
Abstract
Purpose
This study aimed to investigate the mediation effects of resilience in the correlation between burden and Quality of Life (QoL) among Family Caregivers (FCs) of stroke survivors.
Patients and Methods
This cross-sectional study was conducted using outpatient services. The study sample included 134 FCs from stroke survivors. Demographic and clinical information were obtained using medical records and questionnaires. The Connor-Davidson Resilience Scale (CD-RISC) was used to measure FCs’ resilience. Caregiver Burden (CB) scale was used to measure FCs burden. The WHOQOL-BREF was used to measure the QoL of the FCs. Path analysis was used to determine the mediating effect of resilience on CB and QoL. To address the influence of resilience, path coefficients were divided into direct and indirect effects.
Results
The results of the path analysis between the CD-RISC and CB scale were significant at 0.01. The same was true for the path between the CD-RISC and WHOQOL-BREF (p< 0.01). The path coefficients were divided into direct and indirect effects to address the influence of resilience on CB and QoL. The findings showed that resilience negatively correlated with the FCs burden (β = −0.279; 95% CI, − 0.383–0.175) and explained a 17.2% variance in the burden (R2 = 0.172, p < 0.001). QoL also negatively predicted the CB (β = −0.279; 95% CI, 0.025–0.279) and positively predicted resilience (β = 0.152; 95% CI, −0.365–0.193). The CB and resilience accounted for 34.7% of the variance in QoL (R2 = 0.347, p < 0.001). The indirect effect of CB on QoL mediated by resilience was −0.042 and the direct effect of burden on QoL was −0.321.
Conclusion
Resilience negatively mediated the correlation between CB and QoL of FCs of stroke survivors. Addressing resilience interventions in palliative care could alleviate this burden and improve the QoL of stroke survivors.
Introduction
According to World Stroke Organization in 2019, there were 3.3 million stroke cases worldwide that end up in death each year.Citation1 Stroke can significantly impact the disability in Activities of Daily Living (ADL), alter roles and functions within the family, lead to changes in social interactions, and result in reduced employment opportunities.Citation2,Citation3 Family caregivers (FCs) have roles and responsibilities in taking care of the member of the family who suffers from stroke. Several studies have elucidated that the scope of Caregiver Burden (CB) encompasses the strain experienced by individuals caring for a disabled family member.Citation4,Citation5 Although the FCs of stroke survivors experience stress and burden while caring for the patient, providing care for a sick family member is considered normal.Citation4 As FCs of stroke survivors, several consequential impacts are observed. Specifically, FCs attending to stroke patients with functional disabilities experience a 3.7-fold increase in risk of burden compared to those caring for stroke patients without such disabilities.Citation5 In addition, another study found that FCs of stroke survivors with emotional and cognitive problems were reported to have high levels of burden.Citation6 Thus, burdens would have negative impacts such as Quality of Life (QoL) and physical and psychological health deterioration.Citation7
Previous studies have underscored the necessity of resilience among FCs when confronting stressful conditions or bearing the burdens associated with caring for ill family members. Resilience is defined as the capacity to adapt successfully to disturbances that threaten function and development. Furthermore, a caregiver’s resilience is closely associated with emotional intelligence and mental health.Citation8 Resilience also increased positive emotions and reduced negative emotions and feelings of overload among caregivers.Citation8 A previous systematic review indicated that a caregiver’s resilient coping style can mitigate the risk of stress and burden, thereby facilitating adaptation during caring for ill family members.Citation9 Resilience exhibited by FCs plays a pivotal role in achieving effective adaptation to manage life’s pressures.Citation10 Having resilience in the family organizing process would build family connections, adaptability, and family resources.Citation11,Citation12 Thus, resilience is necessary for the adaptation of high-risk care due to stroke.Citation10
Since the quality of life of both stroke patients and their families has become the goal of palliative care,Citation13,Citation14 it is imperative that QoL receives focused attention. This entails a thorough review of studies on QoL, particularly those investigating methods to improve it. Many studies have shown that burden is correlated with QoL. Burden arises from the tasks of FCs in caring for stroke patients, economic difficulties, and changes in family roles. Such burdens precipitate symptoms of stress, anxiety, and sleep disturbances among FCs, consequently diminishing their QoL.Citation15,Citation16 In the context of resilience theory, resilience is needed under stressors and burden conditions, exerting a positive influence.Citation11 Previous research has proven the role of resilience as a mediator in the correlation between CB and QoL among FCs of the cancer population.Citation17 Similarly, resilience serves as a mediator between the burden experienced by FCs of stroke survivors and the depressive symptoms observed in patients.Citation18
Considering the importance of resilience in supporting FCs to achieve an optimal QoL, research examining the resilience of FCs and the correlation between CB and QoL is needed. To our knowledge, no published studies have examined the influence of FC resilience on CB and QoL among stroke survivors. Addressing this gap, the current study aimed to investigate the influence of resilience on the correlation between CB and QoL among FCs of stroke survivors. In this context, this study sought to address the following questions.
What is the level of resilience among FCs of stroke survivors?
Is there a correlation between resilience, CB and QoL in FCs of stroke survivors?
Does resilience influence CB and QoL of FCs among stroke survivors?
Materials and Methods
Design
This descriptive cross-sectional study was conducted between May and July 2020. This manuscript was prepared following the STROBE (Strengthening the reporting of observational studies in epidemiology) Checklist.
Participants
To calculate the required sample size, we used G*Power 3.1.7. Studies of these three variables are rare. Therefore, this study used Cohen’s f2 0.15, a power set of 0.95, and a significance at the level of 0.05. So, the minimum sample was 107 samples. In this study, 134 participants were involved using purposive sampling. The inclusion criteria were as follows: relatives of patients aged >18 years, a minimum of two hours of involvement in caring per day, and caring for patients for at least three months. In total, 145 eligible participants were contacted. An appointment was set for data collection from participants’ residences. Eleven participants were excluded from the study due to cancelled appointments and unverified residential locations. Consequently, this may have introduced potential bias, diminishing the representativeness of the study population. All FCs who met the inclusion criteria were included in this study. Upon providing their informed consent, participants proceeded to complete the assessment form.
Procedures
The participants were recruited from two Health Community Services in Indonesia. Once potential participants were identified and deemed eligible, the researcher (S˙ ID) explained all the study procedures, provided a copy of the written consent form, and made an appointment. As this study was conducted in humans, the procedures were performed following the ethical standards of the Declaration of Helsinki. The data were collected from FCs residences instead of Health Community Services to make FCs more comfortable Data were collected using the FCs Characteristics Form, Connor-Davidson Resilience Scale (CD-RISC), Caregiver Burden (CB) scale, and WHOQOL-BREF through face-to-face interviews with the researcher. Data collection from each participant required approximately 30 minutes.
Data Collection
An FC characteristic form was created to assess the participants’ sociodemographic information. The Connor-Davidson Resilience Scale (CD-RISC) is a measure of resilience.Citation19 It comprises of 25 items, each rated on a scale ranging from 0 to 4 points, with higher scores reflecting greater resilience. The scale assesses five components: 1) personal competence, high standards, and tenacity; 2) trust in one’s instincts, tolerance of negative affect, and strengthening the effects of stress; 3) positive acceptance of change and secure relationships; 4) control; and 5) spiritual influence. It showed good internal consistency (Cronbach’s alpha value of 0.89) and test–retest reliability, with an intraclass correlation coefficient of 0.87. It also presents good convergent validity with the Kobasa hardiness measureCitation20 and divergent validity with the Cohen stress measure.Citation21 The Cronbach’s α in this study was 0.857 among 134 FCs of stroke survivors involved.
Caregiver Burden (CB) scale using a 22-item scaleCitation22 that was developed in Sweden. The CB scale was divided into five components as a result of the previous factor analysis: general strain, isolation, disappointment, emotional involvement, and environment. The items are scored from 1 to 4 (never, rarely, sometimes, and always, respectively) and cover questions about caregivers’ health, feelings of psychological well-being, relationships, social networks, physical workload, and environmental aspects. The total burden index consists of the average of all 22 items with higher scores indicating a greater level of burden. The validity and internal consistency were tested among 150 family caregivers to 83 patients with dementia and 67 patients with stroke showing good agreement with Cronbach alpha values of about 0.70–0.87 for the five components.Citation22 The Cronbach’s α in this study was 0.933.
The WHOQOL-BREF measures caregivers’ QoL.Citation23 The Indonesia version of this scale has been validated.Citation24 Responses to each item of this 26-item self-report are recorded on a scale ranging from 0 (never) to 4 (always). This scale assesses four components: physical health, psychological and social relationships, and environment. The total score, computed by summing the individual item scores, ranged from 0 to 140. Higher scores indicate better QoL. Cronbach’s α of the Indonesian version of this scale was 0.88,Citation24 and 0.885 in our study.
Analysis
The sociodemographic characteristics of the participants were examined by calculating their frequencies and percentages. The Shapiro–Wilk test was used to examine whether the assumption of normality was met and, consequently, to ensure the appropriateness of the parametric analyses. The variables were normally distributed; therefore, parametric analysis was used. The associations and interrelations among CB, resilience, and QoL were examined using Pearson’s correlation analysis as measured both total and domains score. We also investigate the mediating effect of resilience, both directly and indirectly, in the correlation between burden and QoL as measured by total score. Unstandardized indirect effects for each variable and 95% confidence intervals (CIs) were also computed. For all analyses, the level of statistical significance was set at p < 0.05. All analyses were performed using IBM SPSS (version 29.0; IBM Corp., Armonk, NY, USA).
Ethical Considerations
Ethical approval for this study was obtained from the ethical board of the Faculty of Medicine, Universitas Diponegoro (No.77/EC/KEPK/FK-UNDIP/IV/2022). Necessary permissions were also obtained from the Health Ministry Office of Central Java, Indonesia, which regulates the Community Health Services in which this study was conducted. Furthermore, verbal and written informed consent was obtained from each participant before their inclusion in the sample, and anonymity was ensured. All written materials created during the study were used for research only.
Results
Sociodemographic Characteristics
The average age of the FCs was 50.4 ± 13.3 years. Of these, 61.2% (n = 82) were female, and 92.5% (n = 124) were married. Furthermore, 55.2% (n = 74) possessed at least a basic education degree, 54.5% (n = 74) had been providing care for more than 12 months, 38.8% (52) FCs were wives, 48.3% (62) reported an income above regional minimum wage, and 56.7% (76) belonged to nuclear families ().
Table 1 Characteristics of FCs (n=134)
FCs’ Resilience, CB, and QoL
The FCs reported moderate levels of resilience (CD-RISC total scores: 76.74 ± 7.99, min-max = 51–93), and low levels of burden (CB scale total scores: 40.6 ± 11.89 min-max = 23–73). The FCs reported high levels of QoL (WHOQOL-BREF total scores: 92.4 ± 6.7, min-max = 64–113) ().
Table 2 FCs Burden, Resilience, and Quality of Life
The Interrelationships Among Resilience, CB and QoL
The total CD-RISC score was significantly and negatively correlated with the total CB scale (−0.378) and positively with WHOQOL-BREF scores (0.246). The majority of the CD-RISC domains were significantly and negatively correlated with the CB scale. Pearson’s correlation coefficients ranged from 0.172 to 0.392 (all p < 0.01 or 0.05). Additionally, the CD-RISC domain scores were mostly significantly correlated with the environmental domain score of WHOQOL-BREF scores. Pearson’s correlation coefficients ranged from 0.204–0.383 (all p < 0.01 or 0.05). The total CD-RISC score and domains of CD-RISC were not significantly correlated with the physical health, psychological health, and social relationship domains of QoL ().
Table 3 Correlation of CB Scale, CD-RISC, and WHOQOL-BREF
The total CB scale was significantly and negatively correlated with the total WHOQOL-BREF (−0.566). The total CB scale and domains mostly correlated with social relationship and environment domains of WHOQOL-BREF scores. Pearson’s correlation coefficients ranged from 0.352–0.706 (all p < 0.01 or 0.05) ().
The Influences of Resilience on CB and QoL
Path analysis was used to determine the mediation of resilience on CB and QoL of FCs of stroke survivors (). As the normality of data was established, the maximum likelihood solution was used to formulate the model. The following standardized solutions to the specified measurement equations were produced using the maximum likelihood solution:
Equation (1): resilience (CD-RISCS) = (– 0.41) burden (CB) + (0.05) error.
Equation (2): resilience (CD-RISCS) = (0.18) QoL (CQOLC) + (0.06) error.
QoL= (–0.49) burden + (0.18) resilience + (0.044) error
Figure 1 The Model of Mediating Effect of Resilience on the Correlation between Burden and QoL among FCs of Stroke Survivors.
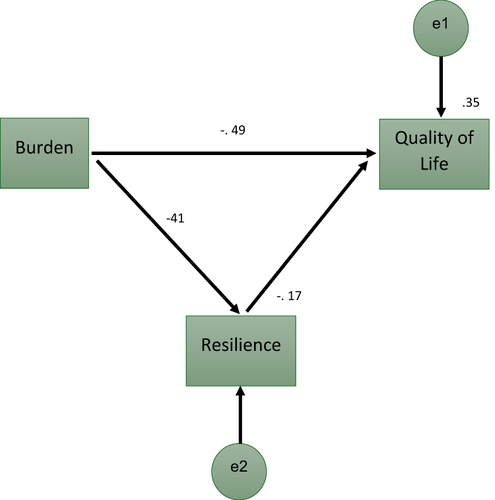
As shown in the path analysis model (), all paths between the variables were significant. The path between the CD-RISCS and CB scale was significant at the 0.01 level. The same was true for the path between the CD-RISC and WHOQOL-BREF (p< 0.01). The path coefficients were divided into direct and indirect effects to address the influence of resilience on CB and QoL. The direct and indirect effects of resilience on the correlation between CB and QoL are shown in and , respectively. This analysis supported the relationships proposed in the model. The findings showed that resilience negatively correlated with burden (β = −0.279; 95% CI, −0.383 – −0.1.75) and explained 17.2% of FCs burden (R2 = 0.172, P < 0.001). QoL was also negatively predicted by the burden (β = −0.279; 95% CI, 0.025–0.279) and resilience (β = 0.152; 95% CI, −0.365–0.193). Burden and resilience explained 34.7% of the variance in QoL (R2 = 0.347, P < 0.001) (). The indirect effect of burden on QoL mediated by resilience was −0.042 and the direct effect of burden on QoL was −0.321. Resilience mediated the correlation between burden and QoL ().
Table 4 Estimate Regression Weights
Table 5 Direct Effect, Indirect Effect, Total Effect, and Non-Causal Effect on Resilience, Burden, and QoL Among FCs Stroke Survivors
Discussion
This study aimed to assess resilience, CB, and QoL levels among FCs of stroke survivors, explore correlations between these variables, and examine the mediating role of resilience. Findings revealed moderate resilience, low caregiver burden, and high QoL. A significant negative correlation between resilience and CB, and a positive correlation between resilience and QoL were identified, alongside a negative correlation between CB and QoL. Importantly, resilience was found to mediate the relationship between CB and QoL, suggesting that enhancing resilience may alleviate the negative impact of CB on QoL.
In this study, resilience levels among FCs of stroke survivors were found to be moderate. This contrasts with findings from another study in West Sumatra Province, Indonesia, where FCs predominantly exhibited high resilience.Citation25 Interestingly, the latest study also unveiled that ethnicity plays a significant role in influencing resilience levels. The ethnic distinctions between the Javanese and the people of West Sumatra appear to contribute to this variance in resilience.Citation25 Furthermore, a study in China observed that resilience tends to be lower during the initial six months post-stroke onset, suggesting that families are still adapting to the new caregiving situation during this period. As such, resilience is in a state of development, highlighting the dynamic nature of coping mechanisms over time.Citation26 The phenomena differ from this study, where FCs vary from one month to more than one year in caring for stroke patients.
This study identified that the burden experienced by FCs of stroke survivors was low, contrasting with findings from another study in Indonesia where FCs predominantly reported a moderate level of burden.Citation27 That Indonesian study was conducted in a hospital outpatient setting, focusing on patients who had recently been discharged. The differing results could be attributed to the fact that these caregivers had only recently encountered the challenges of caregiving, hence lacking the capacity to effectively manage the burden at that time.Citation27 Conversely, this study involved FCs who had been caring for stroke survivors over a longer period post-attack, suggesting that these caregivers had become more accustomed to the obstacles associated with caregiving and had improved their adaptation strategies for dealing with the burden. A study in Brazil also reported a moderate level of burden among FCs, with participants in a hospital setting, indicating that their capacity to cope with the burden had not yet developed.Citation28 Additionally, research conducted in Myanmar found that the burden on FCs ranged from moderate to severe levels,Citation29 further highlighting the variability in caregiving experiences and the impact of caregiving duration and setting on the perceived burden.
This study found that FCs of stroke survivors reported a high level of QoL, contrasting with studies from Brazil and Burma, where FCs’ QoL was reported as moderate.Citation28,Citation29 The difference may stem from the setting of the studies; in Burma and Brazil, research was hospital-based, focusing on FCs who were likely facing immediate healthcare challenges impacting their physical and psychological well-being. Conversely, this study, conducted within the community, suggests that FCs have had the opportunity to adapt physically, mentally, and socially to the challenges of caregiving. This adaptation process is indicative of their overall well-being and suggests that community-based FCs may navigate and overcome obstacles more effectively, contributing to higher QoL levels.Citation30
This study reveals that resilience is crucial for FCs of stroke survivors, showing a negative correlation with CB. This aligns with findings from China, where resilience is similarly inversely related to CB. Caregiving is highlighted as a complex role, encompassing various challenges like social burden, responsibility, and emotional struggles, which significantly affect FCs’ lives.Citation31 Resilience emerges as a key coping mechanism, enhancing welfare,Citation30 and mitigating burden.Citation8 Furthermore, resilience’s benefits extend to improving recovery outcomes and reducing emotional distress, fostering a collaborative and supportive environment among caregivers.Citation32 It encourages an active lifestyle, a positive outlook, and mindfulness, underscoring the importance of resilience in managing caregiving challenges effectively.Citation31
This study highlighted the positive correlation between resilience and QoL, echoing past findings on resilience’s crucial role in boosting QoL for FCs of individuals with mental disorders.Citation15 Caregivers with greater resilience are better equipped to enhance their QoL, adeptly manage stressful situations, and not merely endure but also thrive, achieving a renewed equilibrium and positive development.Citation15 Resilience, viewed as a personal strength, impacts QoL across personal, family, and social levels. Particularly for dementia caregivers, engaging in self-care and leisure, especially during the disease’s moderate phase, is vital for boosting resilience.Citation33 In Indonesia, resilience among FCs of stroke survivors is influenced by socioeconomic and ethnic factors, indicating the substantial effect of cultural and environmental contexts on resilience.Citation25 Conceptual studies suggest that enhancing family resilience can improve outcomes for all members facing caregiving challenges, thus elevating overall QoL. These insights underscore the need to support resilience through personal care, family involvement, and social networks to better caregiving experiences and outcomes, highlighting QoL improvements.Citation34
This study identifies a significant correlation between CB and QoL, resonating with findings from prior research. Caregivers of stroke survivors, who often experience mental disorders, face a multifaceted burden that detrimentally impacts their QoL.Citation35 This burden encompasses a wide range of issues, including social responsibilities, advocacy challenges, emotional conflicts such as ambivalence and guilt, and difficulties in accepting the caregiving role, especially prevalent among families dealing with motor neuron diseases.Citation31 The caregiving role is inherently challenging, exerting adverse effects on various aspects of family caregivers’ lives, including their physical, psychological, and social well-being.Citation6 These negative impacts elucidate the correlation between burden and QoL, given that QoL encompasses physical, psychological, social relationships, and environmental domains.Citation24 Further support for this correlation comes from studies highlighting the negative relationship between burden and multiple QoL domains, including environmental factors, overall QoL levels, and physical health.Citation28 Moreover, CB emerges as a pivotal factor in explaining QoL variations, with education and perceived social support also playing significant roles among family caregivers of stroke survivors.Citation29 Additionally, the negative interplay between caregivers’ poor self-rated health, lower education levels, and QoL underscores the influence of both patient and caregiver factors—such as psychological, social, and physical functioning and caregiver health status—on the caregiving experience.Citation36
The present findings emphasize the influence of resilience on the association between burden and QoL. Moreover, the findings suggest that FCs have a moderate level of resilience, which is correlated with caregivers’ burden and QoL. According to this concept, family resilience refers to the capacity of a family to withstand and rebound from adversity. The fundamental premise of the family systems theory is that serious crises and persistent life challenges have an impact on the whole family, and, in turn, key family processes mediate adaptation for individual members, their relationships, and the family unit.Citation11 Resilience is essential for adapting the process to high-risk caregiving situations.Citation37
Other research supports the notion that recognizing and cultivating resilience, along with its related psychological aspects, can help mitigate stress and burden while enhancing well-being. Families of caregivers confronting the burden of some circumstances benefit significantly from resilience through collective confidence, interconnectedness, positive life of view, resourcefulness, open communication patterns, and collaborative problem-solving.Citation37 Being resilient involves engaging actively, adopting a positive outlook on life, and embracing the present moment to manage the burden and adversity effectively.Citation31,Citation37 Family resilience can lead to positive outcomes for all members, especially when navigating the challenges associated with caregiving.Citation34
Other studies highlighted the critical role of resilience in facilitating coping mechanisms among patients. Higher resilience leads to healthier psychological adaptation. Adaptation can affect the readiness of FCs to deal with acute or chronic traumatic events from the impact of caring for stroke patients.Citation38 Resilience also indirectly impacts how FCs cope with and manage challenging clinical situations that require early identification and treatment of the emotional and physical needs of patients.Citation9 Adaptation also affect the readiness of FCs in caring for stroke patients.Citation38 Overall, systematic study synthesized that a resilient coping style is correlated with a high QoL, good mental health, and increased personal resources that helped improve the caregiving experience in chronic illness context and reduced CB.Citation9
This study further demonstrates that resilience mediates the relationship between CB and QoL, a phenomenon also observed in research involving FCs of cancer patients. In these studies, resilience is identified as both a mediator and a risk factor for CB and QoL. Specifically, lower level of resilience among FCs are linked to increased burden and diminished QoL, whereas resilience serves as a protective factor against the negative impacts of CB on depressive symptoms.Citation17 One study highlighted the protective role of resilience in alleviating the negative influences of CB on depressive symptoms among stroke survivors’ FCs.Citation18 The significant and negative influence of stroke-related CB on QoL underscores that the potential of enhancing FCs’ resilience to alleviate their burden and, consequently, improve their QoL. The findings of this study, alongside others,Citation17,Citation18 support the premise of family resilience theory, positing that resilience can foster positive outcomes.Citation11
Burden and QoL were the focus of palliative care, yet efforts to address these issues often encounter obstacles.Citation14 The presence of resilience alongside CB and QoL suggests a viable pathway for reducing burden and improving QoL. The American Heart Association (AHA) recommends the promotion and implementation of patient-and family-centered care within the palliative care framework. Addressing the palliative care needs of patients and families throughout illness can complement the existing practices and improve the QoL of stroke patients, their families, and their care providers.Citation39 Resilience intervention in palliative care have the potential to lessen the burden and improve the QoL among FCs of stroke survivors.
This study is subject to certain limitations. This study did not investigate the factors that may influence resilience or QoL. Consequently, potential biases arising from other factors that could impact the mediation role of resilience in the relationship between burden and QoL remain unaddressed. Nevertheless, this study provides clarity in elucidating the mediating effect of resilience in the correlation between burden and QoL.
Implication
These findings have implications for patient and family care and future research. The results underscore the necessity for healthcare providers to acknowledge the importance of FCs’ resilience, CB and QoL. These factors are intricately linked to the Quality of Care received by stroke survivors, which in turn, influences the psychological well-being of the patients. First, nurses should be sensitive to the burden experienced by FCs, including the burden of care, social obligations, responsibilities, advocacy, feelings of ambivalence, guilt, and the challenges associated with acceptance. Second, nurses must consider the resilience of FCs to alleviate their burden. Being resilient means becoming active, maintaining a positive perspective of life, and living for the moment. Enhancing resilience through tailored nursing interventions among FCs can serve as a psychological adaptation, enabling FCs to better cope with the demands of caregiving. Additionally, addressing the palliative care needs of patients and families throughout the course of illness can enhance existing care practices and improve the QoL of stroke survivors, their families, and particularly the FCs.Citation39 Given the pivotal role of resilience in the context of caregiving for stroke survivors, there is a compelling case for the development of nursing intervention studies focused on bolstering resilience among FCs. Such research could contribute to alleviating the burden and enhancing the QoL for both caregivers and patients.
Conclusion
Resilience exhibits a mediating effect on the correlation between CB and QoL of FCs among stroke survivors. The implementation of resilience-interventions within palliative care settings has the potential to significantly reduce the CB and enhance the QoL for these caregivers.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We are grateful to all participants who participated in the study.
Additional information
Funding
References
- American Heart Association. Heart disease and stroke statistics update fact sheet at a glance. American Heart Association. 2021. Available from: https://www.heart.org/-/media/phd-files-2/science-news/2/2021-heart-and-stroke-stat-update/2021_heart_disease_and_stroke_statistics_update_fact_sheet_at_a_glance.pdf?la=en. Accessed June 17, 2024.
- Yanti ADL, Santik YDP. Risk factors associated with disability among elderly with stroke in Indonesia: a secondary data analysis of 2018 national basic health research. J Public Heal Trop Coast Reg. 2022;5(3):140–154. doi:10.14710/jphtcr.v5i3.15694
- Lima RJ, Rosa C, Neyla K, Macedo DF. Resilience, functional capacity, and social support of people with stroke sequelae. Rev Eletr Enferm. 2020;22(59542):1–8.
- Eriksson GM, Kamwesiga JT, Guidetti S. The everyday life situation of caregivers to family members who have had a stroke and received the rehabilitation intervention in Uganda. Arch Public Health. 2021;79(1):1–10. doi:10.1186/s13690-021-00618-z
- Achilike S, Beauchamp JES, Cron SG, et al. Caregiver burden and associated factors among informal caregivers of stroke survivors. J Neurosci Nurs. 2020;52(6):277–283. doi:10.1097/JNN.0000000000000552
- Freytes IM, Sullivan M, Schmitzberger M, et al. Types of stroke-related deficits and their impact on family caregiver’s depressive symptoms, burden, and quality of life. Disabil Health J. 2021;14(2):101019. doi:10.1016/j.dhjo.2020.101019
- Liu Z, Heffernan C, Tan J. Caregiver burden: a concept analysis. Int J Nurs Sci. 2020;7(4):438–445. doi:10.1016/j.ijnss.2020.07.012
- de-Torres García I, Bustos F, Arango-Lasprilla JC, Fernández-Berrocal P. Emotional intelligence abilities of caregivers of patients with acquired brain injury and cognitive impairment: are they related to overload or resilience? Ansiedad y Estres. 2021;28(1):55–61. doi:10.5093/anyes2022a6
- Palacio GC, Krikorian A, Gómez-Romero MJ, Limonero JT. Resilience in caregivers: a systematic review. Am J Hosp Palliat Med. 2020;37(8):648–658. doi:10.1177/1049909119893977
- Inci FH, Temel AB. The effect of the support program on the resilience of female family caregivers of stroke patients: randomized controlled trial. Appl Nurs Res. 2016;32:233–240. doi:10.1016/j.apnr.2016.08.002
- Walsh F. Family Resilience: a Dynamic Systemic Framework. In: Ungar M, editor. Multisystemic Resilience. Oxford University Press; 2021:255–270.
- Chan ACY, Piehler TF, Gwk H. Resilience and mental health during the COVID-19 pandemic: findings from Minnesota and Hong Kong. J Affect Disord. 2021;295:771–780. doi:10.1016/j.jad.2021.08.144
- Aparicio M, Centeno C, Carrasco JM, Barbosa A, Arantzamendi M. What are families most grateful for after receiving palliative care? Content analysis of written documents received: a chance to improve the quality of care. BMC Palliat Care. 2017;16(1):1–11. doi:10.1186/s12904-017-0229-5
- Steigleder T, Kollmar R, Ostgathe C. Palliative Care for Stroke Patients and Their Families: barriers for Implementation. Front Neurol. 2019;10:1–8. doi:10.3389/fneur.2019.00164
- Karimirad MR, Seyedfatemi N, Noghani F, Dehkordi AH, Barasteh S. The relationship between resilience and quality of life in family caregivers of patients with mental disorders. J Clin Diagn Res. 2018;12:11. doi:10.7860/JCDR/2018/29369.12239
- Masoudian N, Sarmadi M, Najafi R, Najafi F, Maleki S. Burden of care and quality of life in home caregivers of patients with stroke in Iran. Home Health Care Manag Pract. 2019;31(4):213–218. doi:10.1177/1084822319843137
- Uzar-Ozçetin YS, Dursun Sİ. Quality of life, caregiver burden, and resilience among the family caregivers of cancer survivors. Eur J Oncol Nurs. 2020;48. doi:10.1016/j.ejon.2020.101832
- Fang L, Dong M, Fang W, Zheng J. Relationships between care burden, resilience, and depressive symptoms among the main family caregivers of stroke patients: a cross-sectional study. Front Psychiatry. 2022;13(3). doi:10.3389/fpsyt.2022.960830
- Connor KM, Davidson JRT. Development of a new Resilience scale: the Connor-Davidson Resilience scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
- Kobasa SC. Stressful life events, personality, and health: an inquiry into hardiness. J Pers Soc Psychol. 1979;37(1):1–11. doi:10.1007/BF00263951
- Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
- Elmståhl S, Malmberg B, Annerstedt L. Caregiver’s burden of patients 3 years after stroke assessed by a novel caregiver burden scale. Arch Phys Med Rehabil. 1996;77(2):177–182. doi:10.1016/S0003-9993(96)90164-1
- World Health Organization. The World Health Organization Quality of Life (WHOQOL)- BREF Edisi Bahasa Indonesia. Program Mental Health. 2004:1–5. Available from: 10.1023/B:QURE.0000018486.91360.00. Accessed June 17, 2024.
- Resmiya L, Misbach IH. Development tool of quality of life in Indonesia (Pengembangan Alat Ukur Kualitas Hidup Indonesia). J Ilm Pendidik Lingkung Dan Pembang. 2016;17(01):34–41. doi:10.21009/plpb.171.04
- Rusti S, Helda H, Ronoatmodjo S, Sunarti E, Latifah MM, Andreas AM. Determinants of family resilience in ischemic stroke patients. Open Access Maced J Med Sci. 2022;10:1246–1251. doi:10.3889/oamjms.2022.9783
- Zhang W, Zhou W, Ye M, Gao Y, Zhou L. Family resilience of stroke survivors within 6 months after a first-episode stroke: a longitudinal study. Front Psychiatry. 2022;13. doi:10.3389/fpsyt.2022.968933
- Asti AD, Novariananda S, Sumarsih T. Caregiver burden and stress among stoke patients (beban caregiver dan stres keluarga pasien stroke). J Ilm Kesehat Keperawatan. 2021;17(2):157. doi:10.26753/jikk.v17i2.667
- Caro CC, Costa JD, Da Cruz DMC. Burden and quality of life of family caregivers of stroke patients. Occup Ther Heal Care. 2018;32(2):154–171. doi:10.1080/07380577.2018.1449046
- Ba MS, Monkong S, Leelacharas S, Satitvipawee P. Factors explaining quality of life among family caregivers of people with stroke in Myanmar: a cross-sectional study. Pacific Rim Int J Nurs Res. 2022;26(2):355–369.
- Kumar R, Kaur S. Predictors of quality of life and its impact on coping styles in stroke caregivers. J Neurol Disord. 2017;05(02):2–5. doi:10.4172/2329-6895.1000336
- Weisser FB, Bristowe K, Jackson D. Experiences of burden, needs, rewards and resilience in family caregivers of people living with motor neuron disease/amyotrophic lateral sclerosis: a secondary thematic analysis of qualitative interviews. Palliat Med. 2015;29(8):737–745. doi:10.1177/0269216315575851
- Meyers EE, McCurley J, Lester E, Jacobo M, Rosand J, Vranceanu AM. Building resiliency in dyads of patients admitted to the neuroscience intensive care unit and their family caregivers: lessons learned from William and Laura. Cogn Behav Pract. 2020;27(3):321–335. doi:10.1016/j.cbpra.2020.02.001
- Gómez-Trinidad MN, Chimpén-López CA, Rodríguez-Santos L, Moral MA, Rodríguez-Mansilla J. Resilience, emotional intelligence, and occupational performance in family members who are the caretakers of patients with dementia in Spain: a cross-sectional, analytical, and descriptive study. J Clin Med. 2021;10(18):1–18. doi:10.3390/jcm10184262
- Herdiana I, Suryanto D, Handoyo S. Family resilience: a conceptual review. Adv Soc Sci Educ Humanit Res. 2018;133(1984):42–48. doi:10.2991/acpch-17.2018.9
- Efi P, Fani K, Eleni T, et al. Quality of life and psychological distress of caregivers of stroke people. Acta Neurol Taiwan. 2017;26(4):154–166.
- Tsai YH, Lou MF, Feng TH, Chu TL, Chen YJ, Liu HE. Mediating effects of burden on quality of life for caregivers of first-time stroke patients discharged from the hospital within one year. BMC Neurol. 2018;18(1):1–9. doi:10.1186/s12883-018-1057-9
- Oh S, Chang SJ. Concept analysis: family resilience. Open J Nurs. 2014;04(13):980–990. doi:10.4236/ojn.2014.413105
- Simpson G, Jones K. How important is resilience among family members supporting relatives with traumatic brain injury or spinal cord injury? Clin Rehabil. 2013;27(4):367–377. doi:10.1177/0269215512457961
- Holloway RG, Arnold RM, Creutzfeldt CJ, et al. Palliative and end-of-life care in stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45:1887–1916. doi:10.1161/STR.0000000000000015