
Abstract
Background
Epidemiological studies have repeatedly investigated the association between anxiety and hypertension. However, the results have been inconsistent. This study aimed to summarize the current evidence from cross-sectional and prospective studies that evaluated this association.
Methods
Seven common databases were searched for articles published up to November 2014. Cross-sectional and prospective studies that reported an association between the two conditions in adults were included. Data on prevalence, incidence, unadjusted or adjusted odds ratios or hazard ratios, and 95% confidence intervals (CIs) were extracted or calculated by the authors. The pooled odds ratio was calculated separately for cross-sectional and prospective studies using random-effects models. The Q test and I Citation2 statistic was used to assess heterogeneity. A funnel plot and modified Egger linear regression test were used to estimate publication bias.
Results
The search yielded 13 cross-sectional studies (n=151,389), and the final pooled odds ratio was 1.18 (95% CI 1.02–1.37; PQ<0.001; I2=84.9%). Eight prospective studies with a total sample size of 80,146 and 2,394 hypertension case subjects, and the pooled adjusted hazard ratio was 1.55 (95% CI 1.24–1.94; PQ<0.001; I2=84.6%). The meta-regression showed that location, diagnostic criteria for anxiety, age, sex, sample size, year of publication, quality, and years of follow-up (for prospective study) were not sources of heterogeneity.
Conclusion
Our results suggest that there is an association between anxiety and increased risk of hypertension. These results support early detection and management of anxiety in hypertensive patients.
Introduction
Hypertension, one of the most common diseases worldwide, is estimated to affect one quarter of all adults, and has been identified as the leading cause of mortality and the third cause of disability-adjusted life years worldwide.Citation1 According to a report by Kearney et al the total number of adults with hypertension in 2025 was predicted to increase to 1.56 billion worldwide.Citation2 Identifying and characterizing modifiable risk factors of hypertension remain important for public health and clinical medicine.
Hypertension has a multifactorial etiology, where genetic as well as psychosocial and environmental factors appear to be of importance.Citation3,Citation4 However, there are complex physiological processes involved and the linkage among psychosocial factors and hypertension is not fully understood.Citation5–Citation7 Anxiety is one of the most common psychiatric illnesses in adults and is a major public health problem in many countries,Citation8,Citation9 damaging the affected individual’s health and quality of life.Citation10 Because both hypertension and anxiety confer significant public health challenges, the association between the two conditions has recently attracted attention.
A number of epidemiological studies have been conducted to investigate this association, with inconsistent results reported. Some investigations show that anxiety is associated with hypertension, individuals with anxiety having a higher risk of hypertension than those without anxiety.Citation11–Citation14 Further, hypertension patients have a higher risk of anxiety than those without hypertension.Citation15,Citation16 However, some researchers do not support the role of anxiety symptoms in the development of hypertension.Citation17,Citation18 Some studies have even reported that anxiety is associated with a decrease in blood pressure.Citation19,Citation20 To date, there has not been a meta-analysis to explore the association between anxiety and hypertension. Therefore, we summarized the available data from cross-sectional and prospective studies, and performed meta-analyses to investigate the cross-sectional correlation and longitudinal relationship between anxiety and hypertension.
Methods
Search strategy
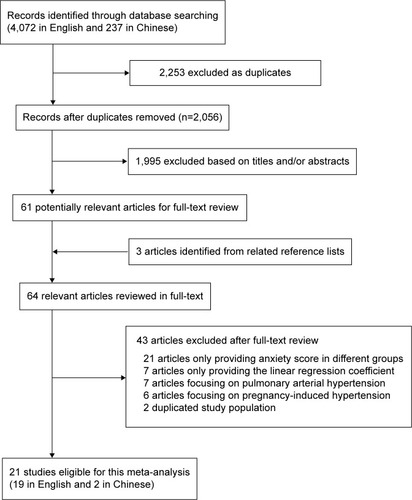
A comprehensive search, restricted to human studies published in the English or Chinese language, was performed using the following databases: PubMed, ISI Web of Science, EMBASE, PsycInfo, China National Knowledge Infrastructure, China Biology Medical literature database, and Database of Chinese Scientific and Technical Periodicals. The search terms (“anxiety” or “worry” or “post-traumatic stress” or “panic” or “agoraphobia” or “phobia” or “obsessive-compulsive”) and (“hyperten*” or “high blood pressure”) were used in various combinations for relevant articles without time restriction ( shows details of the search process and study selection). The last search was performed on November 6, 2014. In addition, we searched and identified studies not captured by our database by reviewing the reference lists in retrieved articles.
Figure 1 Flow diagram of studies selection in meta-analysis.
Inclusion criteria
Articles were considered for inclusion in the systematic review if: the authors reported data from an original, peer-reviewed study (ie, not case reports, comments, letters, meeting abstracts, or review articles); the study was a cross-sectional or prospective study with an adult population (age ≥18 years); the exposure of interest was one or more types of anxiety defined according to standard instruments: and odds ratio (OR), relative risk, or hazard ratio (HR) with 95% confidence interval (CI; or data to calculate it) were reported. If multiple articles were published from the same population, the most informative report was included.
Data extraction and quality assessment
The following data were extracted from each study: the first author’s name, year of publication, study site, number of participants, and years of follow-up for prospective studies, participants’ characteristics (age range or mean age and sex composition), anxiety measures, analysis strategy (statistical models and covariates adjusted in the models), and results (prevalence, incidence, unadjusted or adjusted OR, and 95% CI). For some studies providing ORs for different types of anxiety, we used meta-analysis to incorporate these values into one combined OR that presents the association of anxiety with hypertension. The nine-star Newcastle-Ottawa ScaleCitation21 and eleven-score Agency for Healthcare Research and QualityCitation22 were used, respectively, to estimate the quality of prospective studies and cross-sectional studies. Study inclusion, data extraction, and quality assessment were performed by two independent investigators (YP and JY). Any disagreement was settled by discussion among all of the authors.
Statistical analysis
The research strategy has been described in previous studies.Citation23 The pooled measure was calculated as the inverse variance-weighted mean of the logarithm of the OR (HR) with 95% CI to assess the strength of association between anxiety disorders and risk of hypertension. Heterogeneity among studies was assessed using the Q test and the I2 statistic, which describes the proportion of total variation attributable to between-study heterogeneity as opposed to random error or chance.Citation24 In the presence of substantial heterogeneity (I2>50%),Citation25 the DerSimonian and Laird random effect model (REM) was applied as the pooling method; otherwise, the fixed effect model was adopted. Meta-regression with restricted maximum likelihood estimation was performed to assess the potentially important covariates exerting substantial impact on between-study heterogeneity. The “leave one out” sensitivity analysisCitation26 was conducted using I2>50% as the criterion to assess the key studies with substantial impact on between-study heterogeneity. An analysis of influence was conducted,Citation27 which describes how robust the pooled estimator is to removal of individual studies. An individual study is suspected of excessive influence if the point estimate of its omitted analysis lies outside the 95% CIs of the combined analysis. Publication bias was estimated using Egger’s regression asymmetry test.Citation28 All statistical analyses were performed using STATA/SE version 13.1 (Stata Corporation, College Station, TX, USA). All P-values were two-sided, and those less than 0.05 were considered to be statistically significant.
Results
Literature search and study selection
The study’s identified and selected procedures are summarized in . Twenty-one studies were finally included in our analysis. Among them, 13 cross-sectional studiesCitation11,Citation15,Citation18,Citation20,Citation29–Citation37 (two in the USA, five in Europe, three in the People’s Republic of China, one in Brazil, one in South Africa, and one worldwide) and eight prospective studiesCitation6,Citation12–Citation14,Citation17,Citation38–Citation40 (six in the USA and two in Europe) of the association between anxiety and hypertension were included in the analysis. General characteristics in the published articles included in this meta-analysis are shown in and . The duration of follow-up ranged from 1 to 25 years for the prospective studies. Stars in and indicate the quality of the study. Among the 13 studies in , three scored nine stars, five scored eight stars, and five scored seven stars. Among the eight studies in , one scored nine stars, five scored eight stars, and one scored six stars. The ORs were extracted or calculated from the original articles. Other characteristics, such as age of participants, sample size, and diagnostic criteria for anxiety were also presented in and .
Table 1 Characteristics of cross-sectional studies in the meta-analysis
Table 2 Characteristics of prospective studies included in the meta-analysis
Cross-sectional studies of the association between anxiety and hypertension
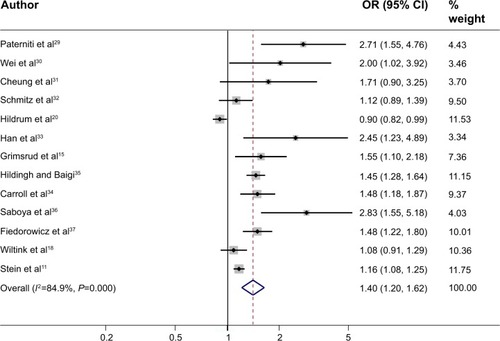
Thirteen cross-sectional studies including 151,389 subjects were included in the analysis of the association of anxiety with risk of hypertension. REM was used because substantially significant between-study heterogeneity was observed (PQ<0.001; I2=84.9%). Pooled results showed that anxiety had a significant positive association with hypertension (OR 1.40, 95% CI 1.20–1.62; ). Significant publication bias was detected (P=0.016). After trim and fill analysis, the final result was still significant (OR 1.18, 95% CI 1.02–1.37).
Figure 2 Random effects meta-analysis of cross-sectional studies of the association between anxiety and hypertension (13 studies included).
Abbreviations: OR, odds ratio; CI, confidence interval.
Prospective studies of anxiety predicting hypertension risk
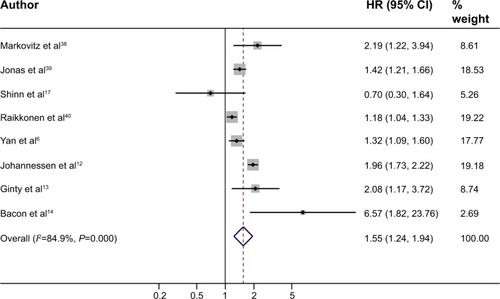
Eight prospective studies investigated the association between the baseline anxiety status and incident hypertension with a total sample size of 80,146 and 2,394 hypertension case subjects. Characteristics of the studies are shown in . The pooled adjusted HR by REM was 1.55 (95% CI 1.24–1.94; ), with strong heterogeneity detected (PQ<0.001; I2=84.6%). No publication bias was detected (P=0.663).
Figure 3 Random effects meta-analysis of prospective studies of the association between anxiety and risk of hypertension (eight studies included).
Abbreviations: HR, hazards ratio; CI, confidence interval.
Sources of heterogeneity and sensitivity analysis
The strong heterogeneities between studies were found in both cross-sectional studies and prospective studies. The univariate meta-regression, with the covariates of location (categorized as American, European, East Asian, and other), diagnostic criteria for anxiety (categorized as structured diagnostic interviews, ie, Diagnostic and Statistical Manual of Mental Disorders or International Classification of Diseases, and self-report symptom scales), age (categorized only as middle-aged and other) and sex, sample size, year of publication, quality, and years of follow-up (≥7 and <7, only for prospective study), showed that none of the aforementioned covariates had a significant impact on between-study heterogeneity.
Subgroup analyses for location, diagnostic criteria for anxiety, age, sex, years of follow-up (only for prospective study) also did not find a source of heterogeneity and indicated that the effects of anxiety in nearly all subgroups were still significant ().
Table 3 Subgroup analyses to explore source of heterogeneity
“Leave one out” sensitivity analysis was performed for the all groups with an I2>50%, and the pooled results did not change substantially.
Discussion
To the best of our knowledge, this is the first meta-analysis examining the association between anxiety and hypertension using data from both cross-sectional and prospective studies. We found that anxiety and hypertension were significantly correlated in cross-sectional studies, and a direct association was also observed in prospective studies.
Some cross-sectional studies reported a higher anxiety score in participants with hypertension than for those without hypertension. However, the methods used for assessment of anxiety varied significantly in the different studies. Therefore, we could not pool the anxiety scores; instead, we pooled the ORs, a measure of association that was more consistent across studies. Our final pooled OR was 1.18 (95% CI 1.02–1.37), suggesting that anxiety and hypertension are significantly related. The pooled ORs remained significant in subgroups for location, diagnosis criteria for anxiety, age, and sex. Although strong heterogeneity was found, meta-regression showed that the location, diagnostic criteria for anxiety, age and sex, sample size, year of publication and quality were not the source of between-study heterogeneity.
Cross-sectional studies do not provide the temporal relationship between anxiety and hypertension, so we conducted a further meta-analysis to investigate the association between anxiety and hypertension in prospective studies. The pooled adjusted HR by REM was 1.55 (95% CI 1.24–1.94), indicating that anxiety was an independent risk factor for incident hypertension. This prospective association between anxiety and hypertension was consistent with results from the cross-sectional studies and also in agreement with two recent meta-analyses showing a reciprocal association between anxiety and coronary heart diseaseCitation41 and between anxiety and heart rate variability.Citation42 Anxiety and depression are closely linked.Citation43 A previous review also shows an increased risk of hypertension in depressed patients and an increased risk of depression in hypertensive patients.Citation44 However, a recent meta-analysis in the elderly does not support that view that hypertension is a possible risk factor of depression.Citation45 Considering current contradictory results in original articles,Citation46 a systematic review should be undertaken to explore the relationship between depression and hypertension with the most up-to-date evidence.
The mechanism between anxiety and hypertension is complex. Generally, anxiety increases blood pressure, systemic vascular resistance, sympathetic activity, plasma renin activity, the homeostasis model, and blood lipids. First, anxiety increases blood pressure in the short term, and the white coat effect derived from anxiety is a typical example.Citation47,Citation48 A recent ambulatory blood pressure monitoring study reported that anxiety disorder was associated with nocturnal and early morning hypertension in hypertensive outpatients.Citation49 Second, anxiety has a close relationship with the renin angiotensin system and increases the level of angiotensin II.Citation50,Citation51 Long-term anxiety may decrease vascular variability, so that persistent vascular resistance leads to hypertension.Citation52 Third, some experiments show that patients with anxiety usually have physiological signs of sympathetic activation, and anxiety can strongly stimulate sympathetic nervous outflow and the vasovagal reflex.Citation53,Citation54 Rozanski et al contend that anxiety can activate the sympathetic nervous system, increase cardiac output, constrict blood vessels, and raise arterial blood pressure.Citation55
Moreover, a long-term anxiety state will improve the sympathetic response and more easily activate the sympathetic nervous system.Citation56 Activation of the sympathetic nervous system not only reduces renal blood flow, increases renal water and sodium retention, and elevates blood pressure,Citation57 but also damages endothelial cells, causes endothelial dysfunction and increasing the risk of atherosclerosis. Sympathetic activation can cause abnormal hemodynamic changes and abnormal lipid metabolism, such as decreasing high-density lipoprotein cholesterol and increasing low-density lipoprotein cholesterol, which affects endothelial function.Citation58 In addition, endothelial cells in animals with heightened sympathetic nervous activity present structural changes and greater immunoreactivity.Citation59 Fourth, the hypothalamo-pituitary-adrenal axis is the major physiological stress response system in the body.Citation60 When this axis is dysfunctional, increasing steroid hormone secretion causes water and sodium retention, leading to high blood pressure.Citation61 Further, the indirect association between anxiety and increased risk of hypertension might also derive from the characteristics of anxious subjects, who usually have a more unhealthy lifestyle in general. In other words, they usually have some adverse behaviors, such as increased eating, smoking, and alcohol use, and take less exercise, due to stress and anxiety, that impacts health.Citation62
On the other hand, previous studies have also found that patients with hypertension awareness have an increased risk of anxiety disorders.Citation16,Citation32 Thus, anxiety and hypertension may interact to affect human health. Moreover, anxiety is one of the barriers in treatment of hypertension.Citation63 Khatib et al identify stress, anxiety, and depression as the most common reported barriers hindering or delaying lifestyle modification.Citation64 Therefore, conventional antihypertensive therapy with psychological support and antianxiety treatment, such as diazepam,Citation65 and metacognitive detached mindfulness therapy and stress management trainingCitation66 could achieve better efficacy in hypertensive patients with anxiety.
This meta-analysis had several strengths. It is the first to explicitly examine the association between anxiety and hypertension on the basis of a comprehensive literature search. This meta-analysis also had a large sample size, which increased the accuracy of the effect estimate. However, the potential limitations of this meta-analysis should be considered. First, it only included English and Chinese language articles; eligible articles published in other languages were not included in this analysis, which may influence the pooled estimated value. Second, because of the inability to obtain raw data, we could perform only a study-level but not a patient-level meta-analysis, which enabled us to adjust for multiple factors. Third, the measurements of anxiety varied among the 21 included studies with regard to different diagnostic instruments, so this might affect the pooled results. We suggest that the DSM-IV should be a preferred instrument to diagnose anxiety disorder in the future because it is the newest standard developed by many experts. Fourth, the outcomes of anxiety and hypertension in our study focused on OR, relative risk, and HR, so some studies with other indices, such as a linear regression coefficient, were excluded. Finally, the heterogeneity between studies included in our study should be paid attention to, although some common factors have been considered to detect the source of heterogeneity.
The results of this meta-analysis indicate an association between anxiety and increased risk of hypertension.
Conclusion
It is important to explore the short-term and long-term effect of anxiety on hypertension. In addition, importance should be attached to the bidirectional association between anxiety and hypertension, especially in the treatment of hypertension. Moreover, the association between anxiety and increased risk of hypertension in this meta-analysis might be confounded by various factors. Therefore, large-scale, randomized controlled trials are recommended to assess the impact of anxiety on incidence rates of hypertension.
Acknowledgments
The study was supported by the army logistics scientific research funds (AWS13J003), the Psychological Subject of the General Logistics Department (12XLZ211), and the National Science and Technology Support Project (2009BAI77B04).
Disclosure
All authors declare that they have no competing interests in this work.
References
- World Health OrganizationGlobal health risks: mortality and burden of disease attributable to selected major risks Available from: http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdfAccessed January, 19 2015
- KearneyPMWheltonMReynoldsKMuntnerPWheltonPKHeJGlobal burden of hypertension: analysis of worldwide dataLancet2005365945521722315652604
- FavaCDaneseEMontagnanaMSerine/threonine kinase 39 is a candidate gene for primary hypertension especially in women: results from two cohort studies in SwedesJ Hypertens201129348449121178783
- KowalikMPsychosomatic aspects of arterial hypertension in womenAnn Univ Mariae Curie Sklodowska Med200459124524916145989
- MarkovitzJHJonasBSDavidsonKPsychologic factors as precursors to hypertensionCurr Hypertens Rep200131253211177704
- YanLLLiuKMatthewsKADaviglusMLFergusonTFKiefeCIPsychosocial factors and risk of hypertension: the Coronary Artery Risk Development in Young Adults (CARDIA) studyJAMA2003290162138214814570949
- ByrdJBBrookRDAnxiety in the “age of hypertension”Curr Hypertens Rep2014161048648625164965
- ReevesWCStrineTWPrattLAMental illness surveillance among adults in the United StatesMMWR Surveill Summ201160Suppl 312921881550
- McEvoyPMGroveRSladeTEpidemiology of anxiety disorders in the Australian general population: findings of the 2007 Australian National Survey of Mental Health and WellbeingAust N Z J Psychiatry2011451195796722044173
- MendlowiczMVSteinMBQuality of life in individuals with anxiety disordersAm J Psychiatry2000157566968210784456
- SteinDJAguilar-GaxiolaSAlonsoJAssociations between mental disorders and subsequent onset of hypertensionGen Hosp Psychiatry201436214214924342112
- JohannessenLStrudsholmUFoldagerLMunk-JørgensenPIncreased risk of hypertension in patients with bipolar disorder and patients with anxiety compared to background population and patients with schizophreniaJ Affect Disord2006951–3131716777235
- GintyATCarrollDRoseboomTJPhillipsACde RooijSRDepression and anxiety are associated with a diagnosis of hypertension 5 years later in a cohort of late middle-aged men and womenJ Hum Hypertens201327318719022592133
- BaconSLCampbellTSArsenaultALavoieKLThe impact of mood and anxiety disorders on incident hypertension at one yearInt J Hypertens2014201495309424672713
- GrimsrudASteinDJSeedatSWilliamsDMyerLThe association between hypertension and depression and anxiety disorders: results from a nationally-representative sample of South African adultsPLoS One200945e555219440241
- HamerMBattyGDStamatakisEKivimakiMHypertension awareness and psychological distressHypertension201056354755020625078
- ShinnEHPostonWSCKimballKTSt JeorSTForeytJPBlood pressure and symptoms of depression and anxiety: a prospective studyAm J Hypertens200114766066411482304
- WiltinkJBeutelMETillYPrevalence of distress, comorbid conditions and well being in the general populationJ Affect Disord2011130342943721106250
- HildrumBRomildUHolmenJAnxiety and depression lowers blood pressure: 22-year follow-up of the population based HUNT study, NorwayBMC Public Health20111160121797992
- HildrumBMykletunAStordalEBjellandIDahlAAHolmenJAssociation of low blood pressure with anxiety and depression: the Nord-Trondelag Health StudyJ Epidemiol Community Health2007611535817183016
- WellsGASheaBO’ConnellDThe Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses2000 Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.aspAccessed January 19, 2015
- RostomADubéCCranneyACeliac Disease-Appendix D Quality Assessment FormsRockville, MD, USAAgency for Healthcare Research and Quality2004
- PanAKeumNOkerekeOIBidirectional association between depression and metabolic syndrome: a systematic review and meta-analysis of epidemiological studiesDiabetes Care20123551171118022517938
- HigginsJPThompsonSGQuantifying heterogeneity in a meta-analysisStat Med200221111539155812111919
- HigginsJPThompsonSGDeeksJJAltmanDGMeasuring inconsistency in meta-analysesBMJ2003327741455756012958120
- PatsopoulosNAEvangelouEIoannidisJPSensitivity of between-study heterogeneity in meta-analysis: proposed metrics and empirical evaluationInt J Epidemiol20083751148115718424475
- TobiasAAssessing the influence of a single study in the meta-analysis estimateStata Technical Bulletin1999471517
- EggerMDavey SmithGSchneiderMMinderCBias in meta-analysis detected by a simple, graphical testBMJ199731571096296349310563
- PaternitiSAlperovitchADucimetierePDealbertoMJLepineJPBisserbeJCAnxiety but not depression is associated with elevated blood pressure in a community group of French elderlyPsychosom Med1999611778310024070
- WeiTZengCChenLWangSLiSChenQAnxiety or/and depression in patients with hypertensionChinese Journal of Hypertension200366870 Chinese
- CheungBMAuTChanSThe relationship between hypertension and anxiety or depression in Hong Kong ChineseExp Clin Cardiol2005101212419641663
- SchmitzNThefeldWKruseJMental disorders and hypertension: factors associated with awareness and treatment of hypertension in the general population of GermanyPsychosom Med200668224625216554390
- HanJYinXMXuFHongXLiangYQWangZYA case-control study on depression and anxiety in hypertensive patientsZhonghua Liu Xing Bing Xue Za Zhi2008292125127 Chinese18686850
- CarrollDPhillipsACGaleCRBattyGDGeneralized anxiety and major depressive disorders, their comorbidity and hypertension in middle-aged menPsychosom Med2010721161919933507
- HildinghCBaigiAThe association among hypertension and reduced psychological well-being, anxiety and sleep disturbances: a population studyScand J Caring Sci201024236637120102543
- SaboyaPMZimmermannPRBodaneseLCAssociation between anxiety or depressive symptoms and arterial hypertension, and their impact on the quality of lifeInt J Psychiatry Med201040330732021166340
- FiedorowiczJGHeJMerikangasKRThe association between mood and anxiety disorders with vascular diseases and risk factors in a nationally representative sampleJ Psychosom Res201170214515421262417
- MarkovitzJHMatthewsKAKannelWBCobbJLD’AgostinoRBPsychological predictors of hypertension in the Framingham Study. Is there tension in hypertension?JAMA199327020243924438230620
- JonasBSFranksPIngramDDAre symptoms of anxiety and depression risk factors for hypertension? Longitudinal evidence from the National Health and Nutrition Examination Survey I Epidemiologic Follow-up StudyArch Fam Med19976143499003169
- RaikkonenKMatthewsKAKullerLHTrajectory of psychological risk and incident hypertension in middle-aged womenHypertension200138479880211641289
- RoestAMMartensEJde JongePDenolletJAnxiety and risk of incident coronary heart disease: a meta-analysisJ Am Coll Cardiol2010561384620620715
- ChalmersJAQuintanaDSAbbottMJKempAHAnxiety disorders are associated with reduced heart rate variability: a meta-analysisFront Psychiatry201458025071612
- SteinDJGurejeODepression and anxiety in the developing world: is it time to medicalise the suffering?Lancet2004364943023323415262087
- ScalcoAZScalcoMZAzulJBLotufo NetoFHypertension and depressionClinics (Sao Paulo)200560324125015962086
- LongJDuanGTianWHypertension and risk of depression in the elderly: a meta-analysis of prospective cohort studiesJ Hum Hypertens11202014 Epub ahead of print
- LichtCMde GeusEJSeldenrijkADepression is associated with decreased blood pressure, but antidepressant use increases the risk for hypertensionHypertension200953463163819237679
- SpruillTMPickeringTGSchwartzJEThe impact of perceived hypertension status on anxiety and the white coat effectAnn Behav Med20073411917688391
- OgedegbeGPickeringTGClemowLThe misdiagnosis of hypertension: the role of patient anxietyArch Intern Med2008168222459246519064830
- KayanoHKobaSMatsuiTAnxiety disorder is associated with nocturnal and early morning hypertension with or without morning surge – ambulatory blood pressure monitoringCirc J20127671670167722481104
- SaavedraJMAndoHArmandoIAnti-stress and anti-anxiety effects of centrally acting angiotensin II AT1 receptor antagonistsRegul Pept2005128322723815837532
- BraszkoJJKulakowskaAWinnickaMMEffects of angiotensin II and its receptor antagonists on motor activity and anxiety in ratsJ Physiol Pharmacol200354227128112832727
- FujinoTNakagawaNYuhkiKDecreased susceptibility to renovascular hypertension in mice lacking the prostaglandin I 2 receptor IPJ Clin Invest2004114680581215372104
- LambertEDawoodTStraznickyNAssociation between the sympathetic firing pattern and anxiety level in patients with the metabolic syndrome and elevated blood pressureJ Hypertens201028354355020139772
- BajkoZSzekeresCCKovacsKRAnxiety, depression and autonomic nervous system dysfunction in hypertensionJ Neurol Sci20123171–211211622425019
- RozanskiABlumenthalJAKaplanJImpact of psychological factors on the pathogenesis of cardiovascular disease and implications for therapyCirculation199999162192221710217662
- NaritaKMurataTHamadaTInteractions among higher trait anxiety, sympathetic activity, and endothelial function in the elderlyJ Psychiatr Res200741541842716494899
- DiBonaGFThe sympathetic nervous system and hypertension: recent developmentsHypertension200443214715014707153
- ManciaGGrassiGThe autonomic nervous system and hypertensionCirc Res2014114111804181424855203
- HarrisKFMatthewsKAInteractions between autonomic nervous system activity and endothelial function: a model for the development of cardiovascular diseasePsychosom Med200466215316415039499
- KudielkaBMWüstSHuman models in acute and chronic stress: assessing determinants of individual hypothalamus-pituitary-adrenal axis activity and reactivityStress200913111420105052
- HashimotoKMakinoSHirasawaRAbnormalities in the hypothalamo-pituitary-adrenal axis in spontaneously hypertensive rats during development of hypertensionEndocrinology19891253116111672547578
- BonnetFIrvingKTerraJLNonyPBerthezeneFMoulinPAnxiety and depression are associated with unhealthy lifestyle in patients at risk of cardiovascular diseaseAtherosclerosis2005178233934415694943
- BautistaLEVera-CalaLMColomboCSmithPSymptoms of depression and anxiety and adherence to antihypertensive medicationAm J Hypertens201225450551122258334
- KhatibRSchwalmJDYusufSPatient and healthcare provider barriers to hypertension awareness, treatment and follow up: a systematic review and meta-analysis of qualitative and quantitative studiesPLoS One201491e8423824454721
- GrossmanENadlerMSharabiYThalerMShacharAShamissAAntianxiety treatment in patients with excessive hypertensionAm J Hypertens2005189 Pt 11174117716182105
- AhmadpanahMPaghaleSJBakhtyariAEffects of psychotherapy in combination with pharmacotherapy, when compared to pharmacotherapy only on blood pressure, depression, and anxiety in female patients with hypertensionJ Health Psychol1072014 Epub ahead of print