
Abstract
Purpose
To examine whether parasomnia symptoms are associated with increased odds of childhood asthma and wheeze, and the role of preterm birth.
Patients and Methods
The Shanghai Children’s Allergy Study was cross-sectionally conducted in 31 kindergartens and 17 primary schools in Shanghai, China. After excluding the missing data of gestational week and child’s age, this study included a total of 16,487 individuals with a mean age of 7.74 years and 52.4% of males. The association between parasomnia symptoms and wheeze/asthma was assessed by univariate and multivariate analyses. The interaction effects of parasomnias and preterm birth were primarily evaluated by P for multiplicative interaction, and the relative excess risk due to interaction (RERI), attributable proportion due to interaction (AP), and synergy index (SI) were also measured.
Results
Parasomnias, especially rapid eye movement (REM) parasomnia symptoms, were associated with an increased risk of childhood wheeze/asthma, and the interaction between parasomnia and preterm birth exhibited an excess risk of current wheeze (RERI, 1.43; 95% CI, 0.41–2.45) and ever asthma (RERI, 0.75; 95% CI, 0.01–1.50). In the stratification analyses, the combination of parasomnia symptoms and preterm birth had higher odds of wheeze/asthma. And the odds of current wheeze (OR, 4.55; 95% CI, 1.69–12.25; p=0.003) and ever asthma (OR, 6.17; 95% CI, 2.36–16.11; p<0.001) were much higher in cumulative parasomnia symptoms plus very preterm birth. And sensitive analyses were further conducted in populations without sleep disordered breathing (SDB), and an allergen test subgroup, yielding similar results.
Conclusion
Parasomnia symptoms are associated with increased odds of childhood wheeze/asthma, and the odds were even higher in premature population. The findings suggest that parasomnia symptoms, as a developmental sleep disorder, are supposed to be closely watched among children who have asthma or are at risk for asthma, and that preterm children deserve more attention.
Introduction
Parasomnias, characterized by abnormal movement or partial arousals while sleeping, are one of the most common developmental disorders in children.Citation1 The development and establishment of sleep structures occur during the undifferentiated, spontaneous fetal activity in the womb, known as “pre-sleep”.Citation1 According to its occurrence at different sleep periods, parasomnias are mainly divided into rapid eye movement (REM) and non-REM (NREM) parasomnias.Citation1–3 The pathophysiology of parasomnias has not been elucidated, detrimental perinatal factors might have an impact on the maturity of some neural circuits, resulting in parasomnia symptoms.Citation4 Up to 50% of children reported experiencing at least one parasomnia episode, which is prevalent before the age of five, and with the maturation of the nervous system, it tends to ease by about ten.Citation1,Citation5 Research on the health effects of parasomnia symptoms is scarce. Although evidence indicates that they might cause potential health injuries, there is controversial clinical advice on whether or not to intervene.
As a leading chronic disease in children, asthma usually onsets by the age of four.Citation6 Wheezing usually be an early symptom of later asthma, and about 3–5% of childhood asthma persists to adulthood, and more than 10% of childhood asthma relapses in adulthood, often with a worse prognosis.Citation6 Since genetic influences are insufficient to explain the alarming increase in asthma prevalence, many underestimated factors have been proposed to be involved in the pathogenesis of asthma.Citation7 From both the biomedical and public health perspective, increased asthma risks have been linked to preterm birth, and data on more readily modifiable factors of asthma among preterm newborns are relatively scarce.Citation7
Generally, previous studies have established a relationship between poor sleep characteristics, including sleep-wake habits, sleep duration, and sleep disordered breathing (SDB), with an increased risk of wheeze/asthma.Citation8–10 Parasomnia is modulated by several neural circuits, including γ-aminobutyric acid (GABA) and serotonin circuits.Citation2,Citation3 In neuroimmune pathophysiology in asthma, inflammatory mediators and neurotransmitters seem to facilitate the crosstalk and positive feedback loops between immune cells and nervous systems.Citation11,Citation12 However, regarding neuro-immune crosstalk, epidemiologic data on the association between parasomnia and asthma are quite sparse. To our knowledge, 15 studies have looked at a certain kind of parasomnia symptom with conflicting results. Restless leg syndrome,Citation13,Citation14 bruxism,Citation15–18 and sleep terrorCitation19,Citation20 were found to have supportive correlations, whereas enuresis had inconsistent results, with 5 positive relationshipsCitation21–25 and 2 non-significant associations.Citation26,Citation27 Others, like sleep talking, sleepwalking, sleep terror, and nightmares, have rarely been touched by previous studies.
Our aim was, therefore, to estimate the association of both specific and holistic parasomnia symptoms with childhood wheeze/asthma. Given the importance of fetal maturation in the development of parasomnia,Citation1 the interaction role of preterm and parasomnia with the association of wheeze/asthma would be given a point evaluation. Considering SDB is potentially a key confounder in the association between parasomnia and asthma, sensitivity analyses were performed on children without SDB. It is hoped that our study would be conducive to calling for clinical concerns about the health effects of parasomnia symptoms, as well as paying special attention to children with special sleep traits, and strengthening the emphasis on the long-term health of premature children.
Material and Methods
Study Design and Population
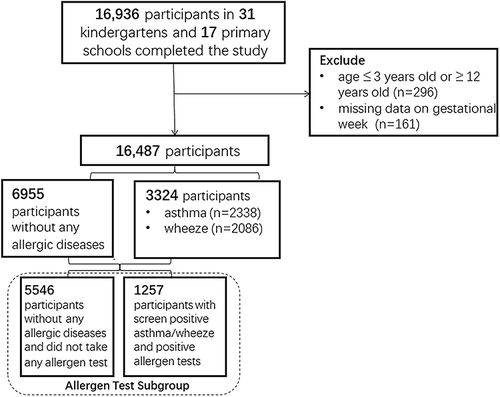
This cross-sectional study used data from the Shanghai Children’s Allergy Study, which took place in Shanghai, China, from April 12 to June 1, 2019.Citation28 A multistage cluster sampling strategy was adopted. Among a total of 9 urban areas and 8 suburban/rural areas in Shanghai, 31 kindergartens and 17 primary schools in 7 urban areas (Xuhui, Huangpu, Hongkou, Putuo, Changning, Yangpu, and Pudong New Area) and 6 suburban/rural areas (Minhang, Jinshan, Qingpu, Songjiang, Baoshan, and Chongming) were randomly sampled. After permission was obtained from these schools, the children and their caregivers were told of the study’s purposes and were advised that participation was voluntary. Informed consent form and the questionnaire were provided to the eligible population. Of all the 16,936 children included, a total of 16,487 children aged 3–12 years met the criteria after removing the missing data on gestational age and child age (). Ethical approval was obtained from the ethics committee of Shanghai Jiao Tong University School of Medicine (Ethics Approval Number: SJUPN-201717) in accordance with the Declaration of Helsinki. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies was followed.
Figure 1 Flow chart of this study. For this study, a total of 16,963 students were recruited from 36 kindergartens and 17 primary schools. 296 children were ruled out because they were not between the ages of 3 and 12, and 161 were ruled out owing to missing data on gestational week, leaving 16,487 children in the final analysis. In the analysis process, 6955 children without any allergic diseases (asthma, wheeze, allergic rhinitis, eczema, food allergy, and drug allergy) were regarded as the control group, and 2086 being screened for current wheeze and 2338 being screened for ever asthma. In the allergen test subgroup, 1257 children who had a positive response to both current wheeze/ever asthma and the allergen test were included, while 5546 children who did not have any of the stated allergic diseases and did not take the allergen test were regarded as reference group.
Allergic Outcomes
The current study used the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire to assess childhood allergic diseases.Citation29 In brief, information on ever-diagnosed asthma and current wheeze, as well as children’s allergen tests, was asked (details are described in the Supplement Figure 1). The Cronbach’s alpha coefficient of the ISAAC questionnaire in the sampled children was 0.94. The validity determined by the Kaiser-Meyer-Olkin method was 0.94.
Exposure
Sleep characteristics were assessed by the Children’s Sleep Habits Questionnaire (CSHQ), which was widely adopted to evaluate sleep characteristics from eight domains for children aged 2–12 years.Citation30,Citation31 In the CSHQ, the parasomnias subscale has seven items, including NREM parasomnias (sleep walking, sleep terror), REM parasomnias (sleep talking, sleep restless, and nightmares), and other symptoms (bruxism, enuresis); and the SDB subscale has three items, including loud snoring, stopped breathing, and snorts and gasps. Each question had three options, 1 = rarely (0–1 time/week), 2 = sometimes (2–4 times/week), and 3 = usually (5–7 times/week).Citation30,Citation31 Suffering from a specific parasomnia symptom was defined as answering “sometimes” or “usually” to the related question;Citation32 and SDB was defined as at least two SDB-related symptoms occurring two or more times per week.Citation33 Of the parasomnia and SDB subscales, the test–retest reliability (ICCs) was 0.46 and 0.43, and the internal consistency (Cronbach’s alpha) was 0.83 and 0.77, respectively, which were similar to previous studies.Citation34,Citation35
In terms of gestational weeks, a gestational age of less than 36 weeks is defined as a preterm birth. Further, moderate preterm and very preterm were classified as gestational age at 33–36 weeks and less than 32 weeks, respectively.
Additional Covariates
Information was collected on child age, gender, child overweight/obesity (defined as over 85% of standard age and sex-specific percentileCitation36), parent’s educational level, family income, family structure, family allergic history, family sleep disorder history, maternal age at delivery, maternal pre-pregnancy overweight (body mass index ≥25),Citation37 smoking, drinking, and negative life events in the mother’s life during pregnancy, cesarean delivery, low birth weight (birth weight <2500g),Citation38 multiple pregnancies, breastfeeding <6 months, passive smoking, and pet-keeping at home in the first year of child’s life. All these variables were recognized as potential confounders.
Statistical Analysis
The Chi-square test and t-test were adopted to compare the group differences where appropriate. Both crude and adjusted logistic regressions were conducted to explore the association of parasomnias with childhood wheeze/asthma. For the dependent variable, “1” indicates children with ever asthma, or with current wheeze, and “0” indicates the absence of any of the following allergy symptoms, including asthma, wheeze, allergic rhinitis, eczema, food allergy, and drug allergy (the determination of allergic rhinitis, eczema, food allergy, and drug allergy was illustrated in the Supplement Figure 1). In adjusted models, we first controlled for the demographic factors, then for the maternal and perinatal factors.
The following analyses were conducted to assess the association between parasomnias and wheeze/asthma while considering the possible role of preterm birth. First, both the multiplicative and additive interactions were performed to evaluate the possible interaction effects between preterm birth and parasomnias on the odds of childhood wheeze/asthma. When the combined OR was greater than the sum of parasomnias and preterm birth, there was an interaction on the additive scale. The three main indexes are calculated with the following equations, and computations were made for the 95% CIs with the Hosmer–Lemeshow delta method: the relative excess risk due to interaction (RERI) = RR11 − RR10 − RR01 + 1; the proportion attributable to interaction (AP) = RERI/RR11; the synergy index (SI) = (RR11 − 1)/([RR10 – 1] + [RR01 – 1]). RERI or AP of 0, or synergy index of 1 suggests no interaction.Citation39 Second, each single parasomnia symptom was enrolled to analyze their association with ever asthma and current wheeze, stratified by gestational age (full-term vs preterm birth). Multiple testing corrections were implemented using the Benjamini and Hochberg false discovery rate methods.Citation40 Finally, the association of cumulative parasomnia symptoms with wheeze/asthma was investigated, with preterm birth being further stratified (full-term vs moderately preterm (33–36 weeks) vs very preterm birth (≤32 weeks)).
Sensitivity analyses were performed on the SDB excluded population (n = 15,884) and the allergen testing subgroup (n = 6803). In the allergen test subgroup, “1” was coded for those with positive screens for wheeze/asthma and allergen tests, “0” was for those without any screened allergic symptoms and did not take the allergen test.
All analyses were performed using SPSS, version 23.0 (IBM-SPSS Statistics Inc) and R, version 3.5.3 (The R Foundation for Statistical Computer, www.r-project.org). A 2-sided p value <0.05 was recognized to be statistically significant.
Results
Our analysis comprised 16,487 children (8641 males [52.4%]) with a mean (SD) age of 7.74 (2.33) years after excluding the missing data on gestational age (n = 161) and child age (n = 296). A total of 2086 (12.7%) children were screened as having current wheeze, 2338 (14.2%) as having ever-diagnosed asthma, and 6955 were not screened with any allergic symptoms (). In the allergen test subgroup, 1257 children were in the case group, and 5546 were in the control group ().
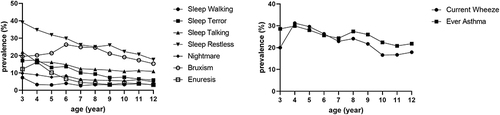
Children with wheeze/asthma were more likely to be younger, overweight/obesity, male, and have higher education of parents, higher family income, extended family life, family histories of allergies and sleep disorders, mothers of higher delivery age and experiencing negative life events during pregnancy, born by cesarean, preterm birth, breastfed for a shorter period of time, with more passive smoke exposure and keeping pet during first year of life (). The prevalence of current wheeze, ever-diagnosed asthma, and parasomnias was shown to be decreased with age (). The parasomnias were more likely to be occurred in children born preterm, particularly in the very preterm population (). Meanwhile, children with current wheeze and ever asthma were more likely to have parasomnia symptoms, with the exception of sleep walking ().
Table 1 Sample Characteristics
Table 2 Comparison of Parasomnia Symptoms Between Gestational Age Groups, and of Respiratory Allergic Groups in the Preterm Group
Figure 2 Age specific prevalence of current wheeze/ever asthma and single parasomnia symptoms.
Interaction Effects of Parasomnia and Preterm Birth on Childhood Current Wheeze and Ever Asthma
As reported in , after adjusting for all confounders, the multiplicative interaction between parasomnia and preterm birth was only significant in current wheeze (OR, 1.48; 95% CI, 1.01–2.19; p=0.049), while their interaction effects on the additive scale were presented to be both significant in current wheeze (RERI, 1.43; 95% CI, 0.41–2.45) and ever asthma (RERI, 0.75; 95% CI, 0.01–1.50). Compared with children who have neither preterm nor parasomnias, those only with preterm were associated with an increased risk of current wheeze (OR, 1.42; 95% CI,1.07–1.90; p=0.017); those only having parasomnias were associated with increased odds of current wheeze (OR, 1.66; 95% CI, 1.46–1.88; p<0.001) and ever asthma (OR, 1.56; 95% CI, 1.38–1.75; p<0.001); and the co-existence of parasomnia and preterm birth showed the most pronounced association with both current wheeze (OR, 3.50; 95% CI, 2.61–4.70; p<0.001) and ever asthma (OR, 2.60; 95% CI, 1.94–3.47; p<0.001).
Table 3 Interactive Associations Between Parasomnia, Preterm Birth and Current Wheeze and Ever Asthma
Association of Single Parasomnia Symptom and Childhood Current Wheeze and Ever Asthma, Stratified by Full-Term vs Preterm Children
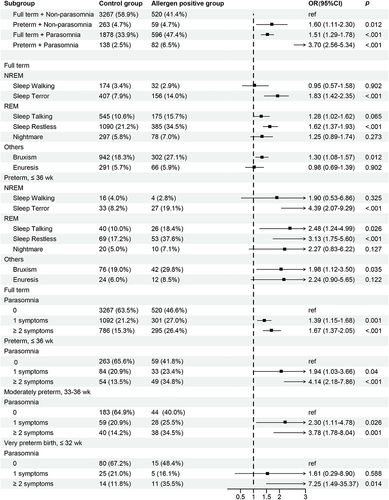
Considering the correlation between each parasomnia symptom (Supplement Table 1), we corrected the p values for multiple comparisons. As detailed in , regarding NREM parasomnias, an absence of association of sleepwalking with wheeze and asthma in the full-term group was reported, while significance was found in ever asthma in the preterm birth group after adjusting for all covariates (OR, 2.37; 95% CI, 1.06–5.34; corrected p=0.037). For REM parasomnias, the significant associations with current wheeze an ever asthma were consistently established in both full-term and preterm groups, whereas the strengths were higher in children born preterm. In terms of other parasomnia symptoms, similarly, bruxism was observed to be related to increased odds of current wheeze and ever asthma, and the odds were higher in the preterm group. The significant associations of enuresis with wheeze and asthma were only presented in the preterm children, even after full adjustments (ever asthma: OR, 2.35; 95% CI, 1.21–4.57; corrected p=0.014; current wheeze: OR, 2.56; 95% CI, 1.34–4.90; corrected p=0.009).
Table 4 Association Between Single Parasomnia Characteristic and Current Wheeze and Ever Asthma
Cumulative Association Between Parasomnias and Childhood Current Wheeze and Ever Asthma, Stratified by Full-Term vs Preterm Children
Further subdivided to create a hierarchy on preterm variables (), it showed that the more parasomnia symptoms children have, the higher the odds of current wheeze and ever-diagnosed asthma they would have in all three groups. Moreover, the shorter the gestational age, the higher the odds of current wheeze and ever asthma. Two or more parasomnia symptoms with very preterm birth were most strongly associated with both current wheeze (OR, 4.55; 95% CI, 1.69–12.25; p=0.003) and ever-diagnosed asthma (OR, 6.17; 95% CI,2.36–16.11; p<0.001).
Table 5 Association Between Parasomnia Symptoms and Current Wheeze and Ever Asthma, Stratified by Gestational Age
In the sensitivity analyses, either among the population without SDB (Supplement Tables 2–4) or in Allergen Test Subgroup ( and Supplement Tables 5–7), similar results were observed in most cases.
Figure 3 Forest plot for allergen test subgroup. Model adjusted for child age, overweight/obesity, gender, mother’s educational level, father’s educational level, family income, family structure, family allergic history, family sleep disorder history, maternal age at delivery, maternal pre-pregnancy overweight, maternal smoking, maternal drinking, negative life event, cesarean delivery, preterm birth, low birthweight, multiple pregnancy, breastfeeding, passive smoking, pet keeping during first year of life.
Discussion
To the best of our knowledge, this is the largest population-based study to discuss the association between parasomnia symptoms and the risk of childhood wheeze/asthma in its full range, considering the interaction effect of preterm birth. We should highlight two core findings. First, parasomnia symptoms, especially REM parasomnias, were associated with increased odds of current wheeze and ever asthma in children, with the trend being the more parasomnia symptoms, the higher the risks. Second, preterm birth interacts with parasomnia symptoms of an additive magnitude, suggesting that the combination of very preterm birth with multiple parasomnia symptoms has the highest odds of childhood wheeze/asthma. The sensitivity analyses performed in populations without SDB symptoms and with allergen test results yield similar results. Our findings indicate that the sleep health of children, especially in children with wheeze/asthma, requires practical support, and premature children merit more attention.
Concurring with previous evidence from clinic populations that implemented objective measures of parasomnia, the current study verifies the positive relationship between parasomnia symptoms (enuresis, sleep restlessness, sleep terror, and bruxism) and wheeze/asthma.Citation13–25 Moreover, our finding extends preliminary work with novel evidence for the relationship of the other parasomnia symptoms (sleep talking, sleepwalking, and nightmares) with childhood wheeze/asthma. Two other studies of enuresis in the early 1970s yielded inconsistent results.Citation26,Citation27 One involving 234 Caucasians from the upper-middle-class compared the persistent enuresis conditions in children who were treated for respiratory allergies and health controls,Citation26 and the other, involving a sample size of 55, used serum IgE as an indicator of allergy.Citation27 Both reported no association. The limited sample sizes may decrease statistical power and increase the probability of false negatives,Citation26,Citation27 and the diagnostic criteria for allergy only with IgE may include asymptomatic people or those with other allergic symptoms.Citation27 Back to the results of our study, the significant association between enuresis and wheeze/asthma was only exhibited in children born preterm, suggesting that the physiology early in life may play a pivotal role in that relationship. Broadly, our findings illustrated a comprehensive relationship between both combined and independent parasomnia symptoms and childhood wheeze/asthma, thereby making a prominent contribution to a cursory evidence base.
The underpinning mechanism between parasomnias and asthmatic diseases may be explained by the long-standing neuro-immune interactions. During NREM parasomnias, inactivation of the frontal lobe could produce disinhibition of the basal ganglia and activation of central pattern generator (functional clustering of motor neurons).Citation2 And NREM parasomnias have been suggested to be linked with anomalies in serotonin metabolism.Citation2 Serotonin could increase airway resistance, and allergen exposure results in serotonin-positive cells within the airway epithelia.Citation41 Besides, greater degrees of airway inflammation could be generated, as T cell proliferation and the release of proinflammatory cytokines like interleukin-2 (IL-2) and interferons (IFNs) are both dependent on serotonin-1A receptor activation.Citation42 As for REM parasomnias, they are indicated to be induced by the hyperpolarization of motor neurons by GABA and glycine during REM sleep, resulting in muscle atonia.Citation3 GABA has actions in the epithelium that are linked to bronchial remodeling,Citation11 and the GABA pathway could modulate mucus differentiation and result in increased excitability of vagal preganglionic neurons, elevating cholinergic output to the airways and producing airway hyperresponsiveness and chronic constriction.Citation43–45 And REM parasomnias are also suggested to be associated with an increase in inflammatory monocytes and mature natural killer cells, which may exert a role in regulating airway inflammation.Citation46,Citation47 For genetic etiologies, we performed the bidirectional Mendelian randomization, and revealed that genetically predicted insomnia was the risk factor for asthma, whereas asthma was not genetically associated with an increased risk of insomnia.Citation48 Conversely, shortness of breath, airway hyperresponsiveness, and the psychological stress caused by asthmatic symptoms, may be triggers for the occurrence of parasomnia.Citation49 And asthma-induced stress may also be a trigger for parasomnia.Citation1 As an airway obstruction condition, SDB was suggested to be a comorbidity of parasomnias and asthma.Citation21,Citation23,Citation25 However, due to a lack of or limited sample of SDB data in prior studies, this hypothesis has not been further investigated.Citation21,Citation25 In our analyses, the results of subgroup without SDB were consistent with our primary findings, implying that the link between parasomnias and childhood asthma/wheezing could be independent of SDB.
It is also the first time that our study found that the additive interaction effects of preterm birth with parasomnias could amplify the risk of childhood wheeze/asthma. Existing evidence has reported links between preterm birth and both wheeze/asthmaCitation7,Citation50 and parasomnias,Citation51 but no one has ever examined the role of preterm in the association between parasomnias and asthma. Since sleep develops during fetal life, prematurity is linked to poor sleep quality and later bedtimes in school-aged children, according to a systematic evaluation of nine qualitative cohort studies.Citation52 Our findings further support the “Developmental Origins of Health and Disease (DOHaD)” paradigm,Citation53 linking premature birth with the later impaired nervous system and lung development. Given the foregoing, it is recommended that future research focuses more on the impact of disrupted sleep, particularly in vulnerable infants born preterm, in order to optimize the chances of reducing asthma burden in these children.
Several limitations of this study should be noted. First, the assessment of parasomnias and asthmatic symptoms was done by parent-reported questionnaires. However, the CSHQ and ISAAC questionnaires we adopted were universally used, and their reliability and validity have been verified.Citation35 Parasomnia symptoms are comparatively obvious and easily detectable, and the questionnaire allowed us to assess a wide range of parasomnia symptoms in a large epidemiological study. The ascertainment of asthmatic symptoms was based on the questions asked about the doctor-diagnosed situations, and the allergen test subgroup was further applied to verify the result. And the age-specific prevalence trends we found were consistent with the previous literature.Citation1,Citation4 Second, although we extensively adjusted for prenatal and perinatal factors, there could be other unadjusted confounders. This may limit our results due to our inability to adequately distinguish between confounding and mediation in a cross-sectional setting. Third, the pathological link between each of the different symptoms, comorbid symptoms and wheeze/asthma may be divergent and have not been clarified. Generally, multiple parasomnia symptoms can coexist.Citation1–3,Citation54,Citation55 It is not known whether treatment of one or more of the major parasomnia symptoms will be accompanied by relief or elimination of other symptoms, thereby providing the maximum health benefit. Or alternatively, remission of asthma might help with any parasomnia symptoms. As the cross-sectional study is incapable of determining the temporal relationship, further prospective and mechanistic studies are warranted to prove the in-depth relationship.
Conclusion
Our study demonstrates the association of comprehensive parasomnia symptoms with childhood wheeze/asthma, while also considering the role of prematurity. In particular, multiple parasomnia symptoms combined with extreme prematurity are most strongly associated with increased odds of wheezing/asthma in children. The finding provides further insight into the pathophysiologic mechanism of wheeze/asthma from the perspective of sleep and even neuro-immune interactions, where parasomnia symptoms, as developmental sleep disorders, merit heeding in children with wheeze/asthma. Furthermore, as a vulnerable population, both late and very preterm babies need more prompt attention.
Abbreviations
REM, rapid eye movement; SDB, sleep disordered breathing; GABA, γ-aminobutyric acid; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; ISAAC, International Study of Asthma and Allergies in Childhood; CSHQ, Children’s Sleep Habits Questionnaire; RERI, relative excess risk due to interaction; AP, attributable proportion due to interaction; SI, synergy index; IL-2, interleukin-2; IFNs, interferons; DOHaD, Developmental Origins of Health and Disease.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Kotagal S. Parasomnias in childhood. Sleep Med Rev. 2009;13(2):157–168. doi:10.1016/j.smrv.2008.09.005
- Zadra A, Pilon M. NREM parasomnias - ScienceDirect. Handb Clin Neurol. 2011;99:851–868.
- Dauvilliers Y, Schenck CH, Postuma RB, et al. REM sleep behaviour disorder. Nat Rev Dis Primers. 2018;4(1):19. doi:10.1038/s41572-018-0016-5
- Nevsimalova S, Prihodova I, Kemlink D, Skibova J. Childhood parasomnia–a disorder of sleep maturation? Eur J Paediatr Neurol. 2013;17(6):615–619. doi:10.1016/j.ejpn.2013.05.004
- Ophoff D, Slaats MA, Boudewyns A, Glazemakers I, Van Hoorenbeeck K, Verhulst SL. Sleep disorders during childhood: a practical review. Eur J Pediatr. 2018;177(5):641–648. doi:10.1007/s00431-018-3116-z
- Fuchs O, Bahmer T, Rabe KF, von Mutius E. Asthma transition from childhood into adulthood. Lancet Respir Med. 2017;5(3):224–234.
- Castro-Rodriguez JA, Forno E, Rodriguez-Martinez CE, Celedón JC. Risk and protective factors for childhood asthma: what is the evidence? J Allergy Clin Immunol Pract. 2016;4(6):1111–1122. doi:10.1016/j.jaip.2016.05.003
- Koinis-Mitchell D, Kopel SJ, Seifer R, et al. Asthma-related lung function, sleep quality, and sleep duration in urban children. Sleep Health. 2017;3(3):148–156. doi:10.1016/j.sleh.2017.03.008
- Meltzer LJ, Beebe DW, Jump S, et al. Impact of sleep opportunity on asthma outcomes in adolescents. Sleep Med. 2020;65:134–141. doi:10.1016/j.sleep.2019.07.014
- Sánchez T, Castro-Rodríguez JA, Brockmann PE. Sleep-disordered breathing in children with asthma: a systematic review on the impact of treatment. J Asthma Allergy. 2016;9:83–91. doi:10.2147/jaa.S85624
- Pavón-Romero GF, Serrano-Pérez NH, García-Sánchez L, Ramírez-Jiménez F, Terán LM. Neuroimmune Pathophysiology in Asthma. Front Cell Dev Biol. 2021;9:663535. doi:10.3389/fcell.2021.663535
- Kabata H, Artis D. Neuro-immune crosstalk and allergic inflammation. J Clin Invest. 2019;129(4):1475–1482. doi:10.1172/jci124609
- Pearson VE, Gamaldo CE, Allen RP, Lesage S, Hening WA, Earley CJ. Medication use in patients with restless legs syndrome compared with a control population. Eur J Neurol. 2008;15(1):16–21. doi:10.1111/j.1468-1331.2007.01991.x
- Güngen AC, Güngen B, Aydemir Y, Aras YG, Çoban H, Düzenli H. The relationship between restless legs syndrome and bronchial asthma. Clin Respir J. 2018;12(4):1460–1465. doi:10.1111/crj.12684
- Motta LJ, Bortoletto CC, Marques AJ, Ferrari RA, Fernandes KP, Bussadori SK. Association between respiratory problems and dental caries in children with bruxism. Indian J Dent Res. 2014;25(1):9–13. doi:10.4103/0970-9290.131047
- Amato JN, Tuon RA, Castelo PM, Gavião MB, Barbosa Tde S. Assessment of sleep bruxism, orthodontic treatment need, orofacial dysfunctions and salivary biomarkers in asthmatic children. Arch Oral Biol. 2015;60(5):698–705. doi:10.1016/j.archoralbio.2015.02.011
- Fehlberg BK, Barros MBA, Lima MG. Health behaviors and multimorbidity associated with bruxism: population-based study. Oral Dis. 2021. doi:10.1111/odi.13928
- Ramos PFC, de Lima MDM, de Moura MS, Bendo CB, Moura L, Lima CCB. Breathing problems, being an only child and having parents with possible sleep bruxism are associated with probable sleep bruxism in preschoolers: a population-based study. Sleep Breath. 2021;25(3):1677–1684. doi:10.1007/s11325-020-02281-0
- Meltzer LJ, Pugliese CE. Sleep in young children with asthma and their parents. J Child Health Care. 2017;21(3):301–311. doi:10.1177/1367493517712064
- Fagnano M, Bayer AL, Isensee CA, Hernandez T, Halterman JS. Nocturnal asthma symptoms and poor sleep quality among urban school children with asthma. Acad Pediatr. 2011;11(6):493–499. doi:10.1016/j.acap.2011.05.006
- Dahan P, de Bessa J Jr., de Oliveira DM, et al. Association between asthma and primary nocturnal enuresis in children. J Urol. 2016;195(4 Pt 2):1221–1226. doi:10.1016/j.juro.2015.10.081
- Rawashdeh YF, Hvistendahl GM, Kamperis K, Hansen MN, Djurhuus JC. Demographics of enuresis patients attending a referral centre. Scand J Urol Nephrol. 2002;36(5):348–353. doi:10.1080/003655902320783854
- Tsai JD, Chen HJ, Ku MS, et al. Association between allergic disease, sleep-disordered breathing, and childhood nocturnal enuresis: a population-based case-control study. Pediatr Nephrol. 2017;32(12):2293–2301. doi:10.1007/s00467-017-3750-0
- Yılmaz-Durmuş S, Alaygut D, Soylu A, Alparslan C, Köse S, Anal Ö. The association between monosymptomatic enuresis and allergic diseases in children. Turk J Pediatr. 2018;60(4):415–420. doi:10.24953/turkjped.2018.04.009
- Ozkaya E, Aydın SC, Yazıcı M, Dundaröz R. Enuresis Nocturna in children with asthma: prevalence and associated risk factors. Ital J Pediatr. 2016;42(1):59. doi:10.1186/s13052-016-0266-3
- Siegel S, Rawitt L, Sokoloff B, Siegel B. Relationship of allergy, enuresis, and urinary infection in children 4 to 7 years of age. Pediatrics. 1976;57(4):526–528. doi:10.1542/peds.57.4.526
- Kaplan GW, Wallace WW, Orgel HA, Miller JR. Serum immunoglobulin E and incidence of allergy in group of enuretic children. Urology. 1977;10(5):428–430. doi:10.1016/0090-4295(77)90128-5
- Chen Y, Zhu J, Lyu J, et al. Association of maternal prepregnancy weight and gestational weight gain with children’s allergic diseases. JAMA Netw Open. 2020;3(9):e2015643. doi:10.1001/jamanetworkopen.2020.15643
- Asher MI, Montefort S, Björkstén B, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet. 2006;368(9537):733–743. doi:10.1016/s0140-6736(06)69283-0
- Goodlin-Jones BL, Sitnick SL, Tang K, Liu J, Anders TF. The children’s sleep habits questionnaire in toddlers and preschool children. J Dev Behav Pediatr. 2008;29(2):82–88. doi:10.1097/dbp.0b013e318163c39a
- Waumans RC, Terwee CB, Van den Berg G, Knol DL, Van Litsenburg RR, Gemke RJ. Sleep and sleep disturbance in children: reliability and validity of the Dutch version of the child sleep habits questionnaire. Sleep. 2010;33(6):841–845. doi:10.1093/sleep/33.6.841
- Goodwin JL, Kaemingk KL, Fregosi RF, et al. Parasomnias and sleep disordered breathing in caucasian and Hispanic children - the Tucson children’s assessment of sleep apnea study. BMC Med. 2004;2:14. doi:10.1186/1741-7015-2-14
- Kaditis AG, Alonso Alvarez ML, Boudewyns A, et al. Obstructive sleep disordered breathing in 2- to 18-year-old children: diagnosis and management. Eur Respir J. 2016;47(1):69–94. doi:10.1183/13993003.00385-2015
- Li SH, Jin XM, Shen XM, et al. [Development and psychometric properties of the Chinese version of children’s sleep habits questionnaire]. Zhonghua Er Ke Za Zhi. 2007;45(3):176–180. Chinese.
- Owens JA, Spirito A, McGuinn M. The Children’s Sleep Habits Questionnaire (CSHQ): psychometric properties of a survey instrument for school-aged children. Sleep. 2000;23(8):1043–1051. doi:10.1093/sleep/23.8.1d
- Kostovski M, Tasic V, Laban N, Polenakovic M, Danilovski D, Gucev Z. Obesity in childhood and adolescence, genetic factors. Pril. 2017;38(3):121–133. doi:10.2478/prilozi-2018-0013
- World Health Organization. Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995;854:1–452.
- Blencowe H, Krasevec J, de Onis M, et al. National, regional, and worldwide estimates of low birthweight in 2015, with trends from 2000: a systematic analysis. Lancet Glob Health. 2019;7(7):e849–e860. doi:10.1016/s2214-109x(18)30565-5
- Hosmer DW, Lemeshow S. Confidence interval estimation of interaction. Epidemiology. 1992;3(5):452–456. doi:10.1097/00001648-199209000-00012
- Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. R Stat Soc Ser B. 1995;57:289–300.
- Kajekar R, Pieczarka EM, Smiley-Jewell SM, Schelegle ES, Fanucchi MV, Plopper CG. Early postnatal exposure to allergen and ozone leads to hyperinnervation of the pulmonary epithelium. Respir Physiol Neurobiol. 2007;155(1):55–63. doi:10.1016/j.resp.2006.03.002
- Arreola R, Becerril-Villanueva E, Cruz-Fuentes C, et al. Immunomodulatory effects mediated by serotonin. J Immunol Res. 2015;2015:354957. doi:10.1155/2015/354957
- Feldman MB, Wood M, Lapey A, Mou H. SMAD signaling restricts mucous cell differentiation in human airway epithelium. Am J Respir Cell Mol Biol. 2019;61(3):322–331. doi:10.1165/rcmb.2018-0326OC
- Haxhiu MA, Kc P, Moore CT, et al. Brain stem excitatory and inhibitory signaling pathways regulating bronchoconstrictive responses. J Appl Physiol. 2005;98(6):1961–1982. doi:10.1152/japplphysiol.01340.2004
- Haxhiu MA, Rust CF, Brooks C, Kc P. CNS determinants of sleep-related worsening of airway functions: implications for nocturnal asthma. Respir Physiol Neurobiol. 2006;151(1):1–30. doi:10.1016/j.resp.2005.07.009
- Farmen K, Nissen SK, Stokholm MG, et al. Monocyte markers correlate with immune and neuronal brain changes in REM sleep behavior disorder. Proc Natl Acad Sci USA. 2021;118(10). doi:10.1073/pnas.2020858118
- Gangwar RS, Minai-Fleminger Y, Seaf M, et al. CD48 on blood leukocytes and in serum of asthma patients varies with severity. Allergy. 2017;72(6):888–895. doi:10.1111/all.13082
- Li R, Chen Y, Zhao A, et al. Exploring genetic association of insomnia with allergic disease and asthma: a bidirectional Mendelian randomization study. Respir Res. 2022;23(1):84. doi:10.1186/s12931-022-02009-6
- Maski K, Owens JA. Insomnia, parasomnias, and narcolepsy in children: clinical features, diagnosis, and management. Lancet Neurol. 2016;15(11):1170–1181. doi:10.1016/s1474-4422(16)30204-6
- Hadchouel A, Rousseau J, Rozé JC, et al. Association between asthma and lung function in adolescents born very preterm: results of the EPIPAGE cohort study. Thorax. 2018;73(12):1174–1176. doi:10.1136/thoraxjnl-2017-211115
- Nishizaki N, Obinata K, Kantake M, et al. Association between the frequency of bedwetting and late preterm birth in children aged ≥5 years. Acta Paediatr. 2019;108(2):282–287. doi:10.1111/apa.14481
- Visser SSM, van Diemen WJM, Kervezee L, et al. The relationship between preterm birth and sleep in children at school age: a systematic review. Sleep Med Rev. 2021;57:101447. doi:10.1016/j.smrv.2021.101447
- Barker DJ. The origins of the developmental origins theory. J Intern Med. 2007;261(5):412–417. doi:10.1111/j.1365-2796.2007.01809.x
- Arnulf I, Uguccioni G, Gay F, et al. What does the sleeping brain say? Syntax and semantics of sleep talking in healthy subjects and in parasomnia patients. Sleep. 2017;40(11). doi:10.1093/sleep/zsx159
- Dhondt K, Baert E, Van Herzeele C, et al. Sleep fragmentation and increased periodic limb movements are more common in children with nocturnal enuresis. Acta Paediatr. 2014;103(6):e268–72. doi:10.1111/apa.12610