
Abstract
Herpes simplex encephalitis is a rare disease. In adults, most of the reported cytomegalovirus (CMV) infections are seen in immunocompromised patients. We present a case of 67-year-old Chinese male with the coinfection of CMV and herpes simplex virus type II (HSV-II). He had no history of being treated with immunosuppressants, showed symptoms of psychosis and was scored 109 on the Positive and Negative Syndrome Scale. This patient presented with a rare case of coinfection of CMV and herpes simplex virus type II with psychotic symptoms.
Keywords:
Introduction
Although herpes simplex virus (HSV) infections are very common worldwide, herpes simplex encephalitis (HSE) is a rare disease with an incidence of one case per 250,000–500,000 individuals per year. Approximately 50% of patients with HSE are older than 50 years.Citation1 Cytomegalovirus (CMV), another member of the herpesvirus family, is the most common cause of congenital infection, with a prevalence rate of 0.2%–2.5% in all live newborns.Citation2,Citation3 In adults, most reported CMV infections are seen in immunocompromised patients such as those with HIV (human immunodeficiency virus)Citation4,Citation5 and after chemoradiotherapy.Citation6 In these cases, the patients were also co-infected with HSV. Here, we present a patient with coinfection of CMV and HSV type II (HSV-II), who was admitted to the hospital for acute psychotic symptoms, but never treated with immunosuppressants before this admission.
Case report
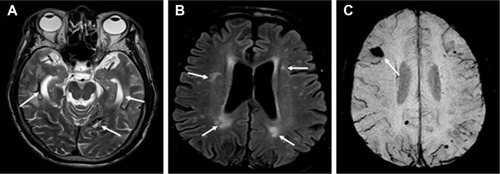
For acute psychotic symptoms of delirium, delusion of persecution, fidget, over-alertness, and aggressive behaviors, a 67-year-old Chinese man was sent to the outpatient department of the Shantou Central Hospital, Guangdong province, People’s Republic of China, on October 15, 2013. Three days before, the patient complained of headache. On October 14, he became suspicious, had delusion of persecution, and ran around. On the same day, he was sent to the local hospital where a magnetic resonance imaging was performed showing multiple hyperintensities in the left occipital lobe and temporal lobes in the T2-weighted images (). In addition, multiple hyperintensity lesions were seen in the temporal and parietal lobes and demyelination lesions in the white matter surrounding the lateral ventricles in the fluid-attenuated inversion recovery images (). Then, the patient was referred to the Shantou Central Hospital, Affiliated Shantou Hospital of Sun Yat-sen University on October 15.
Figure 1 Magnetic resonance imaging of the patient’s brain.
On examination, the patient was somnolent and in the delirious state. But, physical examinations showed no abnormalities (normal blood pressure and there was no fever). There was no meningeal irritation sign and no Babinski sign on either sides. The Positive and Negative Syndrome Scale score was 109 (positive syndrome score of 36, negative of 14, and general of 59). The patient had no history of head trauma and hospitalization for mental disorders or any tumors, according to the family members.
Emergency treatment was started with the administration of the tranquilizer sodium phenobarbital (100 mg) to reduce dysphoria and aggressive behaviors, the mood stabilizer sodium valproate (100 mg, administered in two fractions) to stabilize the mental state of the patient, and the antipsychotic olanzapine (10 mg, administered in four fractions) for the delusion of persecution. In addition, along with supportive treatments (piracetam 20 grams in 100 mL 0.9% sodium chloride), empirical administration of antiviral treatment (ganciclovir 250 mg in 0.9% sodium chloride) was instituted under suspicion of viral encephalitis.
On October 16, a blood examination was performed which showed no anemia and leukocytosis, but presented a higher percentage of neutrophil number (80.60%; reference range 40%–75%), a lower percentage of lymphocytes (11.70%; reference range 20%–50%), very high levels of creatine kinase (CK; 619 U/L, reference range 0–174 U/L) and its isoenzyme (CKMB; 39 U/L, reference range 0–24 U/L). In addition, a higher level of C-reactive protein (CRP, 113 mg/L; 0–8 mg/L) was found. No HIV antibodies were found. Chest radiographs (October 17) showed stale tuberculous lesions in the upper lobe of right lung.
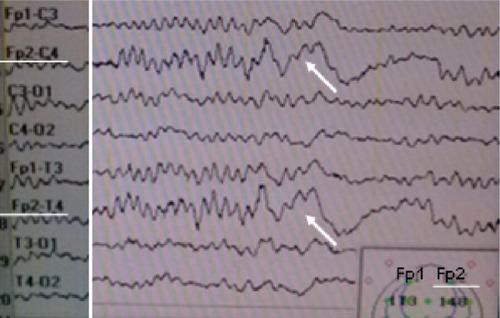
On October 18, while the psychotic symptoms were improved, rough breath sounds were heard in the lungs, suggesting the presence of an infection there. Therefore, the antibiotic treatment with piperacillin-tazobactam (4,500 mg in 0.9% sodium chloride) was initiated while the other treatments continued. On the same day, an electroencephalogram was performed showing slow waves characterized by strong peaks of delta and theta frequencies in the frontal lobe of the right hemisphere (). On October 19, a susceptibility-weighted imaging was performed, which more clearly showed the stale hemorrhages in the frontal lobe of the right hemisphere (), in addition to those seen in the left occipital lobe and temporal lobes of both sides.
Figure 2 The electroencephalogram of the patient showing slow-waves characterized by strong peaks of delta (δ) and theta (θ) frequencies in the right frontal lobe.
The outcomes of cerebrospinal fluid (CSF) examination came out on October 20, 21, and 22, respectively, showing blood cells in normal ranges, mild lower levels of chloride (117 mmol/L; reference range 120–132 mmol/L), and glucose (2.41 mmol/L; reference range 2.8–4.5 mmol/L). No bacteria were found. But both anti-CMV IgG and anti-HSV-II IgM were positive, supporting a diagnosis of coinfection with HSV-II and CMV in the brain. His body temperature was 37.3°C. The antiviral and antipsychotic treatments continued.
On October 28, as required by the family members, the patient was discharged. His psychotic symptoms were significantly improved as evidenced by the reduction of Positive and Negative Syndrome Scale from 109 to 71 (positive syndrome score of 14, negative of 13, and general of 44).
The patient continued the antiviral and antipsychotic treatments at home after the discharge from the hospital. He died of progressive cachexia 4 months after the discharge (February 26, 2014), although his psychotic symptoms did not relapse. The patient’s family members authorized the publication of his case. The ethics committee of the Shantou Central Hospital did not require approval for this case study.
Discussion
Except for one early case report,Citation7 all other double infections of the central nervous system (CNS) with CMV and HSV were reported in immunocompromised patients.Citation4–Citation6,Citation8 The patient reported here had no history of being treated with immunosuppressants. His blood examination showed normal cell count despite of the presence of anti-CMV IgG and anti-HSV-II IgM in CSF, which is in accordance with the reported evidence for increased production of antibodies against several neurotropic infectious pathogens including HSV-I, HSV-II, and CMV, in the CSF of individuals with bipolar disorderCitation9 or autism spectrum disorders.Citation10,Citation11 The mild signs of CNS inflammation in this patient may account for the absence of seizures and focal neurological signs although he presented primarily acute psychotic symptoms and mental status changes. In line with this patient with HSV-II infection, neurological sequelae were more frequent among patients with HSV-I compared with those infected with HSV-II.Citation12 In addition, CMV encephalitis in immunocompetent individuals has been associated with mild signs of CNS inflammation, including absent to moderate pleocytosis.Citation13–Citation15 In contrast, CMV in immunocompromised patients was featured with more severe clinical manifestations.Citation5,Citation6,Citation16
The pathological hallmark of HSE is hemorrhagic necrosis in the medial part of the temporal lobes. In addition, adjacent areas such as the orbital surface of the frontal lobe and cingulate gyrus may be involved. In line with these, magnetic resonance imaging of this patient showed hemorrhages in multiple regions of the brain, including the right frontal lobe, left occipital lobe, and the temporal lobes of both sides. The hemorrhage in the right frontal lobe may be related to the peaks of delta and theta frequencies seen in electroencephalogram of this brain region. In addition, this patient showed multiple small infarctions and demyelination in the white matter surrounding the lateral ventricles. The multiple small infarctions may be the consequence of CMV infection. In line with this speculation, animal, and human studiesCitation17–Citation20 have shown the CMV-induced damage of microvascular endothelium, vasculitis, thrombotic occlusions, and hemorrhages.
Another feature of this patient is a very high level of CRP in his blood. The co-existence of high CRP level and the antibodies to CMV and HSV-II reminded us of a recent human study, in which the CRP level was strongly associated with viral detection rate and mixed viral/bacterial detection rate; whereas the rate of bacterial detection was not associated with the CRP level.Citation21 More significantly, plasma CRP was an independent predictor of mortality in patients with chronic obstructive pulmonary disease caused by virus infections.Citation21,Citation22
In summary, we present a case of a 67-year-old male with coinfection of CMV and HSV-II and without history of being treated with immunosuppressants. The presence of his psychosis symptoms and absence of neurological manifestations may represent the clinical features of coinfection of CMV and HSV-II.
Disclosure
The authors report no conflicts of interest in this work.
References
- LakemanFDWhitleyRJDiagnosis of herpes simplex encephalitis: application of polymerase chain reaction to cerebrospinal fluid from brain-biopsied patients and correlation with disease. National Institute of Allergy and Infectious Diseases Collaborative Antiviral Study GroupJ Infect Dis19951718578637706811
- MalmGEngmanMLCongenital cytomegalovirus infectionsSemin Fetal Neonatal Med20071215415917337260
- González-SánchezHMMonsiváis-UrendaASalazar-AldreteCAEffects of cytomegalovirus infection in human neural precursor cells depend on their differentiation stateJ Neurovirol20152134635725851778
- VagoLNebuloniMSalaECoinfection of the central nervous system by cytomegalovirus and herpes simplex virus type 1 or 2 in AIDS patients: autopsy study on 82 cases by immunohistochemistry and polymerase chain reactionActa Neuropathol1996924044088891073
- KatchanovJBrandingGStockerHCombined CMV- and HSV-1 brainstem encephalitis restricted to medulla oblongataJ Neurol Sci201433922923024582285
- SuzukiHIHangaishiAHosoyaNHerpes simplex encephalitis and subsequent cytomegalovirus encephalitis after chemoradiotherapy for central nervous system lymphoma: a case report and literature reviewInt J Hematol20088753854118415654
- YanagisawaNToyokuraYShirakiHDouble encephalitis with herpes simplex virus and cytomegalovirus in an adultActa Neuropathol197533153164173128
- LaskinOLStahl-BaylissCMMorgelloSConcomitant herpes simplex virus type 1 and cytomegalovirus ventriculoencephalitis in acquired immunodeficiency syndromeArch Neurol1987448438472820361
- StichOAndresTAGrossCMGerberSIRauerSLangoschJMAn observational study of inflammation in the central nervous system in patients with bipolar disorderBipolar Disord20151729130225109751
- GentileIZappuloEBonavoltaRPrevalence of herpes simplex virus 1 and 2 antibodies in patients with autism spectrum disordersIn Vivo20142866767124982239
- GentileIZappuloEBonavoltaRPrevalence and titre of antibodies to cytomegalovirus and epsteinbarr virus in patients with autism spectrum disorderIn Vivo20142862162624982232
- MoonSMKimTLeeEMKangJKLeeSAChoiSHComparison of clinical manifestations, outcomes and cerebrospinal fluid findings between herpes simplex type 1 and type 2 central nervous system infections in adultsJ Med Virol2014861766177125042344
- PhillipsCAFanningWLGumpDWPhillipsCFCytomegalovirus encephalitis in immunologically normal adults. Successful treatment with vidarabineJAMA197723822992300199755
- ProschSSchielkeEReipAHuman cytomegalovirus (HCMV) encephalitis in an immunocompetent young person and diagnostic reliability of HCMV DNA PCR using cerebrospinal fluid of nonimmunosuppressed patientsJ Clin Microbiol199836363636409817887
- StudahlMRickstenASandbergTBergströmTElowsonSCytomegalovirus encephalitis in four immunocompetent patientsLancet1992340104510461357442
- XuXBergmanPWillowsTCMV-associated encephalitis and antineuronal autoantibodies – a case reportBMC Neurol2012128722947340
- FoucarEMukaiKFoucarKSutherlandDEVan BurenCTColon ulceration in lethal cytomegalovirus infectionAm J Clin Pathol1981767888016274185
- FrancisNDBoylstonAWRobertsAHGParkinJMPinchingAJCytomegalovirus infection in gastrointestinal tracts of patients with HIV-1 or AIDSJ Clin Pathol198942105510642555397
- GoldenMPHammerSMWankeCAAlbrechtMACytomegalovirus vasculitis. Case reports and reviews of the literatureMedicine (Baltimore)1994732462557934809
- PersoonsMCJStalsFSVan Dam MierasMCEBruggemanCAMultiple organ involvement during experimental cytomegalovirus infection is associated with disseminated vascular pathologyJ Pathol19981841031099582535
- ClarkTWMedinaMJBathamSCurranMDParmarSNicholsonKGC-reactive protein level and microbial aetiology in patients hospitalised with acute exacerbation of COPDEur Respir J201545768625186260
- LuSLiTXiXPrognosis of 18 H7N9 avian influenza patients in ShanghaiPLoS One20149e8872824695420