
Abstract
Purpose
Emerging evidence shows that positive airway pressure (PAP) treatment of obstructive sleep apnea (OSA) and upper airway resistance syndrome (UARS) in chronic insomnia patients (proposed “complex insomnia” disorder) leads to substantial decreases in insomnia severity. Although continuous PAP (CPAP) is the pressure mode most widely researched, intolerance to fixed pressurized air is rarely investigated or described in comorbidity patients. This retrospective study examined dual pressure, autoadjusting PAP modes in chronic, complex insomnia disorder patients.
Patients and methods
Chronic insomnia disorder patients (mean [SD] insomnia severity index [ISI] =19.11 [3.34]) objectively diagnosed with OSA or UARS and using either autobilevel PAP device or adaptive servoventilation (ASV) device after failing CPAP therapy (frequently due to intolerance to pressurized air, poor outcomes, or emergence of CSA) were divided into PAP users (≥20 h/wk) and partial users (<20 h/wk) for comparison. Subjective and objective baseline and follow-up measures were analyzed.
Results
Of the 302 complex insomnia patients, PAP users (n=246) averaged 6.10 (1.78) nightly hours and 42.71 (12.48) weekly hours and partial users (n=56) averaged 1.67 (0.76) nightly hours and 11.70 (5.31) weekly hours. For mean (SD) decreases in total ISI scores, a significant (group × time) interaction was observed (F[1,300]=13.566; P<0.0001) with PAP users (–7.59 [5.92]; d=1.63) showing superior results to partial users (−4.34 [6.13]; d=0.81). Anecdotally, patients reported better tolerability with advanced PAP compared to previous experience with CPAP. Both adaptive servoventilation and autobilevel PAP showed similar ISI score improvement without statistical differences between devices. Total weekly hours of PAP use correlated inversely with change in insomnia symptoms (r=−0.256, P<0.01).
Conclusion
Insomnia severity significantly decreased in patients using autoadjusting PAP devices, but the study design restricts interpretation to an association. Future research must elucidate the interaction between insomnia and OSA/UARS as well as the adverse influence of pressure intolerance on PAP adaptation in complex insomnia patients. Randomized controlled studies must determine whether advanced PAP modes provide benefits over standard CPAP modes in these comorbidity patients.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Chronic insomnia is noted to be the “most prevalent sleep disorder worldwide”.Citation1 Extensive research has evaluated the etiology and assessment of insomnia,Citation2–Citation7 economic impact,Citation1,Citation5,Citation8,Citation9 and evidence-based pharmacological and nonpharmacological treatments.Citation1,Citation5,Citation6,Citation9–Citation11 Yet, according to Edinger et alCitation12 “[t]he optimal insomnia nosology has yet to be determined.” In a recent prospective, validation study, the constructs of “insomnia due to [various conditions] and obstructive sleep apnea were well supported”.Citation12 Surprisingly, only a small corpus of research has investigated the relationships between obstructive sleep apnea (OSA) or upper airway resistance syndrome (UARS) and insomnia.Citation13–Citation17 In the earliest works, Guilleminault et alCitation18,Citation19 showed a link between central sleep apnea and insomnia. More than 20 years later, Lichstein et alCitation20 demonstrated an OSA rate of 43% in older insomnia patients; and in 2001, we proposed the term “complex insomnia” to categorize the comorbidity between chronic insomnia and OSA or UARS, after the unexpected discovery of a 90% rate of objectively diagnosed sleep breathing disorders in a consecutive series of crime victims seeking treatment for insomnia and nightmares.Citation21
From other clinical perspectives, several research groups have demonstrated that 30–60% of OSA patients present with clinically meaningful comorbid insomnia symptoms.Citation17,Citation22–Citation25 In a recent study among a large sample of chronic insomnia disorder patients regularly using yet failing prescription or over-the-counter sleep aids, 91% were objectively diagnosed with OSA or UARS.Citation26 Nasal cannula pressure transducer technology appears to yield the most accurate rates of complex insomnia in the samples studied.Citation27
Much as these findings are thought-provoking; a series of commentaries on causal relationships between insomnia and sleep-disordered breathing have been especially provocative by raising questions about a potential bidirectional relationship between insomnia and sleep breathing disorders.Citation28–Citation31 And, each of these published viewpoints noted a likely requirement for multimodal, evidence-based treatments to address this unusual comorbidity, that is, treatment of insomnia symptoms may require cognitive behavioral therapy for insomnia (CBT-I) or sedatives as well as positive airway pressure (PAP) therapy.Citation28,Citation29,Citation31
Nine studies conducted since 2000 evaluated the effects of sleep-disordered breathing treatments on chronic insomnia ().Citation32–Citation40 All studies, despite weaknesses of retrospective designs in the majority, systematically demonstrated clear-cut improvements following the use of PAP, upper airway surgery, bariatric surgery, or nasal dilator strips.Citation32–Citation40 One of the 9 studies looked at PAP therapy sequentially applied after CBT-I.Citation37 In another study, a small sample of insomnia patients (n=56) who previously failed and then ceased the use of standard forms of continuous PAP (CPAP) therapy were subsequently titrated with adaptive servoventilation (ASV), after which 75% of them reinitiated PAP with this advanced technology.Citation39 Among the 39 ASV users, large decreases in the insomnia severity index (ISI)Citation2 were noted (16.8 vs 9.7; P=0.001; d=1.40) after an average of 1.3 years of ASV use.Citation39
Table 1 Prior research investigations on the impact of sleep-disordered breathing treatments on chronic insomnia severityTable Footnotea
A distinctive observation in this ASV study pinpointed the ubiquitous inability of chronic insomnia disorder patients with comorbid OSA/UARS to adapt to standard PAP devices, such as continuous positive airway pressure (CPAP), continuous positive airway pressure with expiratory pressure relief (CFLEX), automatic continuous positive airway pressure (APAP), and Bilevel positive airway pressure (BPAP) due to self-reported discomfort and intolerance triggered by the vaguely defined phenomenon of expiratory pressure intolerance (EPI)Citation41,Citation42 even among those using PAP devices with basic expiratory pressure relief (EPR) systems.Citation39 These adverse effects resolved with ASV use,Citation43 and in our clinical experience, many insomnia patients also adapt well to autobilevel PAP (ABPAP) devices.Citation43,Citation44 Anecdotally, manually titrated, autoadjusting algorithms embedded in these devices create a smoother airflow delivery system, which in turn diminishes insomnia patients’ anxious responses to pressurized air.Citation43,Citation44 These findings are consistent with prior research showing the inadequacy of exclusive reliance on autotitrating algorithms in these devices,Citation45 despite their known ambulatory rescue capabilities.Citation46,Citation47
To examine the effects of manually titrated, dual-pressure, autoadjusting technologies on insomnia outcomes, we conducted a retrospective chart review on a nonrandomized controlled cohort of chronic insomnia patients who presented with moderate-to-severe symptoms and comorbid OSA/UARS. All patients were currently using advanced PAP technology. We hypothesized:
Regular users of advanced PAP devices would demonstrate greater decreases in insomnia severity compared to a control group of partial users;
Increased hours of use of advanced PAP technology would correlate inversely with change in insomnia severity.
Patients and methods
Study criteria and consent
Adult patients who met the following criteria were included: 1) ISI ≥15; 2) subjective report of multiple indicators of psychophysiological insomnia, poor sleep hygiene or psychiatric comorbidity as the most likely causes of insomnia; 3) objectively diagnosed OSA (apnea–hypopnea index [AHI] ≥5) or UARS (AHI <5 and respiratory disturbance index ≥15); 4) failed standard forms of PAP therapy (see “Procedure for CPAP failure determination” section for detailed explanation) at Maimonides Sleep Arts & Sciences (MSAS) or at a previous sleep facility; 5) completed one or more in-lab manual titrations with autoadjusting technology; 6) filled a prescription, initiated and maintained the use of ABPAP or ASV, and returned for follow-up; and 7) provided subjective and objective follow-up measures at clinic appointments. As per standard protocol at MSAS, all patients provided verbal and written consents for their medical information to be used anonymously for research and educational purposes in the context of chart and data reviews. This study was approved by Los Alamos Medical Center’s Institutional Review Board.
Chart review and extracted sample
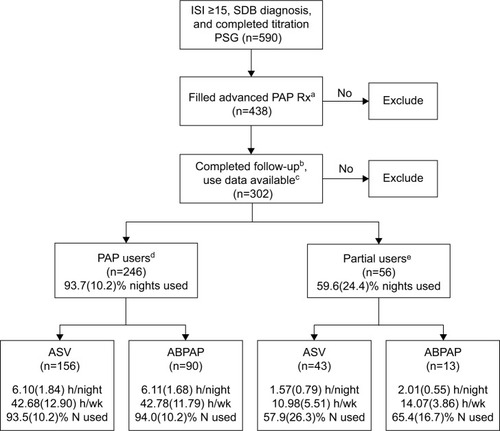
This retrospective chart review commenced with all patients seen at MSAS between March 2011 and August 2014 (n=1,967). Adult patients were included who presented with intake ISI scores ≥15, diagnosed with OSA or UARS, and underwent a titration polysomnography (PSG). Of the 590 eligible patients, 438 patients filled prescriptions for ABPAP or ASV, of whom 302 patients provided follow-up outcome measures (ISI and Epworth Sleepiness Scale [ESS]) and objective data downloads (ODD) on average 6.9 months from the initiation of therapy ().
Figure 1 Flowchart of inclusion criteria and group definition.
Abbreviations: ABPAP, autobilevel positive airway pressure; ASV, adaptive servoventilation; ESS, Epworth Sleepiness Scale; h, hours; ISI, insomnia severity index; N, nights; PAP, positive airway pressure; PSG, polysomnography; Rx, prescription; SDB, sleep disordered breathing; wk, week.
Procedure for CPAP failure determination
In our clinical experience in working with predominantly psychiatric patients with sleep disorders, we observed frequent problems with EPI triggered by fixed pressurized airflow devices,Citation39,Citation43,Citation44 and this phenomenon often heralds “claustrophobic tendencies” in relationship to or irrespective of mask issues.Citation48–Citation50 Since 2005, our policies and procedures focused on preventing or eliminating EPI and related claustrophobic tendencies in vulnerable patients with co-occurring insomnia and psychiatric conditions (Supplementary materials).Citation39,Citation44,Citation51–Citation55 As noted in , main pathways ultimately led to CPAP failure in this study cohort, and subjective and objective EPI were the most common problems, necessitating a switch to advanced PAP devices. Overall, taking into account patients’ efforts to attempt multiple modes of PAP, the average patient experienced multiple (~5 per patient) reasons for failure.
Figure 2 Timing of subjective and objective PAP mode failure.a
Abbreviations: ABPAP, autobilevel positive airway pressure; AHI, apnea–hypopnea index; BPAP, Bilevel PAP; CAI, Central Apnea Index; CPAP, continuous positive airway pressure; CSA, central sleep apnea; EPI, expiratory pressure intolerance; MSAS, Maimonides Sleep Arts & Sciences; OSA, obstructive sleep apnea; PAP, positive airway pressure; PSG, polysomnography; SA, sleep apnea; SDB, sleep disordered breathing; UARS, upper airway resistance syndrome.
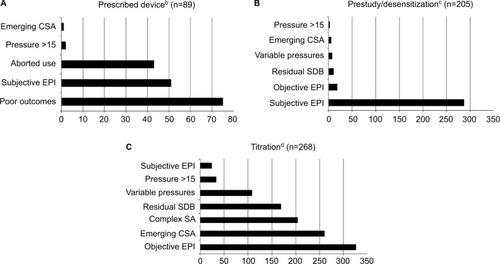
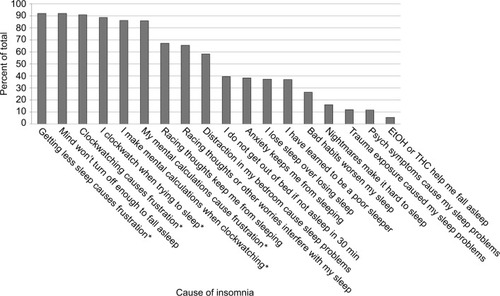
Figure 3 Subjective symptoms for psychophysiological conditions and poor sleep hygiene reported at intake.a
Abbreviations: EtOH, alcohol; THC, marijuana TMB-10, Time Monitoring Behavior questionnaire.
Of the 89 patients prescribed PAP devices to use at home, failure was mainly due to poor outcomes (persistently elevated ISI, fatigue, or daytime symptoms despite PAP therapy use), subjective EPI, and aborted use (). For 205 patients during their prestudy PAP desensitization, subjective expiratory intolerance was the main reason for traditional PAP mode failures (). For 268 patients undergoing a sleep technologist conducted titration, PAP failure was largely due to objectively observed EPI, emergent central-like pause(s), complex sleep apnea (CompSA), and residual sleep breathing events persisting despite pressure increases (). A total of 1,625 specific indications of failure manifested with various PAP modes for these 302 patients, which eventually led to insurance coverage for the use of autoadjusting PAP technology.
PSG and titration practice model for autoadjusting technology
PSG was conducted and scored with American Academy of Sleep Medicine (AASM) guidelines to diagnose OSA/UARS.Citation56 For titrations, our policies and procedures align with AASM guidelinesCitation41 and other researchCitation57 to normalize the airflow curve by eliminating all breathing events including respiratory effort-related arousals (RERAs).Citation41,Citation57 We also follow 2006 AASM practice parameters for BPAP indications “[…]where high pressure is needed and the patient experiences difficulty exhaling against a fixed pressure[….]” This adverse EPI effect (described earlier for CPAP failure) occurs while increasing the pressure to resolve RERAs, especially for patients on fixed CPAP. Subjective or objective EPI manifests in patients with anxiety symptoms (an omnipresent insomnia finding). When manually titrating advanced technology in the sleep laboratory, a fine-tuning process permits minute increases in inspiratory pressures to treat RERAs while simultaneously providing concomitant pressure relief through fastidious titration of expiratory pressures. Thus, the synergistic goals of normalized airflow and patient comfort are achieved.Citation39,Citation47
A sequential changing of pressure delivery modes follows an algorithm that begins with CPAP, which then moves to either CPAP or APAP with an EPR setting or to BPAP, followed by ABPAP and finally ASV when CompSA or in some cases subthreshold CompSA develops. To eliminate RERAs without aggravating EPI, pressures are titrated by 0.2–0.4 cm/H2O increments.Citation39,Citation47
Advanced PAP technology prescription practices
Using the above algorithm in the manual titration of autoadjusting dual-pressure devices has resulted in the vast majority of complex insomnia patients ultimately receiving a prescription for either an ABPAP device or an ASV device at our center, which specializes in the treatment of complex patients suffering psychiatric comorbidities. Thus, a minority of patients used standard CPAP devices at home. Some used APAP or BPAP devices for varying periods of time before returning to the sleep center with the complaint of poor to mediocre results, at which point a repeat titration was conducted, and ABPAP or ASV was prescribed as qualified by insurance criteria.Citation47
Subjective and objective determinations of hours of PAP use
Hours of PAP use and percentage of nights used (nights with PAP use divided by total number of nights) were determined by ODD. Rarely (<10% of sample), ODDs were not available due to computer or software malfunction. In these instances, subjective report for hours of PAP use was determined by patient report on bed time, wake time, time of mask removal, estimated nightly PAP use, and corroboration with bed partner. ODD was available for 275 patients (ASV =177; ABPAP =98), and personal estimates of nightly use were obtained in 27 patients (ASV =22; ABPAP =5).
Nonrandom assignment divided patients into the following 2 groups: PAP users (n=246; ≥20 h/wk, averaging 6.10 [1.78] h/night and 42.71 [12.48] h/wk) and partial users (n=56; <20 h/wk, averaging 1.67 [0.76] h/night and 11.70 [5.31] h/wk). The cutoff value of 20 h/wk was calculated based on CMS compliance standards of 70% of nights with ≥4 h per night use (ie, 4.9 nights ≥4 h =19.6 h/wk).
Additional metrics
Intake and follow-up scores for ISI questions # 1–3 were analyzed individually to examine changes in the type of insomnia: sleep onset insomnia (SOI), sleep maintenance insomnia (SMI), and early morning awakening (EMA). To further identify insomnia severity, subjective sleep indices (time in bed, total sleep time, sleep onset latency, and wake after sleep onset) were reported at intake; sleep efficiency was calculated from these responses. As an additional measure of change in insomnia, frequency of sleep aid use was gathered at intake and clarified at follow-up. Psychiatric history (including trauma history and claustrophobia) was obtained at intake to identify comorbid disorders. To evaluate the presence of comorbid sleep disorders, patients treating periodic limb movement disorder or restless leg syndrome were identified at the time of most recent follow-up.
Data analyses
Descriptive statistics provided baseline characteristics, including sociodemographics and standard self-report sleep metrics and hours of objective use of PAP therapy. Analysis of variance (ANOVA) compared use means among groups. PAP user and partial user groups, as well as ASV and ABPAP groups, were compared for changes in insomnia severity with repeated measures ANOVA, including within- and between-subjects analyses while controlling for subjective psychiatric comorbidities. Pearson product-moment correlations were conducted on hours of use by change in insomnia symptom severity. Cohen’s d measured within-subjects effect sizes, and Hedge’s g measured between-subjects effect sizes due to unequal sample sizes. Statistical significance was 0.05. All continuous variables were expressed as mean (SD).
Results
Baseline characteristics
Our study sample was predominantly overweight (body mass index =31.59 [8.00]), Caucasian (61.9%) or Hispanic (28.1%), married or living with partner (67.2%), males (55.6%) with a bachelor’s degree or higher (48.0%), and age 53.44 (14.21) years. OSA was diagnosed in 274 and UARS in 28 patients. ESS total score was 10.89 (6.02), just above the most conservative cutoff for clinically meaningful daytime sleepiness (). For 246 PAP users, 156 used ASV and 90 used ABPAP, and for 56 partial users, 43 used ASV and 13 used ABPAP ().
Table 2 Sociodemographics, psychiatric history, and baseline subjective sleep and objective respiratory indices for PAP users vs partial usersTable Footnotea
Subjective intake data were consistent with chronic insomnia in the moderate-to-severe range (ISI score =19.11 [3.34]) with an insomnia chronicity of 10.28 (7.33) years. identifies indicators of psychophysiological conditioning and poor sleep hygiene, which patients directly attributed to their insomnia, such as learning to be a poor sleeper, losing sleep over losing sleep, and time monitoring behavior. Patients endorsed an average of 9.48 (3.68) of a possible 18 indicators for maladaptive sleep behaviors. Medical co-morbidities were reported in 96.7% of all patients (, see Supplementary Results for details of system categories). Three-quarters (75.2%) of all patients reported at least one psychiatric condition or disorder ().
Hours of use by objective data or subjective report by PAP mode
Nightly and weekly hours of use were nearly identical for ASV users (6.10 [1.84], 42.68 [12.90]) and ABPAP users (6.11 [1.68], 42.78 [11.79]). Nightly hours for ASV and ABPAP partial users (1.57 [0.79] vs 2.01 [0.55]; P=0.067, g=0.58) and weekly hours (10.98 [5.51] vs 14.07 [3.86]; P=0.065, g=0.59) were not significantly different, albeit the effect sizes indicated that ABPAP use was moderately greater than ASV use. There was a significant difference in the percentage of nights used between PAP users and partial users (93.7 [10.2] vs 59.6 [24.4]; P=0.001, g=2.44); no difference was found between modes among PAP users (93.5 [10.2] vs 94.0 [10.2]; P=0.7, g=0.05) or partial users (57.9 [26.3] vs 65.4 [16.7]; P=0.3, g=0.27) for ASV vs ABPAP respectively ().
Changes in insomnia severity
For decreases in total ISI scores, a significant (group × time) interaction was observed (F[1,288]=13.895; P<0.0001) with PAP users (−7.59 [5.92]; d=1.63) showing superior results compared to partial users (−4.34 [6.13]; d=0.81). Clinical severity decreased markedly in the PAP user group to below the currently applied clinical cutoff of 15, equivalent to less than a moderate level of insomnia (11.43 [5.73]), whereas partial users remained above the moderate level of severity (15.18 [6.60]) ().
Figure 4 Within-group comparison of mean (SD) intake vs follow-up ISI values for (A) Total sample (n=302), (B) ASV sample (n=199), and (C) ABPAP sample (n=103).
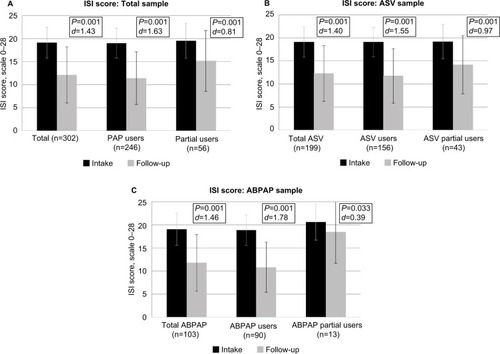
Within PAP users, ISI scores significantly decreased for both the ASV (n=156; −7.32 [5.98]; d=1.55; ), and ABPAP groups (n=90; −8.02 [5.83]; d=1.78; ) without significant differences between PAP modes (P=0.59).
In partial users, ISI scores significantly decreased for the ASV group (n=43; −5.00 [6.19]; d=0.97; ), but ISI decrease among ABPAP users was not significant (n=13; −2.15 [5.63]; P=0.33; d=0.39; ), albeit without differences between groups (P=0.24; g=0.46).
To provide a more clinically relevant view of the changes in insomnia severity, we measured the following 2 ISI clinical cutoffs: subclinical insomnia (<11) and nonclinical insomnia (<8). There was a significant difference in PAP users vs partial users attaining subclinical ISI scores (112 [45.5%] vs 15 [26.8%], P=0.01). Nonclinical ISI scores were attained in 59 (24.0%) PAP users and 9(16.1%) partial users, with no significant difference between the groups, P=0.20.
Examining individual insomnia subtype scores (SOI, SMI, and EMA) at intake revealed no significant differences between PAP users and partial users. Follow-up scores for each of the 3 insomnia subtypes showed significant improvement in the PAP users (n=243) with large effect sizes, whereas partial users’ (n=56) improvements were non-significant with small-to-medium effect sizes (). Mean improvements were as follows in the PAP user group: SOI (-0.76 [1.14]; d=0.70), SMI (−0.86 [1.19]; d=0.87), and EMA (−0.74 [1.43]; d=0.65).
Figure 5 Within-group comparison of mean intake vs follow-up valuesa for 299b patients on the following 3 ISI questions: SOI, SMI, and EMA.
Abbreviations: ABPAP, autobilevel positive airway pressure; ASV, adaptive servoventilation; EMA, early morning awakenings; ISI, insomnia severity index; PAP, positive airway pressure; SMI, sleep maintenance insomnia; SOI, sleep onset insomnia.
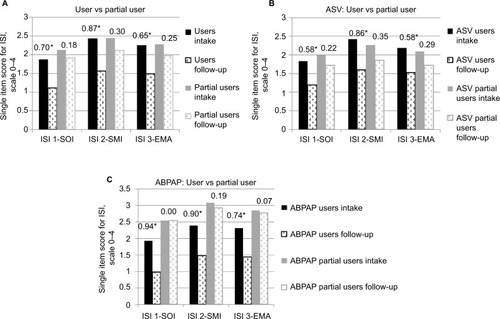
Within ASV subjects, users’ (n=154) ISI subtype scores significantly decreased as follows: SOI (−0.64 [1.14]; d=0.58), SMI (−0.83 [1.20]; d=0.86), and EMA (−0.67 [1.33]; d=0.58) (). And, within ABPAP subjects, users’ (n=89) insomnia subtype scores significantly decreased as follows: SOI (−0.96 [1.13]; d=0.94), SMI (−0.90 [1.17]; d=0.90), and EMA (−0.88 [1.58]; d=0.74) ().
Of the 302 total patients, 135 reported taking prescription or over-the-counter medications for insomnia at intake (108 PAP users [ASV 74 and ABPAP 34] and 28 partial users [ASV 20 and ABPAP 8]) ( for the list of medications). At follow-up, 80 of the 135 sleep aid users reported no change in insomnia medication, whereas 40 reported a decrease in medication, including 33 PAP users (ASV 23 and ABPAP 10) and 7 partial users (ASV 3 and ABPAP 4). An additional 3 patients reported an increase in medication (ASV users 3).
Numerous significant changes also occurred with day-time sleepiness outcomes (ESS), but effects were small (Supplementary materials). There was a significantly greater proportion of PAP users treating leg jerks compared to partial users. However, when comparing change in ISI score for PAP users vs partial users treating leg jerks, no significant difference was found (Supplementary materials). Controlling for psychiatric history also did not affect results.
Correlations between hours of use and change in insomnia severity
When analyzing all 302 patients, total weekly hours of PAP use correlated inversely with change in insomnia symptoms (r=−0.256, P<0.01). Looking at each mode individually, insomnia symptoms decreased with total weekly hours of PAP use for all ASV patients (n=199, P=0.001, r=−0.235) and for all ABPAP patients (n=103, P=0.002, r=−0.299), suggesting potential efficacy in both groups. The difference between the 2 correlations was not significant (z=0.56, P=0.58).
Discussion
In a medium-size clinical sample of OSA/UARS patients diagnosed with comorbid, moderate-to-severe insomnia symptoms (the proposed complex insomnia designation),Citation21 large improvements manifested in association with the use of manually titrated, autoadjusting PAP technology. Correlations between hours of use with either ASV or ABPAP and improvements in insomnia were highly significant. Taken together, the findings appear to support the emerging theory on OSA/UARS as a causative factor in insomnia pathophysiology, albeit in the absence of a randomized controlled prospective trial, the results of this case series of clinical patients can only be described as an association between sleep-disordered breathing and insomnia symptoms. However, from an anecdotal perspective, it seemed clear that these advanced devices proved especially well-suited for relieving the problem of EPI among vulnerable insomnia patients suffering from generalized distress or specific anxiety about using PAP therapy.
Future studies must use more rigorous protocols to evaluate the relationships between these 2 most common sleep disorders. Although a small number of studies have already been conducted (), new protocols are needed with various evidence-based forms of therapy for OSA/UARS, including different PAP therapy modes, oral appliances, upper airway surgery, and even weight loss treatments. Based on this study and that of past research, newer studies must quantify more precisely the extent to which the treatment of sleep breathing problems improves insomnia symptoms as well as the extent of residual insomnia symptoms. Programs with combination therapies including PAP and CBT-I or PAP and sedatives are likely to provide the most clinical relevance and generalizability, given the high proportion of insomnia disorder patients who would benefit optimally from both treatments instead of just one. Urgent research is warranted to examine PAP vs CBT-I, PAP vs PAP/CBT-I, and finally PAP/CBT-I vs CBT-I, because of the growing demand for nonpharmacological treatment of insomniaCitation11,Citation28,Citation58 as well as the rising need to increase access for evidence-based insomnia interventions through on-line therapies.Citation58,Citation59 Results should attempt to rapidly clarify how best to implement these treatment regimens in clinical and non-clinical settings.
To assist in the development of this new therapeutic framework, we initiated a randomized single-blind, controlled study on the benefits of ASV vs CPAP therapy in chronic insomnia disorder patients (clinical trials # NCT02365064). Also, other clinical and research groups have begun development to treat complex insomnia patients with multimodal therapies,Citation58,Citation60–Citation62 and early results suggest the importance of these approaches.
The study has several limitations due to the nonrandomized, retrospective case series design with a medium-sized sample. Selection bias may have occurred as not all insomnia patients presenting to our center underwent PSG testing or filled their PAP prescriptions. Thus, by focusing only on users of PAP devices, our results provide no information on cost-effectiveness. The cohort reported a wide range of psychiatric comorbidity that may limit generalizability of our findings. Information regarding other factors such as medication changes, other insomnia treatments, and education on sleep hygiene was unavailable for this review. Regardless of the potential therapeutic impact, speculatively PAP may have acted as a relaxation placebo for some patients. Also, this cohort may have been more motivated to pursue treatment, and the results may not translate to insomniacs who did not move forward with diagnostic or treatment steps. Our sleep center focuses on an experiential model of patient education via greater use of hands-on coaching and titrationsCitation47 as well as encouraging struggling patients to reach out rapidly to problem solve. These 2 patient-centric features of our sleep medical center may lead to greater interactions between the patients and our sleep staff and, therefore, might limit the generalizability of our findings for centers that might spend less time with their patients. In addition, ineffective treatment or nontreatment of comorbid sleep disorders could have had an effect on PAP use and, in some cases, insomnia severity. Our data represent an association between advanced PAP technology and observed decreases in insomnia; a prospective, randomized controlled protocol with monitoring of longitudinal progress is needed to confirm or reject these findings in a sample of chronic insomnia patients. In particular, it will prove highly relevant to determine whether or not more advanced PAP technology devices are more suitable for complex insomnia patients.
Conclusion
Improvements in insomnia severity were greater in regular users of autoadjusting PAP devices compared to a nonrandom control group of partial users, and the former group demonstrated average decreases in insomnia below the clinical ISI cutoff for moderate insomnia. Increased hours of autoadjusting PAP use correlated inversely with change in insomnia severity. Autoadjusting PAP devices seemed especially salient for complex insomnia patients, who were prone to anxious tendencies that may have increased vulnerability to EPI and claustrophobic feelings. Speculatively, advanced PAP technology may provide an adaptation advantage for those who might otherwise struggle with traditional PAP therapy devices.Citation39,Citation43,Citation44,Citation47
Acknowledgments
We are grateful to the Los Alamos Medical Center and the Los Alamos Medical Center Sleep Laboratory for administrative and clinical assistance in the completion of this study. This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplementary materials
Methods
Although research and conventional wisdom often allude to a very narrow window (eg, 3–4 d) in which patients may accept or reject positive airway pressure (PAP) therapy,Citation1–Citation3 there does not seem to be a formal policy or protocol on how to act on this information to improve patient compliance. Patients are commonly sent home on continuous PAP (CPAP) with the notion that they will learn to get used to it, notwithstanding their progress by day 4.
In our sleep laboratory, we proactively attempt to trouble-shoot issues that may interfere early in the patient’s adaptation experience.Citation4–Citation8 Our desensitization protocol on the night of the titration seeks extensive patient feedback regarding comfort with both pressurized air and the mask. Instead of presuming that the patient will tolerate pressurized airflow over time, we make the assumption that more discomfort indicates a lesser likelihood for adaptation. Thus, when a patient reports discomfort with mask or pressurized air, we seek to remedy the discomfort during the desensitization or the actual titration. Although, in some cases, the discomfort may be minor and easily fixed by changing a mask size or style, we often encounter more serious complaints with pressurized air that are best defined as claustrophobic tendencies or frank claustrophobic responses.Citation4–Citation8
Our objective is to increase physiological and psychological comforts during the desensitization and titration instead of waiting for discomfort to abort the patient’s effort when using PAP at home. In practical terms, every patient will try CPAP, but in vulnerable insomnia and psychiatric patients, there is usually an immediate, negative response to this mode due to difficulties breathing out against fixed pressurized air. Most patients rapidly report the elimination of this discomfort, accompanied by a new sense of comfort, after switching to a dual-pressure device. Later, while asleep during the titration, we seek to eliminate all respiratory effort-related arousals (RERAs) without provoking further episodes of subjective or objective expiratory pressure intolerance (EPI), and we have found manually titrating patients on autoadjusting dual-pressure devices (adaptive servoventilation [ASV] and autobilevel PAP [ABPAP]) to be well-suited to achieve these results.Citation4,Citation7,Citation8
Last, in applying our protocol to eliminate RERAs as well as EPI, we have also noticed a set of objective markers that tend to correlate with a normalized airflow signal – normal on both inspiration and expiration. Specifically, a normalized airflow signal appears linked to fewer arousals, awakenings, and sleep stage shifts,Citation7,Citation9 as well as a greater degree of sleep efficiency, rapid eye movement (REM) sleep rebound,Citation10 and possibly REM sleep consolidation (uninterrupted periods of REM sleep) as described by Riemann et al.Citation11
Results
Medical comorbidities are reported in . Of the 302 patients, 292 patients reported at least one medical comorbidity with an average of >5 comorbidities per patient. Comorbidities were classified into categories and were defined as: arthritis/pain – arthritis (96), chronic fatigue syndrome (23), chronic pain (85), fibromyalgia (23); cardiac – heart disease (9), myocardial infarction (8), heart failure (2), premature ventricular contractions (8), atrial fibrillation (10), bradycardia (5), tachycardia (13), heart surgery (16), and other heart conditions (17); drug/alcohol abuse – drug addiction (13) and alcoholism (14); endocrine – diabetes (44), menopausal symptoms (51), obesity (111), thyroid problems (59); hypertension (133); kidney – bladder problems (55) and kidney problems (9); neurologic – epilepsy/seizure (10), head injury with concussion (50), head injury without concussion (29), and stroke (6); pulmonary – allergies (177), asthma (54), deviated septum (61), emphysema (3), nasal trauma (16), sinus problems (113), current smoker (18), former smoker (68), and tonsillectomy (69); and reflux (115).
Epworth Sleepiness Scale (ESS) scores for the entire sample decreased by 2.47 (5.14) from 10.89 (6.02) to 8.42 (5.44) (P=0.001; d=0.43). The PAP user group (n=246) showed a significant decrease in ESS scores (mean [SD] =2.60 [5.35]; P=0.001; d=0.46). Among ASV users (n=156), ESS scores significantly decreased (2.93 [5.34]; P=0.001; d=0.50), and among ABPAP users, ESS scores significantly decreased (2.03 [5.35]; P=0.01; d=0.38) without significant differences between PAP pressure modes (P=0.20; g=0.17).
ESS scores did not significantly decrease for the 56 partial users (mean [SD] change =1.91 [4.12]; P=0.10; d=0.31), the 43 ASV partial users (2.05 [4.30]; P=0.13; d=0.33), or the 13 ABPAP partial users (1.46 [3.57]; P=0.55; d=0.23) without significant difference between PAP pressure modes (P=0.66; g=0.14). There was no significant difference between changes in ESS scores among PAP modes (P=0.21; g=0.15), although the changes within each mode were significant: ASV (2.74 [5.13]; P=0.001; d=0.46) and ABPAP (1.96 [5.15]; P=0.01; d=0.36).
There was a significant difference in the proportion of patients treating leg jerks between users and partial users (84/246 [34.1%] vs 10/56 [17.9%]; P=0.017). Similar findings existed within ASV user and partial user groups (58/156 [37.2%] vs 9/43 [20.9%]; P=0.047); among ABPAP patients, there were too few partial user subjects to allow statistical analysis. Among ASV and ABPAP users, there were no significant differences in the proportions of patients treating leg jerks (67/199 [33.7%] vs 27/103 [26.2%]; P=0.19). Change in insomnia severity index score from intake to follow-up for users (19.29 [3.33]–12.06 [5.98]) and partial users (19.40 [3.27]–12.80 [5.31]) treating leg jerks compared to users (18.88 [3.18]–11.10 [5.59]) and partial users (19.54 [3.93]–15.70 [6.79]) not treating leg jerks was not significant (P=0.14).
Table S1 Categorized medications used for insomnia at intake
References
- BudhirajaRParthasarathySDrakeCLEarly CPAP use identifies subsequent adherence to CPAP therapySleep200730332032417425228
- WeaverTEKribbsNBPackAINight-to-night variability in CPAP use over the first three months of treatmentSleep19972042782839231953
- WeaverTEGrunsteinRRAdherence to continuous positive airway pressure therapy: the challenge to effective treatmentProc Am Thorac Soc20085217317818250209
- KrakowBUlibarriVAFoley-SheaMRTidlerAMcIverNDAdherence and subthreshold adherence in sleep apnea subjects receiving positive airway pressure therapy: a retrospective study evaluating differences in adherence versus useRespir Care20166181023103227118876
- KrakowBMelendrezDHaynesPIntegrating psychosocial and biomedical CPAP adherence models. A commentary on: “improving CPAP use by patients with the sleep apnea/hypopnea syndrome (SAHS)” (HM Engleman & MR Wild)Sleep Med Rev20037544144414573379
- KrakowBUlibarriVMelendrezDKiktaSTogamiLHaynesPA daytime, abbreviated cardio-respiratory sleep study (CPT 95807-52) to acclimate insomnia patients with sleep disordered breathing to positive airway pressure (PAP-NAP)J Clin Sleep Med20084321222218595433
- KrakowBUlibarriVASanchezJNKiktaSMcIverNMelendrezDDriving on “auto”: hands-on is more effective than hands-freeJ Clin Sleep Med20128334334422701395
- KrakowBUlibarriVARomeroEAThomasRJMcIverNDAdaptive servo-ventilation therapy in a case series of patients with co-morbid insomnia and sleep apneaJ Sleep Disord Treat Care20132110
- LaffanACaffoBSwihartBJUtility of sleep stage transitions in assessing sleep continuitySleep201033121681168621120130
- KooBBWigginsRMolinaCREM rebound and CPAP complianceSleep Med201213786486822705243
- RiemannDSpiegelhalderKNissenCREM sleep instability – a new pathway for insomnia?Pharmacopsychiatry201245516717622290199
Disclosure
Dr Krakow’s financial disclosures are as follows. He has 6 main activities related to his work in sleep medicine. For websites, he owns and operates the following 6 sites that provide education and offer products and services for sleep disorder patients: www.nightmaretreatment.com, www.ptsdsleepclinic.com, www.sleeptreatment.com, www.sleepdynamictherapy.com, www.soundsleep-soundmind.com, and www.nocturiacures.com. Regarding other professional services, he is the medical director of a National DME company Classic SleepCare® for which his sole functions are consultation and quality assurance. He has neither patient encounters nor does he benefit from the sale of any DME equipment. For intellectual property, he markets and sells the following 3 books for sleep disorder patients: Insomnia Cures, Turning Nightmares into Dreams, and Sound Sleep, Sound Mind. For clinical services, he owns and operates the following commercial sleep center: Maimonides Sleep Arts & Sciences, Ltd. For educational and consulting services, he conducts CME/CEU educational programs for medical and mental health providers to learn about sleep disorders. Sometimes these programs involve the attendee paying a fee directly to our center. Other times, he conducts the workshops at other locations, which may be paid for by vendors such as Respironics and ResMed or other institutions such as the AMEDDC&S, VAMC, and regional sleep center conferences. He is also a president of a nonprofit sleep research center, the Sleep & Human Health Institute (www.shhi.org) that occasionally provides consultation services or receives grants for pilot studies, the most recent of which was ResMed ~$400,000 January 2015 (funding for randomized control trial of PAP treatment in insomnia patients). The authors report no other conflicts of interest in this work.
References
- UnbehaunTSpiegelhalderKHirscherVRiemannDManagement of insomnia: update and new approachesNat Sci Sleep2010212713823616705
- BastienCHVallieresAMorinCMValidation of the insomnia severity index as an outcome measure for insomnia researchSleep Med20012429730711438246
- EdingerJDBonnetMHBootzinRRDerivation of research diagnostic criteria for insomnia: report of an American Academy of Sleep Medicine Work GroupSleep20042781567159615683149
- RichardsonGSHuman physiological models of insomniaSleep Med20078suppl 4S9S1418346677
- RothTIntroduction – advances in our understanding of insomnia and its managementSleep Med20078suppl 3252618032105
- Schutte-RodinSBrochLBuysseDDorseyCSateiaMClinical guideline for the evaluation and management of chronic insomnia in adultsJ Clin Sleep Med20084548750418853708
- RiemannDSpiegelhalderKFeigeBThe hyperarousal model of insomnia: a review of the concept and its evidenceSleep Med Rev2010141193119481481
- BottemanMHealth economics of insomnia therapy: implications for policySleep Med200910suppl 1S22S2519647482
- HussainMTSheaSAWake up to insomnia: future approaches to the management of insomniaNat Sci Sleep20113333523616716
- PigeonWRBishopTMMarcusJAAdvances in the management of insomniaF1000Prime Rep201464824991425
- HarsoraPKessmannJNonpharmacologic management of chronic insomniaAm Fam Physician200979212513019178064
- EdingerJDWyattJKStepanskiEJTesting the reliability and validity of DSM-IV-TR and ICSD-2 insomnia diagnoses. Results of a multitrait-multimethod analysisArch Gen Psychiatry20116810992100221646568
- BenetoAGomez-SiuranaERubio-SanchezPComorbidity between sleep apnea and insomniaSleep Med Rev200913428729319246219
- LaviePInsomnia and sleep-disordered breathingSleep Med20078suppl 4S21S2518346673
- LuysterFSBuysseDJStrolloPJJrComorbid insomnia and obstructive sleep apnea: challenges for clinical practice and researchJ Clin Sleep Med20106219620420411700
- WickwireEMCollopNAInsomnia and sleep-related breathing disordersChest201013761449146320525657
- KrakowBMelendrezDFerreiraEPrevalence of insomnia symptoms in patients with sleep-disordered breathingChest200112061923192911742923
- GuilleminaultCEldridgeFLDementWCInsomnia with sleep apnea: a new syndromeScience197318141028568584353301
- GuilleminaultCEldridgeFLPhillipsJRDementWCTwo occult causes of insomnia and their therapeutic problemsArch Gen Psychiatry1976331012411245971033
- LichsteinKLRiedelBWLesterKWAguillardRNOccult sleep apnea in a recruited sample of older adults with insomniaJ Consult Clin Psychol199967340541010369061
- KrakowBMelendrezDPedersenBComplex insomnia: insomnia and sleep-disordered breathing in a consecutive series of crime victims with nightmares and PTSDBiol Psychiatry2001491194895311377413
- GuilleminaultCPalombiniLPoyaresDChowdhuriSChronic insomnia, postmenopausal women, and sleep disordered breathing: part 1. Frequency of sleep disordered breathing in a cohortJ Psychosom Res200253161161512127179
- KrellSBKapurVKInsomnia complaints in patients evaluated for obstructive sleep apneaSleep Breath20059310411016091954
- HagenCPatelAMcCallWVPrevalence of insomnia symptoms in sleep laboratory patients with and without sleep apneaPsychiatry Res20091702–327627719896722
- SmithSSullivanKHopkinsWDouglasJFrequency of insomnia report in patients with obstructive sleep apnoea hypopnea syndrome (OSAHS)Sleep Med20045544945615341889
- KrakowBUlibarriVAMcIverNDPharmacotherapeutic failure in a large cohort of patients with insomnia presenting to a sleep medicine center and laboratory: subjective pretest predictions and objective diagnosesMayo Clin Proc201489121608162025236429
- KrakowBJUlibarriVAMooreBAMcIverNDPosttraumatic stress disorder and sleep-disordered breathing: a review of comorbidity researchSleep Med Rev201524374525644985
- PigeonWRSateiaMJIs insomnia a breathing disorder?Sleep2012351589159023204600
- LanierWLRamarKSleep medication failure and newly diagnosed obstructive sleep apnea: the role of brain function modulation by muscle afferent activityMayo Clin Proc201489121591159525467642
- CollopNACan’t sleep? You may have sleep apnea!Chest200112061768176911742898
- CollopNI don’t sleep because I can’t breatheSleep Med201314980723746824
- BjornsdottirEJansonCSigurdssonJFSymptoms of insomnia among patients with obstructive sleep apnea before and after two years of positive airway pressure treatmentSleep201336121901190924293765
- GlidewellRNRennBNRobyEOrrWCPredictors and patterns of insomnia symptoms in OSA before and after PAP therapySleep Med201415889990525011662
- GuilleminaultCPalombiniLPoyaresDChowdhuriSChronic insomnia, premenopausal women and sleep disordered breathing: part 2. Comparison of nondrug treatment trials in normal breathing and UARS post menopausal women complaining of chronic insomniaJ Psychosom Res200253161762312127180
- GuilleminaultCDavisKHuynhNTProspective randomized study of patients with insomnia and mild sleep disordered breathingSleep200831111527153319014072
- KrakowBLowryCGermainAA retrospective study on improvements in nightmares and post-traumatic stress disorder following treatment for co-morbid sleep-disordered breathingJ Psychosom Res200049529129811164053
- KrakowBMelendrezDLeeSAWarnerTDClarkJOSklarDRefractory insomnia and sleep-disordered breathing: a pilot studySleep Breath200481152915026935
- KrakowBMelendrezDSisleyBNasal dilator strip therapy for chronic sleep-maintenance insomnia and symptoms of sleep-disordered breathing: a randomized controlled trialSleep Breath2006101162816496118
- KrakowBUlibarriVARomeroEAThomasRJMcIverNDAdaptive servo-ventilation therapy in a case series of patients with co-morbid insomnia and sleep apneaJ Sleep Disord Treat Care20132110
- NguyenXLChaskalovicJRakotonanaharyDFleuryBInsomnia symptoms and CPAP compliance in OSAS patients: a descriptive study using data mining methodsSleep Med201011877778420599419
- KushidaCAChediakABerryRBClinical guidelines for the manual titration of positive airway pressure in patients with obstructive sleep apneaJ Clin Sleep Med20084215717118468315
- RestaOGuidoPPiccaVScarpelliFFoschinoMPThe role of the expiratory phase in obstructive sleep apnoeaRespir Med199993319019510464877
- KrakowBUlibarriVAFoley-SheaMRTidlerAMcIverNDAdherence and subthreshold adherence in sleep apnea subjects receiving positive airway pressure therapy: a retrospective study evaluating differences in adherence versus useRespir Care20166181023103227118876
- KrakowBUlibarriVASanchezJNKiktaSMcIverNMelendrezDDriving on “auto”: hands-on is more effective than hands-freeJ Clin Sleep Med20128334334422701395
- MarroneOInsalacoGSalvaggioABonsignoreGRole of different nocturnal monitorings in the evaluation of CPAP titration by autoCPAP devicesRespir Med200599331332015733507
- GentinaTFortinFDouayBAuto bi-level with pressure relief during exhalation as a rescue therapy for optimally treated obstructive sleep apnoea patients with poor compliance to continuous positive airways pressure therapy--a pilot studySleep Breath2011151212720204535
- KrakowBUlibarriVAMcIverNDReversal of CPAP failure with the REPAP retitration protocolRespir Care2017
- CasasIde la CalzadaMDGuitartMRocaADiagnosis and treatment of the phobia due to treatment with air using nasal continuous pressureRev Neurol200030659359610863736
- ChasensERPackAIMaislinGDingesDFWeaverTEClaustrophobia and adherence to CPAP treatmentWest J Nurs Res200527330732115781905
- EdmondsJCYangHKingTSSawyerDARizzoASawyerAMClaustrophobic tendencies and continuous positive airway pressure therapy non-adherence in adults with obstructive sleep apneaHeart Lung201544210010625744632
- KrakowBMelendrezDWarnerTDDorinRHarperRHollifieldMTo breathe, perchance to sleep: sleep-disordered breathing and chronic insomnia among trauma survivorsSleep Breath20026418920212524572
- KrakowBMelendrezDHaynesPIntegrating psychosocial and biomedical CPAP adherence models. A commentary on: “improving CPAP use by patients with the sleep apnea/hypopnea syndrome (SAHS)” (HM Engleman & MR Wild)Sleep Med Rev20037544144414573379
- KrakowBSound Sleep, Sound Mind: 7 Keys to Sleeping Through the NightNew YorkJohn Wiley & Sons2007
- KrakowBUlibarriVMelendrezDKiktaSTogamiLHaynesPA daytime, abbreviated cardio-respiratory sleep study (CPT 95807-52) to acclimate insomnia patients with sleep disordered breathing to positive airway pressure (PAP-NAP)J Clin Sleep Med20084321222218595433
- KrakowBKrakowJUlibarriVAMcIverNDFrequency and accuracy of “RERA” and “RDI” terms in the Journal of Clinical Sleep Medicine from 2006 through 2012J Clin Sleep Med201410212112424532993
- BerryRBBudhirajaRGottliebDJRules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. deliberations of the sleep apnea definitions Task Force of the American Academy of Sleep MedicineJ Clin Sleep Med20128559761923066376
- CaleroGFarreRBallesterEHernandezLDanielNMontserrat CanalJMPhysiological consequences of prolonged periods of flow limitation in patients with sleep apnea hypopnea syndromeRespir Med2006100581381716388943
- EdingerJDSimmonsBElzKStockSPieCAA pilot test of an online cognitive-behavioral insomnia therapy for patients with comorbid insomnia and sleep apneaSleep201538A236
- AndersonKNGoldsmithPGardinerAA pilot evaluation of an online cognitive behavioral therapy for insomnia disorder – targeted screening and interactive web design lead to improved sleep in a community populationNat Sci Sleep20146434924669197
- CrawfordMRTurnerADWyattJKFoggLFOngJCEvaluating the treatment of obstructive sleep apnea comorbid with insomnia disorder using an incomplete factorial designContemp Clin Trials20154714615226733360
- OngJCCrawfordMRKongAManagement of obstructive sleep apnea and comorbid insomnia: a mixed-methods evaluationBehav Sleep Med118 Epub2015121526619760
- OngJCCrawfordMRInsomnia and obstructive sleep apneaSleep Med Clin20138338939824015117