
Abstract
Objective
Interactions between psychological, biological and environmental factors are important in development of trichotillomania and skin picking. The aim of this study is to determine the relationship of traumatic life events, symptoms of post-traumatic stress disorder and dissociation in patients with diagnoses of trichotillomania and skin picking disorder.
Methods
The study included patients who was diagnosed with trichotillomania (n=23) or skin picking disorder (n=44), and healthy controls (n=37). Beck Depression Inventory, Traumatic Stress Symptoms Scale and Dissociative Experiences Scale were administered. All groups checked a list of traumatic life events to determine the exposed traumatic events.
Results
There was no statistical significance between three groups in terms of Dissociative Experiences Scale scores (P=0.07). But Beck Depression Inventory and Traumatic Stress Symptoms Scale scores of trichotillomania and skin picking groups were significantly higher than the control group. Subjects with a diagnosis of trichotillomania and skin picking reported statistically significantly higher numbers of traumatic and negative events in childhood compared to healthy subjects.
Conclusion
We can conclude that trauma may play a role in development of both trichotillomania and skin picking. Increased duration of trichotillomania or skin picking was correlated with decreased presence of post-traumatic stress symptoms. The reason for the negatively correlation of severity of post-traumatic stress symptoms and self-harming behavior may be speculated as developing trichotillomania or skin picking symptoms helps the patient to cope with intrusive thoughts related to trauma. Future longitudinal research must focus on whether trauma and post-traumatic stress or trichotillomania and skin picking precede the development of mental disorder.
Introduction
Trichotillomania (TTM) has been first defined in the 19th century as a syndrome that leads to noticeable hair loss by pulling out one’s own hair. The hair pulling behavior is accompanied by a feeling of distress, and it leads to gratification or relief while pulling the hair.Citation1 TTM is mainly involved in pulling out hair, and less frequently pulling out hairs from different parts of the body.Citation2 The bodily area of pulling out hair is reported as 75% scalp hair, 53% eyelashes, 42% eyebrows, 10% beard, and 17% pubic area, and it is seen in more than one area with increasing age.Citation3 TTM was classified under the title of “Impulse Control Disorders Not Classified Elsewhere” in Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-R) and as “Habit and Impulse Disorder” in International Classification of Diseases, tenth revision (ICD-10).Citation4 Although there are many assumptions about TTM, the etiology is not clear.Citation5 While discussing TTM to be classified within the obsessive spectrum before Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5), it has been reported that, in a person suffering from mental trauma, obsessive–compulsive disorder (OCD) symptoms might have been developed in order to cope with anxiety and intrusive thoughts associated with trauma.Citation6
People with TTM might shift their focus from traumatic material to pulling out hair in order to reduce their anxiety. Owing to phenomenological and neurobiological similarities with OCD, several researchers have suggested that TTM might be better conceptualized as an obsessive–compulsive spectrum disorder, and it has been classified under obsessive–compulsive and related disorders title in DSM-5.Citation7,Citation8 Skin picking (SP) is an irresistible scratching and picking urge to the extent that skin lesions are caused by the patients due to excessive excoriation. Frequency of SP is reported to be 2% in patients admitted to a dermatology clinic,Citation9 4% in university students,Citation10 and 5.4% in a nonclinical population.Citation11 SP disorder is mostly accompanied by major depressive disorder and OCD. It is reported to be more frequent in women. Although SP has been recommended to be classified in impulse control disorders not otherwise specified in DSM-IV-TR,Citation12 it was classified in obsessive–compulsive disorder and related disorders section in DSM-5.Citation13
TTM diagnostic criteria are as follows according to DSM-5Citation13:
Trichotillomania
recurrent pulling out of one’s hair, resulting in hair loss;
repeated attempts to decrease or stop hair pulling;
the hair pulling causes clinically significant distress or impairment in social, occupational, or other important areas of functioning;
the hair pulling or hair loss is not attributable to another medical condition (eg, a dermatological condition); and
the hair pulling is not better explained by the symptoms of another mental disorder (eg, attempts to improve a perceived defect or flaw in appearance in body dysmorphic disorder).
SP diagnostic criteria are as follows according to DSM-5Citation13:
SP disorder
recurrent SP resulting in skin lesion;
repeated attempts to decrease or stop SP;
the SP causes clinically significant distress or impairment in social, occupational, or other important areas of functioning; and iv. the SP is not attributable to the physiological effects of a substance (eg, cocaine) or another medical condition.
The SP is not better explained by symptoms of another mental disorder (eg, delusions or tactile hallucinations in a psychotic disorder, attempts to improve a perceived defect or flaw in appearance in body dysmorphic disorder, stereotypies in stereotypic movement disorder, or intention to harm oneself in nonsuicidal self-injury).
Personality allegedly plays a role in the development of TTM and SP.Citation14 Emotionality and emotional regulation difficulties, reward dependence and harm avoidance, have been reported among the personality traits in both disorders.Citation15 Environmental factors, boredom, and lack of stimulation have been reported being possible triggers of hair pulling and SP episodes.Citation14 TTM development has been considered to be a behavioral response to stress in order to reduce anxiety or to cope with anxiety.Citation16,Citation17 Various researchers reported the high frequency of traumatic events in the past history of patients with SPCitation18,Citation19 and TTMCitation6,Citation20 compared to healthy population.
In a study on young women, it has been reported that history of sexual abuse and rape in childhood was one of the predictors of SP, but not of TTM.Citation21 Although trauma history is not reported in all patients with a diagnosis of TTM, childhood trauma is reported to be higher when compared to patients without any psychiatric diagnoses.Citation20,Citation22 Exposure to interpersonal violence is reported to be high during the initial phase of the TTM.Citation20 Approximately 76% of patients with TTM have been found to have a history of at least one traumatic life event, and 19% have a lifetime diagnosis of post-traumatic stress disorder (PTSD).Citation23 Results of research suggest that in patients with TTM, PTSD prevalence was found to be higher than the general population but lower than psychiatric sample.Citation23 It is interesting that the number of pulled hairs and duration of hair pulling are negatively correlated with the severity of comorbid PTSD in TTM patients.Citation6 Regarding the relation between TTT, SP, and dissociative symptoms, it has been reported that one-third of SP patients have a feeling of trance or a feeling of mesmerized during SP.Citation24,Citation25 In a study, 21.3% of the patients with TTM had reported depersonalization during pulling out hair.Citation26 Despite the high frequency of dissociative symptoms in TTM and SP, the number of studies is limited.
This study was aimed to search for the relationship of psychological trauma with TTM and SP. A secondary aim was to investigate the presence of dissociative symptoms with TTM or SP.
Methods
The study included 67 outpatients who had been admitted to the Neuropsychiatry Istanbul Hospital between January 2012 and March 2014 and who were diagnosed with TTM (n=23) or SP disorder (n=44) according to the DSM-IV-TR criteria. Also, age- and sex-matched healthy controls (n=37) were included in the study. The normal controls were selected from hospital staff who were compatible with TTM and SP groups in terms of age, sex, and education. Clinical interviews were conducted by three psychiatrists. Demographic and clinical data of the subjects were recorded. Necessary information was given about self-reported list of traumatic events, Traumatic Stress Symptoms Scale (TSSS), the Dissociative Experiences Scale (DES), and the Beck Depression Inventory (BDI), by interviewing psychiatrists and a clinic psychologist, and the subjects were allowed to fill them in the testing room. Self-reported scales were filled in the test room by the patients and were evaluated diagnosis-blind by the clinic psychologist, after all the data were integrated by the three psychiatrists. Patients suffering from a concurrent mental illness other than TTM or SP were excluded. The study protocol conformed to the Declaration of Helsinki; all patients were fully informed and signed consent forms. This study was approved by the Clinical Research Ethics Committee of Üsküdar University.
Screening tools
Sociodemographic data sheet
Data related to age, sex, education, and marital status; bodily areas of TTM and SP; and family history of TTM, SP, and other psychiatric illnesses were collected. Through clinical interviews, patients were evaluated in terms of the presence of comorbid psychiatric disorders.
Structured clinical interview for DSM Axis I disorders
It was for Turkish sample.Citation27
List of traumatic events
It includes 16 traumatic life events prepared by the researcher in order to determine the traumatic events to which participants were exposed throughout their lives.
Traumatic Stress Symptoms Scale
TSSS was used in order to measure PTSD. It is developed by Başoğlu et al and reliability and validity studies were performed.Citation28 It includes 23 items, and it is a four-item Likert-type scale by which people evaluate themselves for the past 1 month. Each item is scored between 0 and 3, and the total scores are obtained by summing up the scores of each item. The first 17 items question symptoms of PTSD specified in DSM-IV, and the last six items question depressive symptoms. A total score of 25 or more for the first 17 items indicates a possible diagnosis of PTSD. The cutoff point of the scale is 38 when taking all the items into consideration, 25 when taking PTSD items into consideration, and 8 when taking depression items into consideration. Başoğlu et al has reported that sensitivity and specificity for PTSD is 81%.
Dissociative Experiences Scale
To determine dissociative experiences of individuals, the DES with 28 items was used. Each item of the scale is scored between 0 and 100, and the average of the scores is taken. A score above 30 suggests a diagnosis of dissociative disorder. This self-report scale has been designed by Bernstein et al to determine dissociative experiences.Citation29 Validity and reliability studies for the Turkish version have been conducted by Şar et al.Citation30
Beck Depression Inventory
This scale has been designed by Beck to measure depression severity.Citation31 Validity and reliability studies for the Turkish version have been conducted by Hisli.Citation32 It is a Likert-type scale consisting of 21 items, and each item is scored between 0 and 3. Cutoff point for Turkish version is 17.
Statistical analysis
Statistics Package for Social Sciences (SPSS) 15.0 program was used for statistical evaluation. First, data were calculated as percentages and means, and presented as descriptive statistics. One-way analysis of variance (ANOVA) and chi-square tests were used in evaluating the difference between the three groups’ averages. The relationship between sociodemographic variables and clinical scale scores were investigated by Pearson’s correlation test. In the evaluation of all data, the statistical significance was designed as P<0.05 confidence interval.
Results
The study included 104 subjects in three groups. Twenty-three of the subjects were suffering from TTM, 44 from SP, and 37 were healthy controls. The mean ages of the TTM, SP, and control groups were 32.74±9.12, 31.91±9.27, and 30.7±7.32, respectively. Female patients were more than male patients in all groups as 78.3% (n=18) in the TTM group, 75% (n=33) in the SP group, and 64.9% (n=24) in the control group were females. The study groups did not differ statistically significant in terms of age, sex, and marital status. TTM and SP groups did not differ significantly in terms of illness duration. Also, the groups did not differ significantly in terms of education level, family history of psychiatric illness, and family history of TTM or SP. Some demographic and clinical characteristics and statistical significance levels are shown in .
Table 1 The sociodemographic characteristics of the groups
Family history of TTM in TTM and SP groups were 34.8% (n=8) and 13.6% (n=6), respectively. A statistically significant difference was observed between families of the three groups in terms of TTM (P<0.01). In 30.4% (n=7) of the families of the patients with TTM and in 50% (n=22) of the families of the patients with SP, SP disorder was found. The difference was statistically significant between families of the three groups in terms of SP (P<0.01).
The bodily areas of TTM are as 4.3% (n=1) of the patients with TTM were pulling out chest hair, 8.7% (n=2) only eyebrows, 8.7% (n=2) eyebrows and eyelashes, 4.3% (n=1) hair, eyebrows, and eyelashes, and 74% (n=17) only scalp hair. The bodily areas of SP are as 18.2% (n=8) of the SP group were picking only lips, 4.5% (n=2) intraoral picking and finger edges, 2.3% (n=1) heels, 13.6% (n=6) lips and finger edges, 36.4% (n=16) finger edges, 2.3% (n=1) general, and 11.4% (n=5) face ( and ).
Table 2 Symptom areas in patients with trichotillomania
Table 3 Symptom areas in patients with skin picking disorder
There was no statistical significance between the three groups in terms of DES scores (P=0.07). But BDI and TSSS scores differ significantly between the three groups (P=0.02 and P=0.03, respectively). The difference between BDI scores originates from TTM and control groups (P=0.03) and SP and control groups (P=0.01). The clinical scale scores of the three groups are given in .
Table 4 The clinical scale scores of the three groups
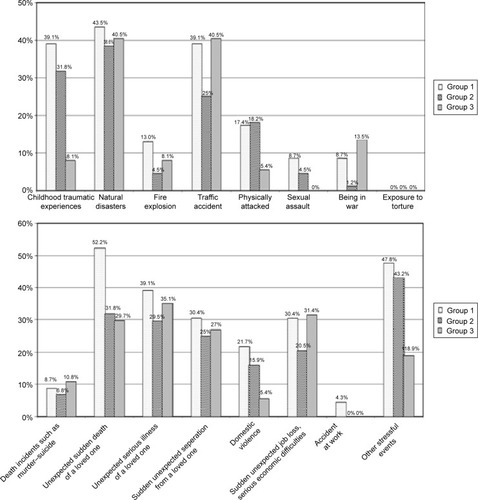
The mean number of reported traumatic life events was 4.0±3.1 in the TTM group, 2.9±2.1 in the SP group, and 2.5±1.4 in the control group (P=0.04). TTM and SP groups did not differ significantly in a number of traumatic life events (P=0.15).
There was no statistically significant difference between the three groups in terms of the types of trauma such as natural disasters (P=0.93), fire explosion (P=0.47), traffic accident (P=0.28), physically attacked (P=0.21), sexual assault (P=0.23), being in war (P=0.17), exposure to torture and other ill-treatment (P=0.25), death incidents such as murder–suicide (P=0.82), unexpected serious illness of a loved one (P=0.17), unexpected sudden death of a loved one (P=0.72), sudden unexpected separation from a loved one (P=0.89), domestic violence (P=0.16), serious economic difficulties (P=0.29), and accidents at work (P=0.17). The difference between the three groups in terms of bad and negative events in childhood (neglect, abuse, extreme violence, sexual harassment, and intercourse = childhood traumatic experiences) was statistically significant (P=0.01). Childhood traumatic experiences in terms of the difference are due to the TTM group ().
Figure 1 Distribution of groups in traumatic life events.
Abbreviations: TTM, trichotillomania; SP, skin picking.
Pearson’s correlation test was applied to sociodemographic data and clinical scale score variables of groups. A positive correlation was found between age and DES (P=0.02, r=−0.29), education and DES (P<0.01, r=−0.29), illness duration and DES (P=0.02, r=−0.28), comorbid illness and TSSS scores (P=0.02, r=+0.27), DES and BDI scores (P<0.01, r=+0.53), and BDI and TSSS scores (P<0.01, r=+0.73). The number of traumatic events was negatively correlated with education (P<0.01, r=−0.31) and positively correlated with comorbid psychiatric illness (P<0.01, r=+0.27), DES score (P<0.01, r=+0.53), and BDI scores (P<0.01, r=+0.73). In all, 30.5% (n=7) of the TTM group and 22.8% (n=10) of the SP group had a diagnosis of PTSD. The average TSSS score of the PTSD diagnosed total group was 36.14±7.5. A total of 80.8% of the total group (n=84) got a score of lesser than 25 points and 19.2% (n=20) got a score above 25 points in TSSS. PTSD positive and negative groups were compared to chi-square test for sociodemographic data and with independent t-test for parametric variables. There was no statistically significant difference observed between the sociodemographic and disease-related variables of PTSD and non-PTSD subjects in the TTM group. In the SP group, there was a difference only in terms of BDI scores between PTSD and non-PTSD subjects (P<0.01). The group with TSSS score over 25 points had a correlation with BDI scores (P<0.01, r=+0.84). In the PTSD negative group, there was a correlation between education level (P<0.01, r=−0.45), DES (P≤0.01, r=+0.32), and BDI scores (P≤0.01, r=+0.49).
There were a total of six subjects with a DES score of ≥30 in this study. In total, 17.4% (n=4) of the TTM group and 4.5% (n=2) of the SP group were diagnosed with dissociative disorder.
Discussion
This study aimed to search for the relationship of psychological trauma with TTM and SP. A secondary aim was to investigate the presence of dissociative symptoms with TTM or SP.
The results of the present study suggest that 34.8% of patients with TTM had TTM history in their families. Previous studies have reported 22.7%Citation33 and 25.5%Citation26 TTM in the families of patients with TTM. In the SP group, we found 50% families with history of TTM. Again, in previous studies, 28.3%Citation26 and 43%Citation19 of the first-degree relatives of the patients with SP disorder has been found to have SP disorder. Although the number of publications is limited, high frequency of positive family history suggests that genetic transmission may be important in the etiology of TTM and SP.Citation34–Citation36 Average duration of illness was found to be 14.83±9.2 years in the TTM group and 13.57±7.8 years in the SP group; it can be said that the average age of onset of TTM and SP was approximately.Citation17,Citation18 In literature, age at disease onset has been defined bimodal as age of childhood and adolescence.Citation33,Citation37 In late onset, more severe course of the disease, greater comorbidity and severity of symptoms, and treatment resistance are observed.Citation38
In our study, BDI scores in TTM and SP groups were significantly higher than healthy subjects. Although BDI scores are not sufficient alone to diagnose major depressive disorder, it refers to depressive tendency. Also in previous studies, risk of developing comorbid mood disorders in patients with TTM has been reported to be increased.Citation33,Citation39 History of traumatic events in childhood, such as neglect, abuse, extreme violence, sexual harassment, or intercourse, and history of any other stressful life events did differ significantly among TTM, SP, and control groups. There was a statistically significant difference in both TTM and SP groups in terms of traumatic and negative events in childhood (neglect, abuse, extreme violence, sexual harassment, and intercourse) when compared to healthy subjects. In a study, childhood sexual trauma has been found as 25.8% and childhood physical abuse as 20.6% in subjects with TTM.Citation6 Gershuny et al reported that the childhood trauma was significantly higher in OCD and TTM groups than in healthy subjects. In this study, emotional neglect was found to be higher in both OCD and TTM groups than in the control group. Physical abuse score in the TTM group was significantly higher than that in healthy controls.Citation6 Boughn and Holdom reported history of violence during the onset of TTM symptoms in 86% of 44 female patients with TTM.Citation20 These studies suggested that childhood traumas may be related to the development of TTM cases. In our study, 30.5% of the TTM group and 22.8% of the SP group were diagnosed with PTSD using TSSS.
In this study, we classified individuals with DES score of ≥30 as possible cases of dissociative disorder, and 17.4% of the TTM group and 4.5% of the SP group were in this group. Congruent with our results, in the study by Lochner et al the frequency of individuals with a DES score of 30 and more was reported as 18.8% in the TTM group.Citation15 In our study and in the study by Lochner et al DES scores were about the same in the TTM group. In studies with Turkish population, the mean DES score was found to be 17.88 and 7.67 in psychiatry inpatients and general population, respectively.Citation40,Citation41 A study investigating the relationship of dissociation and TTM/SP revealed that approximately one in three of the patients with SP was feeling mesmerized during picking behavior.Citation24,Citation25 Another study reported that 21.3% of the patients with TTM reported depersonalization during hair pulling behavior.Citation26
In our study, we found negative correlation between DES and TSSS scores and duration of TTM and SP. In the study by Gershuny et al increased duration and number of hairs pulled were negatively correlated with the presence of PTSD symptoms.Citation6 The reason for the negative correlation of severity of PTSD and TTM may be speculated as developing TTM symptoms helps the patient to cope with intrusive thoughts related to trauma. If TTM is taken into account as a coping mechanism, it may contribute to prevention of PTSD development. The person suffering from the traumatic material may sooth the anxiety by focusing on hair pulling.
The diagnosis of anxiety disorders has encountered various changes in the recently released DSM-5.Citation13 One is the addition of the dissociative subtype of PTSD. The dissociative subtype is not a subset of the core PTSD symptoms, but rather indicates a class of PTSD characterized by additional comorbid symptoms of derealization and/or depersonalization.
Those individuals set a dissociative group who were distinct from those with high PTSD severity and no dissociation and those with low PTSD severity and no dissociation.Citation42
Symptoms of dissociation are important clinical phenomena that may become a target of treatment in cases of TTM with a history of childhood trauma. Dissociative symptoms may also interfere with TTM treatment as dissociation may interfere with the processing of trauma memories and related emotions and cognitions in trauma-focused therapies.
The dissociative symptoms seen in TTM and SP may be associated with a distinct etiology, biology, course, and treatment response. For example, individuals with the dissociative subtype may have different genetic vulnerabilities than individuals who do not dissociate. Providing a clear definition of the TTM and SP comorbidity with dissociative symptomatology would help to understand genetic, neurobiological, cognitive, and psychosocial mechanisms of TTM and SP.
The most obvious limitation of our study is the usage of three self-reported scales (list of traumatic events, TSSS, and DES). The reliability of the scales filled out without a clinician’s intervention is lower than that of structured forms. As the small size of the current study is the major limitation of this study, we cannot come to a conclusion that TTM serves a dissociative or anxiety-relieving function. The study group consisted of individuals who were seeking treatment for TTM or SP. Another limitation of the study is the increased probability of a Type I error associated with multiple t-tests. This is another limitation of the study due to the probability of symptoms of avoidance in individuals with a comorbidity of PTSD; we can speculate that they did not seek treatment and did not participate in the study.
Conclusion
In this study, we included two self-harming groups, SP and TTM, to get information about the relation of self-harming disorders and past traumas. Dissociation, PTSD, and depression mean scores of TTM and SP groups were not statistically different from one another. Although two self-harming groups did not differ significantly from each other in depression or PTSD scores, they were both significantly differing from the healthy control group. We can conclude that trauma and PTSD may play a role in etiology of both TTM and SP. PTSD symptoms reduce with the prolonged TTM and SP illness duration. The reason for the negative correlation of severity of PTSD and TTM may be speculated as developing TTM or SP symptoms helps the patient to cope with intrusive thoughts related to trauma. Future longitudinal research must focus on whether trauma and PTSD or TTM and SP precede the development of mental disorder.
Disclosure
The authors report no conflicts of interest in this work.
References
- ChamberlainSRFinebergNABlackwellADClarkLRobbinsTWSahakianBJA neuropsychological comparison of obsessive–compulsive disorder and trichotillomaniaNeuropsychologia200745465466217005210
- DukeDCKeeleyMLGeffkenGRStrochEATrichotillomania: a current reviewClin Psychol Rev201030218119319926375
- FlessnerCABuschAMHeidemanPWWoodsDWAcceptance-enhanced behavior therapy (AEBT) for trichotillomani and chronic skin picking: exploring the effects of component sequencingBehav Modif200832557959418334614
- World Health OrganizationThe ICD-10 Classification of Mental and Behavioural Disorders Clinical Descriptions and Diagnostic GuidelinesGenevaWHO1992
- KeuthenNJSteinDJChristensonGAHelp for Hair Pullers: Understanding and Coping with TrichotillomaniaOaklandNew Harbinger Publications2001
- GershunyBSBaerLRadomskyASWilsonKAJenikeMAConnections among symptoms of obsessive–compulsive disorder and posttraumatic stress disorder: a case seriesBehav Res Ther20034191029104112914805
- ShoenfeldNRosenbergOKotlerMDannonPNTrichotillomania: pathopsychology theories and treatment possibilitiesIsr Med Assoc J201214212512922693797
- BaerLOsgood-HynesDMinichielloWETrichotillomaniaAmmermanRTLastCGHersenMHandbook of Prescriptive Treatments for Children and AdolescentsNeedham Heights, MAAllyn & Bacon1999277292
- ArnoldLMAuchenbachMBMcElroySLPsychogenic excoriation. Clinical features, proposed diagnostic criteria, epidemiology and approaches to treatmentCNS Drugs200115535135911475941
- BohneAWilhelmSKeuthenNJBaerLJenikeMESkin picking in German students. Prevalence, phenomenology, and associated characteristicsBehav Modif200226332033912080904
- HayesSLStorchEABerlangaLSkin picking behaviors: an examination of the prevalence and severity in a community sampleJ Anxiety Disord200923331431919223150
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders4th edWashington, DCAmerican Psychiatric Association1994
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders5th edWashington, DCAmerican Psychiatric Association2013
- ShustermanAFeldLBaerLKeuthenNAffective regulation in trichotillomania: evidence from a large-scale internet surveyBehav Res Ther200947863764419467648
- LochnerCdu ToitPLZungu-DirwayiNMaraisAvan KradenburgJSeedatSChildhood trauma in obsessive–compulsive disorder, trichotillomania, and controlsDepress Anxiety2002152666811891995
- DiefenbachGJReitnamDWilliamsonDATrichotillomania: a challenge to research and practiceClin Psychol Rev20002028930910779896
- WhiteKressVEKellyBLMcCormickLJTrichotillomania: assessment, diagnosis, and treatmentJ Couns Dev2004822185190
- BordnickPSThyerBARitchieBWFeather picking disorder and trichotillomania: an avian model of human psychopathologyJ Behav Ther Exp Psychiatry1994251891967852601
- NezirogluFRabinowitzDBreytmanAJacofskyMSkin picking phenomenology and severity comparisonPrim Care Companion J Clin Psychiatry200810430631218787665
- BoughnSHoldomJAJThe relationship of violence and trichotillomaniaJ Nurs Scholarsh20033516517012854298
- FavaroAFerraraSSantonastasoPSelf-injurious behavior in a community sample of young women: relationship with childhood abuse and other types of self-damaging behaviorsJ Clin Psychiatry200768112213117284140
- LochnerCSeedatSHemmingsSMJKinnearCJCorfieldVANiehausDJHRDissociative experiences in obsessive–compulsive disorder and trichotillomania: clinical and genetic findingsCompr Psychiatry20044538439115332202
- GershunyBSKeuthenNJGentesELRussoAREmmottECJamesonMCurrent posttraumatic stress disorder and history of trauma in trichotillomaniaJ Clin Psychol200662121521152916897695
- SonarrasonISmariJOlafssonRPEmotion regulation in pathological skin picking: findings from a non-treatment seeking sampleJ Behav Ther Exp Psychiatry20104123824520172501
- WilhelmSKeuthenNJDeckersbachTEngelhardIMForkerAEBearLSelf-injurious skin picking: clinical characteristics and comorbidityJ Clin Psychiatry19996045445910453800
- du ToitPLvan KradenburgJNiehausDJHSteinDJCharacteristics and phenomenology of hair-pulling: an exploration of subtypesCompr Psychiatry20014224725611349246
- ÖzkürkçügilAAydemirÖYıldızMDanacıEAKöroğluEReliability and validity of the Turkish version of the Structured Clinical Interview for DSM-IV [DSM-IV eksen I bozuklukları için yapılandırılmış klinik görüşmenin türkçeye uyarlanması ve güvenilirlik çalışması]İlaç ve Tedavi Dergisi199912233236
- BaşoğluMŞalcıoğluELivanouMAStudy of the validity of a screening instrument for traumatic stress in earthquake survivors in TurkeyJ Trauma Stress20011449150911534881
- BernsteinEMPutnamFWFrankWDevelopment, reliability and validity of a dissociation scaleJ Nerv Ment Disord198647285293
- ŞarVKundakçıTKızıltanEDisosiyatif Yaşantılar Ölçeği’nin (DES-II) geçerlik ve güvenirliği. [Dissociative Experiences Scale (DES-II) reliability and validity]Ulusal Psikiyatri KongresiAntalya199733 Turkish
- BeckATWardCHMendelsonMMockJErbaughJAn inventory for measuring depressionArch Gen Psychiatry1961456157113688369
- HisliNThe reliability and validity analysis of the Turkish version of Beck Depression Inventory in university students. [Beck Depresyon Envanterinin üniversite öğrencileri için geçerliliği, güvenirliği]Psikoloji Dergisi19897313
- SchlosserSBlackDWBlumNGoldsteinRBThe demography, phenomenology, and family history of 22 persons with compulsive hair pullingAnnals Clin Psychiatry19946147152
- OdlaugBLGrantJEPathologic skin pickingGrantJESteinDJWoodsDWKeuthenNJTrichotillomania, Skin Picking, and Other Body-Focused Repetitive BehaviorsWashington, DCAmerican Psychiatric Publishing20122141
- GreerJMCapecchiMRHoxb8 is required for normal grooming behavior in miceNeuron2000331233411779477
- ZuchnerSCuccaroMLTran-VietKNCopeHKrishnanRRPericak-VanceMASLITRK1mutations in trichotillomaniaMol Psychiatry20061188788917003809
- MansuetoCSRogersKETrichotillomania: Epidemiology and Clinical Characteristics Clinical Manual for the Treatment of Trichotillomania, Skin-picking, and Other Stereotypic DisordersArlington, VAAmerican Psychiatric Publishing2011
- LewinABPiacentiniJFlessnerCAWoodsDWFranklinMEKeuthenNJDepression, anxiety, and functional impairment in children with trichotillomaniaDepress Anxiety200926652152719016486
- DukeDCBodzinDKTavaresPGeffkenGRStorchEAThe phenomenology of hair pulling in a community sampleJ Anxiety Disord20092381118112519651487
- TutkunHSarVYargicLIOzpulatTYanıkMKızıltanEFrequency of dissociative disorders among psychiatric inpatients in a Turkish University ClinicAm J Psychiatry19981558008059619153
- AkyuzGDoganOSarVYargicLITutkunHFrequency of dissociative identity disorder in the general population in TurkeyCompr Psychiatry19994015115910080263
- SteinDJKoenenKCFriedmanMJHillEMcLaughlinKAPetukhovaMDissociation in posttraumatic stress disorder: evidence from the world mental health surveysBiol Psychiatry20137330231223059051