Abstract
Paliperidone palmitate is a new long-acting antipsychotic injection for the treatment of acute and maintenance therapy in schizophrenia. Paliperidone (9-hydroxyrisperidone) is the major active metabolite of risperidone and acts at dopamine D2 and serotonin 5HT2A receptors. As with other atypical antipsychotics, it exhibits a high 5HT2A:D2 affinity ratio. It also has binding activity as an antagonist at α1-and α2 adrenergic receptors and H1 histaminergic receptors, but has virtually no affinity for cholinergic receptors. Paliperidone palmitate has been shown to be effective in reducing Positive and Negative Syndrome Scale total scores in four short-term trials in acute schizophrenia. It was also effective as maintenance therapy in a long-term trial in which time to recurrence of symptoms was significantly longer in paliperidone-treated patients compared with placebo. In addition, paliperidone was shown to be noninferior to risperidone long-acting injection in one study, but this noninferiority was not established in another longer study comparing the two drugs. Treatment should be initiated with 234 mg on day 1 and 156 mg on day 8, followed by a recommended monthly maintenance dose of 39–234 mg based on efficacy and tolerability. Paliperidone palmitate is generally well tolerated, although it can cause weight gain and a rise in prolactin levels, which is generally greater in women than in men. Overall, paliperidone palmitate may have advantages over other currently available long-acting injections, and therefore may be a useful alternative for the treatment of schizophrenia, although further long-term trials comparing it with active treatments are warranted.
Introduction
Poor compliance with medication remains a major cause for concern in the management of schizophrenia. It has been shown that more than 35% of patients experience compliance problems within the first few weeks of therapy, and only 25% are fully compliant after two years.Citation1 A combination of factors may contribute to this problem, including lack of insight, negative symptoms, cognitive decline, and poor tolerability of available agents. These have a major negative impact on compliance which, in turn, leads to considerable risk of relapse, thus reducing the likelihood of full recovery to the baseline level of functioning.Citation1
Conventional antipsychotic depot formulations were first introduced in the 1960s as a means to improve compliance with therapy. However, the negative symptoms of schizophrenia are not adequately managed by these older drugs, and their high propensity to cause extrapyramidal symptoms and raised prolactin levels has limited their use over time. Of late, after many years of research and development, pharmaceutical companies have also succeeded in formulating certain atypical antipsychotics into long-acting injections. Risperidone was the first atypical agent to be formulated as a long-acting injection, administered every two weeks. However, supplementary oral treatment is required for the first 4–6 weeks of intramuscular therapy due to the delay in reaching steady-state plasma levels. In addition, although the three licensed doses (25 mg, 37.5 mg, and 50 mg every two weeks) have been shown to be equally effective in clinical trials, the lowest dose (25 mg every two weeks) has been shown to be relatively less effective in practice.Citation2
Olanzapine has also been recently formulated into a pamoate suspension for intramuscular administration every 2–4 weeks. With this product, a safety risk emerged during clinical trials known as “post-injection syndrome”, consisting of an unexpected high degree of sedation, confusion, dizziness, altered speech, and/or unconsciousness occurring in a small number of patients following injection.Citation3 The incidence of this has been estimated as 1.2% of patients treated, or 0.07% of injections given.Citation4 The formulation went on to gain its license despite this adverse effect, but with the recommendation that a three-hour patient observation period follow each injection, a restriction that will most likely limit its use for practical reasons, as well as the safety issues involved.Citation4
While the introduction of atypical antipsychotic drugs has been of some benefit to patients, the use of these new agents has been accompanied by serious adverse effects also limiting their clinical use. Atypical antipsychotics have been implicated in the development of metabolic disorder,Citation5 consisting of raised cholesterol and triglycerides alongside impaired glucose tolerance.Citation6 The likelihood of experiencing these adverse effects varies amongst the different drugs in this class. Furthermore, considerable weight gainCitation7 is an additional risk, often leading to early treatment discontinuation and poor compliance with therapy. As a result, despite the increasing number of agents being developed for the management of schizophrenia, there are still many individuals who are not receiving adequate benefit or not able to tolerate currently available agents. The introduction of paliperidone once-monthly injections is therefore a welcome addition to the market. In this paper, the pharmacology, pharmacokinetics, efficacy, and safety of paliperidone palmitate are reviewed, and its potential place in the treatment of schizophrenia is discussed.
Paliperidone palmitate
Paliperidone palmitate is the most recent atypical antipsychotic to be developed as a long-acting injection and was approved by the US Food and Drug Administration in August 2009 for acute and maintenance therapy in adult patients with schizophrenia. A marketing authorization application has been submitted to the European Medicines Agency, whereby following approval, it will be marketed in Europe, and marketing applications in other areas of the world are ongoing.
Pharmacology
Paliperidone, also described as 9-hydroxyrisperidone, is the major active metabolite of risperidone. Its pharmacology and mechanism of action are therefore believed to be similar to that of risperidone. Paliperidone acts as an antagonist at dopamine D2 and serotonin 5HT2A receptors, exhibiting a high 5HT2A:D2 affinity ratio, as with other atypical agents.Citation8 It also has binding activity as an antagonist at α1- and α2-adrenergic receptors and H1-histaminergic receptors, but has virtually no affinity for cholinergic receptors.Citation8–Citation10 Paliperidone’s activity profile suggests that it has the potential to cause orthostatic hypotension, weight gain, and sedation. However, because it has no antagonistic activity at cholinergic receptors, it has a low propensity to cause anticholinergic adverse effects and cognitive impairment.
Pharmacokinetics
Paliperidone palmitate is a benzisoxazole derivative which is hydrolyzed to the active moiety, paliperidone, and absorbed into the systemic circulation (see ). The palmitate ester of paliperidone is an aqueous suspension which utilizes nanoparticle technology. The resulting increased surface area leads to rapid release of medication and therefore a relatively short time to steady state. Following an injection, active paliperidone plasma levels have been detected from day 1, therefore coadministration with oral paliperidone on initiation of therapy is not required. Following the intramuscular administration of single doses in the deltoid muscle, on average a 28% higher peak concentration is observed compared with injection in the gluteal muscle. However, after four injections, there is no difference between the time to maximum plasma concentration and area under the curve between the two injection sites.Citation11,Citation12 Thus, the two initial deltoid muscle injections on days 1 and 8 (see ) help to attain therapeutic drug concentrations rapidly.Citation13
Figure 1 Formation of paliperidone from paliperidone palmitate.
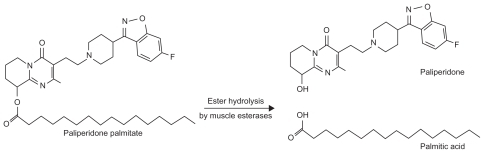
Table 1 Paliperidone palmitate injection dose and administration informationCitation13
Paliperidone is largely excreted unchanged in the urine. Four metabolic pathways have been identified for the metabolism of paliperidone including dealkylation, hydroxylation, dehydrogenation, and benzisoxazole scission, although none accounted for more than 10% of the oral dose administered.Citation13 While cytochrome P450 (CYP) 2D6 and CYP3A4 have been implicated in the metabolism of paliperidone in in vitro studies, these isoenzymes play a limited role in the metabolism of paliperidone in vivo. The nanocrystal molecules which make up the paliperidone palmitate suspension also allow it to undergo slow dissolution, yielding a half-life of 25–49 days (see ).Citation13–Citation16 The relatively long half-life allows for the monthly administration of paliperidone intramuscular injections.
Table 2 Pharmacokinetic properties of paliperidone palmitateCitation13–Citation16
Efficacy in schizophrenia
Efficacy in clinical trials
The therapeutic efficacy of paliperidone palmitate once-monthly injection has been evaluated in four short-term (nine- and 13-week) multicenter, randomized, double-blind, placebo-controlled trials in acute schizophrenia.Citation14,Citation17–Citation19 In all four trials, the injection was administered on days 1, 8, and 36 and, in the 13-week trials, also on day 64. Paliperidone palmitate’s efficacy as maintenance therapy in schizophrenia has also been evaluated in a 52-week recurrence prevention studyCitation20 and a further 52-week, open-label extension phase of this study.Citation21 In addition, two studies compared its clinical efficacy with intramuscular long-acting risperidone injection.Citation22,Citation23 Many of these studies are currently only available as poster presentations. The main efficacy findings from the trials are summarized below (and also in ).
Table 3 Summary of efficacy studies for paliperidone palmitate
Acute efficacy
The primary efficacy endpoint in all studies was the mean change in Positive and Negative Syndrome Scale (PANSS) total scoreCitation24 from baseline to endpoint. Secondary endpoints included changes in Clinical Global Impression of Severity (CGI-S),Citation25 PANSS factor and subscale scores, and Personal and Social Performance Scale (PSP).Citation26
In the largest dose-response study, intramuscular paliperidone was effective in the treatment of adult patients with acute schizophrenia, producing significant (P ≤ 0.034) and dose-related changes in PANSS total score from baseline for each of the three paliperidone groups (39, 156, and 234 mg) compared with placebo.Citation18 A significant change in PANSS total score was observed as early as day 8 for paliperidone 39 and 234 mg and from day 22 for paliperidone 156 mg, and was maintained until the endpoint. Significantly more patients on paliperidone responded to treatment (39 mg 33.5%, P = 0.007; 156 mg 41.0%, P < 0.001; 234 mg 40.0%, P < 0.001) compared with placebo (20.0%).Citation18
These findings are supported by two smaller, published, dose-response studies.Citation14,Citation17 In the first study, both doses of paliperidone (78 mg and 156 mg) produced significant (P ≤ 0.001) mean changes from baseline in PANSS total score (−5.2 [21.5)] and −7.8 [19.4], respectively) compared with placebo (6.2 [18.3]).Citation14 In the second study, significant changes in PANSS total score compared with placebo were noted with the 156 mg dose (P = 0.019) but not with the 78 mg dose (P = 0.19).Citation17 No statistical comparison was performed for the 234 mg treatment group, therefore a dose-response relationship could not be ascertained from this study.
Long-term efficacy
There has also been a long-term maintenance study of recurrence prevention using paliperidone palmitate, which consisted of five phases, including a seven-day screening, washout, and tolerability period, a nine-week, open-label transition phase during which intramuscular paliperidone was initiated, a 24-week, open-label, maintenance phase with flexible dosing until week 21, a randomized, double-blind, placebo-controlled phase of variable duration,Citation20 and an optional 52-week, open-label extension phase.Citation21 A recurrence event was defined as time to the first emergence of one or more of the following: hospitalization (for symptoms of schizophrenia), prespecified changes in PANSS scores or clinically significant deliberate self-injury or aggressive behavior. The primary outcome measure was time from randomization to the first recurrent event. A preplanned interim analysis was carried out in order to minimize the number of patients exposed to placebo. In the interim analysis (planned after 68 relapse events) paliperidone palmitate was superior to placebo, with recurrence of events seen in 15 (10%) patients in the paliperidone group compared with 53 (34%) patients in the placebo group,Citation20 yielding a numbers needed to treat of five (95% confidence interval [CI] 4–7).Citation27
In the open-label extension phase of this study, improvements from baseline to the endpoint were observed on PANSS, PSP, and CGI-S assessment.Citation21 Overall improvements in PANSS total scores observed during the previous study phases were maintained during the open-label phase for patients treated with paliperidone (mean ± SD of the change in PANSS total score −4.3 ± 15.43). The greatest improvement in PANSS total score occurred in patients who were treated with placebo in the double-blind phase (−8.4 ± 19.43). Functional improvement as measured by the PSP scale, also continued during the open-label phase, with the greatest improvement observed in patients previously on placebo in the double-blind phase (change in PSP score 6.0 ± 13.20). The authors reported that the majority of patients stayed in this open-label phase for one year, and demonstrated maintenance of symptoms as well as functional improvements.
Efficacy compared with active comparator
Paliperidone palmitate injection was compared with risperidone long-acting injection (RLAI) in a 53-week noninferiority study.Citation22 Patients were randomized (1:1) to receive double-blind flexible doses of paliperidone 39–156 mg every four weeks by gluteal injection (after two initiation doses of 78 mg on days 1 and 8) or RLAI 25, 37.5, or 50 mg every two weeks. Oral supplementation with risperidone was provided to the RLAI patients (as well as a placebo injection on day 1), and matched paliperidone patients received oral placebo and two-weekly placebo injections to coincide with RLAI frequency.
Although both agents resulted in decreases in PANSS total score (−12 ± 21.2 for paliperidone and −14 ± 19.8 for RLAI), paliperidone was not shown to be noninferior to RLAI, based on the predetermined margin of 5 points. Least-squares means change in PANSS total score was 2.6 points lower (95% CI −5.84, 0.61) for RLAI compared with paliperidone. As such, the predetermined margin for noninferiority (lower limit of the 95% CI should be greater than −5 points) was not met (by 0.84 points). However, the authors concluded that noninferiority was not established because patients had been initiated with suboptimal initial dosing of paliperidone, substantially lower than the initiation doses currently recommended in the product labeling. Therefore, this may have resulted in lower plasma concentrations until day 260 compared with those in the RLAI group. In addition, the authors believed that utilization of the gluteal initiation site may have also led to lower plasma levels of paliperidone, because this site of administration is associated with lower initial exposure.
Consequently, another noninferiority study between paliperidone palmitate and RLAI was performed, acknowledging the optimized initiation dosing regimen for paliperidone.Citation23 This was a randomized (1:1), double-blind, double-dummy, active- controlled, parallel-group, 13-week comparative Phase III study. Paliperidone deltoid injections of 234 mg on day 1 and 156 mg on day 8 were given, followed by once-monthly flexible dosing (78–234 mg) as either deltoid or gluteal injections (and placebo injections matched to RLAI). The other group received RLAI starting at 25 mg on day 8, followed by biweekly injections which could be increased up to 37.5 mg on day 36 and up to 50 mg on day 64 (and placebo injections matched to the paliperidone initiation regimen). Patients on RLAI received oral risperidone supplementation (1–6 mg from days 1–28), while the paliperidone group received a matching oral placebo.
The primary endpoint was the change in PANSS total score from baseline to the double-blind endpoint. Noninferiority of paliperidone compared with RLAI was to be concluded if the lower limit of the two-sided 95% CI exceeded −5. Additional secondary endpoints included PANSS subscales, CGI-S, and PSP. Unlike the previous study, the lower limit of the 95% CI of the treatment difference for the change in PANSS total score did exceed the prespecified protocol noninferiority margin of −5, and therefore paliperidone was shown to be noninferior to RLAI (point estimate [95% CI] 0.4 [−1.62; 2.38]). In addition, both groups showed similar improvements in CGI-S and PSP, as well as other secondary measures.Citation23 Limitations of this study include its relatively short duration, lasting only 13 weeks compared with 53 weeks in the previous one, and therefore the longer-term efficacy of paliperidone palmitate cannot be compared with RLAI from these findings. Furthermore, doses above 25 mg were not allowed in the RLAI group for several weeks, despite evidence to show that RLAI 25 mg may be ineffective in the majority of patients.Citation2 In fact, many patients in clinical practice nowadays are being initiated on 37.5 mg of RLAI, and the higher doses are generally used a lot sooner in the therapeutic regimen.
Safety and tolerability
The safety and tolerability of paliperidone palmitate were also assessed in the studies already described. The main findings are summarized in this section (and in ). Treatment emergent adverse effects (TEAEs) occurring more frequently in the paliperidone palmitate groups than in the placebo group included insomnia, headache, dizziness, sedation, vomiting, schizophrenia, injection site pain, extremity pain, myalgia, and extrapyramidal symptoms.Citation14,Citation17
Table 4 Summary of safety studies for paliperidone palmitate
Safety in acute therapy
In the nine-week study, parkinsonian-type adverse effects, including drooling and hypertonia, were the most common extrapyramidal side effects, and occurred more frequently in the paliperidone groups than placebo.Citation14 Other extrapyramidal side effects occurred similarly in all groups and were not considered severe in intensity. Median prolactin levels remained elevated for the paliperidone treatment groups compared with median predose treatment values, whereas prolactin levels decreased to pretreatment values in the placebo patients (see ). The percentage of patients with a > 7% increase in weight was reported to be 6–8% of patients in the paliperidone groups versus 4% for placebo-treated patients. Although the authors considered this weight increase to be low, it was still up to twice that seen in the placebo patients, therefore may be of clinical significance and a potential cause of metabolic complications. In addition, significant mean increases in body weight and body mass index from baseline to endpoint were observed for the 156 mg dose (P ≤ 0.001 for both measures) and increases for the 78 mg dose compared with placebo were P = 0.036 for body mass index and P = 0.059 for weight (see ). The incidence of increased heart rate was higher for paliperidone-treated patients (17%) than for placebo (8%), as was the incidence of orthostatic hypotension (9% versus 4%, respectively), although none of the latter were reported as adverse effects or symptomatic, and the incidence of tachycardia was low (<2%). In addition, although the study was not powered to assess safety, cardiac tolerability appeared to be good, with no patients on paliperidone experiencing QTc prolongation or a QTc > 450 msec during the study.Citation14
In the small 13-week trial, the frequency of glucose-related adverse effects was the same (2%) in the placebo and paliperidone groups.Citation17 As in the previous study, clinically relevant weight increases (>7% from baseline to endpoint) were more common among patients in the paliperidone groups (78 mg 12%, 156 mg 10%, 234 mg 4%) compared with placebo (2%), although the percentage of people with clinically relevant weight increases did not rise with increasing dose. In addition, mean increases in weight from baseline to endpoint were modest, and ranged from 0.9 to 1.5 kg but did not appear to be dose-related (see ). However, mean increases in prolactin levels from baseline to endpoint were seen in all paliperidone groups, and increases were larger for the 156 mg and 234 mg groups than for the 78 mg group in both women and men, suggesting a dose-related relationship. There were no clinically relevant changes in vital signs, electrocardiogram (ECG) recordings, or other clinical laboratory parameters, and local injection site tolerability was reported to be good.
In the largest dose-response study, the incidence of TEAEs leading to study discontinuation was similar across treatment groups (placebo 6.7%, paliperidone 6.1%–8%).Citation18 However, the incidence of serious TEAEs was higher in the placebo group (14%) than in the paliperidone groups (39 mg 9.4%, 156 mg 13.3%, 234 mg 8%). The most commonly reported serious TEAEs for paliperidone were worsening or exacerbation of schizophrenia (4.9%) and psychotic disorder (2.9%), although these figures were lower than those reported for placebo (6.1% and 4.3%, respectively). Unlike the previous study, a weight increase of 7% or higher was found to occur more frequently with the higher doses of paliperidone (see ). There were no clinically relevant changes from baseline in vital signs, ECG recordings, or other laboratory parameters (including fasting glucose levels and serum lipids) in the paliperidone groups. In addition, injection site tolerability was said to be good, with investigators rating injection site pain similar to that with placebo.
Safety in long-term therapy
Findings from the long-term relapse prevention study showed that weight increase occurred more frequently in patients treated with paliperidone palmitate (7%) than placebo (1%), as did the blood glucose increase in the paliperidone group (3%) versus placebo (1%).Citation20 Mean weight, from transition baseline to the double-blind endpoint, increased by 1.9 kg for paliperidone-treated patients, but remained unchanged for placebo patients. Abnormal weight increases (≥7%) also occurred in twice as many paliperidone patients as placebo patients from both transition and double-blind baselines (see ). There were no clinically relevant changes from transition baseline to the double-blind end-point in extrapyramidal symptom rating scales and no reports of orthostatic hypotension or ECG changes during the double-blind phase (although ECG changes were seen in the transition and maintenance open-label paliperidone phases). In accordance with other studies, prolactin levels increased for the paliperidone group, again more in women than in men, while levels decreased in the placebo group (see ). No other laboratory parameter changes were noted, and injection site tolerability was similar in all groups.Citation20
Other safety data
The safety and tolerability of initiating treatment with paliperidone palmitate via either deltoid or gluteal injections were investigated in a study comparing the two administration routes.Citation28 This crossover trial included 252 stable outpatients randomly assigned 1:1:1 to three dose groups of paliperidone (see ) and two treatment sequences including deltoid muscle injection (13 weeks), followed by gluteal muscle injection (12 weeks), or the reverse. The proportion of patients with injection-site pain appeared to be higher after deltoid administration compared with gluteal administration (41% deltoid, 26% gluteus), based on the 90% CI of investigator evaluations of the presence of local symptoms at the injection site. The overall incidence of TEAEs did not differ significantly between deltoid injections (period 1 = 64%, period 2 = 51%) and gluteal injections (period 1 = 63%, period 2 = 46%), and there was no dose-dependent increase in the incidence of TEAEs. Evaluation of pain by patients revealed slightly more intense pain following deltoid injections compared with gluteal injections for the 78 mg and 117 mg doses of paliperidone, but no difference was detected for the 156 mg dose. There were no clinically significant changes in extrapyramidal symptom rating scales regardless of the injection site or the dose.Citation28
Safety compared with active comparator
In the two noninferiority studies of paliperidone palmitate and RLAI, the overall rates of TEAEs were found to be similar between the two groups. In the first study, rates of TEAEs were 76% in the paliperidone group and 79% in the RLAI group,Citation22 whereas in the second study, rates of TEAEs were 57.9% in the paliperidone group and 52.8% in the RLAI group.Citation23 Therefore, neither drug can be associated with a higher incidence of adverse effects based on these results. In both studies, the incidence of extrapyramidal symptoms was similar in both groups, with the exception of hyperkinesias which was less common in the paliperidone group than in the RLAI group in the first study (6% versus 10%, respectively).Citation22 With regard to weight changes, weight actually decreased in the paliperidone palmitate group in the first study compared with RLAI (which caused a slight weight increase), whereas in the second study, mean body weight increases were similar at the endpoint between the two treatment groups (see ). In addition, in the second study, there were no clinically relevant changes in vital signs or ECG, and the incidence of glucose-related TEAEs, as well as investigator assessments of the injection site, were similar in both treatment groups.Citation23 Overall, it appears that both paliperidone palmitate and RLAI have comparable adverse effect profiles. However, the second study only lasted 13 weeks, and so long-term comparisons cannot be made. In addition, both studies are currently only available in poster format, thus not allowing for a thorough evaluation of the data.
Summary of safety data
In summary, paliperidone is relatively well tolerated but, like many other antipsychotics, and as expected from its pharmacological profile, it can cause weight gain and an increase in prolactin levels. Whether weight gain is dose-related or not is still debatable based on the current evidence. However, the rise in prolactin has been shown to be greater with higher doses. In all studies, there were no clinically relevant changes in vital signs, ECG recordings, or other clinical laboratory parameters, and local injection site tolerability was reported to be good. The majority of currently available trials are short-term, therefore additional longer trials are required in order to assess paliperidone palmitate’s long-term safety profile, in particular with regard to changes in metabolic parameters because these may not be picked up in short-term studies. Paliperidone injection and RLAI were found to have comparable adverse effect profiles. compares the adverse effects of paliperidone with other antipsychotic agents.
Table 5 Adverse effects of paliperidone compared to other antipsychotics
Discussion
Paliperidone palmitate has been shown to be effective in reducing PANSS total scores in both acute and maintenance treatment of schizophrenia. Improvements in PANSS total scores observed in the majority of studies were greater with higher doses of paliperidone, suggesting a dose-response relationship. Paliperidone injection is generally well tolerated but can cause weight gain and dose-related raised prolactin levels. In two noninferiority studies comparing paliperidone with RLAI, paliperidone injection only proved to be noninferior to RLAI in one study. Paliperidone and RLAI were shown to have comparable adverse effects. Additional long-term trials comparing paliperidone palmitate’s efficacy and safety with active comparators are required. The fact that some of the current data for paliperidone injection are only available as poster presentations is an important limitation for its evaluation.
Conclusion
Given the importance of treatment adherence in schizophrenia, and taking into consideration the compliance problems that often accompany the illness, long-acting antipsychotic injections are a valuable form of therapy. Paliperidone palmitate once-monthly injections may be a useful alternative in a currently limited market. The recommended dosage regimen is 234 mg on day 1 followed by 156 mg a week later, both administered in the deltoid muscle. The recommended maintenance dose is 117 mg monthly, which may be adjusted, based on efficacy and tolerability, within a 39–234 mg range, administered in either the deltoid or gluteal muscle. Paliperidone palmitate has some advantages over available agents, including a faster onset of action than RLAI and the absence of a requirement for oral supplementation at the start of therapy. Therefore, it may be a suitable option in patients who refuse oral treatment. In addition, it is available in a wider variety of strengths than RLAI, allowing for a more specialized and patient-specific dose titration regimen. Since paliperidone can be given either in the deltoid or gluteal muscle after initiation has been established, this improves flexibility of administration. It also has the added advantage of not requiring refrigeration for safe storage. Furthermore, unlike with olanzapine pamoate, “post-injection syndrome” was not reported during the clinical trials with paliperidone, which makes it a suitable agent when a postinjection observation period is not practical.
Disclosure
The author reports no conflict of interest in this work.
References
- NasrallahHAThe case for long-acting antipsychotic agents in the post-CATIE eraActa Psychiatr Scand2007115426026717355516
- TaylorDMYoungCPatelMXProspective 6-month follow-up of patients prescribed risperidone long-acting injection: Factors predicting favourable outcomeInt J Neuropsychopharmacol20069668569416939663
- Eli Lilly and Company LimitedSummary of Product CharacteristicsZypadhera 210 mg, 300 mg, and 405 mg, powder and solvent for prolonged release suspension for injection2009 Available at: http://emc.medicines.org.uk/Accessed on Jul 14, 2010
- BisharaDTaylorDUpcoming agents for the treatment of schizophrenia. Mechanism of action, efficacy and tolerabilityDrugs200868162269229618973393
- NasrallahHAAtypical antipsychotic-induced metabolic side effects: Insights from receptor-binding profilesMol Psychiatry2008131273517848919
- HaddadPMAntipsychotics and diabetes: Review of non-prospective dataBr J Psychiatry Suppl200447S80S8615056599
- TaylorDMMcAskillRAtypical antipsychotics and weight gain – a systematic reviewActa Psychiatr Scand2000101641643210868465
- LeysenJEJanssenPMMegensAASchotteARisperidone: A novel antipsychotic with balanced serotonin-dopamine antagonism, receptor occupancy profile, and pharmacologic activityJ Clin Psychiatry199455Suppl5127520908
- SchotteAJanssenPFGommerenWRisperidone compared with new and reference antipsychotic drugs: In vitro and in vivo receptor bindingPsychopharmacology (Berl)19961241257738935796
- van BeijsterveldtLEGeertsRJLeysenJERegional brain distribution of risperidone and its active metabolite 9-hydroxyrisperidone in the ratPsychopharmacology (Berl)1994114153627531352
- CletonARossenuSCrauwelsHAssessment of the dose proportionality of paliperidone palmitate 25, 50, 100 and 150 mg EG. A new long-acting injectable antipsychotic, following administration in the deltoid or gluteal musclesPoster presented at American Society for Clinical Pharmacology and TherapeuticsOrlando, FL2008 Apr 2–5
- CletonARossenuSHoughDEvaluation of the pharmacokinetic profile of deltoid versus gluteal intramuscular injections of paliperidone palmitate in patients with schizophreniaPoster presented at the American Society for Pharmacology and TherapeuticsOrlando, FL2008 Apr 2–5
- JanssenOnce-monthly Invega Sustenna: Paliperidone palmitate extended-release injectable suspension2009 Available at: http://www.invegasustenna.com/invegasustenna/assets/hcp/01PM09110.pdfAccessed on Jul 14, 2010
- KramerMLitmanRHoughDPaliperidone palmitate, a potential long-acting treatment for patients with schizophrenia. Results of a randomized, double-blind, placebo-controlled efficacy and safety studyInt J Neuropsychopharmacol201013563564719941696
- SamtaniMNVermeulenAStuyckensKPopulation pharmacokinetics of intramuscular paliperidone palmitate in patients with schizophrenia: A novel once-monthly, long-acting formulation of an atypical antipsychoticClin Pharmacokinet200948958560019725593
- SedkyKNazirRLindenmayerJPLippmanSPaliperidone palmitate: Once monthly treatment option for schizophreniaCurrent Psychiatry Online2010934850
- GopalSHoughDWXuHEfficacy and safety of paliperidone palmitate in adult patients with acutely symptomatic schizophrenia: A randomized, double-blind, placebo-controlled, dose-response studyInt Clin Psychopharmacol2010410 [Epub ahead of print]
- PandinaGJLindenmayerJPLullJA randomized, placebocontrolled study to assess the efficacy and safety of 3 doses of paliperidone palmitate in adults with acutely exacerbated schizophreniaJ Clin Psychopharmacol201030323524420473057
- NasrallahHAGopalSGassmann-MayerCEfficacy and safety of three doses of paliperidone palmitate, an investigational longacting injectable antipsychotic in schizophreniaPoster presented at the Institute on Psychiatric Services Annual MeetingChicago, IL2008 Oct 2–5
- HoughDGopalSVijapurkarULimPMorozovaMEerdekensMPaliperidone palmitate maintenance treatment in delaying the time-to-relapse in patients with schizophrenia: A randomized, double-blind, placebo-controlled studySchizophr Res201011623107117
- GopalSVijapurkarULimPMorozovaMEerdekensHoughDA 52-week open-label study of the safety and tolerability of paliperidone palmitate in patients with schizophreniaJ Psychopharmacol Online-First78201010.1177/0269881110372817
- FleischhackerWWGopalSSamtaniMOptimization of the dosing strategy for the long-acting injectable antipsychotic paliperidone palmitate: Results of two randomized double-blind studies and population pharmacokinetic simulationsPoster presented at the American Society for Pharmacology and TherapeuticsScottsdale, AZ2008 Dec 7–11
- PandinaGLaneRGopalSA randomized, double-blind, comparative study of flexible doses of paliperidone palmitate and risperidone long-acting therapy in patients with schizophreniaPoster presented at the 48th American College of NeuropsychopharmacologyHollywood, FL2009 Dec 6–10
- KaySRFiszbeinAOplerLAThe positive and negative syndrome scale (PANSS) for schizophreniaSchizophr Bull19871322612763616518
- HaroJMKamathSAOchoaSThe Clinical Global Impression-Schizophrenia scale: A simple instrument to measure the diversity of symptoms present in schizophreniaActa Psychiatr Scand Suppl2003416162312755850
- PatrickDLAdriaenseenIMorosiniPLGagnonDRothmanMReliability, validity and sensitivity to change of the Personal and Social Performance scale in patients with acute schizophreniaPoster presented at Collegium Internationale NeuropsychopharmacologicumChicago, IL2006 Jul 9–13
- CitromeLPaliperidone palmitate – review of the efficacy, safety and cost of a new second-generation depot antipsychotic medicationInt J Clin Pract201064221623919886879
- HoughDLindenmayerJPGopalSSafety and tolerability of deltoid and gluteal injections of paliperidone palmitate in schizophreniaProg Neuropsychopharmacol Biol Psychiatry20093361022103119481579
- CoppolaDLiuYGopalSLong-term safety, tolerability and pharmacokinetics of paliperidone palmitate 234mg (150 mg eq.), the highest marketed dose: A one-year open-label study in patients with schizophreniaPoster presented at the American Society for Pharmacology and TherapeuticsAtlanta, GA2010 Mar 17–30
- TaylorDPatonCKapurSThe Maudsley Prescribing Guidelines10th EditionLondonInforma Healthcare2009