
Abstract
Background
Blonanserin is a second-generation antipsychotic used for the treatment of schizophrenia in Japan and Korea. The present study aimed to examine early prediction of blonanserin in patients with schizophrenia.
Methods
An 8-week, prospective, single-arm, flexible-dose clinical trial of blonanserin in patients with schizophrenia was conducted under real-world conditions. The inclusion criteria were antipsychotic naïve, and first-episode schizophrenia patients or schizophrenia patients with no consumption of any antipsychotic medication for more than 4 weeks before enrollment in this study. The positive predictive value, negative predictive value, sensitivity, specificity, and predictive power were calculated for the response status at week 4 to predict the subsequent response at week 8.
Results
Thirty-seven patients were recruited (56.8% of them had first-episode schizophrenia), and 28 (75.7%) completed the trial. At week 8, blonanserin was associated with a significant improvement in the Positive and Negative Syndrome Scale (PANSS) total score (P<0.0001) and in positive (P<0.0001), negative (P<0.0001), and general subscale scores (P<0.0001). In terms of percentage improvement of PANSS total scores from baseline to week 8, 64.9% of patients showed a ≥20% reduction in the PANSS total score and 48.6% showed a ≥30% reduction. However, 8.1% of patients experienced at least one adverse event. Using the 20% reduction in the PANSS total score at week 4 as a definition of an early response, the negative predictive values for later responses (ie, reductions of ≥30 and ≥40 in the PANSS total scores) were 88.9% and 94.1%, respectively. The specificities were 80.0% and 51.6%, respectively.
Conclusion
Our results suggest that the blonanserin response at week 4 could predict the later response at week 8.
Keywords:
Introduction
Blonanserin was approved in Japan in January 2008 and in Korea in August 2009 for the treatment of schizophrenia (in the People’s Republic of China, a Phase III clinical trial has been completed, NCT01516424). Blonanserin is classified as a second-generation antipsychotic (SGA). It has antagonistic activity toward serotonin 2A receptor (Ki=0.812 nM), dopamine D2 receptor (Ki=0.142 nM), and dopamine D3 receptor (Ki=0.494 nM) as well as a weak antagonistic activity toward dopamine D1 receptor (Ki=1,070 nM) and adrenergic α1 receptor (Ki=26.7 nM). However, it is almost completely devoid of histamine H1 (Ki>100 nM) and muscarinic M1 antagonistic activity (Ki>100 nM).Citation1 Blonanserin has a unique pharmacological receptor profile, with higher dopamine D2 receptor occupancy than other SGAs and lower antagonistic activity toward serotonin 2A receptor than other SGAs.Citation2 Our meta-analysis revealed that blonanserin is superior to haloperidol in the improvement of the negative subscale score of the Positive and Negative Syndrome Scale (PANSS).Citation3,Citation4 In addition, blonanserin carries a lower risk of hyperprolactinemia and weight gain than risperidone.Citation4,Citation5 This evidence suggests that blonanserin can be used for the treatment of schizophrenia as a first-line antipsychotic such as aripiprazole.
A recent aripiprazole study involving first-episode psychosis revealed that the response at week 3 of aripiprazole treatment accurately predicts the later response (at week 6).Citation6 Nonetheless, no reports have described early prediction of a blonanserin response in patients with schizophrenia. In the present clinical trial, we enrolled patients with first-episode schizophrenia and patients with schizophrenia who did not take any antipsychotic medication for more than 4 weeks before enrollment in this study. Patients with first-episode antipsychotic naïve, schizophrenia are reported to be more sensitive to the adverse effects of antipsychotics than other groups of patients.Citation7,Citation8 In addition, several studiesCitation9,Citation10 have suggested that patients with first-episode schizophrenia respond to low doses of anti psychotic medication.Citation11 Because the blonanserin dose was slowly increased during the present clinical trial, the time point for early prediction of the blonanserin response was set to week 4. Thus, an 8-week, prospective, single-arm, flexible-dose clinical trial of blonanserin in patients with schizophrenia was conducted in real-world clinical settings. We tested whether improvement after the first 4 weeks of treatment can predict the response after 8 weeks.
Materials and methods
Subjects
The present study was conducted from July 2009 to January 2014 at the Fujita Health University Hospital and the Okehazama Hospital. The patients were diagnosed according to the Diagnostic and DSM-IV (Statistical Manual of Mental Disorders, Fourth Edition) criteria with a consensus of at least two experienced psychiatrists on the basis of unstructured interviews and a review of all medical records. All subjects met the following inclusion criteria: 1) patients with first-episode schizophrenia and patients with schizophrenia who did not take any antipsychotic medication for more than 4 weeks before enrollment in this study; 2) age 20–70 years; 3) no neurological or systemic disease, including disturbance of hematopoiesis; 4) no history of electroconvulsive therapy within 6 months prior to the study enrollment; 5) absence of pregnancy; and 6) no dependence on any addictive substances other than nicotine in the past 5 years before enrollment. All subjects underwent laboratory blood testing and electrocardiography at the time of enrollment, and no patients were excluded from the study because of a medical problem.
The clinical trial was described in detail to the subjects, and written informed consent was obtained from all participants and their guardians. This study was approved by the Ethics Committees of Fujita Health University and Okehazama Hospital.
Procedures
Because several studiesCitation9,Citation10 have suggested that patients with first-episode schizophrenia respond to low doses of an antipsychotic,Citation11 all patients received the dose of blonanserin in the range of 4–24 mg/day. The dose of blonanserin was slowly increased (initial dose, 4 mg/day) as a rule unless severe side effects occurred (in such cases, it was slowly decreased). The blonanserin dosage was adjusted at the discretion of a treating psychiatrist. Lorazepam, brotizolam, and biperiden were allowed during our clinical trial (by prescription and for valid clinical reasons).
Evaluation of psychopathology, tolerability, and safety
Patients were tested for psychotic symptoms using PANSSCitation3 at baseline and then again after 4 and 8 weeks. All participants were monitored for adverse events every week by means of full physical examination and general questioning about adverse effects, and the responses were then recorded. All participants underwent blood tests for a complete blood count at week 8 and for liver function, kidney function, electrolytes, prolactin, triglycerides, total cholesterol, and fasting glucose at baseline and at weeks 4 and 8 of the trial.
Statistical analysis
The changes in the PANSS total and subscale scores from baseline to endpoint were evaluated. In addition, the percentage of improvement in the PANSS total score from baseline to week 8 was analyzed (clinical response was defined with increasing stringency, ie, at least 10%, 20%, 30%, or 40% reduction in the PANSS total score) as previous studies.Citation12–Citation15 Intent-to-treat analysis was performed using the last observation carried forward (LOCF) method. Subjects who had at least two data points (from the measurements) were entered into study analyses. Each participant’s last observation was taken as the endpoint. Paired Student’s t-test was used to assess statistical significance of the change in psychopathology scores or in laboratory test values from baseline to endpoint. Moreover, the positive predictive value, negative predictive value (NPV), sensitivity, specificity, and predictive power were calculated for the response status at week 4 to predict the subsequent response at week 8.Citation12–Citation15 Response criteria with high NPV and high specificity are particularly useful because clinicians have to quickly change the course of a treatment if the treatment is unlikely to be effective.Citation12–Citation15 To determine associations between symptom reductions and the response status, we used chi-square tests. A change in the PANSS total score at week 4 was also examined, as was a change in the PANSS total score at week 8; using regression analysis. All calculations were performed via JMP software (JMP 5.2. 1J, SAS Japan Inc., Tokyo, Japan), and a P-value of <0.05 was assumed to denote statistical significance.
Results
Demographics and other characteristics of the patients are presented in . Thirty-seven patients (56.8% of them had a diagnosis of a first-episode schizophrenia) were eventually recruited, and 28 (75.7%) completed the trial. Nine patients (24.3%) discontinued the study medication at week 4 because of lack of efficacy, adverse effects, or withdrawn consent ().
Figure 1 The participants in the study.
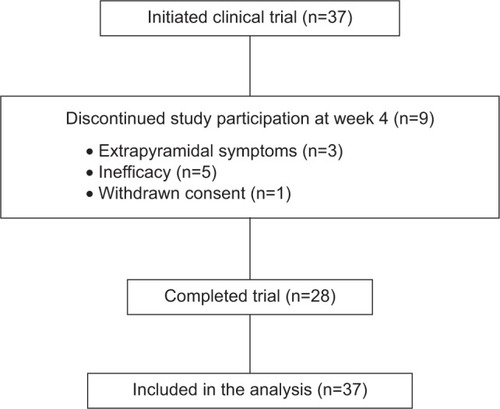
Table 1 Participants’ demographics
At week 8, blonanserin was associated with a significant improvement in the PANSS total score (P<0.0001) and in positive (P<0.0001), negative (P<0.0001), and general subscale scores (P<0.0001) (). A total of 64.9% of the patients showed a ≥20% reduction in the PANSS total score, and 48.6% of the patients showed a ≥30% reduction (). There were no significant differences in demographic characteristics of the participants between responders and nonresponders (). Considering a 20% reduction in the PANSS total score at week 4 as a definition of an early response, NPVs for later responses (ie, reductions of ≥30 and ≥40 in the PANSS total scores) were 88.9% and 94.1%, respectively (). The specificities were 80.0% and 51.6%, respectively (). A change in the PANSS total score at week 4 was also associated with that at week 8 in regression analysis (P<0.0001, β=0.833).
Figure 2 The response rate.
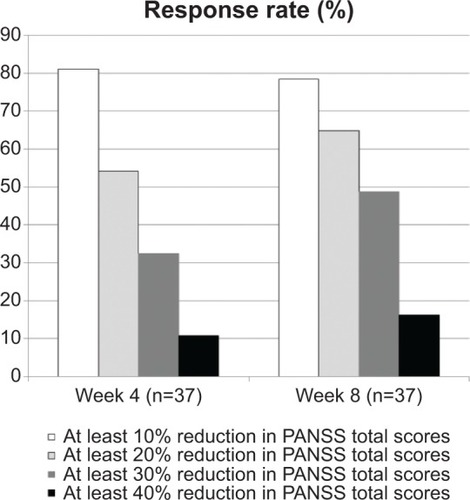
Table 2 Changes from baseline to week 4 and to week 8 in the PANSS total scores and PANSS subscores
Table 3 Conditional probabilities that the response at week 4 will predict the response at week 8 using thresholds for an early response of ≥10%, ≥20%, and ≥30% improvement in the PANSS total scores and thresholds for later responses of ≥20%, ≥30%, and ≥40% improvement in the PANSS total score
Three patients (8.1%) experienced extrapyramidal side effects and akathisia. Two of the three patients discontinued their participation in the study because of the extrapyramidal side effects. No patients had other adverse effects such as weight change, QTc prolongation (on an electrocardiogram), or aberrations in blood tests. Blonanserin nonresponders were more likely to use antiparkinsonian drugs than responders ().
Discussion
The present study is the first clinical trial examining early prediction of a blonanserin response in patients with schizophrenia. We observed significantly reduced PANSS scores and high response rates as a result of blonanserin treatment in patients with first-episode schizophrenia and in patients with schizophrenia who did not take any prior anti psychotic medication similar to the previous blonanserin study of antipsychotic naïve first-episode schizophrenia.Citation1 Our present data indicate that blonanserin is well tolerated. Response criteria with high NPV and high specificity are particularly useful because clinicians have to quickly change the course of a treatment if the treatment is unlikely to be effective. When we used the 10% reduction in the PANSS total score at week 4 as a definition of an early response, the specificity of this predictive method was low (). Nonetheless, when we used a 20% or 30% reduction in the PANSS total score at week 4 as a definition of an early response, then specificity, NPV, and predictive power were high (). Therefore, if a patient does not show an improved PANSS total score (reduction by >20%) at week 4, the physician should switch from blonanserin to some other antipsychotic. Our results suggest that a blonanserin response after 4 weeks can predict the later response at week 8. On the other hand, we must note as follows: considering a 10% reduction in the PANSS total score at week 4 as a definition of an early response, positive predictive values for later responses (ie, reductions of >20 and >30 in the PANSS total scores) were 76.7% and 60.0%, respectively.
Other studies showed that improvement of psychopathology after 1, 2, or 3 weeks of antipsychotic treatment can predict the later response to the antipsychotic drug in question (after 6 or 8 weeks).Citation12–Citation15 Therefore, the response to treatment of schizophrenia with blonanserin may be predicted as early as 4 weeks into the trial. On the other hand, because we slowly increased the blonanserin dose to ensure the safety of our treatment regimen, we believe that it was rather late in the treatment course when blonanserin reached an optimal dose for the patients. In fact, the mean blonanserin dose at week 2 and 4 was 8.37 (5.20) mg/day [mean (standard deviation)] and 12.5 (7.32) mg/day, respectively.
With regard to the safety of our study protocol, only three patients (8.1%) developed extrapyramidal side effects during this clinical trial, and the incidence of extrapyramidal side effects was lower than that in previous Phase III clinical trials of blonanserin.Citation16–Citation19 Nonetheless, three patients (8.1%) received an antiparkinsonian drug during the study. All three received a maximal dose of blonanserin (24 mg/day) because their psychopathological symptoms did not improve after treatment with a moderate dose of blonanserin. Our results suggest that if a patient’s psychopathology does not improve significantly after treatment with a moderate dose of blonanserin for 4 weeks, the treating physician may be able to switch from blonanserin to another antipsychotic before increasing the dose of blonanserin to the maximum in patients with antipsychotic naïve, first-episode schizophrenia with no consumption of any antipsychotic medication for more than 4 weeks.
One of the main limitations of this study is the small sample size. In addition, the clinical trial did not include a control arm of a placebo or active treatment, the trial was not randomized, and the patients and physicians were not blinded to the group assignment of patients. Because of the lack of a control group, the efficacy and tolerability of blonanserin observed in this study cannot be compared with those of other antipsychotic drugs in this population of patients. The Phase III clinical trials of blonanserinCitation16–Citation19 did not use the definition of a drug response using PANSS; therefore, we could not compare our results with those of similar studies. Nonetheless, our present study suggests that blonanserin significantly improves psychopathological symptoms. Although the duration of study was short (8 weeks), first-episode schizophrenia patients may often respond slower than multiple-episode patients. Moreover, the current study was not the fixed-dose of blonanserin, and the patients in the study were not tested for psychotic symptoms using PANSS at 1, 2, and 3 weeks as in the previous studies.Citation12–Citation15 Therefore, early prediction of blonanserin response observed in this study cannot be directly compared with other antipsychotic drugs in this population of patients in other studies.Citation12–Citation15 Finally, it may not be trivial that intent-to-treat analysis was performed using LOCF method in the study. This method may give a biased estimate of the treatment effect and underestimate the variability of the estimated result.Citation20 It is not clearly justified why this analysis in particular is appropriate and valid.
In conclusion, our findings suggest that blonanserin is effective and well tolerated in patients with first-episode schizophrenia and patients with schizophrenia who did not take any antipsychotic medication for more than 4 weeks before enrollment in this study in Japan. Our results suggest that the response at week 4 of blonanserin predicts the later response (at week 8). Because of the small sample size and the lack of a comparator, a double-blind randomized controlled trial should be conducted to further validate the use of blonanserin for the treatment of schizophrenia.
Acknowledgments
We thank Ms Y Matsumoto, Ms M Tani, Ms S Isogai, Ms M Niwa, Mr N Tanaka, Ms M Miyako, Ms E Shibata, Ms N Hayakawa, and Ms A Adachi for the technical support.
Disclosure
Dr Kishi has received speaker’s honoraria from Abbott, Astellas, Daiichi Sankyo, Dainippon Sumitomo, Eli Lilly, GlaxoSmithKline, Yoshitomi, Otsuka, Meiji, Shionogi, Janssen, Novartis, Tanabe-Mitsubishi and Pfizer. Dr Matsuda has received speaker’s honoraria from Dainippon Sumitomo, Eli Lilly, Otsuka, and Pfizer. Dr Fujita has received speaker’s honoraria from Eli Lilly, Mochida, GlaxoSmithKline, Janssen, Yoshitomi, and Otsuka. Dr Iwata has received speaker’s honoraria from Astellas, Dainippon Sumitomo, Eli Lilly, GlaxoSmithKline, Janssen, Yoshitomi, Otsuka, Meiji, Shionogi, Novartis, and Pfizer.
References
- TenjinTMiyamotoSNinomiyaYProfile of blonanserin for the treatment of schizophreniaNeuropsychiatr Dis Treat2013958759423766647
- MiyamotoSDuncanGEMarxCELiebermanJATreatments for schizophrenia: a critical review of pharmacology and mechanisms of action of antipsychotic drugsMol Psychiatry20051017910415289815
- KaySRFiszbeinAOplerLAThe positive and negative syndrome scale (PANSS) for schizophreniaSchizophr Bull19871322612763616518
- KishiTMatsudaYNakamuraHIwataNBlonanserin for schizophrenia: systematic review and meta-analysis of double-blind, randomized, controlled trialsJ Psychiatr Res201347214915423131856
- KishiTMatsudaYIwataNCardiometabolic risks of blonanserin and perospirone in the management of schizophrenia: a systematic review and meta-analysis of randomized controlled trialsPLoS One201492e8804924505373
- ParkJIChoDHHahnSWThe advantage of using 3-week data to predict response to aripiprazole at week 6 in first-episode psychosisInt Clin Psychopharmacol2014292778523970176
- ChatterjeeAChakosMKoreenAPrevalence and clinical correlates of extrapyramidal signs and spontaneous dyskinesia in never-medicated schizophrenic patientsAm J Psychiatry199515212172417298526237
- CorrellCUManuPOlshanskiyVNapolitanoBKaneJMMalhotraAKCardiometabolic risk of second-generation antipsychotic medications during first-time use in children and adolescentsJAMA2009302161765177319861668
- LiuCCChienYLHsiehMHHwangTJHwuHGLiuCMAripiprazole for drug-naive or antipsychotic-short-exposure subjects with ultra-high risk state and first-episode psychosis: an open-label studyJ Clin Psychopharmacol2013331182323277261
- GaebelWRiesbeckMWölwerWMaintenance treatment with risperidone or low-dose haloperidol in first-episode schizophrenia: 1-year results of a randomized controlled trial within the German Research Network on SchizophreniaJ Clin Psychiatry200768111763177418052570
- KahnRSFleischhackerWWBoterHEffectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: an open randomised clinical trialLancet200837196181085109718374841
- CorrellCUMalhotraAKKaushikSMcMenimanMKaneJMEarly prediction of antipsychotic response in schizophreniaAm J Psychiatry2003160112063206514594760
- LeuchtSBuschRKisslingWKaneJMEarly prediction of antipsychotic nonresponse among patients with schizophreniaJ Clin Psychiatry200768335236017388703
- LeuchtSZhaoJEarly improvement as a predictor of treatment response and remission in patients with schizophrenia: a pooled, post-hoc analysis from the asenapine development programJ Psychopharmacol201428438739424429222
- LeuchtSShamsiSABuschRKisslingWKaneJMPredicting antipsychotic drug response – replication and extension to six weeks in an international olanzapine studySchizophr Res20081011–331231918308513
- MiuraSClinical evaluation of blonanserin for schizophrenia: a randomized controlled study comparing blonanserin with riperidoneJpn J Clin Psychopharmacol200811297314
- MurasakiMClinical evaluation of blonanserin for schizophrenia: a double-blind trial comparing blonanserin with haloperidolJpn J Clin Psychopharmacol20071020592079
- GarciaERobertMPerisFNakamuraHSatoNTerazawaYThe efficacy and safety of blonanserin compared with haloperidol in acute-phase schizophrenia: a randomized, double-blind, placebo-controlled, multicentre studyCNS Drugs200923761562519552488
- YangJBahkWMChoHSEfficacy and tolerability of blonanserin in the patients with schizophrenia: a randomized, double-blind, risperidone-compared trialClin Neuropharmacol201033416917520661022
- MallinckrodtCHKaiserCJWatkinJGMolenberghsGCarrollRJThe effect of correlation structure on treatment contrasts estimated from incomplete clinical trial data with likelihood-based repeated measures compared with last observation carried forward ANOVAClin Trials20041647748916279288