
Abstract
The regularity of sleep/wake patterns across multiple days is emerging as an important determinant of health. However, the association between sleep regularity and health outcomes in the aging population is not well understood. The current systematic review identified 22 publications that examined the relationship between sleep regularity and selected health outcomes: cardiovascular risk, cognitive impairment, and mortality. All studies were published after 2010, reflecting a growing research interest in daily sleep regularity. Low sleep regularity was consistently associated with higher cardiovascular risk and elevated risk of all-cause mortality. Results on cognitive impairment are mixed, with inconsistency likely attributed to small sample sizes and differences in sleep regularity assessment. Overall, regularity in sleep carries important information about health and should be included in future studies that collect daily sleep measures. Gaps in literature and methodological shortcomings are discussed.
It is widely acknowledged that advancing age brings about changes in both the duration and quality of sleep.Citation1 These age-related differences are systematically related to cardiovascular health,Citation2 cognitive abilities,Citation3 dementia,Citation4 and all-cause mortality.Citation5 Most existing literature on sleep and health outcomes has largely focused on single-night assessment of sleep duration and efficiency. However, no two nights of sleep are the same, and the day-to-day variations in sleep metrics can carry additional information about a person’s health compared to average measures.
The day-to-day variation in sleep/wake patterns sleep metrics (ie duration and bedtime) over an observation period has been reported across a wide age range.Citation6 This variation, also known as sleep regularity, has been linked to health-relevant factors such as mental well-being and physical illness.Citation7–9 Sleep regularity can be quantified as the intra-individual standard deviations of sleep metrics across days (duration, bedtime and fragmentation) or as similarity in sleep/wake patterns across 24 hours (sleep regularity index).Citation10 Wrist actigraphy and other wearable devices have made it feasible to objectively assess daily sleep regularity at scale and over periods of weeks and longer, offering a richer understanding of sleep’s relationship with health.
A comprehensive reviewCitation11 by Bei et al in 2016 identified 53 publications examining the correlates of sleep regularity across the lifespan. The review found that low sleep regularity, despite imperfect assessments, was associated with adverse health outcomes. Although most studies in the Bei et al, review appear not to be explicitly designed to evaluate sleep regularity, over a third (19) of the studies included older adults over the age of 50, indicating a substantial interest in examining the relationship between sleep and health outcomes in this age group.
The current review will specifically focus on sleep regularity in older adults over the age of 50. The declines in both physical and cognitive health that come with aging, leading to premature mortality, impose substantial costs on both healthcare and public service systems. Various measures of sleep have been examined as potential biomarkers in aging.Citation12,Citation13 In the 2016 review by Bei et al, cardiovascular risk and cognitive impairment/dementia were the two most studied outcomes in older adults. The current review would explicitly focus on these two health outcomes with the most evidence and the ultimate health outcome (premature mortality).
Recent large-scale epidemiological studies, integrating actigraphy for objective sleep measurement, have paved the way for more in-depth investigations into how sleep regularity interacts with important health outcomes. Datasets like MrOS,Citation14 SOF,Citation14 MESA,Citation15 and UK BiobankCitation16–18 combine multi-night actigraphy-measured sleep with assessments of cardiovascular risk factors, cognitive impairment, and dementia. Some of these datasets, such as UK Biobank, tracked mortality.Citation16,Citation18 Consequently, there has been a notable increase in publications since the 2016 review focusing on sleep regularity and its implications for health in the aging population.
Considering this emerging research topic, the primary objective of this review is to systematically compile existing evidence regarding the importance of sleep regularity on cardiovascular health, cognitive impairment/dementia, and risk of premature mortality in older adults. After summarizing the available literature, we sought to identify gaps in current knowledge, to guide future research in this area.
Methods
Data Sources and Searches
The initial search was done through PubMed and Web of Science, using pre-specified search terms. A filter was applied in all databases to include studies on human adults aged 50 and above.
Included articles met the following requirements: a) measured sleep (ir)regularity, b) include a sample of older adults (average age 50+), c) reported health outcomes including cardiovascular risk factors, cognitive functioning and dementia and incident of mortality and d) reported associations between sleep regularity measures from a) and health measures from c).
The search terms used for PubMed and PsycInfo are combinations of the following terms: “Sleep (ir)regularity” OR “Sleep variability” OR “(ir)regular sleep” OR “variation in sleep” AND “Ageing” OR “Aging” OR “older adults” OR “elderly” OR “senior” NOT “review” NOT “meta-analysis” NOT “sleep deprivation” NOT “sleep apnea” NOT “commentary” NOT “animal”.
Study Selection
Articles were excluded if they only assessed sleep regularity and health outcomes in: (a) patients with sleep disorders (ie, insomnia and sleep apnea), and (b) lifespan samples of adults without separately reporting results for older adults. Articles were excluded if sleep regularity was associated with other health factors: (a) cardiometabolic diseases (incl. diabetes), (b) mood disorders, and (c) other diseases (incl. COVID-19 infection).
Articles were also excluded if sleep regularity was assessed after sleep manipulation (eg, sleep deprivation experiments or pharmacological trials).
Reference lists of included studies and previous reviewsCitation11,Citation19,Citation20 were also searched.
Data Extraction
For each study, a series of pre-defined characteristics were systematically extracted: a) year of publication, b) mean age of older participants, c) device used to assess sleep (ir)regularity, d) metrics used to quantify sleep (ir)regularity, e) number of days of sleep recording, f) sample size, and g) availability of data (ie, open databases).
Definition of Sleep Regularity
Sleep (ir)regularity is defined as the daily variation in sleep/wake pattern. Measures of sleep (ir)regularity include standard deviation and coefficients of variance of sleep metrics (ie, duration, timing, and efficiency), or the sleep regularity index (SRI)Citation10 which indexes the average concordance in sleep/wake state across two consecutive-24-hour periods. For the current review, all metrics that assess daily variation in sleep/wake patterns were eligible, including self-reported sleep regularity. In the results section, high sleep regularity refers to low standard deviations of sleep metrics or a high sleep regularity index.
Outcome Measures
Outcomes evaluated were all-cause mortality, cognitive impairment including dementia and cardiovascular risk factors, which were blood pressure (including hypertension), BMI, waist circumference, cardiovascular diseases (including events in the heart and brain), adiposity, and obesity.
Quality Assessment
We utilized the quality assessment scale adopted by Bei et al in their 2016 systematic review.Citation11 This assessment scale includes ratings of: 1) A priori aim/hypothesis; 2) Sample size justification; 3) Sample representativeness; 4) Number of days; 5) Quality of sleep measures; 6) Quality of correlates measures; 7) Rates of missing in daily data; 8) Inferences and conclusions. Quality of sleep measures was rated based on the following criteria: a) if a wearable/nearable tracker was used to assess sleep, the device was a research-grade device (eg actigraph) or well-validated commercial device (eg, Fitbit); b) quality control and processing of tracker data followed a standard approach (eg, removal of days with less than 8 hours of recording); c) if a self-report questionnaire was used, it had a question specifically for sleep regularity within the past week/month.
Results
Search results
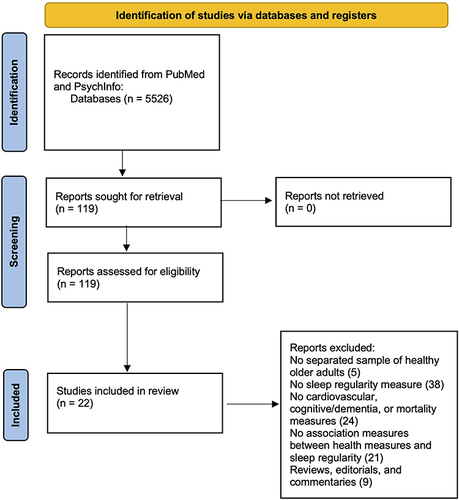
Systematic searches returned 5526 records for title and abstract screening. After initial screening, 119 articles were selected for full-text screening, 22 of which were included for data extraction and review. See for a flowchart of the search process. Characteristics of the included studies are presented in .
Table 1 Characteristics of Included Studies
Figure 1 PRISMA Flow chart for the literature search.
Context and Design
All included studies were published after 2010. Almost all studies (21 out of 22) were observational. The single intervention study did not target sleep or sleep regularity.Citation26 Seven studies analyzed sleep and health data from public datasets that are accessible to researchers (MESA, MrOS, SOF, and UK Biobank). In addition, six studies were part (ancillary data) of large-scale epidemiological studies that aimed to examine public health.
Characteristics of the Samples
Most studies (17 out of 21) were conducted in North America or Europe, three studies were conducted in Japan and one in Korea.
Two studies included older patients with mild cognitive impairment and Alzheimer’s disease. The 20 other studies recruited cognitively normal community-dwelling older adults. Thirteen studies have sample sizes over 1000, the other 9 studies have sample sizes under 200. One studyCitation25 included some middle-aged adults, with a mean age of 50. All other studies have mean ages over 55.
Measurements and Analyses of Sleep Regularity
Seventeen studies used standard deviations of sleep metrics to assess regularity. Three used the SRI. The remaining two studies used participants’ self-reported sleep regularity ratings. Eighteen studies used wrist-worn accelerometer-based devices to assess sleep/wake activities. One study used an infrared motion sensor to detect movements in bed. One study used a sleep diary, and two studies used a single question in a sleep questionnaire to assess self-report sleep regularity.
Quality Assessment
Quality assessment of individual studies is presented in . Inferences and conclusions from all studies were well supported by results. Most studies recruited representative samples (21 out of 22) and well-validated health outcome measures (21 out of 22). Majority of the studies used well-validated assessment devices for daily sleep/wake patterns (19 out of 22). Most studies have a-prior hypotheses about sleep regularity and health outcomes (14 out of 22). Only 5 studies recorded sleep for more than 7 days, and 2 studies used one-time self-report sleep regularity estimates. None of the studies provided justification of sample size, although most studies (14) had sample sizes over 200 suggesting sufficient power. No study reported the number of days when data were missing.
Table 2 Quality Assessment of Included Studies
Primary Findings
Of the 22 studies included in the current review, 10 examined associations of sleep regularity with cardiovascular health (including cardiovascular diseases and risk factors). Nine studies examined sleep regularity with cognitive functioning in healthy older adults and with dementia status in patients. The remaining 3 studies examined how sleep (ir)regularity was associated with all-cause mortality.
Sleep Regularity and Cardiovascular Risk/ Adiposity
The cardiovascular risk factor examined by most studies was body weight (N=7). In general, low sleep regularity was related to high BMI, large waist circumference, high body fat, increased fat mass and high likelihood of obesity.Citation7,Citation14,Citation21,Citation23,Citation24 In a lifestyle intervention study, low baseline sleep regularity was associated with less decrease in weight and BMI in older adults.Citation26
Fewer studies examined the likelihood of cardiovascular diseases. Low sleep regularity was related to greater prevalence of hypertension, high systolic and diastolic blood pressures, and high risk of developing cardiovascular diseases.Citation7,Citation21,Citation22,Citation25 Only one study examined health of the cardiovascular system directly and found high sleep duration variability was associated with high coronary artery calcium burden and abnormal ankle-brachial index.Citation15
Almost all studies in this domain assessed sleep regularity objectively across only 3–7 days in large samples (N>1000). Results from this group were largely consistent in showing a negative correlation between sleep irregularity and cardiovascular health. Only one study assessed subjective sleep regularity with a sleep questionnaire, and this study reported non-significant association between self-reported variability in sleep duration and obesity.Citation27
Sleep Regularity and Cognitive Impairment/Dementia
Studies in this domain were highly heterogeneous in both sleep assessment methods and samples recruited. Sleep regularity was assessed using research-grade actigraphy, commercial smart watch, infrared motion sensor, and sleep diary. Intra-individual standard deviations of sleep duration, bedtime, onset latency, and fragmentation were all examined. Most studies included small samples of healthy older adults, MCI patients, and patients with dementia. Some studies included both patients and healthy older adults.
Four studies examined the relationship between sleep (ir)regularity and risk/biomarkers of dementia. Low sleep regularity was related to high risk of developing MCI or dementia, increased β-amyloid burden, and lower cortical thickness and gray matter volume.Citation28–30,Citation35 However, results seem to differ between healthy older adults and MCI patients, and between the various measures of sleep (ir)regularity. One study reported high sleep duration variability was associated with increased β-amyloid burden in MCI patients,Citation30 while another study found high sleep fragmentation variability related to frontal amyloid burden in healthy older adults but not in patients with MCI.Citation28
Four studies examined the relationship between sleep regularity and cognitive functions. Three found a significant negative relationship between sleep irregularity and cognitive performanceCitation30,Citation34,Citation36 while the other one reported null results.Citation33 Such inconsistency may be related to methods of sleep assessments. The only study that reported non-significant relationship between sleep duration variability used a subjective sleep diary to track sleep.Citation33
Two studies compared sleep (ir)regularity in persons belonging to different categories of cognitive function (healthy vs MCI vs dementia) and reported conflicting results. One studyCitation31 found that patients with Alzheimer’s disease had the lowest sleep regularity compared to MCI patients and healthy controls. When comparing MCI and health controls, however, this study found no significant difference. Another study also compared sleep regularity between MCI patients and healthy controls, but results showed that MCI patients had higher sleep regularity than healthy controls.Citation32 More studies comparing sleep regularity between the preclinical stages of dementia (MCI and healthy aging) are needed, to clarify the relationship between sleep (ir)regularity and the trajectory of cognitive decline towards MCI and Alzheimer’s disease.
Sleep Regularity and All-Cause Mortality
All three studies with large samples found that low sleep regularity was associated with premature mortality. Objectively assessed low sleep regularity was associated with increased mortality riskCitation17 and was found to be a stronger predictor of increased all-cause mortality risk than sleep duration.Citation18 Self-report irregular sleep pattern was also associated with increased all-cause mortality risk.Citation37
Discussion
Summary of Findings
The current review is the first to examine health correlates of sleep regularity in older adults. The resultant literature, although limited in number, highlights the emerging importance of assessing sleep regularity on multiple health outcomes. All studies were published after 2010, and most had clear hypotheses about sleep regularity and health outcomes. High sleep regularity was consistently associated with lower risks of cardiovascular disease and all-cause mortality and to a lesser extent cognitive impairment/dementia risk.
Measures of body weight, such as obesity and BMI, were the most examined cardiovascular risk factors concerning sleep regularity (7 studies). In contrast, three studies examined hypertension status, two examined incidents of cardiovascular disease, and only one examined direct cardiovascular health index such as ankle-brachial index. The imbalance in outcome measures could be attributed to study designs. Most studies in this group used data collected by large-scale epidemiological research, where body weight measures were more common than measures of other cardiovascular risk factors. More studies with broader outcomes are needed to expand our understanding of how sleep regularity influences cardiovascular health in older adults.
Studies that examined cognitive impairments and dementia, on the other hand, mostly collected data instead of using existing epidemiological datasets. As a result, studies in this group had small sample sizes of less than 200. Devices used to track sleep also varied in this group, including research-grade actigraphy, self-report sleep diary, commercial smartwatch (Fitbit), and infrared motion sensor. It is possible that small sample sizes and different sleep assessment devices contributed to inconsistent results from this group. Large-scale studies with well-validated devices are needed for this topic.
Three recent studies with large sample sizes (N>5000) linked mortality with sleep regularity in older adults. The mean follow-up time from sleep assessment ranges from 7.8 years to 15 years. Sleep assessments from all three studies were collected at a single time point and for a short time period (eg 7 days). Longitudinal studies with multiple sleep assessments would provide more insight into how changes in sleep-wake patterns influence premature mortality risk. In particular, analysis of missingness data might yield additional insights about sleep behavior and its relation to health risk.
Gaps and Future Directions
The most common assessment of sleep regularity was the intra-individual standard deviations. While standard deviation provides a straightforward and replicable assessment of regularity,Citation38 it is prone to systematic time effects (eg weekday weekend difference) that may inflate irregularity.Citation39 Furthermore, most studies used standard deviations with 7 days or less of sleep recordings to quantify sleep regularity. Mathematical models have shown significant fluctuations in standard deviations aggregated for 3 to 14 days.Citation40 Standard deviations calculated from short (less than 14 days) recording periods, therefore, may not be representative of one’s sleep regularity. It is recommended that future studies record sleep for more than 14 days to better quantify regularity using standard deviations.Citation41
Most studies, especially those in the cardiovascular health and mortality groups, used data collected by large-scale epidemiological research (eg MESA and UK Biobank). Although the advantages of using data from these research projects include large sample sizes and comprehensive health assessment, sleep was not the main outcome of these studies. As a result, these studies all had short actigraphy recording time and high missing data rate, such that some studies included subjects with only 2 or 3 nights of data. Results from these studies could be confounded by unstable standard deviations calculated from low quality, short recordings. Replication of the existing results with long and high quality actigraphy recordings is necessary.
Furthermore, comparison of results between studies was difficult due to the non-standardized assessment of sleep regularity across studies. Although most studies used standard deviations of sleep duration and bedtime, standard deviations of sleep fragmentation, efficiency, and onset latency were also examined by some studies. Additionally, the SRICitation10 was examined by a few studies as well. The variety of sleep regularity metrics may provide some insights into the multidimensional aspect of sleep health. However, it would be useful to standardize the assessment of sleep regularity to enable comparison across studies and replication of results.
Another obstacle to comparing results between studies was the various devices used to assess sleep regularity. While most studies used wrist-worn actigraphy to track sleep, a few studies used other devices such as an infrared sensor and subjective questionnaires. Past studies have demonstrated that there are only weak correlations between subjective and objective sleep measures,Citation42,Citation43 therefore results using different devices are not directly comparable. The heterogeneity observed in the group of studies examining the relationship between sleep regularity and cognitive functioning/dementia status may be attributed to the heterogeneous devices and methods used. Assessment of sleep regularity may be more suitable by objective devices than subjective recalls, especially in older adults whose memory is in decline.
Although low sleep regularity has been associated with negative health outcomes in older adults, the age-related difference in objective sleep regularity has not been clearly defined. Questionnaire-based studies found that older adults reported more regular sleep patterns than younger adults.Citation6,Citation44 To our knowledge, there is no study comparing objective sleep regularity between older and younger adults. There is also a need for longitudinal studies to track changes in sleep regularity patterns. If old age is indeed associated with high sleep regularity, a decline in regularity could be used as a potent behavior risk marker predicting cardiovascular events and cognitive impairment/dementia by clinicians and researchers.
While discussing potential mechanisms for specific correlations is outside of the scope of this review, it is important to note that environmental factors such as sleep environment and culture also affect sleep regularity. Recent publications examining sleep patterns in users of commercial trackers across the globe showed that people in Asian countries had lower sleep regularity compared to people in Europe/North America.Citation45 Only 3 studies in the current review were conducted outside of Europe/North America, signaling a need for diversity and global collaboration in examining the health correlates of sleep regularity.
Conclusion
In summary, the current review found that low sleep regularity was associated with worse cardiovascular health, increased risk of dementia and higher incidence of all-cause mortality in the aging population. Overall, the literature is small, but growing rapidly. Assessment of sleep regularity is not standardized and mostly inadequate. With the increasing popularity and accessibility of commercial wearable devices, future studies of aging on health should assess sleep regularity as an important determinant. It is also important to standardize sleep regularity assessment methods. Lastly, sleep (ir)regularity likely has a bi-directional relationship with cardiovascular disease and cognitive impairment in older adults. Results from the current reviews are associational. Future interventional studies should explore the potential causal effects of sleep disorders, cardiovascular disease, and cognitive impairment.
Disclosure
The authors report no conflicts of interest in this work.
References
- Ohayon MM, Carskadon MA, Guilleminault C, Vitiello MV. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: developing normative sleep values across the human lifespan. Sleep. 2004;27(7):1255–1273. doi:10.1093/sleep/27.7.1255
- German C, Makarem N, Fanning J, et al. Sleep, sedentary behavior, physical activity, and cardiovascular health: mesa. Med Sci Sports Exerc. 2020;53(4):724–731. doi:10.1249/mss.0000000000002534
- Qin S, Leong RLF, Ong JL, Chee MWL. Associations between objectively measured sleep parameters and cognition in healthy older adults: a meta-analysis. Sleep Med Rev. 2022;67:101734. doi:10.1016/j.smrv.2022.101734
- Zhao C, Noble JM, Marder K, Hartman JS, Gu Y, Scarmeas N. Dietary patterns, physical activity, sleep, and risk for dementia and cognitive decline. Curr Nutr Rep. 2018;7(4):335–345. doi:10.1007/s13668-018-0247-9
- Cheng GHL, Malhotra R, Østbye T, Chan A, Ma S, Lo JC. Changes in nocturnal sleep and daytime nap durations predict all-cause mortality among older adults: the panel on health and ageing of Singaporean elderly. Sleep. 2018;41(7). doi:10.1093/sleep/zsy087
- Dillon HR, Lichstein KL, Dautovich ND, Taylor DJ, Riedel BW, Bush AJ. Variability in self-reported normal sleep across the adult age span. Journals Gerontology Ser B. 2015;70(1):46–56. doi:10.1093/geronb/gbu035
- Lunsford-Avery JR, Engelhard MM, Navar AM, Kollins SH. Validation of the sleep regularity index in older adults and associations with cardiometabolic risk. Sci Rep-UK. 2018;8(1):14158. doi:10.1038/s41598-018-32402-5
- Coelho J, Pecune F, Levavasseur Y, et al. From improved sleep regularity to reduced sleep complaints and mental health conditions: a population-based interventional study using a smartphone-based virtual agent. SLEEP. 2023;46(9). doi:10.1093/sleep/zsad165
- Roumelioti ME, Argyropoulos C, Buysse DJ, Nayar H, Weisbord SD, Unruh ML. Sleep quality, mood, alertness and their variability in CKD and ESRD. Nephron Clin Pr. 2010;114(4):c277–c287. doi:10.1159/000276580
- Phillips AJK, Clerx WM, O’Brien CS, et al. Irregular sleep/wake patterns are associated with poorer academic performance and delayed circadian and sleep/wake timing. Sci Rep-UK. 2017;7(1):3216. doi:10.1038/s41598-017-03171-4
- Bei B, Wiley JF, Trinder J, Manber R. Beyond the mean: a systematic review on the correlates of daily intraindividual variability of sleep/wake patterns. Sleep Med Rev. 2016;28:108–124. doi:10.1016/j.smrv.2015.06.003
- Mander BA, Winer JR, Walker MP. Sleep and human aging. Neuron. 2017;94(1):19–36. doi:10.1016/j.neuron.2017.02.004
- Ravyts SG, Dzierzewski JM. Sleep and healthy aging: a systematic review and path forward. Clin Gerontol. 2022;1–13. doi:10.1080/07317115.2022.2064789
- Patel SR, Hayes AL, Blackwell T, et al. The association between sleep patterns and obesity in older adults. Int J Obesity. 2014;38(9):1159–1164. doi:10.1038/ijo.2014.13
- Full KM, Huang T, Shah NA, et al. Sleep irregularity and subclinical markers of cardiovascular disease: the multi‐ethnic study of atherosclerosis. J Am Heart Assoc. 2023;12(4):e027361. doi:10.1161/jaha.122.027361
- Windred DP, Jones SE, Russell A, et al. Objective assessment of sleep regularity in 60 000 UK Biobank participants using an open-source package. Sleep. 2021;44(12). doi:10.1093/sleep/zsab254
- Wallace ML, Lee S, Stone KL, et al. Actigraphy-derived sleep health profiles and mortality in older men and women. Sleep. 2022;45(4). doi:10.1093/sleep/zsac015
- Windred DP, Burns AC, Lane JM, et al. Sleep regularity is a stronger predictor of mortality risk than sleep duration: a prospective cohort study. Sleep. 2023:zsad253. doi:10.1093/sleep/zsad253
- Chaput JP, Dutil C, Featherstone R, et al. Sleep timing, sleep consistency, and health in adults: a systematic review 1. Appl Physiology Nutrition Metabolism. 2020;45(10):S232–S247. doi:10.1139/apnm-2020-0032
- Makarem N, Zuraikat FM, Aggarwal B, Jelic S, St-Onge MP. Variability in sleep patterns: an emerging risk factor for hypertension. Curr Hypertens Rep. 2020;22(2):19. doi:10.1007/s11906-020-1025-9
- Häusler N, Marques-Vidal P, Haba-Rubio J, Heinzer R. Association between actigraphy-based sleep duration variability and cardiovascular risk factors – results of a population-based study. Sleep Med. 2020;66:286–290. doi:10.1016/j.sleep.2019.02.008
- Huang T, Mariani S, Redline S. Sleep irregularity and risk of cardiovascular events the multi-ethnic study of atherosclerosis. J Am Coll Cardiol. 2020;75(9):991–999. doi:10.1016/j.jacc.2019.12.054
- Kim M, Sasai H, Kojima N, Kim H. Objectively measured night‐to‐night sleep variations are associated with body composition in very elderly women. J Sleep Res. 2015;24(6):639–647. doi:10.1111/jsr.12326
- Ogilvie RP, Redline S, Bertoni AG, et al. Actigraphy measured sleep indices and adiposity: the multi-ethnic study of atherosclerosis (Mesa). Sleep. 2016;39(9):1701–1708. doi:10.5665/sleep.6096
- Parise BK, Santos RB, Mesas AE, et al. Sleep irregularity and the association with hypertension and blood pressure levels: the ELSA-Brasil study. J Hypertens. 2023;41(4):670–677. doi:10.1097/hjh.0000000000003392
- Papandreou C, Bulló M, Díaz-López A, et al. High sleep variability predicts a blunted weight loss response and short sleep duration a reduced decrease in waist circumference in the PREDIMED-Plus Trial. Int J Obes. 2020;44(2):330–339. doi:10.1038/s41366-019-0401-5
- Sasaki N, Fujiwara S, Yamashita H, et al. Association between obesity and self-reported sleep duration variability, sleep timing, and age in the Japanese population. Obes Res Clin Pr. 2018;12(2):187–194. doi:10.1016/j.orcp.2017.10.008
- André C, Tomadesso C, Flores R, et al. Brain and cognitive correlates of sleep fragmentation in elderly subjects with and without cognitive deficits. Alzheimers Dementia Diagnosis Assess Dis Monit. 2019;11(1):142–150. doi:10.1016/j.dadm.2018.12.009
- Diem SJ, Blackwell TL, Stone KL, et al. Measures of sleep–wake patterns and risk of mild cognitive impairment or dementia in older women. Am J Geriatric Psychiatry. 2016;24(3):248–258. doi:10.1016/j.jagp.2015.12.002
- Fenton L, Isenberg AL, Aslanyan V, et al. Variability in objective sleep is associated with Alzheimer’s pathology and cognition. Brain Commun. 2023;5(2):fcad031. doi:10.1093/braincomms/fcad031
- Guarnieri B, Maestri M, Cucchiara F, et al. Multicenter study on sleep and circadian alterations as objective markers of mild cognitive impairment and alzheimer’s disease reveals sex differences. J Alzheimer’s Dis. 2020;78(4):1707–1719. doi:10.3233/jad-200632
- Hayes TL, Riley T, Mattek N, Pavel M, Kaye JA. Sleep habits in mild cognitive impairment. Alzheimer Dis Assoc Disord. 2014;28(2):145–150. doi:10.1097/wad.0000000000000010
- McCrae CS, Vatthauer KE, Dzierzewski JM, Marsiske M. Habitual sleep, reasoning, and processing speed in older adults with sleep complaints. Cognitive Ther Res. 2012;36(2):156–164. doi:10.1007/s10608-011-9425-4
- Okuda M, Noda A, Iwamoto K, et al. Effects of long sleep time and irregular sleep–wake rhythm on cognitive function in older people. Sci Rep-UK. 2021;11(1):7039. doi:10.1038/s41598-021-85817-y
- Silva NCBS, Falck RS, Chan PCY, et al. The association of sleep and cortical thickness in mild cognitive impairment. Exp Gerontol. 2022;167:111923. doi:10.1016/j.exger.2022.111923
- Westerberg CE, Lundgren EM, Florczak SM, et al. Sleep influences the severity of memory disruption in amnestic mild cognitive impairment. Alz Dis Assoc Dis. 2010;24(4):325–333. doi:10.1097/wad.0b013e3181e30846
- Omichi C, Koyama T, Kadotani H, et al. Irregular sleep and all-cause mortality: a large prospective cohort study. Sleep Heal. 2022;8(6):678–683. doi:10.1016/j.sleh.2022.08.010
- Ram N, Gerstorf D. Time-structured and net intraindividual variability: tools for examining the development of dynamic characteristics and processes. Psychol Aging. 2009;24(4):778–791. doi:10.1037/a0017915
- Estabrook R, Grimm KJ, Bowles RP. A monte carlo simulation study of the reliability of intraindividual variability. Psychol Aging. 2012;27(3):560–576. doi:10.1037/a0026669
- Óskarsdóttir M, Islind AS, August E, Arnardóttir ES, Patou F, Maier AM. Importance of getting enough sleep and daily activity data to assess variability: longitudinal observational study. Jmir Form Res. 2022;6(2):e31807. doi:10.2196/31807
- Lau T, Ong JL, Ng BKL, et al. Minimum number of nights for reliable estimation of habitual sleep using a consumer sleep tracker. Sleep Adv. 2022;3(1). doi:10.1093/sleepadvances/zpac026
- Unruh ML, Redline S, An M, et al. Subjective and objective sleep quality and aging in the sleep heart health study. J Am Geriatr Soc. 2008;56(7):1218–1227. doi:10.1111/j.1532-5415.2008.01755.x
- McCarter SJ, Hagen PT, Louis EK, et al. Physiological markers of sleep quality: a scoping review. Sleep Med Rev. 2022;64:101657. doi:10.1016/j.smrv.2022.101657
- Kramer CJ, Kerkhof GA, Hofman WF. Age differences in sleep–wake behavior under natural conditions. Pers Individ Differ. 1999;27(5):853–860. doi:10.1016/s0191-8869(99)00034-3
- Willoughby AR, Alikhani I, Karsikas M, Chua XY, Chee MWL. Country differences in nocturnal sleep variability: observations from a large-scale, long-term sleep wearable study. Sleep Med. 2023;110:155–165. doi:10.1016/j.sleep.2023.08.010