Abstract
Myasthenia gravis (MG) is an autoimmmune disease in which autoantibodies to different antigens of the neuromuscular junction cause the typical weakness and fatigability. Treatment includes anticholinesterase drugs, immunosuppression, immunomodulation, and thymectomy. The autoimmune response is maintained under control by corticosteroids frequently associated with immunosuppressive drugs, with improvement in the majority of patients. In case of acute exacerbations with bulbar symptoms or repeated relapses, modulation of autoantibody activity by plasmapheresis or intravenous immunoglobulins provides rapid improvement. Recently, techniques removing only circulating immunoglobulins have been developed for the chronic management of treatment-resistant patients. The rationale for thymectomy relies on the central role of the thymus. Despite the lack of controlled studies, thymectomy is recommended as an option to improve the clinical outcome or promote complete remission. New videothoracoscopic techniques have been developed to offer the maximal surgical approach with the minimal invasiveness and hence patient tolerability. The use of biological drugs such as anti-CD20 antibodies is still limited but promising. Studies performed in the animal model of MG demonstrated that several more selective or antigen-specific approaches, ranging from mucosal tolerization to inhibition of complement activity or cellular therapy, might be feasible. Investigation of the transfer of these therapeutic approaches to the human disease will be the challenge for the future.
Background
Myasthenia gravis (MG) is an autoimmune disorder characterized by fluctuating muscle weakness and fatigability on exertion, in which autoantibodies to proteins of the neuromuscular junction (NMJ) are pathogenically relevant.Citation1 To date 2 major types of antibodies are routinely detectable, ie, antibodies against the acetylcholine receptor (AChR) and to a muscle specific kinase (MuSK). Anti-AChR and anti-MuSK antibodies significantly interfere with neuromuscular transmission, and their removal produces clinical improvement; moreover, their pathogenic role has been confirmed in experimental models of MG.Citation2,Citation3 Anti-AChR autoantibodies are detected in about 80% to 85% of patients with generalized MG.Citation1 According to series from different countries variable proportions of patients without anti-AChR antibodies have antibodies to MuSK.Citation4 MG patients without antibodies to either AChR or MuSK are now defined as affected with “seronegative MG”. A recent study reported that 66% of seronegative myasthenic patients have low-affinity antibodies to AChR that cannot be detected by common assays.Citation5
The NMJ, the synapse connecting nerve and muscle, works through the release of acetylcholine (ACh) and its engagement with the receptor on the muscle endplate. In MG the neuromuscular transmission is impaired because of a reduced number of functional AChRs. At least 3 antibody-mediated mechanisms have been proposed to explain AChR impairment: accelerated endocytosis and degradation of AChR; functional blockade of ACh-binding sites; and complement-mediated damage of the postsynaptic membrane. B cells are directly involved in AChR-antibody production and AChR-specific T cells are considered relevant for pathogenesis of MG. The pathogenicity of anti-MuSK antibodies has been a matter of debate; however, MuSK is necessary for the agrin-mediated clustering of AChR on the surface of postsynaptic muscle during development. More recently it has been shown that passive transfer of IgG from anti-MuSK-positive patients can cause myasthenia when injected into mice; moreover, both reduction of AChR density and loss of the normal apposition between pre- and postsynaptic structures were reported.Citation6–Citation8
Thymic abnormalities are frequently present and specifically associated with MG; AChR antibody-positive MG patients show pathological abnormalities (either non-neoplastic or neoplastic) of the thymus in nearly 75% of cases.Citation9 MG is associated with pathological abnormalities of the thymus gland in about 80% to 85% of cases and thymomas have been reported with variable frequencies, in up to 30% of MG patients.
The thymus is suspected to be the main site of autosensitization to AChR, since thymic epithelial cells and muscle-like (myoid) cells express AChR on their surface. AChR-specific T cell lines can be cloned from the thymus, cultured thymic lymphocytes produce AChR-specific autoantibodies, and numerous germinal centers are present within the thymic medulla. However, what triggers autosensitization remains a mystery. Viral involvement has been suspected for a long time but without a definite conclusion. In this regard, we have already shown that Toll-like receptor 4 (an activator of the innate immune response) is overexpressed in the thymus of some MG patients.Citation10 More recently, we demonstrated Epstein-Barr virus persistence and reactivation in MG thymus, suggesting again that a dysregulated infection may contribute to the initiation or perpetuation of the autoimmune response underlying the disease.Citation11
Thymoma, usually a benign epithelial tumor, is found in about 10% to 20% of MG patients, depending on the series reported. Thymoma-associated MG is considered a more severe disease compared with nonthymomatous MG and its outcome relies mainly on prolonged immunosuppressive treatment.Citation12,Citation13
MG is a relatively rare disease whose incidence and prevalence rates have increased over the past 4 to 5 decades.Citation14 The annual MG incidence is reported to be about 2 to 21 per million per year and the prevalence about 200 per million.Citation15,Citation16 The incidence is age- and sex-related: a peak in the second and third decades is observed among women, and in the sixth and seventh decades among men. MG may be under-diagnosed in the elderly.Citation17–Citation19
MG is a chronic disorder, can be extremely severe, but is a treatable disease. Elucidation of the pathogenetic mechanisms of MG has provided a rationale for optimization of treatments (). The therapeutic approach involves 3 different lines: 1) drugs improving neuromuscular transmission, ie, symptomatic therapies; 2) immunomodulating drugs interfering with autoantibody activity on NMJ, ie, corticosteroids, immunosuppressants and therapies modulating circulating autoantibodies (apheresis or intravenous immunoglobulins); and 3) modification of the natural history of the disease, eg, thymectomy.
Figure 1 The immunopathological steps of myasthenia gravis (MG) are summarized as well as the specific targets of therapeutic intervention. In red are outlined the innovative therapeutic approaches.
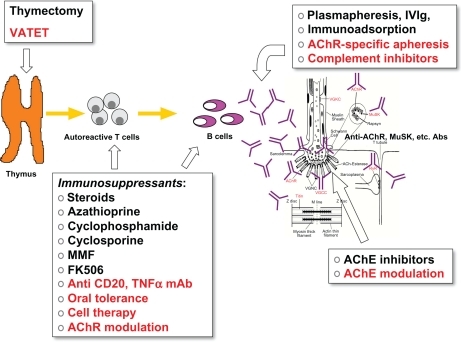
In this review we will summarize and describe each of these lines of treatment, providing what is the state of the art of current treatments and new emerging approaches.
Treatment of myasthenia gravis
Effectiveness of treatment in MG must rely on definite outcomes as was clearly defined by the Myasthenia Gravis Association of America Task Force in 2000. The ultimate goal is to achieve complete stable remission, defined as no myasthenic symptoms or signs without any ongoing treatment for at least 1 year.Citation20,Citation21 Therapies in MG should therefore eliminate patients’ symptoms within the boundaries of adverse events associated with treatment itself.Citation22
Several subtypes of MG have been recognized on the basis of age at onset, weakness distribution, thymus histology, and presence of autoantibodies.Citation16 These subgroups have a different prognosis and need distinct therapeutic strategies. Although treatment options in MG are considered effective and underpinned by scientific evidence (see ), controlled clinical trials are rare leading to limited evidence-based information.Citation23 Current guidelines are based largely on clinical experience, consensus between experts, and retrospective analysis. At present adequate MG treatment usually permits a substantially full, productive life.
Drugs improving neuromuscular transmission
In 1934, physostigmine, an acetylcholinesterase (AChE) inhibitor, was used for the first time for the treatment of a myasthenic patient; it was then substituted by pyridostigmine bromide (PB) in 1954. Oral AChE inhibitors are the first-line treatment for MG. They are symptomatic drugs improving neuromuscular transmission by prolonging the availability of ACh at NMJ and do not interfere with the immune processes that cause and perpetuate MG. AChE inhibitors have a short-term benefit due to their short half-life. European guidelines indicate that AChE inhibitors should be considered as first-line treatment for MG, particularly for mild cases.Citation23 They may also be used as adjunctive treatment in patients with more severe disease also receiving other treatment modalities. PB is the most commonly used AChE inhibitor; its effect begins within 30 minutes, peaks at about 2 hours and lasts for 3 to 4 hours; however, patients may display different individual responses, hence the physician may have to adjust for the optimal dose and the right interval in each patient.
PB is available as:
○ An oral standard tablet, dose 60 mg; this is the most commonly used preparation.
○ A sustained-release preparation (180 mg);Citation24 usually prescribed at bedtime for patients symptomatic during the night or in the early morning. A switch from instant to sustained-release PB as been proposed but still not fully investigated.Citation24
○ A syrup (12 mg/mL) for pediatric use, in patients requiring nasogastric feeding or, very rarely, in those patients with allergic reactions to drug excipients.
○ PB is also available for intramuscular or intravenous administration in the form of 2-mL ampules, containing 5 mg/ml of the drug. About 1/30 of the oral dose of PB may be given parenterally for an equivalent effect. Parenteral administration is useful when patients cannot take therapies orally. Few patients have experienced significant, sometimes fatal, cardiac arrhythmias;Citation25,Citation26 hence intramuscular administration should be preferred.
The dosage schedule must be adjusted according to the clinical status of the patient. The initial oral dose in adults consists of 30 to 60 mg every 4 to 6 hours. Patients requiring more than recommended doses for adequate relief of symptoms are candidates for other modalities of treatment.
Neonatal MG occurs in about 10% of babies born from MG mothers due to placental transfer of maternal AChR-antibodies.Citation27 AChE inhibitors may be used temporarily until MG resolves spontaneously after a few weeks.
Other AChE inhibitors:
○ Neostigmine is an analog of PB and can be administered orally, while neostigmine methylsulfate is given intramuscularly or intravenously. Compared with PB, neostigmine has a shorter action, is less effective and more frequently cause muscarinic side effects.Citation28,Citation29
○ Ambenonium chloride is rarely used because of its long duration of action and greater tendency to accumulate.
○ Edrophonium is a very short-acting AChE inhibitor and is used mainly for diagnostic testing.
AChE inhibitors are generally well tolerated; common adverse effects are mainly due to cholinergic stimulation of muscarinic AChR on smooth muscle and autonomic glands. They occur in about one-third of the patients.Citation30,Citation31 The most frequent are gastrointestinal disorders, such as gut hypermotility, which may lead to abdominal pain and diarrhea; other side effects are increased sweating and bronchial secretion (sometimes patients experience symptoms mimicking bronchial asthma); bradycardia and hypotension are seen more frequently in elderly patients. Side effects can be controlled by oral or parenteral administration of atropine (0.5 to 1 mg in adults and 0.01 mg/kg in children). Patients carrying a polymorphism in the promoter gene encoding the catalytic subunit of AChE show acutely exaggerated sensitivity to conventional doses of AChE inhibitors.Citation32 Nicotinic cholinergic side effects are less frequently observed and occur in patients receiving high doses of AChE inhibitors: muscle fasciculations, cramps, and blurred vision are the most common. Older patients (over 60 years) are more prone to develop cholinergic side effects, while duration of treatment does not correlate with side effects.Citation31 AChE inhibitors may be stopped in the course of a myasthenic crisis to reduce bronchial and salivary secretions;Citation33–Citation35 they will be reintroduced when the patient starts to improve and is ready to be extubated.
Randomized placebo-controlled trials on the efficacy of AChE inhibitors are not available, but case series and daily clinical experience have shown an objective and marked clinical effect.Citation23
AChE inhibitors are relatively ineffective in the treatment of ocular MG: patients shift to other treatments, in particular corticosteroids, which are very effective in ocular MG.Citation22
MG associated with MuSK-antibodies is often more severe than AChR-positive MG and its response to AChE inhibitors is usually insufficient: a high proportion of patients need immunosuppressive treatments.Citation36 AChE inhibitors are poorly tolerated: muscle cramps, fasciculations,Citation37,Citation38 and extra discharges with low-frequency motor nerve stimulation have been described, suggesting an abnormal sensitivity to ACh.Citation31,Citation38 AChE inhibitors are safe during pregnancy.Citation39,Citation40
Immunomodulating therapies interfering with autoantibody effects on NMJ
Conventional and emerging therapies able to interfere with the immunopathogenetic processes underlying MG comprise the following:
Steroids;
Immunosuppressants;
Immunomodulating agents;
Biological and cellular therapies.
Steroid and immunosuppressants are usually used on chronic therapeutic regimen, whereas immunomodulating agents are usually adopted as short-term therapies.
Steroids
Oral steroids are widely used in MG and are recommended as a first-choice drug when immunosuppression is required.Citation23 Notwithstanding their extensive usage, the potential for severe side effects is high and a significant impact on patients’ quality of life is foreseen.Citation9
A variety of steroids has been used in the treatment of MG: the most commonly used is prednisone because of its potent immunosuppressive activity, low anti-edemigen activity and half-life compatible with an alternate-day schedule.Citation41
Retrospective data indicate that prednisone provides a clinical benefit in about 80% of patients;Citation42,Citation43 its effectiveness was confirmed in a systematic Cochrane review.Citation44
The initial dose for the treatment of generalized MG is 1 mg/kg/day. Patients with moderate-to-severe generalized MG are usually hospitalized to initiate steroid therapy because of the risk of a drug-induced exacerbation of the disease; exacerbation may start within the first 2 weeks of steroid treatment and may be extremely severe. Steroid-induced clinical improvement usually begins within 2 to 4 weeks. Different modalities of steroid initiation have been proposed: patients’ condition permitting, the best approach is to start steroid treatment with the highest daily dosage, followed by the shift to an alternate-day regimen and later on, when pharmacological remission or minimal manifestations state are achieved, the search for the minimal effective dose should be pursued.Citation43 Ocular MG usually requires lower dosages, however resistant forms may require higher doses to be effective. A recent study suggested that immunotherapy of ocular MG reduces conversion to generalized MG; however, the reported series were retrospective and a selection bias cannot be excluded; prospective observational studies should be designed to address this important issue.Citation45,Citation46
Side effects of chronic corticosteroids are osteoporosis, cataract, diabetes mellitus, hypertension, gastrointestinal irritation, glaucoma, weight gain, and skin disorders.
Immunosuppressants
Several immunosuppressive drugs are used in the treatment of MG: usually the time to achieve a clinical benefit with these drugs is longer than that of steroids and can take several months. They can be used as single drugs, as an alternative therapy to steroids in those patients with contraindications to it, or frequently used in combination with corticosteroids as “steroid-sparing agents”.Citation9,Citation23 RCT demonstrating the efficacy of immunosuppressive drugs in MG is very limited: larger, longer and well-designed clinical trials are warranted.Citation47
Azathioprine (AZA)
Azathioprine is the most frequently used immunosuppressive drug for MG, because of its preferential effect on T cell replication, with evidence supporting a steroid-sparing effect.Citation20,Citation23,Citation48 The daily dose is 2–3 mg/kg/day. AZA efficacy has been confirmed in a randomized clinical trial (RCT).Citation48 It is generally well tolerated, but liver and bone marrow toxicity is not infrequent. The use of AZA may be optimized by a pharmacogenomic approach by testing TPMT gene polymorphisms.Citation49
Cyclosporin A (CyA)
Cyclosporin A inhibits the production of interleukin (IL)-2 by helper T cells. CyA efficacy was confirmed by a RCT for MG,Citation50 but its use was hampered by the onset of hypertension and nephrotoxicity. CyA is therefore considered a third-line therapy and should be used only in patients intolerant or unresponsive to other immunosuppressants; monitoring of kidney function, blood pressure and detection of CyA plasma levels is necessary. A frequent and intractable side effect is tremor which disappears after discontinuation of the drug. The recommended daily dosage is 5 mg/kg/day twice daily.
Cyclophosphamide
Cyclophosphamide acts mainly on B lymphocytes and was demonstrated to be effective in treatment-resistant MG cases;Citation47,Citation51 however, its use is limited by the risk of adverse side effects, including late development of malignancies or infertility, to patients intolerant or non-responsive to other treatment modalities.Citation23
Mycophenolate mofetil (MMF); tacrolimus (FK506)
These are newer immunosuppressive drugs that may have some benefit as second-line immunosuppressive therapyCitation23 although this was not supported by a recent systematic review.Citation47 Two recent randomized controlled studies did not demonstrate a clear efficacy of MMF in MG patients;Citation52,Citation53 it is likely that the limited duration of the study (9 months) did not allow a correct assessment of the efficacy of MMF in patients already taking pharmacological doses of prednisone. Although the MMF clinical trials were considered negative, they provided relevant clinical and pharmacological information with regard to the design and the methodological aspects of RCTs in MG, eg, it will be necessary to rethink how to set up studies comparing the efficacy of a new immunosuppressive drug in comparison to steroid.
Methotrexate
No studies are available on the use of methotrexate in MG. However, the drug can be considered in treatment-resistant patients when all other treatment options have been tried. Long-term toxicity should be always considered. A Phase II clinical trial is under way (see www.clinicaltrials.gov).
Short-term immunomodulation: plasma-exchange and intravenous immunoglobulins
Plasma-exchange (PE) and intravenous immunoglobulins (IVIg) are generally used to induce a rapid improvement in patients with exacerbation of the disease. Their beneficial effect is rapid, but only temporary, lasting for 4 to 5 weeks.
PE is usually performed by exchanging 1 plasma volume on alternate days. In our experience, a 2-course treatment is usually sufficient to induce clinical improvement,Citation54 although in some cases it may be necessary to repeat more courses according to the patients’ clinical conditions. Methodological flaws related to open studies on PE have been underlined in the Cochrane review on this topic.Citation55 Nevertheless, open studies showed that PE was effective in at least 60% to 70% of treated patients and that improvement was strictly related in time with plasma removal. The main indication to PE, as well as intravenous immunoglobulins, is the acute worsening of the disease (either severe generalized or bulbar) or myasthenic crisis. Other indications include worsening during the start of corticosteroids, and preparation to thymectomy in symptomatic patients. On the basis of our experience we think there is no need to perform PE immediately before thymectomy when MG is well controlled by pharmacological treatment. The chronic use of PE in MG has never been addressed with a definite protocol. Nevertheless, PE can be used at repeated intervals in selected patients in case of frequent relapses, when the response to pharmacological treatment is unsatisfactory after an adequate clinical follow-up, or in patients who have major contraindications to long-term corticosteroids. Limitations to the use of chronic PE are the need for good vascular accesses and the obvious effects on several plasma components in case of intensive protocols. Therefore, the number of sessions and interval between them must be tailored to each patient, taking into account the general clinical conditions, severity of MG, and potential side effects. Because of these limitations, immunoglobulin G (IgG) apheresis should be the technique of choice in severe immunosuppression-resistant patients requiring chronic treatments.
MuSK-positive MG shows a dramatic response to PE (or IVIg).Citation37 This feature is of particular importance in the effort to overcome the prolonged and severe bulbar involvement that frequently occurs in this subset of MG patients. The reason for this clinical behavior is still unclear but is likely related to the activity of anti-MuSK antibodies that do not bind complement, as occurs with anti-AChR antibodies, and therefore might cause a different kind of damage to the neuromuscular junction.
IVIgs are usually administered at a dose of 400 mg/kg body weight/day for 3 to 5 days.Citation56,Citation57 IVIgs have been compared with PE in RCTs,Citation55,Citation58 showing a significant clinical improvement within 2 weeks with no substantial difference between the two treatment options. A recently published trial found no significant superiority of 2 g/kg over 1 g/kg of IVIgs in the treatment of MG exacerbation.Citation56
Thus, PE and IVIg have a similar efficacy; PE is less expensive, but requires specific equipment and side effects are a little more common.Citation23,Citation58 Since good vascular access is mandatory for PE, IVIg represents a good alternative for children and older patients. As reported above for PE, IVIgs are suitable for chronic treatment of patients with unsatisfactory response to ongoing pharmacological treatments. Long-term protocols have not been investigated in detail.Citation59
Semiselective immunoadsorption
The ideal apheretic approach should remove only the specific autoantibody involved in the pathogenesis of the disease under treatment, leaving all the other plasma components unaltered, a specific approach not yet available for clinical practice. A compromise is represented by circulating IgG immunoadsorption (IA), a procedure able to remove IgG and hence specific autoantibodies. Two main ligands are available for clinical use in IgG-mediated disorders. Protein A is a component of the staphylococcal cell wall that binds human IgG with high affinity.Citation60 A second method involves the use of polyclonal sheep anti-human IgG that removes directly circulating IgG by means of an immunological interaction.Citation61 In both cases, plasma is separated by centrifugation and then passed on-line through a set of 2 filters filled with either protein A or sheep antihuman IgG, continuously regenerated throughout the procedure allowing removal of unlimited amounts of antibodies. No replacement fluid is needed and the interaction with coagulation factors is negligible. At least 2 plasma volumes are treated during each session to fully exploit the binding capacity of the filters. We favor the use of IA in patients with severe treatment-resistant MG after adequate clinical follow-up, patients who require frequent PE to keep a satisfactory improvement, or patients who have major contraindications to the use of high dose corticosteroids or other immunosuppressive drugs.
Thymectomy
Thymectomy is mandatory in patients with thymoma and is recommended as an option for nonthymomatous patients with generalized MG, in particular those with acetylcholine antibodies and younger than 60 years, to increase the likelihood of remission or improvement.Citation23,Citation62,Citation63 Several surgical techniques have been proposed but there is general agreement on the maximal approach, ie, extended trans-sternal thymectomy. In recent years, variations in videothoracoscopic techniques have been developed, with either unilateral (video assisted thoracoscopic surgery) or bilateral access to the mediastinum (video assisted thoracoscopic extended thymectomy). In our experience, the use of thoracoscopic thymectomy in nonthymomatous MG was comparable to that of the classical trans-sternal approach; complete stable remission was 50.6% at 6 years of follow-up. Compared with trans-sternal surgery, videothoracoscopic thymectomy is associated with less morbidity and negligible esthetic sequelae.Citation64
The advantage of thymectomy is the chance of long-term benefit reducing or, in some cases, stopping the ongoing chronic medical therapies. However controlled studies demonstrating the benefit of thymectomy are not available. An international, prospective, single-blinded randomized trial of thymectomy in nonthymomatous MG patients is currently ongoing. The role of thymectomy in patients with purely ocular disease is unclear.Citation65,Citation66
New treatment options
Innovation in MG treatment relies mainly on the following aspects: a) the need for new effective therapies that will combine adequate efficacy, reduction of side effects, and use of therapeutic schedules optimized for chronic immunosuppression; b) use of drugs with higher specificities targeting selectively the critical immunopathological steps from AChR sensitization to autoantibody production. Most of this search has been achieved through the use of the animal model of MG (EAMG) and the big issue is the translation from the relatively homogeneous condition of the experimental model to the very heterogeneous condition typical of human MG.
lists new treatment options, showing their use in EAMG and human disease.
Table 1 Biological drugs and experimental treatments tested in animal model of myasthenia gravis (EAMG) or human myasthenia gravis (MG)
Rituximab
Rituximab is a humanized monoclonal antibody to CD20 that causes prolonged B-cell depletion approved for treatment of B-cell lymphoma in adults, and has been used in refractory MG. Small series of patients are available, and both MG with and without thymoma have been treated. Rituximab provides promising expectations for the treatment of MG,Citation67–Citation70 although no RCTs have been conducted so far.
Etanercept
Etanercept blocks tumor necrosis factor-α (TNFα) activity and has been shown to suppress ongoing EAMG.Citation71 Etanercept was used in a prospective pilot trial in corticosteroid-dependent autoimmune MG: 70% of patients who completed the trial improved their muscle strength and lowered corticosteroid requirement. A direct correlation between plasma IL-6, TNF-α, and interferon-γ levels and post-treatment clinical scores of the patients was found.Citation72,Citation73 However disease worsening was seen in some patients and MG has been also observed during treatment of rheumatoid arthritis with etanercept through a RCT.
Complement inhibitors
The role of complement in the pathogenesis of MG is well established; indeed, complement activation by specific autoantibodies is involved in the attack to the NMJ, as demonstrated by localization of C3 activation fragments and membrane attack complex. Recently, administration of a complement inhibitor to experimental MG animals reduced the severity of the disease as well as complement deposition at neuromuscular end-plates; these observations are of great interest for a potential application in humans.Citation74
Oral and nasal tolerance
Oral tolerization to the AChR has been achieved in rats using recombinant fragments of the AChR alpha subunit and in mice with synthetic peptides corresponding to the main immunogenic epitopes of the AChR.Citation75,Citation76 Both approaches were able to reduce the clinical manifestations of the disease in experimental animals as well as specific autoantibodies. Different mechanisms have been postulated, according to the route of administration, dosage (high vs low dose) and schedule. Induction of anti-inflammatory cytokines (particularly transforming growth factor-β) has been observed in tolerized animals. Tolerization has also been induced by the nasal delivery of the antigen. However, the potential transfer of these protocols to humans implies the availability of large amounts of nonimmunogenic autoantigens or recombinant fragments of the original molecule.
Modulation of AChE expression
Innovation in the symptomatic therapy of MG involves the use of oral antisense oligonucleotides able to cause targeted gene transcription inhibition, thus interacting with specific complementary mRNA: EN101 antisense (Monarsen) reduces the levels of read through splicing variant of AChE. Preliminary results from a phase Ib clinical trial seem to be promising;Citation77,Citation78 in particular the effect of EN101 seems to last for more than 24 hours, providing the obvious advantage of a single daily administration.
Cellular therapy
A further perspective for specific immunotherapy in MG may derive from the manipulation of professional antigen-presenting cells (dendritic cells) by AChR proteins or peptides or by the mobilization of antigen-specific regulatory T cells; these therapeutic approaches were shown to be effective in preventing the induction of or in treating EAMG.Citation79–Citation81 However, transfer of such cellular treatments to human beings needs to address several technical and production issues, such as cell specificity, amount of cell production, and good manufacturing practice, which are not yet fully addressed.
Specific anti-AChR removal
Expression of the extracellular domains (ECD) of the different subunits of the AChR by molecular biology techniques provided the basis for a specific removal of anti-AChR antibodies. Indeed, these recombinant ECDs were coupled to insoluble carriers which were used to immunoadsorb antibodies derived from MG patients. Anti-AChR antibodies were depleted and the procedure was sufficiently efficient to eliminate pathogenic factors from MG sera, thus proving the feasibility of the procedure.Citation82 Further improvements will be necessary to increase the efficiency of antibody removal and to scale up the procedure to undergo proper clinical trials.
Reduction of AChR modulation at the NMJ
Reduction of antigenic modulation was attempted in EAMG using different approaches: a) by increasing the expression of rapsyn, a protein essential for the proper anchoring of the AChR at the NMJ; b) by functional competition of monovalent IgG4 anti-AChR antibodies. Both approaches were successful in preventing MG disease activity.Citation83,Citation84
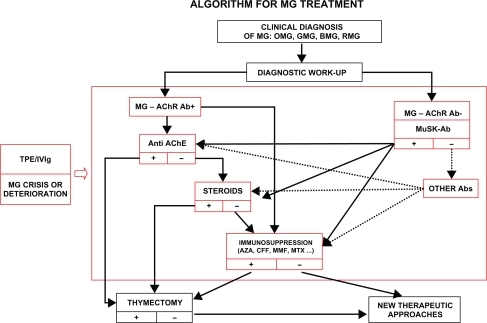
MG, although a rare disease, has become a prototype extensively studied for the identification of the immunopathogenetic mechanisms underlying autoantibody-mediated diseases. The investigation of experimental models, clinical practice (some times dated back to the 1980–1990’s), the development of clinical reaserch, and technological innovation have generated a rationale flow-chart for MG treatment (see ) which considerably improved the prognosis of patients and widened the perspective of more specific and selected therapeutic approaches.
Figure 2 The algorithm for treatment of myasthenia gravis illustrates the different decisional flow-chart for different subgroups of the disease.
Disclosure
The authors disclose no conflicts of interest.
References
- LindstromJMSeyboldMELennonVAWhittinghamSDuaneDDAntibody to acetylcholine receptor in myasthenia gravis. Prevalence, clinical correlates, and diagnostic valueNeurology1976261110541059988512
- VincentAUnravelling the pathogenesis of myasthenia gravisNat Rev Immunol200221079780412360217
- SouroujonMCBrennerTFuchsSDevelopment of novel therapies for MG: Studies in animal modelsAutoimmunity2010435–644646020298126
- WolfeGIOhSJClinical phenotype of muscle-specific tyrosine kinaseantibody-positive myasthenia gravisAnn N Y Acad Sci20081132717518567855
- LeiteMIJacobSViegasSIgG1 antibodies to acetylcholine receptors in ‘seronegative’ myasthenia gravisBrain200813171940195218515870
- ShiraishiHMotomuraMYoshimuraTAcetylcholine receptors loss and postsynaptic damage in MuSK antibody-positive myasthenia gravisAnn Neurol200557228929315668981
- SelcenDFukudaTShenXMEngelAGAre MuSK antibodies the primary cause of myasthenic symptoms?Neurology200462111945195015184594
- ColeRNReddelSWGervásioOLPhillipsWDAnti-MuSK patient antibodies disrupt the mouse neuromuscular junctionAnn Neurol200863678278918384168
- DrachmanDBMyasthenia gravisN Engl J Med199433025179718108190158
- BernasconiPBarberisMBaggiFIncreased Toll-like receptor 4 expression in thymus of myasthenic patients with thymitis and thymic involutionAm J Pathol2005167112913915972959
- CavalcantePSerafiniBRosicarelliBEpstein-Barr virus persistence and reactivation in myasthenia gravis thymusAnn Neurol201067672673820517934
- EvoliAMinisciCDi SchinoCThymoma in patients with MG: characteristics and long-term outcomeNeurology200259121844185012503581
- MaggiLAndreettaFAntozziCThymoma-associated myasthenia gravis: outcome, clinical and pathological correlations in 197 patients on a 20-year experienceJ Neuroimmunol2008201–202237244
- PhillipsLH2ndTornerJCEpidemiologic evidence for a changing natural history of myasthenia gravisNeurology1996475123312388909435
- PhillipsLH2ndThe epidemiology of myasthenia gravisAnn N Y Acad Sci200399840741214592908
- MeriggioliMNSandersDBAutoimmune myasthenia gravis: emerging clinical and biological heterogeneityLancet Neurol20098547549019375665
- AragonèsJMBolíbarIBonfillXMyasthenia gravis: a higher than expected incidence in the elderlyNeurology20036061024102612654975
- VincentACloverLBuckleyCEvidence of underdiagnosis of myasthenia gravis in older peopleJ Neurol Neurosurg Psychiatry20037481105110812876244
- AarliJAMyasthenia gravis in the elderly: Is it differentAnn N Y Acad Sci2008113223824318567874
- MantegazzaRAntozziCPeluchettiDSghirlanzoniACornelioFAzathioprine as a single drug or in combination with steroids in the treatment of myasthenia gravisJ Neurol198823584494533062134
- JaretzkiA3rdBarhonRJErnstoffRMMyasthenia gravis: recommendations for clinical research standards. Task Force of the Medical Scientific Advisory Board of the Myasthenia Gravis Foundation of AmericaNeurology2000551162310891897
- BenatharMKaminskiHJEvidence report: the medical treatment of ocular myasthenia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of NeurologyNeurology200768242144214917460154
- SkeieGOApostolskiSEvoliAGuidelines for the treatment of autoimmune neuromuscular transmission disordersEur J Neurol200613769169916834699
- SiebJPKöhlerWBenefits from sustained-release pyridostigmine bromide in myasthenia gravis: results of a prospective multicenter open-label trialClin Neurol Neurosurg2010112978178420663605
- BerrouschotJBaumannIKalischewskiPSterkerMSchneiderDTherapy of myasthenic crisisCrit Care Med1997257122812359233752
- MayerSAThomasCETherapy of myasthenic crisisCrit Care Med1998266113611379635669
- OosterhuisHJThe natural course of myasthenia gravis: a long term follow up studyJ Neurol Neurosurg Psychiatry19895210112111272795037
- OssermanKEProgress report on mestinon bromide (pyridostigmine bromide)Am J Med195519573773913268474
- Meda Group, Sweden (Data on file).
- BeekmanRKuksJBOosterhuisHJMyasthenia gravis: diagnosis and follow-up of 100 consecutive patientsJ Neurol199724421121189120493
- PungaARSawadaMStålbergEVElectrophysiological signs and the prevalence of adverse effects of acetylcholinesterase inhibitors in patients with myasthenia gravisMuscle Nerve200837330030718069667
- ShapiraMTur-KaspaIBosgraafLA transcription-activating polymorphism in the ACHE promoter associated with acute sensitivity to anti-acetylcholinesterasesHum Mol Genet200099127312810814709
- AhmedSKirmaniJFJanjuaNAn update on myasthenic crisisCurr Treat Options Neurol20057212914115676116
- LacomisDMyasthenic crisisNeurocrit Care20053318919416377829
- Jani-AcsadiALisakRPMyasthenic crisis: guidelines for prevention and treatmentJ Neurol Sci20072611–212713317544450
- EvoliABianchiMRRisoRResponse to therapy in myasthenia gravis with anti-MuSK antibodiesAnn N Y Acad Sci20081132768318567856
- EvoliATonaliPAPaduaLClinical correlates with anti-MuSK antibodies in generalized seronegative myasthenia gravisBrain2003126102304231112821509
- PungaARFlinkRAskmarkHStålbergEVCholinergic neuromuscular hyperactivity in patients with myasthenia gravis seropositive for MuSK antibodyMuscle Nerve200634111111516453324
- FerreroSPrettaSNicolettiAPetreraPRagniNMyasthenia gravis: management issues during pregnancyEur J Obstet Gynecol Reprod Biol2005121212913816054951
- HoffJMDaltveitAKGilhusNEMyasthenia gravis in pregnancy and birth: identifying risk factors, optimising careEur J Neurol2007141384317222111
- FauciASDaleDCBalowJEGlucocorticosteroid therapy: mechanism of action and clinical considerationAnn Intern Med1976843304315769625
- PascuzziRMCoslettHBJohnsTRLong-term corticosteroid treatment of myasthenia gravis: report of 116 patientsAnn Neurol19841532912986721451
- SghirlanzoniAPeluchettiDMantegazzaRFiacchinoFCornelioFMyasthenia gravis: prolonged treatment with steroidsNeurology19843421701746538004
- Schneider-GoldCGajdosPToykaKVHohlfeldRRCorticosteroids for myasthenia gravisCochrane Database Syst Rev20052CD00282815846640
- KupersmithMJOcular myasthenia gravis: treatment successes and failures in patients with long-term follow-upJ Neurol200925681314132019377863
- MeeJPaineMByrneEKingJReardonKO′DayJImmunotherapy of ocular myasthenia gravis reduces conversion to generalized myasthenia gravisJ Neuroophthalmol200323425125514663303
- HartIKSathasivamSSharsharTImmunosuppressive agents for myasthenia gravisCochrane Database Syst Rev20074CD00522417943844
- PalaceJNewsom-DavisJLeckyBA randomized double-blind trial of prednisolone alone or with azathioprine in myasthenia gravis. Myasthenia Gravis Study GroupNeurology1998506177817839633727
- EvansWEMcLeodHLPharmacogenomics – drug disposition, drug targets, and side effectsN Engl J Med2003348653854912571262
- TindallRSRollinsJAPhillipsJTGreenleeRGWellsLBelendiukGPreliminary results of a double-blind, randomized, placebo-controlled trial of cyclosporine in myasthenia gravisN Engl J Med1987316127197243547126
- DrachmanDBAdamsRNHuRJohnsRJBrodskyRARebooting the immune system with high-dose cyclophosphamide for treatment of refractory myasthenia gravisAnn N Y Acad Sci2008113230531418567882
- SandersDBHartIKMantegazzaRAn international, phase III, randomized trial of mycophenolate mofetil in myasthenia gravisNeurology200871640040618434638
- Muscle Study GroupA trial of mycophenolate mofetil with prednisone as initial immunotherapy in myasthenia gravisNeurology200871639439918434639
- AntozziCGemmaMRegiBA short plasma exchange protocol is effective in severe myasthenia gravisJ Neurol199123821031071856735
- GajdosPChevretSToykaKPlasma exchange for myasthenia gravisCochrane Database Syst Rev20024CD00227512519572
- GajdosPTranchantCClairBTreatment of myasthenia gravis exacerbation with intravenous immunoglobulinArch Neurol200562111689169316286541
- ZinmanLNgEBrilVIV immunoglobulin in patients with myasthenia gravis. A randomized controlled trialNeurology2007681183784117353471
- GajdosPChevretSIntravenous immunoglobulin for myasthenia gravisCochrane Database Syst Rev20081CD00227718254004
- DonofrioPDBergerABrannaganTH3rdConsensus statement: the use of intravenous immunoglobulin in the treatment of neuromuscular conditions report of the AANEM ad hoc committeeMuscle Nerve200940589090019768755
- SamuelssonGExtracorporeal immunoadsorption with protein A: technical aspects and clinical resultsJ Clin Apher2001161495211309835
- BoschTTherapeutic apheresis. State of the art in the year 2005Ther Apher Dial20059645946816354277
- BuckinghamJMHowardFMJrBernatzPEThe value of thymectomy in myasthenia gravis: a computer-assisted matched studyAnn Surg19761844534581015890
- GronsethGSBarohnRJPractice parameter: thymectomy for autoimmune myasthenia gravis (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of NeurologyNeurology200055171510891896
- MantegazzaRBaggiFBernasconiPVideo-assisted thoracoscopic extended thymectomy and extended transsternal thymectomy (T-3b) in non-thymomatous myasthenia gravis patients: remission after 6 years of follow-upJ Neurol Sci20032121–2313612809996
- GilbertMEde SousaEASavinoPJOcular myasthenia gravis treatment: the case against prednisone therapy and thymectomyArch Neurol200764121790179218071047
- LuchanokUKaminskiHJOcular myasthenia: diagnostic and treatment recommendations and the evidence baseCurr Opin Neurol200821181518180646
- IllaIDiaz-ManeraJRojas-GarciaRSustained response to Rituximab in anti-AChR and anti-MuSK positive Myasthenia Gravis patientsJ Neuroimmunol2008201–2029094
- LebrunCBourgVTieulieNThomasPSuccessful treatment of refractory generalized myasthenia gravis with rituximabEur J Neurol200916224625019146644
- NelsonRPJrPascuzziRMKesslerKRituximab for the treatment of thymoma-associated and de novo myasthenia gravis: 3 cases and reviewJ Clin Neuromuscul Dis200910417017719494727
- StieglbauerKTopakianRSchäfferVAichnerFTRituximab for myasthenia gravis: three case reports and review of the literatureJ Neurol Sci20092801–212012219272616
- ChristadossPGoluszkoETreatment of experimental autoimmune myasthenia gravis with recombinant human tumor necrosis factor receptor Fc proteinJ Neuroimmunol20021221–218619011777558
- RowinJMeriggioliMNTuzunELeurgansSChristadossPEtanercept treatment in corticosteroid-dependent myasthenia gravisNeurology200463122390239215623708
- TuzunEMeriggioliMNRowinJYangHChristadossPMyasthenia gravis patients with low plasma IL-6 and IFN-gamma benefit from etanercept treatmentJ Autoimmun200524326126815848049
- ChristadossPTuzunELiJSainiSSYangHClassical complement pathway in experimental autoimmune myasthenia gravis pathogenesisAnn N Y Acad Sci2008113221021918567870
- BaggiFAndreettaFCaspaniEOral administration of an immunodominant T-cell epitope downregulates Th1/Th2 cytokines and prevents experimental myasthenia gravisJ Clin Invest199910491287129510545527
- ImSHBarchanDFuchsSSouroujonMCMechanism of nasal tolerance induced by a recombinant fragment of acetylcholine receptor for treatment of experimental myasthenia gravisJ Neuroimmunol20001111–216116811063834
- ArgovZMcKeeDAgusSTreatment of human myasthenia gravis with oral antisense suppression of acetylcholinesteraseNeurology200769769970017698793
- SussmanJDArgovZMcKeeDHazumEBrawerSSoreqHAntisense treatment for myasthenia gravis: experience with monarsenAnn N Y Acad Sci2008113228329018567879
- XiaoBGDuanRSLinkHHuangYMInduction of peripheral tolerance to experimental autoimmune myasthenia gravis by acetylcholine receptor-pulsed dendritic cellsCell Immunol20032231636912914759
- DuanRSAdikariSBHuangYMLinkHXiaoBGProtective potential of experimental autoimmune myasthenia gravis in Lewis rats by IL-10-modified dendritic cellsNeurobiol Dis200416246146715193302
- ShengJRLiLCGaneshBBPrabhakarBSMeriggioliMNRegulatory T cells induced by GM-CSF suppress ongoing experimental myasthenia gravisClin Immunol2008128217218018502693
- TzartosSBitzopoulouKGavraIAntigen-specific apheresis of pathogenic autoantibodies from myasthenia gravis seraAnn N Y Acad Sci2008113229129918567880
- LosenMMartinez-MartinezPPhernambucqMTreatment of myasthenia gravis by preventing acetylcholine receptor modulationAnn N Y Acad Sci2008113217417918567867
- Van der Neut KolfschotenMSchuurmanJLosenMAnti-inflammatory activity of human IgG4 antibodies by dynamic Fab arm exchangeScience200731758441554155717872445