADHD typically require long-term pharmacotherapy. Despite the demonstrated effectiveness of current ADHD medications, treatment discontinuation is fairly common. One-half of all patients fail to adhere to treatment guidelinesCitation6 or discontinue treatment within 2–3 years of starting pharmacologic therapy.Citation7,Citation8 Such behaviors may be associated with suboptimal control of ADHD symptoms,Citation9 increasing the likelihood of serious deleterious effects that can accrue and escalate over time.Citation10 These include social and academic difficulties, behavioral problems such as substance abuse, delinquency, accidental injury,Citation11,Citation12 and poor economic, social, and emotional well-being.Citation12,Citation13 Such consequences impact patients as well as their families and communities.
The decision to discontinue treatment can be associated with a variety of factors, including patient characteristics, patient or caregiver choice, medication-related factors (eg, duration of action, risk–benefit profile, etc), and practitioner-related or health system-related factors.Citation14,Citation15 Although the literature exists on reasons for ADHD treatment discontinuation, a comprehensive review of these studies synthesizing the underlying issues surrounding discontinuation (particularly for specific ADHD populations, medication classes, and geographic locations) could facilitate the design of programs to improve treatment adherence and subsequent patient health outcomes, and would benefit both researchers and providers. This study aimed to meet this need by conducting a systematic literature review of real-world observational studies and review articles of expert opinions on medication discontinuation among patients with ADHD. In particular, the study sought to accomplish three objectives: 1) to explore the extent of patient persistence on (or discontinuation of) ADHD treatment; 2) to examine patient adherence to various ADHD medications; and 3) to evaluate the underlying reasons for patients’ treatment discontinuation. Variations of discontinuation rates, adherence, and reasons for treatment discontinuation were analyzed across subgroups of patients by age group, geographic location, and medication class.
Materials and methods
Systematic literature search
A systematic literature review was performed on October 11, 2013, by searching four main electronic databases via the OvidSPCitation16 interface: MedLineCitation17 (including In-Process and Other Non-Indexed Citations, January 1990–September 2013); EMBASECitation18 (January 1990–September 2013); PsycINFOCitation19 (January 1990–September 2013); and Cochrane Database of Systematic ReviewsCitation20 (January 2005–July 2013). The four sets of search terms used were: disease of interest (terms for “attention- deficit hyperactivity disorder”); selected medication treatments (terms listed in ); treatment discontinuation (terms for discontinuation, adherence, or persistence); and eligible study types (terms for retrospective or observational studies). Publications retrieved from the search were screened using the inclusion and exclusion criteria detailed in , and this review followed the reporting guidelines recommended by Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).Citation21
Table 1 Selection criteria of systematic review
Publications were screened at two levels. At the level I screening, inclusion/exclusion criteria were applied at the title/abstract level. At the level II screening, the full text of each article was reviewed against the selection criteria. The reason for its exclusion was recorded for each article failing level I or level II screening. To ensure complete capture of all relevant studies, the bibliographies of all reviews and meta-analysis articles were examined during level II screening to identify any additional original studies previously not included (via the snowballing technique).Citation22 Reviews and meta-analyses were included for data extraction if they reported expert opinions and/or were not based on original studies. Two researchers conducted the level I and level II screenings independently; a third researcher was consulted to arbitrate disagreements over study inclusions when needed.
Multiple publications (kin studies) arising from the same research study (primary publications) were identified based on the study sample, research team, analytical method, and results, and linked to avoid duplication. Information was extracted from the primary study and, if available, additional information from the kin studies was also extracted and combined with the primary study. Because we sought to understand the nature of all of the available literature on these topics, the scientific quality of the published studies was not assessed in this systematic literature review.
Data extraction
For original research articles meeting the selection criteria, study-level specifics, methodology, and discontinuation data were extracted. Study-level specifics consisted of publication details, study type, data source, participant characteristics, medications of interest, and the geographic location of the study population. Methodology-related data included the patient selection criteria and the time frame for outcome measurement in each specific study. Discontinuation data included definitions of measures, estimates, and reasons (including nonadherence and switching), if available.
For publications reporting expert opinions (reviews, meta-analyses, editorials/commentaries, and treatment guidelines), geographic location, study population, treatment(s) of interest, and reasons and recommendations for medication discontinuation were recorded.
Data synthesis
Data were synthesized for the following three outcomes: 1) persistence/discontinuation; 2) adherence; and 3) reasons for discontinuation (including nonadherence and switching). Persistence was evaluated for patients remaining on therapy and was defined as the time between treatment initiation and discontinuation, while adherence was generally defined based on the proportion of time a patient took a prescribed ADHD medication according to its dosage schedule.
A qualitative summary was constructed for persistence/discontinuation studies based on pharmacy refill records/databases, as well as on patient and parent/caregiver surveys. A quantitative analysis was performed using data that originated from the subset of persistence/discontinuation studies that implemented comparable measure definitions and follow-up periods. For various patient subgroups, pooled estimates of treatment duration were calculated as the weighted average across studies by sample size. These pooled estimates were then compared by patient age group, medication class (stimulants versus nonstimulants), formulation (long-acting [LA] versus short-acting [SA]), and stimulant type (AMPH versus MPH).
A qualitative summary was constructed for the adherence studies (pharmacy refill records/databases, patient and parent/caregiver surveys, and physician assessments) using the level or percentage of patients classified as adherent to ADHD medications. For the subset of adherence studies using comparable measure definitions and follow-up periods, a quantitative analysis was conducted by computing average adherence rates for patient subgroups weighted by sample size. Pooled treatment durations were then compared by age group, medication class, formulation, and stimulant type.
It should be noted that, when interpreting persistence and adherence to medication in the child/adolescent population, drug holidays, which refers to being temporarily off the prescribed medication during nonschool days, should be taken into consideration. Persistence and adherence might be underestimated when their measures were defined without considering drug holidays.
Qualitative summaries were constructed to display the treatment discontinuation reasons extracted from original research and expert opinion articles. Reasons for discontinuation were reported from the patients’, parent/caregivers’, and clinicians’ perspectives and were compared by age group, medication class, and geographic location. The summary encompassed a broad range of discontinuation-related information, including type of discontinuation (permanent or temporary), motivation for switching, and reasons for nonadherent behavior. The reasons for discontinuation were ranked based on reporting frequency across the final set of studies. The ability to conduct quantitative comparisons using these data was limited, owing to differences in discontinuation reason descriptions and heterogeneity across study populations.
Results
Systematic literature search
The initial literature search yielded 1,384 citations. Following the level I screening, 452 publications and an additional eleven studies identified through the citation search were included for full text review. The full text screening identified 127 publications meeting all selection criteria (). The final lists of publications are shown in (original research studies) and (expert opinion articles). Study-level specifics, methodology, and detailed persistence/discontinuation, and/or adherence information were extracted and analyzed for all 127 publications. Details of the number of studies conducted, stratified by age, medication class, and geographic location are summarized in .
Figure 1 PRISMA diagram of the literature selection criteria.
Abbreviations: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; ADHD, attention-deficit/hyperactivity disorder.
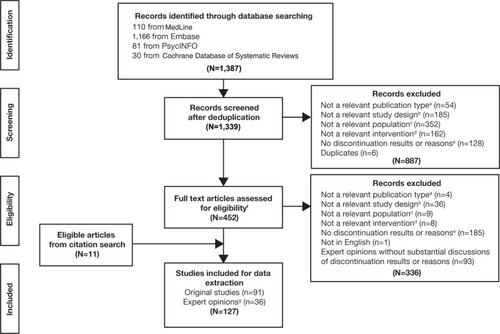
Table 2 Number of studies reporting results for subgroups
Persistence/discontinuation
A total of 67 studies reported findings on persistence/discontinuation: 52 were retrospective database analyses (based on health insurance claims, registries, or patient chart data) and 15 were patient or parent/caregiver surveys.
Database studies
Within the 52 retrospective database studies, three types of persistence measures were reported: discontinuation or continuation/persistence rate; treatment duration; and switching rate. Discontinuation of the index medication was generally defined as a gap, typically 30 days or more, in refill activity after the theoretical end date of the previous prescription.
Considerable heterogeneity existed across methodologies and reported outcomes in the persistence/discontinuation literature, with the most significant differences occurring in the definition of discontinuation, where gap length varied from 15 to 180 days, Citation23–Citation25 and study length varied from 60 days to 6 years.Citation26,Citation27 Given that persistence declines with time, reliable comparisons of discontinuation rate, treatment duration, or switching rate across studies with different study period lengths were not feasible.
Discontinuation or continuation/persistence rate
Thirty-seven studies reported discontinuation or continuation/persistence rates, defined as the proportion of patients who discontinued their index medication or the proportion of patients who continued treatment as prescribed. Of these studies, eleven reported discontinuation rates among combined groups of children, adolescents, and adults, one study focused on adults only,Citation28 and 25 studies focused on children and adolescents only. Three studiesCitation29–Citation31 reported results separately for those patients who were 18 years and under and for those >18 years of age.
Substantial differences in target medication classes existed across the persistence/discontinuation studies. Six studies examined discontinuation rates among nonstimulant users (ATX; guanfacine immediate release [GIR]; GXR; or clonidine users), while 16 studies reported discontinuation rates for stimulants only. Fifteen studies reported rates for both stimulants and nonstimulants. Four studiesCitation8,Citation29,Citation32,Citation33 reported results separately for stimulants and nonstimulants.
ADHD treatment discontinuation rates were reported in ten studies with a follow-up period of 12 months. Discontinuation rates for stimulants ranged from 19.1% for LA stimulant users of all agesCitation29 to 99% for SA MPH pediatric (6–12 years old) users.Citation34 Discontinuation rates for nonstimulants, reported from two studies on the use of ATX, ranged from 26.0% for 6–17 year old Italian patientsCitation33 to 38.3% for 2.5–90 year old Canadians (in Quebec).Citation29
Treatment duration
Thirteen studies reported treatment duration as the time during which patients remained on initial ADHD therapy until they discontinued. Of these, five studiesCitation35–Citation39 () employed the same definition of treatment duration – the number of days that a patient remained on his or her initial therapy during a 12-month follow-up period – and termination, which was defined as a gap of at least 30 days in prescription-filling activity. Of these studies, only four were used to create a pooled estimate (), because two studiesCitation38,Citation39 were kin studies. As Christensen et alCitation38 reported additional results for AMPH, this study was chosen to be used for the analysis of treatment duration. Pooling of persistence estimates was only feasible for the children and adolescents population. Persistence ranged from 93.0 days (for SA stimulants) to 166.5 days (for AMPH). Only one studyCitation38 examined treatment duration among adults, reporting a range from 182.9 days (for MPH) to 252.7 days (for AMPH). The range of treatment duration reported for the overall age group was from 154.3 days (for nonstimulant ATX) to 254.2 days (for stimulants).
Table 3 Studies included in quantitative analysis for persistence
Table 4 Persistence results (reported as mean treatment duration, in days) from quantitative analysis
Switching
Switching to another medication was reported in 19 studies as either the rate of switching or the time to medication switch. Of these, six studiesCitation23,Citation38–Citation42 used a follow-up length of 12 months; the rate of switching in these studies ranged from 3.7% for patients <18 years old (switching from stimulants to nonstimulants)Citation38 to 59% for children aged 6–12 years (switching from SA MPH to an unspecified ADHD medication).Citation23
Patient and parent/caregiver surveys
Fifteen studies used patient or parent/caregiver interviews and surveys to assess persistence on ADHD medication. Of these, one studyCitation43 examined stimulant use among adults, while the remainder focused on ADHD pharmacotherapy among children and adolescents.
Discontinuation or continuation/persistence rates were reported in 13 of the studies. Among children and adolescents, discontinuation rates ranged from 11.1% for 8–18 year old patients, who stopped stimulant use following an average treatment duration of 3.3 years,Citation44 to 96.4% for 4–17 year old Puerto Ricans taking stimulants, and who were observed over a 1-year period.Citation45 Treatment duration was reported in three survey-based studiesCitation46–Citation48 and ranged from 79 days to 2.5 years; however, each study had a different follow-up length. Treatment switching was reported in one parent survey of Taiwanese children; the study found that 57% of patients classified as poor adherents switched from SA to LA MPH.Citation49
Adherence
A total of 26 studies reported adherence results, of which 13 were retrospective database analyses, ten were patient or parent/caregiver surveys, and three were physician surveys.
Database studies
Twelve database studies used health insurance claims data from North American sources; only one study was conducted outside this region.Citation32 Overall, six studies examined adherence in combined populations of children, adolescents, and adults,Citation29,Citation30,Citation38,Citation39,Citation42,Citation50 while the remaining seven focused on adherence among children and adolescents only. Seven studies presented adherence results for both stimulants and nonstimulants, with each reported separately. Five studies assessed adherence to stimulant medications only (AMPH or MPH),Citation24,Citation30,Citation50–Citation52 and one study examined adherence to nonstimulants only (ie, GIR and GXR).Citation53
All studies evaluated adherence as the number of days of medication supplied during a prespecified period. Ten studies defined adherence based on medication possession ratios (MPRs: the ratio of the number of days with medication supply to the total number of days in a defined period), while three studies employed days in possession ratio (DPR),Citation30 annualized prescribed days,Citation54 and proportion of days covered (PDC).Citation42 MPR was reported as a continuous measure of adherence in six studies and as a categorical variable (adherence defined by a given threshold value) in six studies. Of the latter, four studies defined being adherent as having an MPR of >0.8,Citation29,Citation37,Citation39,Citation50 while two employed an adherence threshold of 0.7.Citation51,Citation52
Similar to the persistence/discontinuation studies, the length of study period varied across the 13 database studies, ranging from 3 months to >2 years. The most commonly used study period was 12 months (six studies),Citation32,Citation37–Citation39,Citation42,Citation54 followed by 6 months (three studies)Citation24,Citation30,Citation53 (). As patients’ adherence levels may change over longer study periods, results were interpreted in the context of their observation length.
Table 5 Studies included in quantitative analysis for adherence
A quantitative pooling of MPR results was conducted in which comparable study measures were determined for each of the following groups – children and adolescents, adults, and the combined age group (). Among the six studies measuring adherence during a 12-month period, only two unique studies used the same adherence definition, calculating MPR as the ratio of supply days to the total number of persistent days during the follow-up period.Citation32,Citation38,Citation39 For the three studies using a 6-month period to measure adherence,Citation24,Citation30,Citation53 only two studies used the same MPR definitionCitation30,Citation53 – the ratio of supply days to a fixed postindex period of 180 days (). No pooled results could be estimated using these two studies, however, owing to the lack of a common treatment arm (each study examined a different medication class) ().
Table 6 Adherence results (mean MPR) from quantitative analysis
Children and adolescents
A total of 12 studies reported adherence results for patients aged ≤18 years. For the eight studies in this group using MPR, PDC, or DPR, adherence ranged from 0.28 for treatment-experienced patients receiving SA MPH for 12 months to 0.76 for patients receiving LA MPH for 6 months.Citation24,Citation42 For studies using an MPR cut-off of 0.8, the rate of adherence ranged from 9.8% (for patients using SA stimulants for 12 months) to 64% (for patients receiving stimulants and/or nonstimulants for 12 months).Citation32,Citation37
From the studies using a 12-month period, the pooled MPR for children and adolescents ranged from 0.56 for LA stimulants and AMPH to 0.67 for a nonstimulant (ATX). For the studies using a 6-month period, the pooled MPR ranged from 0.40 for SA stimulants to 0.61 for nonstimulants (GXR and GIR) (). Similar to the persistence analysis, the quantitative analysis for adherence was limited by the small number of studies sharing the same follow-up period and measure definitions.
Adults
Five studies reported adherence results for adults separately, using MPR, PDC, or DPR.Citation29,Citation30,Citation38,Citation39,Citation42 Among the four studies that presented continuous measures of adherence,Citation30,Citation38,Citation39,Citation42 adherence ranged from 0.30 for treatment-experienced patients receiving SA MPH for 12 monthsCitation42 to 0.62 for patients receiving LA AMPH for 12 months.Citation38 Pooling MPR results across adult ADHD studies was not feasible due to a lack of comparability of MPR definitions and study period lengths ().
Patient and parent/caregiver surveys
A total of ten studies conducted surveys and/or interviews to elicit assessments on medication adherence from patients with ADHD and their parents/caregivers. Two studies assessed adherence among adult patients with ADHD,Citation43,Citation55 while the remaining eight focused on child and adolescent populations. Compared with database studies on adherence, patient and parent/caregiver surveys were conducted over a wider geographic area: two in the US;Citation56,Citation57 three in Taiwan;Citation49,Citation58,Citation59 and the remaining five in Norway,Citation43 India,Citation60 Spain,Citation55 Canada,Citation61 and Saudi Arabia.Citation62 Two studies reported combined adherence on both stimulants and nonstimulants,Citation60,Citation62 while the remainder looked only at stimulants. While all ten studies yielded similar adherence trends, multiple differences existed in study design and execution, limiting cross-comparison of results.
Of the ten survey studies, three compared adherence between LA and SA stimulants.Citation43,Citation49,Citation55 Among these three studies, LA stimulants were found to have better adherence (ranging between 74.3% and 97.1%)Citation49,Citation55 than SA stimulants (ranging between 42.9% and 60.0%).Citation43,Citation49 Definitions of adherence varied widely across these studies.
Physician surveys
Three studies used physician-estimated measures for adherence and treating physicians were asked to rate patient adherence on a questionnaire. Definitions of adherence varied widely across all three studies (eg, physicians’ belief on whether patients were consistently compliant;Citation63 identification of patients who were >80% adherent to treatment during weekdays and >50% adherent during weekends and holidays;Citation64 or application of a 6-point scale to rate adherenceCitation65). Thus, adherence rates ranged between 57.1% (African–American youths in the US rated as consistently compliant to stimulants over 2 years)Citation63 and 71.4% (for 6–17 year old western European patients with ADHD evaluated for a minimum of 2 years postdiagnosis).Citation64 As with prior adherence assessments, this analysis was limited by the heterogeneity of methodologies across studies and by small sample sizes.
Reasons for treatment discontinuation
The literature search identified 41 original real-world studies () and 36 expert opinion articles () reporting reasons for treatment discontinuation. Among the 41 original studies, 30 (73%) reported reasons for discontinuation, seven (17%) reported reasons for nonadherence, and seven (17%) reported reasons for switching. Among the 36 expert opinion articles, 19 (53%) reported reasons for discontinuation, while 24 (67%) reported reasons for nonadherence, along with strategies to improve adherence. The following analysis of the reasons for discontinuation encompassed a broad range, including the type of discontinuation (permanent discontinuation of a medication or temporary discontinuation, such as a drug holiday), motivation for switching, and reasons for nonadherent behavior.
Reasons for discontinuation from original research studies
The most common reasons for discontinuing ADHD medications were adverse effects (reported in 30 out of 41 studies) and ineffective symptom control/suboptimal response (in 27 out of 41 studies) (). The studies were classified by age group and then analyzed by medication class, geographic region, and perspective for each age group.
Table 7 Most frequently reported reasons for treatment discontinuation in original studies
Children and adolescents
Thirty-one (76%) studies focused on reasons for discontinuing treatment among children and adolescents. The two most frequently reported discontinuation reasons for children and adolescents were adverse effects and treatment ineffectiveness/suboptimal response (each reported in 21 out of 31 studies). Children and adolescents also frequently discontinued treatment due to poor adherence, parent/caregiver’s decision to discontinue, and feeling that treatment was not needed due to symptom relief. Other reported reasons included patient attitude/dislike of medication, inconvenience of dosing, and the social stigma associated with ADHD and psychiatric medication, all of which are relevant in a school environment and might potentially explain children and adolescents’ difficulty remaining on the medication.
Discontinuation reasons for children and adolescents treated with stimulants were extracted from 18 studies. The frequently cited reasons were: adverse effects; treatment ineffectiveness/suboptimal response; and poor adherence (each reported in more than five out of 18 studies). Other factors – such as symptom control, parent/caregiver’s decision to discontinue, dislike of medication, and dosing inconvenience – were reported less frequently. Discontinuation reasons for children and adolescents treated with nonstimulants were detailed in only four studies.Citation66–Citation69 All four of these studies cited treatment ineffectiveness/suboptimal response, three cited adverse effects, and one cited poor adherence to treatment as reasons for discontinuation. For both medication classes, patient attitude was also a reason for discontinuation, although it was not frequently reported. For children and adolescents living in North America (ten studies), the primary reason for discontinuation was experiencing adverse effects (reported in seven out of ten studies), followed by treatment ineffectiveness/suboptimal response, dislike of medication, symptom relief, and the parent/caregiver’s decision to discontinue (each reported in more than two out of ten studies). In Europe (15 studies), treatment ineffectiveness/suboptimal response was the main reason for discontinuation (reported in 14 out of 15 studies), followed by adverse effects, poor adherence, symptom control, and dosing inconvenience. Among the studies reporting discontinuation reasons from both the patient’s and the parent/caregiver’s perspective (14 studies), the top three discontinuation reasons were adverse effects, treatment ineffectiveness/suboptimal response, and parent/caregiver’s decision to discontinue (each reported in more than four out of 14 studies). Studies reporting discontinuation reasons from the physician’s perspective (14 studies) recounted the same top two reasons, and added poor patient adherence as the third most common reason.
Five of the 41 discontinuation studies (12%) reported discontinuation reasons for children, adolescents, and young adults who were <23 years old. The overall results for this age group were similar to the patterns observed in children and adolescents, but one study reported lack of information about ADHD as the reason for discontinuation. All five studies focused on stimulants as a class or on MPH only. Owing to the small number of studies, information on other subgroups based on geographic region and perspective was sparse.
Adults
Only five (12%) discontinuation studies covered treatment discontinuation reasons in adults. Of these studies, four focused on stimulants.Citation28,Citation36,Citation43,Citation70 The most common reasons for discontinuation were adverse effects and treatment ineffectiveness/suboptimal response (reported in three out of four studies). Other reported reasons included: achievement of symptom relief; misuse of medication; and the patient’s decision to discontinue medication. Due to the small number of studies, information on other subgroups based on geographic region and perspective were sparse.
Reasons for discontinuation based on expert opinions
The literature review identified 36 expert opinion articles on ADHD treatment discontinuation (). The five most frequently encountered reasons for discontinuation were: adverse effects; dosing inconvenience; social stigma associated with ADHD and psychiatric medication; patient attitude; and treatment ineffectiveness/suboptimal response ().
Table 8 Most frequently reported reasons for treatment discontinuation in expert opinions
When discontinuation reasons were analyzed by age group, children and adolescents (67% of expert opinion studies) were shown to have similar reasons as those for the overall population analysis – adverse effects, dosing inconvenience, patient attitude, social stigma, and patient–physician communication. Commonly cited reasons for discontinuation of stimulant use by children and adolescents (12 studies) included: adverse effects, patient attitude, dosing inconvenience, social stigma, and patient–physician communication (each reported in more than three out of 12 studies). Other reasons included: difficulties in swallowing, disorder-related factors, inadequate monitoring, and treatment ineffectiveness/suboptimal response. No study reported discontinuation reasons for nonstimulants. The top five discontinuation reasons cited by experts in North America (17 studies) were: adverse effects, dosing inconvenience, patient attitude, social stigma, and patient–physician communication. Experts in Europe (five studies)Citation71–Citation75 provided similar reasons, with communication being replaced by inadequate monitoring.
In the only study from North America providing data on adult patients with ADHD (3%),Citation76 adverse effects, social stigma, and dosing inconvenience were listed as the reasons for discontinuation.
In the combined age group (30% of expert opinion studies), six studies focused on stimulant discontinuation,Citation65,Citation77–Citation81 and adverse effects were cited as a discontinuation reason in five of them.Citation77–Citation81 Other reasons given by experts for discontinuing stimulants included: treatment ineffectiveness/suboptimal response; difficulties in swallowing; dosing inconvenience; forgetfulness; and social stigma. No study provided discontinuation reasons for nonstimulants. Adverse effects and treatment ineffectiveness/suboptimal response were consistently referred to as the main reasons for discontinuation in the combined age group of children, adolescents, and adults by experts in North America (seven studies) and Europe (two studies).Citation65,Citation77 Experts from North America also cited: dosing inconvenience; forgetfulness; patient attitude, difficulties in swallowing, and social stigma as reasons for discontinuation. No additional reasons were provided by experts in Europe.
Discussion
This literature review examined persistence and adherence to pharmacologic treatment for ADHD and summarized reasons for treatment discontinuation. Where feasible, the analyses were also stratified across subgroups of patients by age group, geographic location, and medication class. Overall, findings from this study indicate that persistence and adherence to ADHD treatment were generally low and that tolerability was cited as an important reason for treatment discontinuation.
In our review of persistence studies, we observed that there was significant heterogeneity in measures of persistence in studies using patient/caregiver and physician surveys. The issue also affected retrospective database analyses, although to a lesser extent. Most of these studies measured persistence as time to a predefined prescription gap. However, variation in gap lengths and follow-up periods still exists. Rates of treatment persistence varied (between 0.1% and 89.9%), depending on definitions across studies. Despite the variations, higher persistence was observed in patients using LA than SA stimulants.
Definitions of adherence were largely based on the number of days of medication supply. For all three types of studies examined – database studies, patient and parent/caregiver surveys, and physician surveys – adherence measure definitions and follow-up periods varied widely. Most studies reported rates of <80% (or a mean MPR of <0.8),Citation82 indicating a low treatment adherence for the ADHD population. From a societal perspective, it is often important to compare adherence across chronic diseases to help payers and policymakers understand how the adherence and its potential impact in one condition is relative to other similar conditions of interest. In general, adherence to ADHD medication was comparable with estimates reported for other psychiatric (schizophrenia, bipolar disorder)Citation83–Citation85 and nonpsychiatric chronic disorders (hyperlipidemia, diabetes, hypertension, etc)Citation82,Citation86,Citation87 with low adherence. There was no clear evidence that any subgroups (by age or medication class) experienced higher adherence than the others, but, in general, children and adolescents seemed to display higher adherence to nonstimulant than to stimulant medications. Adult adherence rates to various stimulant subcategories,Citation30,Citation38 as measured by MPR, suggest that patients on AMPH may have had higher adherence than those taking MPH; however, more comparable studies are needed to validate these results. The adherence estimates were not influenced by the length of the observation periods (eg, 6 months or 12 months).
This systematic literature review identified numerous reasons for discontinuation of ADHD medication. The most commonly cited reason for discontinuation in original research studies and expert opinion reviews was experiencing some adverse effects from the ADHD medication, regardless of age group, medication class, region, prior treatment status, and reporting perspective. Other reasons for discontinuation were generally similar across these two study types, although some differences were worth noting. Ineffectiveness/suboptimal response was one of the most commonly reported reasons in the original studies, but it was reported less frequently in the expert opinion reviews (although it was still within the top five discontinuation explanations). Similarly, poor adherence was a commonly cited reason in the original studies but not in expert opinion reviews. In contrast, dosing inconvenience and social stigma were among the top five reasons in the expert opinion articles, but they were rarely reported in the original studies. Among adults, symptom relief, concerns over drug misuse, and desire to terminate treatment were frequent motivators. Among children and adolescents, discontinuation often occurred due to symptom relief, but also as a result of poor adherence or the parent/caregiver’s decision to discontinue.
This study observed a number of limitations in the existing body of evidence. First, due to the heterogeneity of study designs and methodology, the scope of a quantitative synthesis of persistence and adherence was limited. In the final quantitative analysis, the selection of eligible articles was narrowed down to a small list of directly comparable studies, which limited the generalizability of our conclusions. Second, the majority of original studies discussed reasons for discontinuation without reporting the proportion of patients affected by each reason; therefore, the rank of discontinuation reasons was based on frequencies of being reported in published studies. It was unclear whether most patients discontinued treatment due to the most frequently reported reasons in the literature. Third, reporting bias may exist as this study did not assess scientific quality of the included studies. Another limitation is related to the adverse effects that were reported to be the main reason for discontinuation across studies. The majority of studies did not provide details on the specific adverse effects that led to discontinuation. Hence, it was not clear if a particular side effect was responsible for a patient’s unwillingness to continue treatment or if generally experiencing some unexpected or unpleasant side effect was sufficient to prompt treatment discontinuation.
Among the 91 original observational studies, only eleven studies reported adherence or discontinuation results for the adult ADHD population and, of these, only five original studies provided information on the underlying reasons for treatment discontinuation. Reasons for discontinuation for adults were provided in only one expert opinion article. This limited information on adherence and persistence in adults is one of the key findings and a call for action for further research to understand the adherence and persistence in the adult population.
Another important aspect of ADHD treatment is drug holidays (scheduled temporary suspensions of pharmacologic treatment). In this analysis, drug holidays were not always considered in studies of children and adolescents with ADHD. Stimulant-treated minors are often advised to take drug holidays during their school holidays or, sometimes, even weekends. Thus, observational database studies using persistence and adherence measures based on commonly used treatment gaps of 30 days may not have taken drug holidays into consideration and may have overestimated the rate of discontinuation – a type of attribution bias. Similarly, database studies measuring adherence as MPRs considered drug holidays as nonadherent days and, therefore, the adherence was underestimated in these studies.
Treatment adjustment is a common phenomenon with ADHD medication, and it should be taken into account when studying adherence and persistence measures. For example, the lower adherence and persistence with SA versus LA stimulants observed in the study could be attributed to a dose titration process. Patients initiating ADHD treatment are often started with low doses and then they titrate to an optimal dosage over time, to maximize medication effectiveness and minimize adverse effects.Citation88,Citation89 SA stimulants may be used for the first titrationCitation90 and, then, if the duration of effect of the optimized dosage is not adequate, patients are typically switched to LA formulations.
Over the past few decades, as ADHD knowledge has advanced, the use of alternative treatment modalities, such as the use of nonstimulants as adjunctive therapies to the core stimulant regimen for patients with suboptimal response to stimulant monotherapy, has increased. As ADHD care has evolved, so too should research into the adherence/persistence of these alternative treatment approaches.Citation91 Two nonstimulants have been approved in the US and Canada for adjunctive use.Citation92,Citation93 However, no observational study was identified in this systematic review evaluating persistence/discontinuation and adherence of nonstimulants as adjunctive therapies; these newer treatment modalities may have different usage and outcome patterns compared with ADHD monotherapy.
Finally, differences in treatment settings (specialist versus generalist care) could not be considered in the scope of this review, as it was not reported consistently. Such differences could influence the reporting of specific discontinuation reasons across varying study types. For example, expert opinions may have been written by experienced child psychiatrists, who are more familiar with pharmacological treatment of ADHD – and in particular with stimulants.Citation94 In addition, they may also have access to multiprofessional teams, facilitating patient management through multimodal treatment options, including continuous psychoeducation, cognitive behavioral therapy, parent training, etc. Thus, these practitioners may be less concerned about ineffectiveness/suboptimal response, as observed in our review. In contrast, physician survey studies could potentially include primary care physicians and pediatricians, who may be less familiar with medical treatment regimens for ADHD and thus may exhibit greater concerns regarding ineffectiveness/suboptimal response of the treatment.
These limitations highlight some gaps in the existing literature and provide possible directions for future research. Studies using comparable definitions and follow-up periods for different subgroups of patients with ADHD are needed to fill the current knowledge gap on the actual rates of adherence to pharmacologic treatment for ADHD. In particular, the current review confirms that treatment patterns in adult ADHD are poorly understood and that further studies are still required to shed light on how disease management approaches in this population will be different from that in children and adolescents. Similarly, systematic comparisons across other subgroups based on medication class (stimulants versus nonstimulants) and formulations (LA versus SA) should also be considered to inform what treatment strategies should be adopted to maintain persistence and adherence for these subgroups. In addition, with the increasing use of adjunctive therapies in the treatment of ADHD, disease management can also benefit from more real-world evidence on the treatment patterns of adjunctive therapies. Large observational studies in which patients are closely followed could provide more reliable estimates of treatment persistence and adherence. Future research that comprehensively collects reasons for discontinuation of ADHD treatment – adjusted for differences in treatment settings, age groups, and medication type – is warranted and will help patients and clinicians choose, monitor, and improve future ADHD treatment regimens.
Conclusion
In this systematic literature review and analysis, persistence and adherence to pharmacologic treatments for ADHD were generally inadequate. The highest persistence was generally observed for patients taking LA stimulants (compared with all other formulations) although further comparative studies are needed. The most common reasons for discontinuation extracted from original studies included adverse effects of ADHD medication, treatment ineffectiveness/suboptimal response, and poor patient adherence to treatment. According to expert opinions, the main reasons for discontinuing ADHD medication were adverse effects of medication, dosing inconvenience, and social stigma associated with ADHD and psychiatric disorders in general. The findings suggest that although efficacy, social factors, convenience, and patient attitude may influence treatment adherence and discontinuation, tolerability remains the most important component to consider when deciding on a treatment regimen. Based on these findings, clinicians may be able to help improve treatment adherence and persistence in this chronic disease by educating caregivers and patients on treatment goals, administering LA medications, and continuing to closely follow-up with patients to verify if medication is still effective and well-tolerated and to ensure medication is switched when there are tolerability issues or lack of symptom control.
Acknowledgments
The authors take full responsibility for the content of this paper, but thank Ana Bozas and Gourab De, employees of Analysis Group Inc., who contributed to the preparation of the manuscript, Caudex Medical (supported by Shire International GmbH, Switzerland) for their editorial assistance and for the collation of comments from the authors and other named contributors, and Antonia Panayi of Shire International GmbH for helpful comments.
Supplementary materials
Table S1 A list of ADHD medications approved in North American and European countries
Table S2 List of included original observational studies and bibliographic information
Table S3 List of included studies with expert opinions and bibliographic information
Disclosure
Research for this invited review was funded by the sponsor, Shire Development, LLC. Although the sponsor was involved in the design, collection, analysis, interpretation, and the information fact checking, the content of this manuscript, the ultimate interpretation, and the decision to submit it for publication were made by each of the authors independently. Vanja Sikirica and Kavita Gajria are employees of Shire and hold stock/stock options in Shire. Shire develops and markets medications to treat psychiatric conditions, including ADHD. Jipan Xie, Mei Lu, Yichen Zhong, and Paige Qin are employees of Analysis Group, Inc., a consultant for Shire. Peter Greven reports no financial conflicts of interest.
References
- American Psychiatric AssociationThe Diagnostic and Statistical Manual of Mental Disorders5th editionArlington, VAAmerican Psychiatric Association2013
- PolanczykGde LimaMSHortaBLBiedermanJRohdeLAThe worldwide prevalence of ADHD: a systematic review and metaregression analysisAm J Psychiatry2007164694294817541055
- BrownTEADHD Comorbidities: Handbook for ADHD Complications in Children and AdultsWashington, DCAmerican Psychiatric Press2009
- WuEQHodgkinsPBen-HamadiRCost effectiveness of pharmacotherapies for attention-deficit hyperactivity disorder: a systematic literature reviewCNS Drugs201226758160022712698
- Subcommittee on Attention-Deficit/Hyperactivity DisorderSteering Committee on Quality Improvement and ManagementWolraichMBrownLBrownRTADHD: clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescentsPediatrics201112851007102222003063
- FerrinMTaylorEChild and caregiver issues in the treatment of attention deficit–hyperactivity disorder: education, adherence and treatment choiceFuture Neurol201163399413
- ZetterqvistJAshersonPHalldnerLLångströmNLarssonHStimulant and non-stimulant attention deficit/hyperactivity disorder drug use: total population study of trends and discontinuation patterns 2006–2009Acta Psychiatr Scand20131281707722943458
- GarbeEMikolajczykRTBanaschewskiTDrug treatment patterns of attention-deficit/hyperactivity disorder in children and adolescents in Germany: results from a large population-based cohort studyJ Child Adolesc Psychopharmacol201222645245823234588
- HongJNovickDTreuerTPredictors and consequences of adherence to the treatment of pediatric patients with attention-deficit/hyperactivity disorder in Central Europe and East AsiaPatient Prefer Adherence2013798799524124351
- AdlerLDNierenbergAAReview of medication adherence in children and adults with ADHDPostgrad Med2010122118419120107302
- MannuzzaSKleinRGBesslerAMalloyPLaPadulaMAdult outcome of hyperactive boys. Educational achievement, occupational rank, and psychiatric statusArch Gen Psychiatry19935075655768317950
- ShawMHodgkinsPCaciHA systematic review and analysis of long-term outcomes in attention deficit hyperactivity disorder: effects of treatment and non-treatmentBMC Med2012109922947230
- KleinRGMannuzzaSOlazagastiMAClinical and functional outcome of childhood attention-deficit/hyperactivity disorder 33 years laterArch Gen Psychiatry201269121295130323070149
- CharachAFernandezREnhancing ADHD medication adherence: challenges and opportunitiesCurr Psychiatry Rep201315737123712722
- WongICAshersonPBilbowACessation of attention deficit hyperactivity disorder drugs in the young (CADDY) – a pharmacoepidemiological and qualitative studyHealth Technol Assess20091350iiiivixxi112019883527
- Ovid MedLine [database on the Internet]Bethesda, MDNational Library of Medicine Available from: http://site.ovid.com/products/ovidguide/premdb.htmAccessed January 11, 2014
- MEDLINE® [database on the Internet]Bethesda, MDNational Library of Medicine Available from: http://www.nlm.nih.gov/pubs/factsheets/medline.htmlAccessed October 21, 2013
- Embase [database on the Internet]Philadelphia PAElsevier Inc Available from: http://www.elsevier.com/online-tools/embase/aboutAccessed January 11, 2014
- PsycINFO [database on the Internet]Washington, DCAmerican Psychological Association Available from: http://www.apa.org/pubs/databases/psycinfo/index.aspx?utm_source=BenchmarkEmail&utm_campaign=0319-part01&utm_medium=emailAccessed January 15, 2014
- Cochrane Database of Systematic Reviews (CDSR) [database on the Internet]LondonThe Cochrane Collaboration Available from: http://www.cochrane.org/editorial-and-publishing-policy-resource/cochrane-database-systematic-reviews-cdsrAccessed January 11, 2014
- MoherDLiberatiATetzlaffJAltmanDGPRISMA GroupPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementPLoS Med200967e100009719621072
- GreenhalghTPeacockREffectiveness and efficiency of search methods in systematic reviews of complex evidence: audit of primary sourcesBMJ200533175241064106516230312
- LageMHwangPEffect of methylphenidate formulation for attention deficit hyperactivity disorder on patterns and outcomes of treatmentJ Child Adolesc Psychopharmacol200414457558115662149
- SanchezRJCrismonMLBarnerJCBettingerTWilsonJPAssessment of adherence measures with different stimulants among children and adolescentsPharmacotherapy200525790991716006269
- McCarthySAshersonPCoghillDAttention-deficit hyperactivity disorder: treatment discontinuation in adolescents and young adultsBr J Psychiatry2009194327327719252159
- JohnstonJAYeWVan BruntDLPohlGSumnerCRDecreased use of clonidine following treatment with atomoxetine in children with ADHDJ Clin Psychopharmacol200626438939516855457
- BokhariFASHeilandFLevinePRayGTRisk factors for discontinuing drug therapy among children with ADHDHealth Serv Outcomes Res Methodol200883134158
- BejerotSRydénEMArlindeCMTwo-year outcome of treatment with central stimulant medication in adult attention-deficit/hyperactivity disorder: a prospective studyJ Clin Psychiatry201071121590159720584517
- LachaineJBeaucheminCSasaneRHodgkinsPSTreatment patterns, adherence, and persistence in ADHD: a Canadian perspectivePostgrad Med2012124313914822691908
- LawsonKAJohnsrudMHodgkinsPSasanéRCrismonMLUtilization patterns of stimulants in ADHD in the Medicaid population: a retrospective analysis of data from the Texas Medicaid programClin Ther2012344944956.e422444786
- PottegårdABjerregaardBKGlintborgDKortegaardLSHallasJMorenoSIThe use of medication against attention deficit/hyperactivity disorder in Denmark: a drug use study from a patient perspectiveEur J Clin Pharmacol201369358959822811260
- HodgkinsPSasanéRMeijerWMPharmacologic treatment of attention-deficit/hyperactivity disorder in children: incidence, prevalence, and treatment patterns in the NetherlandsClin Ther201133218820321497704
- DidoniASequiMPaneiPBonatiMLombardy ADHD Registry GroupOne-year prospective follow-up of pharmacological treatment in children with attention-deficit/hyperactivity disorderEur J Clin Pharmacol201167101061106721538145
- ChenCYYehHHChenKHChangISWuECLinKMDifferential effects of predictors on methylphenidate initiation and discontinuation among young people with newly diagnosed attention-deficit/hyperactivity disorderJ Child Adolesc Psychopharmacol201121326527321663429
- PalliSRKamblePSChenHAparasuRRPersistence of stimulants in children and adolescents with attention-deficit/hyperactivity disorderJ Child Adolesc Psychopharmacol201222213914822364400
- MarcusSCWanGJKemnerJEOlfsonMContinuity of methylphenidate treatment for attention-deficit/hyperactivity disorderArch Pediatr Adolesc Med2005159657257815939858
- BarnerJCKhozaSOladapoAADHD medication use, adherence, persistence and cost among Texas Medicaid childrenCurr Med Res Opin201127Suppl 2132221973228
- ChristensenLSasanéRHodgkinsPHarleyCTetaliSPharmacological treatment patterns among patients with attention-deficit/hyperactivity disorder: retrospective claims-based analysis of a managed care populationCurr Med Res Opin201026497798920178404
- HodgkinsPSasanéRChristensenLHarleyCLiuFTreatment outcomes with methylphenidate formulations among patients with ADHD: retrospective claims analysis of a managed care populationCurr Med Res Opin201127Suppl 2536221973231
- GoetzMYehCBOndrejkaIA 12-month prospective, observational study of treatment regimen and quality of life associated with ADHD in central and eastern europe and eastern AsiaJ Atten Disord2012161445920858785
- SikiricaVPliszkaSRBettsKAComparative treatment patterns, resource utilization, and costs in stimulant-treated children with ADHD who require subsequent pharmacotherapy with atypical antipsychotics versus non-antipsychoticsJ Manag Care Pharm201218967668923206211
- SetyawanJHodgkinsPGuérinAComparing treatment adherence of lisdexamfetamine and other medications for the treatment of attention deficit/hyperactivity disorder: a retrospective analysisJ Med Econ201316796297523621503
- LensingMBZeinerPSandvikLOpjordsmoenSFour-year outcome in psychopharmacologically treated adults with attention-deficit/hyperactivity disorder: a questionnaire surveyJ Clin Psychiatry2013741e87e9323419235
- BowenJFentonTRappaportLStimulant medication and attention deficit-hyperactivity disorder. The child’s perspectiveAm J Dis Child199114532912952003477
- BauermeisterJJCaninoGBravoMStimulant and psychosocial treatment of ADHD in Latino/Hispanic childrenJ Am Acad Child Adolesc Psychiatry200342785185512819445
- ErcanESKoseSKutluAAkyolODurakSAydinCTreatment duration of children with attention deficit hyperactivity disorder is related to functioning and prognosisBulletin of Clinical Psychopharmacology2012222148160
- dosReisSButzALipkinPHAnixtJSWeinerCLChernoffRAttitudes about stimulant medication for attention-deficit/hyperactivity disorder among African American families in an inner city communityJ Behav Health Serv Res200633442343017078011
- NiederkirchnerKSlawikLWermelskirchenDRettigKSchäubleBTransitioning to OROS® methylphenidate from atomoxetine is effective in children and adolescents with ADHDExpert Rev Neurother201111449950821469923
- GauSSChenSJChouWJNational survey of adherence, efficacy, and side effects of methylphenidate in children with attention-deficit/hyperactivity disorder in TaiwanJ Clin Psychiatry200869113114018312048
- KemnerJELageMJImpact of methylphenidate formulation on treatment patterns and hospitalizations: a retrospective analysisAnn Gen Psychiatry20065516606463
- MarcusSCDurkinMStimulant adherence and academic performance in urban youth with attention-deficit/hyperactivity disorderJ Am Acad Child Adolesc Psychiatry201150548048921515197
- MarcusSCWanGJZhangHFOlfsonMInjury among stimulant-treated youth with ADHDJ Atten Disord2008121646917934179
- SikiricaVXieJHeTLImmediate-release versus extended-release guanfacine for treatment of attention-deficit/hyperactivity disorderAm J Pharm Benefits201354e85e94
- SalonerBFullertonCMcGuireTThe impact of long-acting medications on attention-deficit/hyperactivity disorder treatment disparitiesJ Child Adolesc Psychopharmacol201323640140923952187
- Ramos-QuirogaJABoschRCastellsXEffect of switching drug formulations from immediate-release to extended-release OROS methylphenidate: a chart review of Spanish adults with attention-deficit hyperactivity disorderCNS Drugs200822760361118547128
- GimpelGACollettBRVeederMAEffects of stimulant medication on cognitive performance of children with ADHDClin Pediatr (Phila)200544540541115965546
- ColettiDJPappadopulosEKatsiotasNJBerestAJensenPSKafantarisVParent perspectives on the decision to initiate medication treatment of attention-deficit/hyperactivity disorderJ Child Adolesc Psychopharmacol201222322623722537185
- ChouWJChouMCTzangRFBetter efficacy for the osmotic release oral system methylphenidate among poor adherents to immediate- release methylphenidate in the three ADHD subtypesPsychiatry Clin Neurosci200963216717519335386
- GauSSShenHYChouMCTangCSChiuYNGauCSDeterminants of adherence to methylphenidate and the impact of poor adherence on maternal and family measuresJ Child Adolesc Psychopharmacol200616328629716768636
- SitholeyPAgarwalVChamoliSA preliminary study of factors affecting adherence to medication in clinic children with attention-deficit/hyperactivity disorderIndian J Psychiatry2011531414421431007
- ThiruchelvamDCharachASchacharRJModerators and mediators of long-term adherence to stimulant treatment in children with ADHDJ Am Acad Child Adolesc Psychiatry200140892292811501692
- Ibrahim elSRRates of adherence to pharmacological treatment among children and adolescents with attention deficit hyperactivity disorderHum Psychopharmacol200217522523112404679
- Hervey-JumperHDouyonKFrancoKNDeficits in diagnosis, treatment and continuity of care in African–American children and adolescents with ADHDJ Natl Med Assoc200698223323816708509
- HodgkinsPSetyawanJMitraDManagement of ADHD in children across Europe: patient demographics, physician characteristics and treatment patternsEur J Pediatr2013172789590623440479
- RothenbergerABeckerABreuerDDöpfnerMAn observational study of once-daily modified-release methylphenidate in ADHD: quality of life, satisfaction with treatment and adherenceEur Child Adolesc Psychiatry201120Suppl 2S257S26521901416
- MazzoneLRealeLManninoVCocuzzaMVitielloBLower IQ is associated with decreased clinical response to atomoxetine in children and adolescents with attention-deficit hyperactivity disorderCNS Drugs201125650350921649450
- TorresAWhitneyJRaoSTilleyCLobelRGonzalez-HeydrichJTolerability of atomoxetine for treatment of pediatric attention-deficit/hyperactivity disorder in the context of epilepsyEpilepsy Behav20112019510221146461
- ScottNGRipperger-SuhlerJRajabMHKjarDFactors associated with atomoxetine efficacy for treatment of attention-deficit/hyperactivity disorder in children and adolescentsJ Child Adolesc Psychopharmacol201020319720320578932
- BanerjeeSUse of atomoxetine in children and adolescents with ADHDProg Neurol Psychiatry20091321820
- DarredeauCBarrettSPJardinBPihlROPatterns and predictors of medication compliance, diversion, and misuse in adult prescribed methylphenidate usersHum Psychopharmacol200722852953617910020
- RothenbergerARothenbergerLGUpdates on treatment of attention-deficit/hyperactivity disorder: facts, comments, and ethical considerationsCurr Treat Options Neurol201214659460722968494
- AshtonHGallagherPMooreBThe adult psychiatrist’s dilemma: psychostimulant use in attention deficit/hyperactivity disorderJ Psychopharmacol200620560261016478756
- SchlanderMIs NICE infallible? A qualitative study of its assessment of treatments for attention-deficit/hyperactivity disorder (ADHD)Curr Med Res Opin200824251553518186971
- BuitelaarJMedoriRTreating attention-deficit/hyperactivity disorder beyond symptom control alone in children and adolescents: a review of the potential benefits of long-acting stimulantsEur Child Adolesc Psychiatry201019432534019823900
- GrahamJBanaschewskiTBuitelaarJEuropean Guidelines GroupEuropean guidelines on managing adverse effects of medication for ADHDEur Child Adolesc Psychiatry2011201173721042924
- DodsonWWPharmacotherapy of adult ADHDJ Clin Psychol200561558960615723384
- RöslerMCasasMKonofalEBuitelaarJAttention deficit hyperactivity disorder in adultsWorld J Biol Psychiatry201011568469820521876
- GrahamLPractice guidelines: AHA releases recommendations on cardiovascular monitoring and the use of ADHD medications in children with heart diseaseAm Fam Physician20097910905910
- CouryDDexmethylphenidate for attention deficit hyperactivity disorderExpert Opin Pharmacother200910162679268519874250
- GreenhillLLPliszkaSDulcanMKAmerican Academy of Child and Adolescent PsychiatryPractice parameter for the use of stimulant medications in the treatment of children, adolescents, and adultsJ Am Acad Child Adolesc Psychiatry2002412 Suppl26S49S11833633
- Van CleaveJLeslieLKApproaching ADHD as a chronic condition: implications for long-term adherenceJ Psychosoc Nurs Ment Health Serv2008468283718777966
- KarveSClevesMAHelmMHudsonTJWestDSMartinBCGood and poor adherence: optimal cut-point for adherence measures using administrative claims dataCurr Med Res Opin20092592303231019635045
- CramerJARosenheckRCompliance with medication regimens for mental and physical disordersPsychiatr Serv19984921962019575004
- ChapmanSCHorneRMedication nonadherence and psychiatryCurr Opin Psychiatry201326544645223880592
- VelliganDIWeidenPJSajatovicMExpert Consensus Panel on Adherence Problems in Serious and Persistent Mental IllnessThe expert consensus guideline series: adherence problems in patients with serious and persistent mental illnessJ Clin Psychiatry200970Suppl 4146 quiz 4719686636
- Dunbar-JacobJMortimer-StephensMKTreatment adherence in chronic diseaseJ Clin Epidemiol200154Suppl 1S57S6011750211
- YeawJBennerJSWaltJGSianSSmithDBComparing adherence and persistence across 6 chronic medication classesJ Manag Care Pharm200915972874019954264
- Centers for Disease Control and Prevention [homepage on the Internet]Attention-Deficit/Hyperactivity Disorder (ADHD)Atlanta, GACenters for Disease Control and Prevention2013 [update July 3, 2013]. Available from: http://www.cdc.gov/ncbddd/adhd/guidelines.htmlAccessed March 19, 2014
- National Institute for Health and Clinical ExcellenceAttention deficit hyperactivity disorder: Diagnosis and management of ADHD in children, young people and adultsManchester, UKNICE2013 Available from: http://www.nice.org.uk/nicemedia/live/12061/42059/42059.pdfAccessed March 19, 2014
- CascadeEKalaliAHWeislerRHShort-acting versus long-acting medications for the treatment of ADHDPsychiatry (Edgmont)200858242719727272
- SikiricaVFridmanMBrunoAHodgkinsPErderMHConcomitant pharmacotherapy of psychotropic medications in EU children and adolescents with attention-deficit/hyperactivity disorderDrugs R D201313427128024271555
- National Institute of Mental HealthMental Health MedicationsBethesda, MDNational Institute of Mental Health2008 Available from: http://www.nimh.nih.gov/health/publications/mental-health-medications/index.shtml#pub8Accessed March 7, 2014
- Canadian Attention Deficit Hyperactivity Disorder Resource AllianceCanadian ADHD Practice GuidelinesToronto, ONCanadian Attention Deficit Hyperactivity Disorder Resource Alliance2011 Available from: http://www.caddra.ca/pdfs/caddraGuidelines2011.pdfAccessed March 7, 2014
- FaraoneSVAnsthelKMDiagnosing and treating attention-deficit/hyperactivity disorder in adultsWorld Psychiatry20087313113618836579