
Abstract
The aims of this study are to determine how the interval changes of the brain structures in the early stage of first-episode schizophrenia relate to the interval changes in the clinical data, including the clinical symptoms of schizophrenia and catecholaminergic measures (plasma homovanillic acid [HVA] and 3-methoxy-4-hydroxyphenylglycol [MHPG]). Regional brain volumes and fractional anisotropy (FA)/mean diffusivity (MD) with diffusion tensor imaging (DTI) were measured at baseline and 6-month follow-up in a 3T magnetic resonance imaging (MRI) system in a cohort of 16 schizophrenic patients, who were in their first episode at the time of baseline MRI. At the time of baseline and follow-up MRI, all 16 patients underwent evaluations that included a psychopathological assessment (Positive and Negative Syndrome Scale [PANSS]) and peripheral catecholaminergic measures (plasma MHPG or HVA). For interval changes between baseline and follow-up MRI data (morphological change, MD, and FA), the correlation/regression analysis was performed as a series of single regression correlations in Statistical Parametric Mapping 5, with the interval changes in PANSS or plasma HVA and MHPG as the covariates of interest. Positive and inverse correlations contrasts were created, and in this preliminary analysis, a family-wise error-corrected threshold of P<0.05 was considered significant. In the correlation/regression analysis, a positive correlation between the FA in the right cerebellar vermis and the MHPG was observed. No significant correlations between the brain volume or MD and any laboratory data (plasma HVA and MHPG) were found. During the 6-month follow-up in the early stage of first-episode schizophrenia, the MHPG changes were correlated with the microstructural FA changes in the cerebellum, which may reflect the functional connections of the noradrenergic system in the cerebellum.
Introduction
Schizophrenia is a neuropsychiatric disorder that shows detectable evidence of brain structural abnormalities in the majority of afflicted individuals during the chronic stages.Citation1 The identification of the structural brain abnormalities in patients with schizophrenia, using magnetic resonance imaging (MRI), has become an important area of neuroimaging research in recent years. Several previous studies using a voxel-wise analysis have reported that the morphological changes are detectable on 3D MRI and/or the reduced fractional anisotropy (FA) on diffusion tensor imaging (DTI) in several regions at the first manifestation of schizophrenia (first-episode schizophrenia).Citation2–Citation5 Use of voxel-wise analysis has also allowed correlation/regression analysis to be performed between the patient’s MRI data and their clinical data. Recently, many studies have looked at the relationship between structural data (including DTI) and clinical data (including the Positive and Negative Syndrome Scale [PANSS]).Citation6,Citation7 One study reported inverse correlations of FA values with PANSS positive symptom scores in the left uncinate fasciculus, right sagittal stratum, and the left superior longitudinal fasciculus.Citation7 In these studies, however, it seems unclear whether the relationship between the structural brain abnormalities and the clinical data really existed, because no study has evaluated the longitudinal changes in patients with first-episode schizophrenia.
The actions of antipsychotic drugs on the dopamine system have led to many examinations of dopaminergic metabolites as possible markers for psychosis and antipsychotic response. However, it has also become clear that the noradrenergic system has extensive interactions with the dopamine system, and may play a role in schizophrenia,Citation8 and may also have a key role in psychotic relapse.Citation9 Interactions between the two systems have been well-studied in the cerebrospinal fluid and plasma of schizophrenic patients through their respective metabolites; plasma homovanillic acid (HVA) and 3-methoxy-4-hydroxyphenylglycol (MHPG) are the major degradation products of the monoamines dopamine and noradrenaline, respectively. Plasma HVA and MHPG are good predictors of response to antipsychotic treatment;Citation10–Citation12 the effects of risperidone (a benzisoxazole derivative belonging to a family of atypical antipsychotic drugs) on plasma levels of HVA and MHPG have been related to its clinical efficacy in ameliorating the positive and negative symptoms of schizophrenia, respectively.Citation11,Citation13 Moreover, recent studies reported that plasma levels of MHPG are decreased in patients in the early stage of first-episode schizophrenia,Citation10,Citation14 which suggests that the MHPG may be a useful biomarker in the early stages of schizophrenia. Although it is of interest to explore whether and how anatomic deficits relate to clinical manifestations and alterations in brain physiology, we know of no voxel-wise correlation/regression analysis in which correlation between MRI data and peripheral catecholaminergic measures have been shown.
Herein, we report the results of a longitudinal MRI study of first-episode schizophrenia conducted to date, to our knowledge, using well-validated and highly reliable state-of-the-art neuroimaging tools. We measured regional brain volumes, FA, and mean diffusivity (MD) during an average of 6 months using high-resolution MRI with a 3T MRI system in a cohort of schizophrenic patients, who were in their first episode at the time of baseline MRI. The aims of this study were to determine how the interval changes of the brain structures in the early stage of first-episode schizophrenia relate to interval changes in the clinical data, including clinical symptoms of schizophrenia and peripheral catecholaminergic measures (plasma HVA and MHPG).
Materials and methods
Subjects
The diagnosis of schizophrenia, according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), requires at least a 6-month duration of signs of the disturbance. In this study, a total of 26 patients who fulfilled the DSM-IV-TR criteria A, B, D, E, and F, were recruited for the study, except for the criterion regarding the disease duration. All subjects underwent baseline magnetic resonance (MR) examinations within 6 months from the date from which the patients fulfilled these criteria. Therefore, all baseline MR examinations were performed during the early stage of first-episode schizophrenia, before a diagnosis of schizophrenia was established.Citation6 After a 6-month follow-up, a diagnosis of schizophrenia was established in 23 of the 26 patients. The symptoms of the remaining patients had completely remitted spontaneously without any medication use preceding the 6-month follow-up. One of the 23 patients was subsequently excluded from the study, because the image quality was impaired by severe artifacts from dental materials. After a 6-month follow-up, the remaining 22 patients were invited for a repeat MR examination (follow-up MRI). This MRI was unavailable for six patients. Therefore, 16 patients (eight males, eight females; mean age: 29.0±11.6 years; age range: 13–52 years) were finally enrolled in the longitudinal study. All were considered to have been in the early stage of first-episode schizophrenia at the time of the baseline MR examinations. All patients were screened by using the Structured Clinical Interview for DSM-IV-TR Disorders (SCID; New York State Psychiatric Institute 1995), and exclusion criteria for all groups were: 1) current or past serious medical illness such as cancer, diabetes mellitus, epilepsy, and cerebral infarction; 2) dependence on alcohol; and 3) illicit substance use such as methamphetamine, narcotics, and marijuana.
The mean duration from the date from which the patients fulfilled the DSM-IV-TR criteria A, B, D, E, and F to the date of baseline MR examination for the patients was 2.9±2.5 months. The duration of psychosis (DUP) was defined as the day of emergence of several symptoms of psychosis to the day when baseline MR examination was performed. The mean DUP was 6.9±6.4 months; therefore, the mean duration from the date of onset of psychotic symptoms to the date on which the patients fulfilled DSM-IV-TR criteria A, B, D, E, and F was 4.1±6.1 months. These two items were reconfirmed by the patients themselves and their family members. At baseline MR examination, the total cumulative exposure to a chlorpromazine equivalent dose of antipsychotic drugs was 214±117 mg (mean ± standard deviation [SD]). One of the 16 patients had not received any medications, and the rest of the 15 patients were treated with atypical antipsychotic drugs (risperidone, n=2; aripiprazole, n=6; olanzapine, n=5; quetiapine, n=2). At follow-up MR examination, the total cumulative exposure to a chlorpromazine equivalent dose of antipsychotic drugs was 390±218 mg. All 16 patients were treated with atypical antipsychotic drugs (risperidone, n=2; aripiprazole, n=6; olanzapine, n=5; quetiapine, n=2; perospirone, n=1).
At the time of baseline and follow-up MR examinations, all 16 patients underwent an evaluation, which included a psychopathological assessment (PANSS) and peripheral catecholaminergic measures (plasma HVA and MHPG).
Magnetic resonance imaging acquisition and image processing for voxel-based morphometry
For baseline and follow-up MR examinations, the MRI data were obtained using a 3.0-Tesla scanner with a three-dimensional fast spoiled gradient recalled acquisition with steady state (3D-FSPGR), which was acquired with parameters of 10/4.1/700 (repetition time [ms]/echo time [ms]/inversion time), a flip angle of 10°, a 24 cm field of view (FOV), and 1.2 mm thick sections 0.47×0.47×1.2 mm resolution. All images were corrected for image distortion due to gradient nonlinearity using ‘GradWarp’Citation15 and for intensity inhomogeneity using ‘N3’.Citation16 Image processing for voxel-based morphometry (VBM),Citation17 a fully automatic technique for computational analysis of differences in regional brain volume throughout the entire brain, was conducted using SPM5 (Statistical Parametric Mapping; v5; Institute of Neurology, London, UK). The 3D-FSPGR images in native space were bias-corrected; spatially normalized; segmented into gray matter, white matter, and cerebrospinal fluid images; and intensity-modulated using SPM5.Citation18 The DARTEL (Diffeomorphic Anatomical Registration Through Exponential Lie Algebra) toolbox was used in a high-dimensional normalization protocol. DARTEL was proposed by Ashburner as an alternative method of normalization in the SPM package.Citation19 In an intensity modulation step, voxel values of the segmented images were multiplied by the measure of warped and unwarped structures derived from the nonlinear step of the spatial normalization. This step converted the relative regional gray matter density into absolute gray matter density, expressed as the amount of gray matter per unit volume of brain tissue before spatial normalization. The resulting modulated gray and white matter images were smoothed with an 8 mm Gaussian kernel.
Diffusion tensor images: MRI scanning protocol
All subjects also underwent DTI examinations with the same scanner and at the same time as 3D-FSPGR. The methods of DTI acquisition and data analysis were similar to those in a previous study.Citation20 In brief, a single-shot, spin-echo planar sequence was used (repetition time/echo time [TR/TE] =12,000/83.3 ms; 4 mm slice thickness; no gap; FOV 26 cm; number of excitations =1, spatial resolution 1.02×1.02×4 mm). The diffusion properties were measured at a b-value of 1,000 s/mm2 along 25 noncollinear directions. Eddy current correction and patient motion correction were performed on the diffusion-weighted basis images using Functional MRI of the Brain (FMRIB)’s Linear Image Registration Tool (FLIRT) from the FMRIB Software Library (FSL).Citation21 The images were corrected for image distortion due to gradient nonlinearity using ‘GradWarp’. Individual FA and MD maps were calculated using the DTIFIT tool implemented in FSL.
Spatial normalization of DTI for SPM analysis
The echo planar sequence used for the acquisition of the diffusion tensor dataset suffers from inherent geometric distortion from magnetic field inhomogeneities. Moreover, the contrast of the FA map is quite different from that of T1-, T2-, or proton density–weighted template images provided with SPM5. Therefore, an FA template specific to this study was created using the data from all participants. Each T2-weighted echo-planar image was co-registered into the 3D-FSPGR image, and the co-registration parameter was applied to the corresponding FA map. The parameters of the normalization used in the spatial normalization step of the 3D-FSPGR images in native space onto the T1 template were also applied to the co-registered FA map. The normalized FA maps were smoothed with an 8 mm isotropic Gaussian kernel, and a mean image (FA template) was created. Thereafter, all FA maps in native space were transformed onto the stereotactic space by registering each of the images to the customized FA template. The normalized FA map was smoothed with an 8 mm isotropic Gaussian kernel.
Image processing for tract-based spatial statistics
The structural distortion of the diffusion-weighted MR images was corrected based on each T2-weighted echo planar image (b=0 s/mm2) by using eddy current correction in the FMRIB Diffusion Toolbox software program (v5.0.4; parts of the FSL). Non-brain tissue of each MR image was deleted using the brain extraction tool. Voxel-wise statistical analysis of the DTI data was performed by using Tract-Based spatial analysis (TBSS; v1.1) software program. The FA volumes were aligned to a target image as follows: 1) apply nonlinear registration of each subject’s FA into the FMRIB58_FA_1 mm standard-space image as the target image; and 2) the target image was affine transformed to 1×1×1 mm MNI 152 (Montreal Neurologic Institute, Montreal, QC) space. A mean FA image was created by averaging the aligned individual FA images, and was then thinned to create an FA skeleton representing white matter tracts common to all subjects. For the FA skeleton, a threshold was set at 0.2 to exclude voxels with low FA values, which are likely to include grey matter or cerebrospinal fluid. Individual FA data and voxel-wise statistical results were projected onto this FA skeleton. Subsequently, the MD were projected onto the mean FA skeleton and also compared between groups at the same spatial location.
Statistical analyses of voxel-based morphometry and DTI
In order to examine the interval changes of brain volume, a new set of images (temporal subtracting image [TSI]) was generated by calculating an interval change on MR images for each patient by subtracting the follow-up images from the baseline images.Citation22 The TSI were created using the following formula: TSI = (baseline image − follow-up image)/0.5 (baseline image + follow-up image). Therefore, the TSI represents the brain volume differences between the follow-up and baseline images for each voxel. Positive voxel values on the image indicate that the baseline MR images had higher intensity values than the follow-up images; negative voxel values on the image indicate that the follow-up images had higher intensity values than the baseline MR images. The same method was applied for creating the TSI on either the FA or MD maps for SPM analysis. We used the FA or MD skeleton to calculate TSI for TBSS.
Measurement of plasma levels of HVA and MHPG
Plasma concentrations of HVA and MHPG were analyzed by high-performance liquid chromatography with electrochemical detection (HPLC-ECD). The plasma HVA levels were analyzed by HPLC-ECD according to the method of Yung et al with a slight modification.Citation23 The plasma MHPG levels were also analyzed by HPLC-ECD according to the method of Ohnishi et al.Citation24
Correlational analysis
The interval changes in clinical or laboratory data were calculated for each subject by subtracting the follow-up data from the baseline data. For each interval change (TSI) between baseline and follow-up MR data (morphological changes, MD, and FA), the correlational analysis was performed as a series of single regression correlations in SPM5, with the interval changes of clinical data (positive and negative PANSS) or laboratory data (plasma HVA and plasma MHPG) as the covariates of interest. Positive and inverse correlations contrasts were created. Family-wise error (FWE) correction was applied. The significance level was set at false discovery rate (FDR)-corrected P<0.05. Significant clusters were identified by specific white matter tract through meticulous comparison to the MRI Atlas of Human White Matter.
Results
There was no significant difference in the global brain volume (total gray matter, total white matter, and intracranial volume) between baseline and follow-up MRI (). Both the positive and negative PANSS at follow-up MRI were significantly lower than those at baseline MRI. The plasma HVA and MHPG at follow-up MRI were significantly lower and higher, respectively, than that at baseline MRI. The mean duration between the baseline and follow-up MRI was 6 months. The laboratory data (plasma HVA and MHPG) were not associated with the dose of antipsychotic drugs both at baseline and after follow-up interval.
Table 1 Demographic and clinical characteristic of the patients at baseline and follow-up MRI
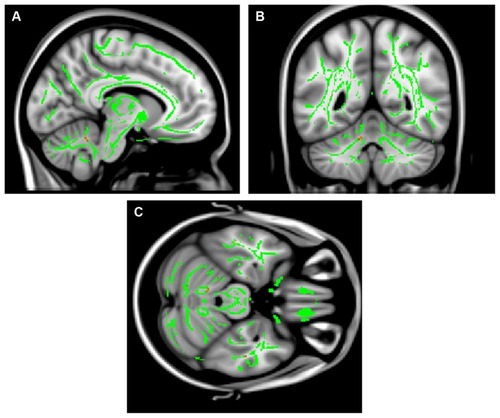
In the correlation/regression analysis, a positive correlation between the MHPG and the FA in the right cerebellar vermis was observed in the SPM analysis ([MNI coordinate x, y, z] on DTI map = [−6, −50, −26], FWE-corrected P=0.012, Z=5.05, T=9.80; ), whereas an inverse correlation between the FA and MHPG was not found in any brain region. The TBSS analysis also showed a positive correlation between the MHPG and FA in the white matter of the right cerebellar vermis ([MNI coordinate x, y, z] on DTI map = [−6, −51, −27], uncorrected P<0.001, cluster size =390; ), although no voxels could survive after correction for multiple comparisons. No significant correlations between the brain volume or MD and any laboratory data (plasma HVA and MHPG) were evident. There were no significant correlations between any MR data (brain volumes, FA, and MD) and PANSS.
Figure 1 Correlation/regression analysis for 16 patients.
Abbreviations: FA, fractional anisotropy; FWE, family-wise error; MHPG, 3-methoxy-4-hydroxyphenylglycol.
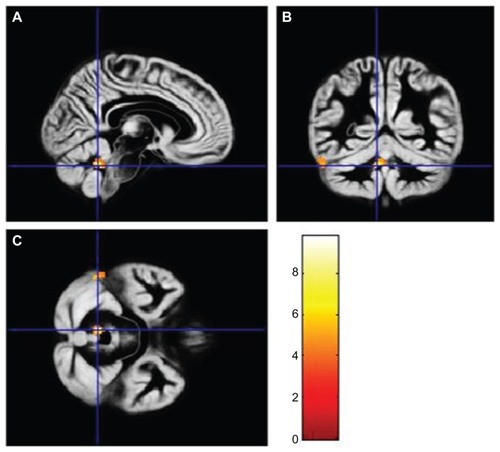
Figure 2 Correlation/regression analysis for 16 patients.
Abbreviations: FA, fractional anisotropy; MHPG, 3-methoxy-4-hydroxyphenylglycol.
At the time of baseline and follow-up, no correlations were found in any brain region between any of the MR data (brain volumes, FA, and MD) and the laboratory data (plasma HVA and MHPG).
Discussion
Schizophrenia usually shows a prepsychotic phase of illness in which a change from premorbid functioning occurs.Citation23 This period is characterized by various mental state features, including nonspecific symptoms such as depressed mood and anxiety as well as subthreshold or attenuated psychotic symptoms. There is increasing interest in the potential for early detection and intervention during the early phase of a psychotic disorder.Citation25 Previous studies have reported that early detection and intervention in schizophrenia may offer a promising opportunity to redirect the illness’ negative course.Citation26,Citation27 In this study, all patients underwent the baseline MR examinations within 6 months from the time they fulfilled DSM-IV-TR criteria A, B, D, E, and F. Therefore, all baseline MR examinations were performed during the early stage of first-episode schizophrenia, before a diagnosis of schizophrenia was established. This is the first longitudinal MRI study to perform VBM analysis and voxel-based analysis of MD and FA maps computed from DTI obtained during the early stage of first-episode schizophrenia.
In the present study, we assessed the interval changes of MRI data and peripheral catecholaminergic measures during an average of 6 months using voxel-wise correlation/regression analysis, because there are individual variations in response to antipsychotic treatment; a positive correlation was observed between the FA in the right cerebellar vermis and MHPG. The reduced FA could be associated with microstructural alteration or damage involving the myelin sheath and/or directional coherence of fiber tracts. Some studies assessed first-episode schizophrenia and reported lower FA values in the patients as compared to controls at widespread brain regions, including the cerebral peduncle.Citation2,Citation3 Some studies conducted in schizophrenic patients demonstrated significantly lower FA than in controls in the cerebellum.Citation28,Citation29 In the present study, plasma MHPG was significantly higher at follow-up than at baseline. This indicates that the FA value in the cerebellum, which has a positive correlation with plasma MHPG, may have increased over the follow-up interval, probably due to the effect of antipsychotic drug treatment.
The neurodegenerative hypothesis in schizophrenia suggests that pathologic alterations in brain morphology may occur after onset of the illness, mainly in the early stages, and may be associated with the illness’ course and severity.Citation30 This hypothesis is supported by both longitudinal clinical and neuroimaging studies after onset.Citation1,Citation31 Several prospective longitudinal studies in first-episode schizophrenia found progressive volume reduction at the initial stage of schizophrenia in the frontal and temporal areas, especially the superior temporal gyrus, Heschl’s gyrus, and amygdala–hippocampal complex;Citation1,Citation32,Citation33 more pronounced volume reduction in these areas was associated with poor outcome, negative symptoms, and a decline in neuropsychological performance.Citation31,Citation33 Furthermore, progressive reduction in cerebellum volume has also been reported in first-episode schizophrenia. In contradiction to this previous study, our results indicate that the FA changes (microstructural tissue alteration) within the cerebellum can be normalized during the early stage of first-episode schizophrenia.
Moreover, our results may also suggest that microstructural changes (FA changes) within the cerebellum relate to norepinephrine activity during the early stage of first-episode schizophrenia. Many regions of the brain are supplied by the noradrenergic systems. The principal centers for noradrenergic neurons are the locus coeruleus and the caudal raphe nuclei. The ascending nerves of the locus coeruleus project to the frontal cortex, thalamus, hypothalamus, and limbic system. Noradrenaline is also transmitted from the locus coeruleus to the cerebellum. Our positive correlation between the FA in the cerebellar vermis and norepinephrine metabolite MHPG may reflect these functional connections in the cerebellum as noradrenergic systems.
Traditionally, the emphasis of studies on cerebellar function has been on the coordination of somatic motor function, control of muscle tone, and equilibrium. However, the cerebellum also shares bidirectional connections with a large portion of the limbic lobe and the associated subcortical nuclei, the amygdaloid complex, the septal nuclei, and various hypothalamic and thalamic nuclei, which are regions of interest to psychiatry through their association with emotional processing. There is accumulating evidence of a cognitive role of the cerebellum,Citation30 including executive function and working memory, which are impaired in schizophrenia.Citation31 The previous neuroimaging studies by the resting-state functional MRICitation34,Citation35 and DTI methodCitation28,Citation29 suggest that the connectivity of the cerebellum is impaired in schizophrenia. Collin et alCitation34 demonstrated that, compared to healthy control subjects, schizophrenia patients showed impaired functional connectivity between the cerebellum and several cerebral regions, including the hippocampus, thalamus, middle cingulate gyrus, triangular part of the inferior frontal gyrus, supplementary motor area, and lingual gyrus. Furthermore, Liu et alCitation35 found that in schizophrenic patients, the bilateral cerebellum showed reduced functional connectivities to some regions compared to controls, such as the left middle temporal gyrus, bilateral middle cingulate cortex, right paracentral lobule, right thalamus, and bilateral cerebellum, and the FA of the left superior cerebellar peduncles was significantly reduced in patients. These results also support the opinion that the cerebellum might play a key role in schizophrenia.
Andreasen et al and Wiser et al proposed that disruption of a cortico–cerebellar–thalamic–cortical circuit (CCTCC) may underlie the combination of symptoms observed in schizophrenia.Citation36,Citation37 This model of schizophrenia as secondary to disrupted development in the CCTCC has been termed ‘cognitive dysmetria’,Citation37 referring to incoordination in the processing, prioritization, retrieval, and expression of information. Our finding that the microstructural changes in the cerebellum occurred during 6-month follow-up in patients with first-episode schizophrenia may be consistent with theoretical accounts of schizophrenia as a disorder of functional integration, and with the cognitive dysmetria hypothesis, which posits a disconnection within the CCTCC as a fundamental abnormality in schizophrenia.
Recent studies have reported the relationship between MRI data and the PANSS. One study reported that a small area of white matter near the right insula showed a positive correlation between the PANSS negative symptoms and apparent diffusion coefficient.Citation38 Another study demonstrated that the positive correlation of FA values with positive symptom scores were seen in the white matter adjacent to the right lateral ventricle, and also found an inverse correlation between FA values in the same brain region and negative symptom scores.Citation6 To the best of our knowledge, however, no previous MRI studies have reported the longitudinal relationship between MRI data and the PANSS in schizophrenic patients. Although the PANSS was improved significantly over the follow-up interval by ongoing antipsychotic drug treatment, correlations between longitudinal MR data and PANSS changes were not found in any brain regions. Therefore, clinical improvement may not necessarily be related to the microstructural changes of the brain. Whitford et al have reported the evidence of progressive white matter atrophy over the first 2–3 years of illness in patients with first-episode schizophrenia, although the psychotic symptoms (PANSS) in these patients improved over this interval.Citation39 The results from these previous studies may support our negative data.
There were several limitations to this study. Firstly, the number of patients was small. Although previous MR studies have reported the cerebellar volume abnormalities in schizophrenia patients,Citation40,Citation41 our study did not show any correlation between brain volume and laboratory data in any brain region. Furthermore, in this study, the correlations between the longitudinal MR data and PANSS changes were not found in any brain regions. Therefore, our small sample size might limit the statistical power in these analyses. Secondly, our patients received various kinds of antipsychotic medication at baseline MR examinations, which may have affected the MR data and peripheral catecholaminergic measures. The DUP classically refers to the duration of untreated psychosis. In this sense, the value of DUP in the present study may not be precise, because the patients had been administered antipsychotic drugs before they underwent baseline MRI. However, it could be ethically problematic to follow the psychotic patients without any antipsychotic drugs until performing an MR examination. Thirdly, the initial symptoms of schizophrenia might start before the patients and their family notice a problem. Finally, the heterogeneity of our sample population may exist by the inclusion of a wide age range or clinical variables, such as disorganization score and intelligence quotient (IQ), in comparison with a previous study.Citation5,Citation30,Citation42–Citation44 Although DeLisi et al reported that approximately 60% of plasma MHPG is derived from the brain,Citation42 it is currently believed that about one-third of plasma MHPG is of brain origin.Citation45 In short, we should note with caution the use of plasma MHPG as an indicator of activities in central noradrenergic neurons as it is predominantly derived from the periphery.
Conclusion
We found evidence that patients with first-episode schizophrenia exhibit a positive correlation of interval changes between the FA in the right cerebellar vermis and the norepinephrine metabolite MHPG during 6-month follow-up; this may reflect both anatomic and functional connections within the cerebellum to the prefrontal cortex, the subcortical limbic structures, and monoamine-producing brainstem nuclei. Our findings also suggest that microstructural FA changes could be reversible during the early stage of first-episode schizophrenia, and that plasma MHPG might therefore be a sensitive marker for the detection of this change.
Disclosure
The authors report no conflicts of interest in this work.
References
- ShentonMEDickeyCCFruminMMcCarleyRWA review of MRI findings in schizophreniaSchizophr Res2001491–215211343862
- CheungVCheungCMcAlonanGMA diffusion tensor imaging study of structural dysconnectivity in never-medicated, first-episode schizophreniaPsychol Med200838687788517949516
- HaoYLiuZJiangTWhite matter integrity of the whole brain is disrupted in first-episode schizophreniaNeuroreport2006171232616361944
- JayakumarPNVenkatasubramanianGGangadharBNJanakiramaiahNKeshavanMSOptimized voxel-based morphometry of gray matter volume in first-episode, antipsychotic-naive schizophreniaProg Neuropsychopharmacol Biol Psychiatry200529458759115866362
- SzeszkoPRArdekaniBAAshtariMWhite matter abnormalities in first-episode schizophrenia or schizoaffective disorder: a diffusion tensor imaging studyAm J Psychiatry2005162360260515741480
- MoriyaJKakedaSAbeOGray and white matter volumetric and diffusion tensor imaging (DTI) analyses in the early stage of first-episode schizophreniaSchizophr Res2010116219620319854618
- SkellyLRCalhounVMedaSAKimJMathalonDHPearlsonGDDiffusion tensor imaging in schizophrenia: relationship to symptomsSchizophr Res200898115716218031994
- HornykiewiczOBrain catecholamines in schizophrenia – a good case for noradrenalineNature198229958834844867121591
- van KammenDPAgrenHYaoJKO’ConnorDTGurklisJPetersJLNoradrenergic activity and prediction of psychotic relapse following haloperidol withdrawal in schizophreniaAm J Psychiatry199415133793847509126
- YoshimuraRNakamuraJUedaNTeraoTEffect of risperidone on plasma free 3-methoxy-4-hydroxyphenylglycol (pMHPG) levels in schizophrenic patients: relationship among plasma concentrations of risperidone and 9-hydroxyrisperidone, pMHPG levels, and clinical improvementInt Clin Psychopharmacol200015317518010870876
- YoshimuraRUedaNShinkaiKNakamuraJPlasma levels of homovanillic acid and the response to risperidone in first episode untreated acute schizophreniaInt Clin Psychopharmacol200318210711112598823
- KakiharaSYoshimuraRShinkaiKPrediction of response to risperidone treatment with respect to plasma concencentrations of risperidone, catecholamine metabolites, and polymorphism of cytochrome P450 2D6Int Clin Psychopharmacol2005202717815729081
- YoshimuraRYanagiharaNHaraKInhibitory effects of clozapine and other antipsychotic drugs on noradrenaline transporter in cultured bovine adrenal medullary cellsPsychopharmacology (Berl)20001491172310789878
- HoriHYoshimuraRYamadaYEffects of olanzapine on plasma levels of catecholamine metabolites, cytokines, and brain-derived neurotrophic factor in schizophrenic patientsInt Clin Psychopharmacol2007221212717159456
- JovicichJCzannerSGreveDReliability in multi-site structural MRI studies: effects of gradient non-linearity correction on phantom and human dataNeuroimage200630243644316300968
- SledJGZijdenbosAPEvansACA nonparametric method for automatic correction of intensity nonuniformity in MRI dataIEEE Trans Med Imaging199817187979617910
- AshburnerJFristonKJVoxel-based morphometry – the methodsNeuroimage2000116 Pt 180582110860804
- AshburnerJFristonKJUnified segmentationNeuroimage200526383985115955494
- AshburnerJA fast diffeomorphic image registration algorithmNeuroimage20073819511317761438
- AbeOYamasueHAokiSAging in the CNS: comparison of gray/white matter volume and diffusion tensor dataNeurobiol Aging200829110211617023094
- JenkinsonMBannisterPBradyMSmithSImproved optimization for the robust and accurate linear registration and motion correction of brain imagesNeuroimage200217282584112377157
- LudersEGaserCJanckeLSchlaugGA voxel-based approach to gray matter asymmetriesNeuroimage200422265666415193594
- YungARPhillipsLJYuenHPPsychosis prediction: 12-month follow up of a high-risk (“prodromal”) groupSchizophr Res2003601213212505135
- OhnishiAMinegishiAIshizakiTEffect of [beta]-adrenoceptor blockade on exercise-induced plasma catecholamine concentration-heart rate response relationshipJ Cardiovasc Pharmacol19871066676742450237
- TanHYAngYGFirst-episode psychosis in the military: a comparative study of prodromal symptomsAust N Z J Psychiatry200135451251911531734
- McGlashanTHA selective review of recent North American long-term followup studies of schizophreniaSchizophr Bull19881445155423064280
- McGlashanTHEarly detection and intervention of schizophrenia: rationale and researchBr J Psychiatry Suppl199817233369764119
- KyriakopoulosMFrangouSRecent diffusion tensor imaging findings in early stages of schizophreniaCurr Opin Psychiatry200922216817619553871
- KanaanRABorgwardtSMcGuirePKMicrostructural organization of cerebellar tracts in schizophreniaBiol Psychiatry200966111067106919733836
- KakedaSKorogiYThe efficacy of a voxel-based morphometry on the analysis of imaging in schizophrenia, temporal lobe epilepsy, and Alzheimer’s disease/mild cognitive impairment: a reviewNeuroradiology201052871172120495793
- Hulshoff PolHEKahnRSWhat happens after the first episode? A review of progressive brain changes in chronically ill patients with schizophreniaSchizophr Bull200834235436618283048
- AsamiTBouixSWhitfordTJShentonMESalisburyDFMcCarleyRWLongitudinal loss of gray matter volume in patients with first-episode schizophrenia: DARTEL automated analysis and ROI validationNeuroimage201259298699621924364
- YoshidaTMcCarleyRWNakamuraMA prospective longitudinal volumetric MRI study of superior temporal gyrus gray matter and amygdala-hippocampal complex in chronic schizophreniaSchizophr Res20091131849419524408
- CollinGHulshoff PolHEHaijmaSVCahnWKahnRSvan den HeuvelMPImpaired cerebellar functional connectivity in schizophrenia patients and their healthy siblingsFront Psychiatry201127322203807
- LiuHFanGXuKWangFChanges in cerebellar functional connectivity and anatomical connectivity in schizophrenia: a combined resting-state functional MRI and diffusion tensor imaging studyJ Magn Reson Imaging20113461430143821976249
- AndreasenNCO’LearyDSCizadloTSchizophrenia and cognitive dysmetria: a positron-emission tomography study of dysfunctional prefrontal-thalamic-cerebellar circuitryProc Natl Acad Sci U S A19969318998599908790444
- WiserAKAndreasenNCO’LearyDSWatkinsGLBoles PontoLLHichwaRDDysfunctional cortico-cerebellar circuits cause ‘cognitive dysmetria’ in schizophreniaNeuroreport199898189518999665622
- ShinYWKwonJSHaTHIncreased water diffusivity in the frontal and temporal cortices of schizophrenic patientsNeuroimage20063041285129116406258
- WhitfordTGrieveSFarrowTVolumetric white matter abnormalities in first-episode schizophrenia: a longitudinal, tensor-based morphometry studyAm J Psychiatry200716471082108917606660
- VolzHGaserCSauerHSupporting evidence for the model of cognitive dysmetria in schizophrenia – a structural magnetic resonance imaging study using deformation-based morphometrySchizophr Res2000461455611099885
- LevittJJMcCarleyRWNestorPGQuantitative volumetric MRI study of the cerebellum and vermis in schizophrenia: clinical and cognitive correlatesAm J Psychiatry199915671105110710401463
- DeLisiLESakumaMGeSKushnerMAssociation of brain structural change with the heterogeneous course of schizophrenia from early childhood through five years subsequent to a first hospitalizationPsychiatry Res1998842–3758810710165
- PantelisCYücelMWoodSJStructural brain imaging evidence for multiple pathological processes at different stages of brain development in schizophreniaSchizophr Bull200531367269616020551
- CollinGDerksEvan HarenNSymptom dimensions are associated with progressive brain volume changes in schizophreniaSchizophr Res20121382–317117622534419
- NagaokaAShinoAIwatsukaHAccelerating effects of dexamethasone and thyroxine on hypertension without accompanying stroke in stroke-prone spontaneously hypertensive ratsLife Sci19792417177763071