
Abstract
It is known that elevated serum homocysteine, decreased folate, and low vitamin B12 serum levels are associated with poor cognitive function, cognitive decline, and dementia. Current literature shows that some psychiatric disorders, mainly affective and psychotic ones, can be related to the levels of vitamin B12, folate, and homocysteine. These results can be explained by the importance of vitamin B12, folate, and homocysteine in carbon transfer metabolism (methylation), which is required for the production of serotonin as well as for other monoamine neurotransmitters and catecholamines. Earlier studies focused on the relationship between folate deficiency, hyperhomocysteinemia, and depressive disorders. Although depressive and anxiety disorders show a common comorbidity pattern, there are few studies addressing the effect of impaired one-carbon metabolism in anxiety disorders – especially in obsessive–compulsive disorder (OCD). This study aimed to measure the levels of vitamin B12, folate, and homocysteine specifically in order to see if eventual alterations have an etiopathogenetic significance on patients with OCD. Serum vitamin B12, folate, and homocysteine concentrations were measured in 35 patients with OCD and 22 controls. In addition, the Structured Clinical Interview for the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition, Text Revision, Yale–Brown Obsessive Compulsive Scale, Hamilton Rating Scale for Depression, and Hamilton Rating Scale for Anxiety were conducted for each patient. It was found that vitamin B12 levels were decreased and homocysteine levels were increased in some OCD patients. Homocysteine levels were positively correlated with Yale–Brown compulsion and Yale–Brown total scores. In conclusion, findings of this study suggest that some OCD patients might have vitamin B12 deficiency and higher homocysteine levels.
Introduction
It is reported that psychiatric symptoms – mainly affective and psychotic ones – can be related to the levels of vitamin B12, folate, and homocysteine.Citation1–Citation5 These observations may be explained by the importance of vitamin B12, folate, and homocysteine in carbon transfer metabolism (methylation), which is required for the production of serotonin, other monoamine neurotransmitters, and catecholamines.Citation6 Earlier studies focused on the relationship between folate deficiency and depressive disorders.Citation7,Citation8 These were followed by several case-controlled studies which revealed increasing prevalence of folate and vitamin B12 deficiency in patients with depression.Citation9,Citation10 Recently, homocysteine has been considered as a sensitive marker for folate deficiency.Citation11,Citation12 Observations on the antidepressant effects of folate supplementation may support the importance of these nutrients in psychopathology.Citation13,Citation14 Although comorbidity of depressive and anxiety disorders is common, there are few studies addressing the effect of impaired one-carbon metabolism in anxiety disorders – especially in obsessive–compulsive disorder (OCD).Citation15–Citation18 OCD shows a prevalence of 1%–3% globally, and it follows a chronic course with increased rates of comorbidity. Thus, it is a global burden on the patients as well as on their families, ie, it decreases the quality of life for both of these parties.Citation19–Citation22 Due to the role of OCD in the quality of life of patients and their families, as well as providing an alternative route of augmentation for pharmacotherapy, further studies investigating the roles of vitamin B12, folate and homocysteine may be worthwhile to carry out. Therefore, this study’s aim was to measure vitamin B12, folate, and homocysteine levels specifically to see whether or not their eventual alterations play a role in the etiopathogenesis and/or subsequent course of OCD.
Materials and methods
Patients who were diagnosed with OCD according to the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria were approached and informed about the aims and methods of the study. Among the patients, the ones who did not have mental retardation and/or psychosis, and the ones who provided their informed consent were enrolled in the study. Other exclusion criteria were defined as the history of any endocrinological condition, being pregnant, lactating or having childbearing potential, having clinically relevant abnormal laboratory test results, including megaloblastic anemia, alcohol abuse and dependence and a positive history of immunologic disease. Twenty-two healthy control subjects who matched with the patients in terms of sex and age were chosen from the hospital staff according to exclusion criteria. The controls were interviewed with the non-patient version of the Structured Clinical Interview for the revised third edition of the DSM to exclude any Axis I Disorder.Citation23 In addition, the controls did not have a history of major mood disorder, dementia, mental retardation, or psychosis in their first-degree relatives. All control subjects had either no history of treatment or were drug-free at least for the last 2 weeks.
The patients were diagnosed with the Structured Clinical Interview for DSM-IV Axis I Disorders.Citation24 The Hamilton Rating Scale for Depression,Citation25 Hamilton Rating Scale for Anxiety,Citation26 and Yale–Brown Obsessive–Compulsive ScaleCitation27 were used for evaluating severity and comorbidities.
Venous blood samples were collected after overnight fasting. Homocysteine, folate, and vitamin B12 levels were measured in all subjects. Blood was drawn into tubes containing ethylenediaminetetraacetic acid/K3, immediately placed on ice, and centrifuged at 4°C. Plasma was separated and immediately stored at −80°C before it was analyzed. Cutoffs (given below) were used to determine vitamin deficiency. As described in the literature, they corresponded to the normal ranges of the assays. Folate deficiency was considered to be present when the serum folate level was <3 ng/mL. Vitamin B12 deficiency was defined as a level of serum vitamin B12 <200 pg/mL.Citation16 Hyperhomocysteinemia was defined as a level of plasma homocysteine >14.0 μmol/L.Citation17
SPSS for Windows version 15.0 (2006; SPSS Inc., Chicago, IL, USA) was used in the statistical analyses. Descriptive statistics were performed with frequency and cross tabulations for categorical variables. Means and standard deviations were measured for numerical variables. The chi-square test was used for comparing independent categorical variables. Monte Carlo simulations were run for multiple groups when comparisons did not meet the chi-square criteria; Fisher’s exact test was used in the comparison of the groups. Student’s t-test was used for comparing the numerical data displaying normal distribution; the Mann–Whitney U-test was performed for the numerical variables not displaying normal distribution. The P-value was set at 0.05 and all of the comparisons were two-tailed.
Results
While the mean age of the patient group was 34.0±10.5 years, it was 33.1±8.3 years in the controls. The patient and control groups were mostly female (88.6% and 86.4%, respectively). The groups had no significant differences in terms of their sociodemographic data.
The mean age at onset of OCD was 22.1±8.5 years and the mean duration of OCD was 141.8±111.0 months in the patient group.
There were no significant differences between the patients and controls in terms of hemoglobin values (13.3±1.4 g/dL and 13.8±1.5 g/dL, respectively; P=0.125). The groups were then compared according to folate, vitamin B12, and homocysteine levels. The results showed that all three variables differed significantly ().
Table 1 Levels of vitamin B12, folate, and homocysteine in patient and control groups
Among the 35 cases with OCD, 31 (88.6%) showed good insight; nine (15.8%) of them were diagnosed with comorbid major depressive disorder according to DSM-IV criteria. Among the ones who were diagnosed with OCD, 34 patients reported a history of treatment for the disorder (97.1%), while four (18.2%) of the control subjects declared that they had received psychiatric help in the past for problems not related to anxiety/mood disorders. Thirty-two patients (91.4%) were taking antiobsessive medicine during the study.
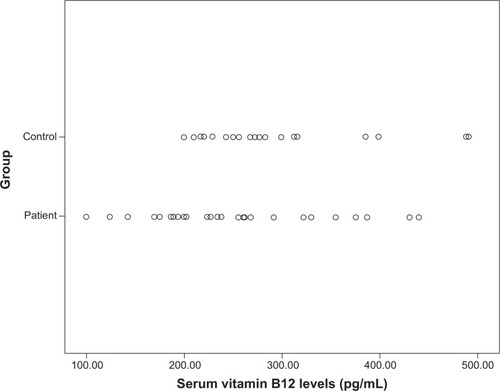
Compared to the control group, the level of vitamin B12 was significantly lower in the patient group (245.4±84.6 versus 291.4±80.9 pg/mL, respectively; P=0.036). The rate of vitamin B12 deficiency (<200 pg/mL) was 31.4% in the patient group, while there was no vitamin B12 deficiency in the control group (). The difference between the groups was statistically significant (P=0.004). Although there was no folate deficiency in either of the groups, the level of homocysteine was found to be significantly higher in the patient group compared to the control group (9.7±2.9 versus 8.1±2.2 μmol/L, respectively; P=0.032). While the highest level of homocysteine was observed in the OCD group with major depressive disorder, the lowest level of homocysteine was in the controls. Levels of the group with OCD without major depressive disorder ranged between the mean averages of these two groups (P=0.06).
Figure 1 Scatter plot of serum vitamin B12 levels of obsessive–compulsive disorder patients and controls.
While hyperhomocysteinemia (>14 μmol/L) was not found in the control group at all, a rate of 14.3% was observed in the patient group. However, this difference was not considered statistically significant (P=0.145).
In the patient group, Spearman’s correlation analysis was performed between levels of vitamin B12, folate, and homocysteine; scores of the Hamilton Rating Scale for Anxiety, Hamilton Rating Scale for Depression, and Yale–Brown Obsession Scale; Yale–Brown compulsion and Yale–Brown total scores; and duration of disease. A statistically significant positive correlation was observed between levels of homocysteine and Yale–Brown compulsion (P=0.021, ρ=0.389) and Yale–Brown total scores (P=0.044, ρ=0.342).
Discussion
There are only a few current studies regarding folate, vitamin B12, and homocysteine values in patients with anxiety disorders – especially with OCD. Hermesh et al indicated that vitamin B12 deficiency was more frequent in OCD patients than controls.Citation15 This suggests that obsessive–compulsive symptoms can be a marker for vitamin B12 deficiency and predicts more well-known symptoms of it. Sharma and Biswas reported a case of a middle-aged male patient presenting with OCD, low levels of serum vitamin B12, and a positive family history of vitamin B12 deficiency who responded well to methylcobalamin replacement.Citation18 Based on this, they suggested a possible etiological role of vitamin B12 in OCD.Citation18 Atmaca et al reported that serum folate values were significantly lower in OCD patients than controls, while homocysteine concentrations were higher in patients compared to controls.Citation16
In the current study, it was found that vitamin B12 levels were decreased and homocysteine levels were increased in at least some of the patients with OCD. Among the OCD patients, the rate of vitamin B12 deficiency was significantly higher compared to the control group while folate deficiency was not found in either group. The rate of hyperhomocysteinemia in the OCD patients seemed to be higher than the control group, although the difference did not have statistical significance. Hyperhomocysteinemia was observed in mood disorders, especially in depressive states, in several studies.Citation9–Citation11 The current finding that the level of homocysteine was most frequent in the group with major depressive disorder may be suggestive of this well-documented relationship, although the association with OCD in general is intriguing and may justify further research.
Hermesh et al suggested that it might point to the possibility that vitamin B12 deficiency characterizes a subgroup of OCD patients.Citation15 Atmaca et al also indicated that folate levels in those patients were significantly and negatively correlated with the scores on the Yale–Brown Obsessive–Compulsive Scale while levels of homocysteine were positively correlated with the duration of illness and Yale–Brown Obsessive–Compulsive Scale scores.Citation16 In the current study, homocysteine levels had a statistically significant positive correlation with Yale–Brown compulsion and Yale–Brown total scores. Considering that the current sample largely consisted of patients who had received previous antiobsessive treatment but had not benefited from it, the high rates of B12 deficiency (and, to a degree, high homocysteine) may be suggestive of a selected group featuring a larger than usual representation of a patient subgroup resistant to treatment in addition to high rates of vitamin B12 deficiency (and hyperhomocysteinemia).
Conclusion
This study showed that some of the patients with OCD had vitamin B12 deficiency and higher homocysteine levels. However, the sample was too small to conclude that this finding is an important biological indicator for OCD. Although more detailed studies regarding this phenomenon are to be carried out, these findings can provide a starting point for future research.
Acknowledgments
The authors would like to express their thanks to the Istanbul Offices of Düzen Laboratories for providing the laboratory analyses of the blood samples used in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
- FafoutiMPaparrigopoulosTLiappasJMantouvalosVTypaldouRChristodoulouGMood disorder with mixed features due to vitamin B12 and folate deficiencyGen Hosp Psychiatry200224210610911869745
- StangerOFowlerBPiertzikKHomocysteine, folate, and vitamin B12 in neuropsychiatric diseases: review and treatment recommendationsExpert Rev Neurother2009991393141219769453
- KaleANaphadeNSapkaleSReduced folic acid, vitamin B12, and docosahexaenoic acid and increased homocysteine and cortisol in never-medicated schizophrenia patients: implications for altered one-carbon metabolismPsychiatry Res20101751–2475319969375
- KimTHMoonSWSerum homocysteine and folate levels in Korean schizophrenic patientsPsychiatry Investig201182134140
- EzzaherAMouhamedDHMechriAHyperhomocysteinemia in Tunisian bipolar I patientsPsychiatry Clin Neurosci201165766467122176285
- BottiglieriTFolate, vitamin B12, and neuropsychiatric disordersNutr Rev199754123823909155210
- CoppenASwadeCJonesSAArmstrongRABlairJALeemingRJDepression and tetrahydrobiopterin: the folate connectionJ Affect Disord1989162–31031072522108
- BottiglieriTLaundyMCrellinRTooneBKCarneyMWReynoldsEHHomocysteine, folate, methylation, and monoamine metabolism in depressionJ Neurol Neurosurg Psychiatry200069222823210896698
- SachdevPSParslowRALuxORelationship of homocysteine, folic acid, and vitamin B12 with depression in a middle-aged community samplePsychol Med200535452953815856723
- KimJMStewartRKimSWYangSJShinISYoonJSPredictive value of folate, vitamin B12, and homocysteine levels in late-life depressionBr J Psychiatry2008192426827418378986
- StablerSPMarcellPDPodellERAllenRHSavageDGLindenbaumJElevation of total homocysteine in the serum of patients with cobalamin or folate deficiency detected by capillary gas chromatography-mass spectrometryJ Clin Invest19888124664743339129
- LindenbaumJHealtonEBSavageDGNeuropsychiatric disorders caused by cobalamin deficiency in the absence of anemia or macrocytosisN Engl J Med198831826172017283374544
- AlpertJEMischoulonDRubensteinGEBottonariKNierenbergAAFavaMFolinic acid (leucovorin) as an adjunctive treatment for SSRI-refractory depressionAnn Clin Psychiatry2002141333812046638
- BaşoğluCAlpay AteşMAlgülAAdjuvant folate with escitalopram treatment and homocysteine, folate, vitamin B12 levels in patients with major depressive disorderBulletin of Clinical Psychopharmacology2009192135142
- HermeshHWeizmanAShaharAMunitzHVitamin B12 and folic acid serum levels in obsessive compulsive disorderActa Psychiatr Scand19887818103176999
- AtmacaMTezcanEKulogluMKirtasOUstandagBSerum folate and homocysteine levels in patients with obsessive–compulsive disorderPsychiatry Clin Neurosci200559561662016194269
- LevineJTiminskyIVishneTElevated serum homocysteine levels in male patients with PTSDDepress Anxiety20082511E154E15717994587
- SharmaVBiswasDCobalamin deficiency presenting as obsessive compulsive disorder: case reportGen Hosp Psychiatry2012345e7e822227032
- FiremanBKoranLMLeventhalJLJacobsonAThe prevalence of clinically recognized obsessive–compulsive disorder in a large health maintenance organizationAm J Psychiatry2001158111904191011691699
- TükelRPolatAÖzdemirÖAksütDTürksoyNComorbid conditions in obsessive–compulsive disorderCompr Psychiatry200243320420911994838
- TürksoyNTükelRÖzdemirÖKaraliAComparison of clinical characteristics in good and poor insight obsessive–compulsive disorderJ Anxiety Disord200216441342312213036
- GururajGPMathSBReddyJYChandrashekarCRFamily burden, quality of life, and disability in obsessive compulsive disorder: an Indian perspectiveJ Postgrad Med2008542919718480523
- SpitzerRLWilliamsJBWGibbonMFirstMBStructured Clinical Interview for DSM-III-R, Non-patient Edition (SCID-NP)Washington, DCAmerican Psychiatric Press1990
- FirstMBSpitzerRLGibbonMWilliamsJBWStructured Clinical Interview for DSM-IV Axis I Disorders, Clinical Version (SCID-CV)Washington, DCAmerican Psychiatric Press1996
- HamiltonMDevelopment of a rating scale for primary depressive illnessBr J Soc Clin Psychology196764278296
- HamiltonMThe assessment of anxiety states by ratingBr J Med Psychol1959321505513638508
- GoodmanWKPriceLHRasmussenSAThe Yale–Brown Obsessive–Compulsive Scale: I. Development, use, and reliabilityArch Gen Psychiatry19894611100610112684084