
Abstract
Purpose
Catathrenia is a rare sleeping disorder characterized by repetitive nocturnal groaning during prolonged expirations. Patients with catathrenia had heterogeneous polysomnographic, comorbidity, craniofacial characteristics, and responses to treatment. Identifying phenotypes of catathrenia might benefit the exploration of etiology and personalized therapy.
Patients and Methods
Sixty-six patients diagnosed with catathrenia by full-night audio/video polysomnography seeking treatment with mandibular advancement devices (MAD) or continuous positive airway pressure (CPAP) were included in the cohort. Polysomnographic characteristics including sleep architecture, respiratory, groaning, and arousal events were analyzed. Three-dimensional (3D) and 2D craniofacial hard tissue and upper airway structures were evaluated with cone-beam computed tomography and lateral cephalometry. Phenotypes of catathrenia were identified by K-mean cluster analysis, and inter-group comparisons were assessed.
Results
Two distinct clusters of catathrenia were identified: cluster 1 (n=17) was characterized to have more males (71%), a longer average duration of groaning events (18.5±4.8 and 12.8±5.7s, p=0.005), and broader upper airway (volume 41,386±10,543 and 26,661±6700 mm3, p<0.001); cluster 2 (n=49) was characterized to have more females (73%), higher respiratory disturbance index (RDI) (median 1.0 [0.3, 2.0] and 5.2 [1.2, 13.3]/h, p=0.009), more respiratory effort-related arousals (RERA)(1 [1, 109] and 32 [13, 57)], p=0.005), smaller upper airway (cross-sectional area of velopharynx 512±87 and 339±84 mm2, p<0.001) and better response to treatment (41.2% and 82.6%, p=0.004).
Conclusion
Two distinct phenotypes were identified in patients with catathrenia, primary catathrenia, and catathrenia associated with upper airway obstruction, suggesting respiratory events and upper airway structures might be related to the etiology of catathrenia, with implications for its treatment.
Introduction
Catathrenia is a rare sleeping disorder, characterized by recurrent episodes of prolonged expiration with the production of groaning sounds during sleep.Citation1 Patients with catathrenia often complained about social embarrassment, and some patients also suffer from unrefreshing sleep and daytime fatigue.Citation2 Since the disease was first reported in 1983,Citation3 there have been controversial findings of its polysomnographic characteristics, classification, combination with obstructive sleep apnea (OSA), craniofacial characteristics, and treatment efficacy.
Early investigations have documented that groaning events tend to occur predominantly in rapid eye movement (REM) sleep,Citation4–7 whereas cases with the predominance in non-REM (NREM) sleepCitation8–10 and equal distribution across sleep stagesCitation11,Citation12 were also reported. A close association between groaning and arousal events has been observed in several studies,Citation13–16 however, a similar association was not replicated in other studies.Citation17 Besides, catathrenia patients combined with OSA seemed to have a better response to the treatment of continuous positive airway pressure (CPAP) or mandibular advancement devices (MAD).Citation8,Citation11,Citation18–20 With the above heterogeneous findings, there has been an ongoing debate about the classification of catathrenia, whether it is a parasomnia or sleep-related breathing disorder.Citation1,Citation21–23
Limited consistency often exists in sleeping disorders, and different subtypes exist.Citation24 Recently, unsupervised cluster analysis has been used to identify subtypes of various sleeping disorders. Gool et al utilized a data-driven clustering algorithm with symptoms, demographics, objective and subjective sleep measures, and laboratory biomarkers and identified 7 clusters of phenotypes of central disorders of hypersomnolence.Citation25 The heterogeneity of OSA, the most common sleep-related breathing disorder, has also been explored by cluster analysis with combinations of symptoms,Citation26–29 polysomnography,Citation30–33 comorbidities,Citation26,Citation27,Citation31,Citation34–36 craniofacial pattern,Citation37–39 and treatment.Citation35,Citation40–43 Similarly, knowledge of the heterogeneity might benefit the exploration of etiology and personalized treatment of catathrenia. Therefore, this study aims to examine the heterogeneity of catathrenia with regard to patients’ demographics, polysomnographic parameters, craniofacial anatomical characteristics, and treatment response with cluster analysis. We hypothesized that there are different phenotypes of catathrenia.
Materials and Methods
Study Participants
This prospective cohort study was conducted at the Department of Orthodontics, Peking University Hospital of Stomatology. From August 2004 to April 2023, a total of 66 patients seeking treatment for catathrenia were included with informed consent. All the patients were diagnosed with catathrenia by full-night audio/video polysomnography at the Sleep Division of Peking University People’s Hospital and Peking University International Hospital. This study was approved by the Institutional Review Board of Peking University School of Stomatology (No. PKUSSIRB 201631128). This study was registered at the Chinese Clinical Trial Registry (No. ChiCTR-COC-17013239). The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Polysomnography
Full-night audio/video polysomnography was recorded using Compumedics E-series (Compumedics, Abbotsford, Victoria, Australia). The details of the polysomnography recording were described elsewhere.Citation17 All the records were evaluated manually by two certified technicians and verified by a researcher. The sleep technicians and researcher who scored the PSG did not participate in data analysis. Standards from the 2012 American Academy of Sleep Medicine (AASM) manual were used to score sleep stages, arousals, and respiratory events.Citation44 Apneas were defined as the oronasal thermal sensor drops by ≥90% of baseline for ≥ 10s. Hypopneas were defined as a ≥ 30% reduction of nasal pressure excursions of baseline amplitude for ≥ 10s, associated with ≥ 3% oxygen desaturation or arousal. Respiratory effort-related arousals (RERA) were defined as an increasing respiratory effort or flattening of the nasal pressure waveform followed by arousal. Since some patients were combined with OSA, the apnea-hypopnea index (AHI) was calculated as apnea and hypopnea events per hour of sleep. The respiratory disturbance index (RDI) was as equal to the AHI + RERA index. Groaning events were defined as deep inspiration followed by a prolonged expiration during which a monotonous vocalization was produced, or an exhalation like a sigh produced at the end of the expiration, without oxygen desaturation. Groaning events were scored separately to calculate the groaning index (GI, groaning events per hour of sleep). Arousal events were defined if there is an abrupt shift of electroencephalogram (EEG) frequency that lasts ≥ 3 s, and a concurrent increase in submental electromyography (EMG) in the REM stage. Groaning events-related arousals were defined in accordance with previous studies, with EEG arousal occurring before the onset of groaning events.Citation45,Citation46
Craniofacial and Upper Airway Structures Measurement
Informed choices were made by the patients to undergo cone-beam computed tomography (CBCT) to analyze craniofacial and upper airway structures. All images were obtained on a CBCT scanner (VATECH, DCTPRO-050Z, Vatech Co, Korea), with a scanning protocol of 120 kV, 5 mA, 13×17cm field of view, 0.25mm voxels, and a scanning time of 40s. All patients were asked to maintain centric occlusion, breathe evenly, and refrain from swallowing.
All the measurements of the craniofacial, upper airway, and surrounding soft tissue structures were assessed using Dolphin Imaging (Version 11.8 Premium; Dolphin Imaging, Chatsworth, CA) by the same examiner. The digital points of skeletal structures, the measurement of cross-sectional area, and the upper airway diameter are shown in and . Lateral cephalograms, radiographs commonly utilized in orthodontic practice, could be built from CBCT. The parameters of maxillofacial structures, upper and lower teeth, and upper airway were illustrated in Figure S1.
Figure 1 Measurements of craniofacial skeletal parameters on cone-beam computed tomography (CBCT). Maxillary length: distance between anterior and posterior nasal spine; anterior maxillary width: distance between left and right upper 3 dentin-enamel junction; posterior maxillary width: distance between the left and right maxillary tuberosity; mandibular width: distance between left and right 3D Gonion; mandibular total length: distance between the 3D condyle and mental protuberance; mandibular body length: distance between the angle of the mandible and mental protuberance; mandibular ramus height: distance between the 3D Gonion and condyle.
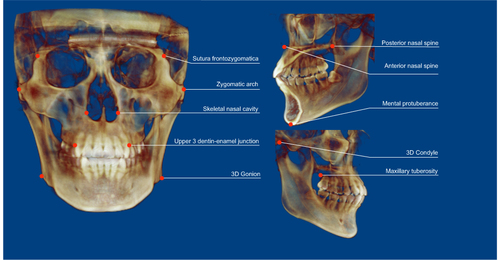
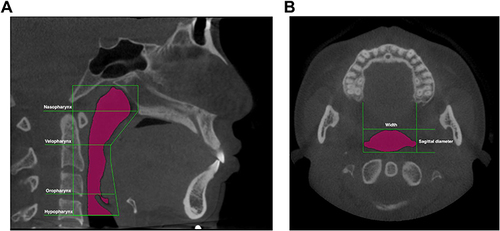
Figure 2 Measurement of upper airway structures. The upper airway is marked in pink. (A) Segmentation of upper airway and measurement of height; (B) measurement of cross-sectional area, width, and sagittal diameter.
Six patients (9%) were randomly selected for the replicated measurement, and the intra-reliability was tested with an intra-class correlation coefficient of 0.87 to 1.00.
Treatment Response
Informed decisions were made by 63 patients to either receive manually-titrated CPAP (n=7) at the Sleep Division of Peking University People’s Hospital or a custom-fit MAD (n=56) at the Department of Orthodontics, Peking University Hospital of Stomatology. Three patients have made the decision to forgo treatment. The design of MAD and the detailed efficacy in the treatment of catathrenia were detailed elsewhere.Citation20 The objective efficacy of treatment was evaluated with full-night audio/video PSG. The decrease of the groaning index (GI) with treatment was considered effective, and patients were classified into effective and ineffective groups.
Statistical Analysis
Normal distribution was analyzed using the Shapiro–Wilks test. Data with normal and skewed distribution were summarized as mean ± standard deviation (SD) and median (interquartile range, IQR), respectively, for continuous variables, and frequencies (percentages) for categorical variables. The K-means cluster analysis was performed using R 4.3.0 (The R Foundation for Statistical Computing, Vienna, Austria). Firstly, correlation analyses were conducted to identify parameters significantly related to GI. Secondly, the average silhouette width (ASW) analysis was used with significantly correlated parameters to determine the optimal number of clusters with the larger ASW, the better the split of clustering.Citation47 Thirdly, the independent t-test and Mann–Whitney test were used to perform inter-group comparisons. Pearson Chi-square test was used for categorical variables comparisons. A p-value less than 0.05 was considered statistically significant.
Results
Patients’ Characteristics
There were 25 males and 41 females included in the study, with an average age of 30.7±10.5 y. The average body mass index (BMI) was 21.9±3.1 kg/m2. The median apnea-hypopnea index (AHI) was 1.5 (IQR 0.4, 4.4) events/h, with fourteen (21.2%) patients diagnosed with OSA. The median RDI was 3.2 (IQR 1.0,12.8) events/h.
Clustering of Patients
A total of 157 parameters, including patients’ demographic characteristics (sex, age, BMI), polysomnographic characteristics (sleep architecture, respiratory events, oxygen saturation, arousal and groaning events), craniofacial and upper airway structures (volume, cross-sectional area, diameter, soft palate, and tongue), were used to explore significant correlation with GI as an initial screening. Thirteen parameters, including arousal index (ArI), number of groaning events, average duration of groaning events, etc, were included in the cluster analysis.
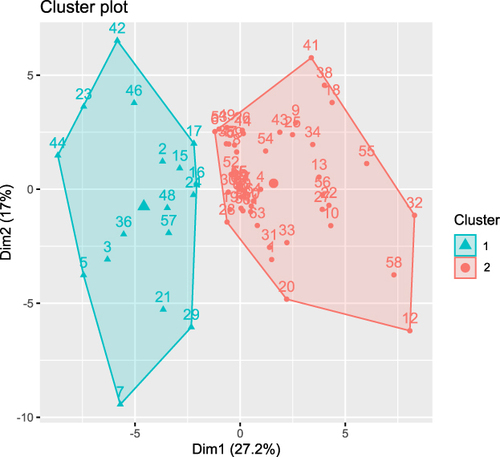
Two homogeneous clusters were identified by ASW (Figure S2) and K-means cluster analysis (). Cluster 1 consisted of 17 patients (25.8%), with a higher proportion (70.6%) of males (12 males, 5 females). Cluster 2 consisted of 49 patients (74.2%), with a higher proportion (73.4%) of females (13 males, 36 females). The distribution of patients’ sex was significantly different between clusters (p=0.003). There were no significant differences in age (34.3±12.6 and 29.5±9.6 y, p=0.106) and BMI (22.3±3.4 and 21.8±3.0 kg/m2, p=0.291) between clusters. Patients’ Epworth sleepiness scale was not statistically different between clusters either (8.1±4.0 and 8.2±3.1, p=0.962). Patients in cluster 1 mainly complained about headaches and difficulty falling asleep, whereas patients in cluster 2 mostly complained about restless sleep, dry mouth, and morning fatigue.
Figure 3 Scattergram for two clusters segregated by cluster analysis.
Subgroup Comparisons of Polysomnographic Characteristics
All the included patients had a median GI of 6.6 (IQR 2.4, 15.7) events/h and a median AHI of 1.5 (IQR 0.4, 4.4) events/h. The polysomnographic characteristics between clusters are shown in . There were no significant differences in sleep architecture between clusters in all patients. The AHI was not statistically different between clusters. However, the RDI of cluster 2 was significantly higher than that of cluster 1 (1.0 [0.3, 2.0] and 5.2 [1.2, 13.3]/h, p=0.009), with more RERA in cluster 2 (1[1, 109] and 32[13, 57], p=0.005) ().
Figure 4 The difference in respiratory disturbance index (RDI) between clusters. **p<0.01.
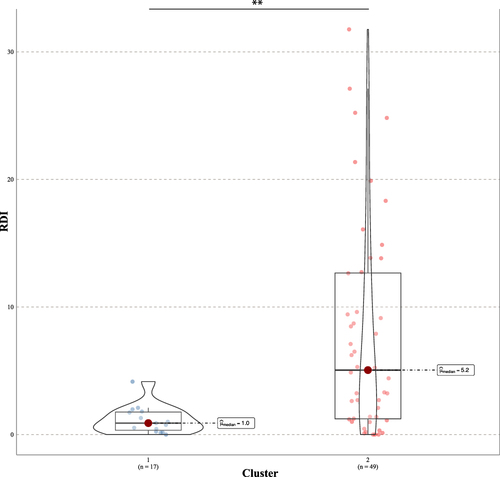
Table 1 The Polysomnographic Characteristics Between Subgroups
The inter-cluster differences in groaning events are shown in . The number of groaning events and groaning index was slightly higher in cluster 1, without statistical difference. However, the shortest and average durations of groaning events were significantly higher in cluster 1 (average duration 18.5±4.8 and 12.8±5.7s, p=0.005) (). The distribution of groaning events across sleep stages (REM-predominance) was similar between clusters. Patients in cluster 2 showed a better response to treatment of CPAP or MAD (41.1% and 82.6%, p=0.004).
Figure 5 The difference in the average duration of groaning events between clusters. **p<0.01.
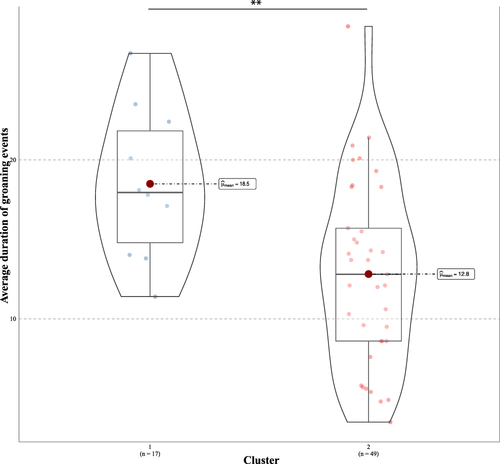
Table 2 The Characteristics of Groaning Events Between Subgroups
Subgroup Comparisons of Craniofacial Characteristics
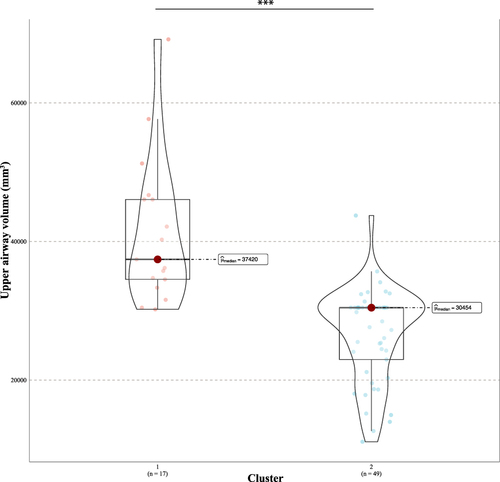
The characteristics of craniofacial and upper airway structures measured with CBCT are shown in . Inter-cluster analyses were performed according to patients’ sex to reduce the significantly different sex distribution on craniofacial anatomical structures. Overall, the 3D skeletal measurements did not show significant inter-cluster differences, except that the posterior maxillary width was larger in cluster 1 (p=0.022). Distinct characteristics were observed in the upper airway structures of different clusters. The upper airway volume was significantly smaller in cluster 2, from the nasopharynx to the hypopharynx, with the inter-cluster trend remaining consistent in both sexes. The minimum and average cross-sectional area and diameter in all the segments of the upper airway tend to be smaller in cluster 2 as well. The inter-cluster difference was slightly different in women, who showed significant differences only in the velopharynx and oropharynx. The characteristics of maxillofacial, upper and lower teeth, and upper airway structures measured with lateral cephalograms are shown in Table S1. Maxillofacial structures were fairly similar between clusters, except female patients in cluster 2 had more proclined upper incisors than those in cluster 1 (99.5±7.7 and 106.9±5.0°, p=0.006). Patients in cluster 1 showed significantly larger upper airways (), consistent with results measured on CBCT. Parameters of the soft palate, tongue, and hyoid bone did not differ between clusters.
Table 3 The Craniofacial Anatomical Characteristics Between Subgroups Measured with Cone-Beam Computed Tomography (CBCT)
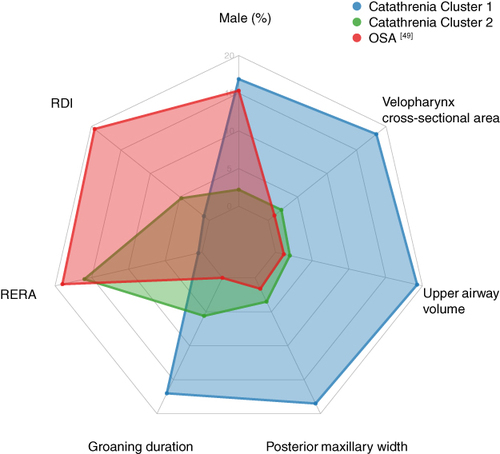
Overall, the polysomnographic and craniofacial characteristics of two phenotypes of catathrenia identified in the study are shown in .
Figure 6 The difference in the upper airway volume between clusters. ***p<0.001.
Discussion
With regard to the heterogenous clinical manifestations and etiology assumptions of catathrenia, this study used a data-driven approach of cluster analysis to explore the phenotypes of catathrenia, combining polysomnographic and craniofacial and upper airway characteristics. This study identified two phenotypes in patients with catathrenia: cluster 1, primary catathrenia, consisting of mainly male patients with longer duration of groaning events, lower RDI, and broader upper airway; cluster 2, catathrenia associated with upper airway resistance, consisting of mostly female patients with shorter duration of groaning events, higher RDI, smaller upper airway, and better response to treatment with MAD or CPAP. The characteristics of hard tissue in the maxillofacial area were similar between clusters.
Distinct craniofacial structures of patients with catathrenia have been discussed in previous studies. In this study, certain parameters of craniofacial structures were also found to vary between clusters of catathrenia. Hao et al compared the lateral cephalograms of catathrenia, OSA, and those without any sleep disorders. They observed that patients with catathrenia had broader upper airways and well-developed mandibles compared to the other two groups.Citation48 Yu et al confirmed these findings with more subjects with catathrenia, and used CBCT for measurement.Citation49 Furthermore, the study also observed patients with catathrenia had a steep cranial base. In the present study, the 3D and 2D measurements of hard tissue, including cranial base and maxillas, were consistently similar between clusters. Two distinct clusters can be identified based on the parameters of the upper airway, with cluster 2 having smaller upper airways despite the patients’ sex.
Figure 7 Two phenotypes of catathrenia identified in the study, compared with OSA. Data of OSA was extracted from reference.Citation49 Patients with catathrenia in cluster 2 exhibit similarities to those with OSA on several parameters, while those in cluster 1 do not.
In this study, the polysomnographic and craniofacial characteristics of patients in cluster 2 were similar to those in patients with sleep-disordered breathing (SDB) – higher RDI, more RERA, relatively narrower upper airway, and better response to treatment options of SDB. On the other hand, patients in cluster 1 had well-developed upper airway structures. Characteristics of cluster 2 might correspond to questions raised by Guilleminault et al that catathrenia is an SDB-related phenomenon that responds appropriately to interventions for SDB,Citation9 who reported seven female catathrenia patients with small upper airways. Besides, cases of catathrenia reported by other investigators also resembled cluster 2 of the current study. Iriarte et al reported a 62-year-old female patient combined with OSA and responded well to CPAP. 11 A 40-year-old female case of catathrenia and OSA reported by Songu, with Mallampati grade 3 upper airways, resulted in a marked improvement with CPAP treatment.Citation18 Craniofacial examinations of previous studies have revealed inconsistent findings on catathrenia, from normal maxillas and upper airway,Citation11,Citation50,Citation51 mandible retrognathiaCitation8,Citation9 to obstructive upper airway,Citation18 and even broad upper airway.Citation48,Citation49 The treatment efficacy of CPAP on catathrenia also varied greatly across studies.Citation8,Citation10,Citation11,Citation19,Citation52 These heterogeneous findings might derive from the phenotypes of catathrenia identified in the study.
Some investigations suggested there is a close association between arousal and groaning events. In this study, patients in cluster 2 had significantly more RERA; however, the arousal index did not differ between clusters, nor did arousals caused by groaning episodes. Muraki et al reported that more than 50% of the groaning episodes occurred after arousal.Citation53 Drakatos et al observed that arousals preceded or coincided with the onset of 84% of groaning events, which were of longer duration than those not associated with arousal.Citation45 Although the cluster analysis of the current study has documented significantly more RERA in cluster 2, the duration of groaning events in cluster 2 was significantly shorter. It might be speculated that arousal events may result from decreased airflow, and groaning events may act as an active maneuver to reduce upper airway resistance. Unfortunately, the results of the current study were unable to reproduce the findings of earlier studies. The association of groaning and arousal events requires further investigation.
The overall AHI of the two clusters was not significantly different in the study, whereas the RDI in cluster 2 was higher than in cluster 1. This study has found that patients in cluster 2 had a better response to treatment interventions for SDB. Some investigators have noticed a close association between catathrenia and OSA.Citation54 Songu et al reported a catathrenia patient combined with OSA treated with CPAP, which resulted in the resolution of groaning sounds and a decrease of AHI.Citation18 Several treatment trials have been conducted for catathrenia, including medications, CPAP, MAD, and surgery.Citation4,Citation9,Citation20,Citation55,Citation56 Yu et al observed that MAD had a better efficacy with respiratory events than groaning events, and anatomical structures of the upper airway might affect efficacy.Citation20 The etiology in cluster 2 might be resistance or obstruction of the upper airway. Patients with relatively smaller upper airway phenotypes responded better in the elimination of groaning events than those with broad upper airway dimensions. On the other hand, the etiology of cluster 1 was not clear, possibly associated with the instability of the neural structures controlling ventilation during sleep, as Poli et al suggested.Citation57 Alternative treatment options might be required to achieve the desired efficacy for patients in cluster 1.
The similarities between cluster 2 catathrenia identified in the current study and OSA have raised another question – whether catathrenia tends to occur in patients with OSA, who have even smaller upper airway structures and more respiratory events at night. Previous studies have pointed out that groaning events, with a flat airflow signal similar to apneas, could be misclassified in home sleep apnea tests (HSAT) and PSG.Citation58,Citation59 Therefore, catathrenia might be common in patients with OSA and has been underdiagnosed. These assumptions considering associations between catathrenia and OSA, need future investigations.
There are some strengths of the study. First, the identification of subtypes of catathrenia improves the knowledge and awareness of the heterogeneity of catathrenia clinical presentations. Second, identifying distinct clinical profiles of catathrenia might be beneficial for personalized therapies in the future. However, there are several limitations of the study. First, all the participants included in the study came from two independent sleep centers, indicating moderate referral bias. The sample size is relatively large for catathrenia. However, it is important to acknowledge that a larger sample size would have potentially yielded more accurate results. Second, the participants in the study were Asian, and racial and ethnic factors were not considered. It is important to note that this study did not cover all possible clinical presentations of catathrenia, including associated symptoms, comorbidities, and acoustic characteristics of groaning sounds. This is because the symptoms exhibited by patients with catathrenia were quite diverse, and the sample size of the study was relatively insufficient for thorough analysis. The robustness and generalizability of phenotypes identified in the study need to be verified in future investigations with more diverse samples.
Conclusion
Two distinct phenotypes were identified in patients with catathrenia, primary catathrenia and catathrenia associated with upper airway obstruction, suggesting respiratory events and upper airway structures might be related to the etiology of catathrenia, with implications for its treatment. There might exist a close association between catathrenia and OSA.
Statement of Significance
The clinical manifestations including polysomnographic characteristics and upper airway evaluations of catathrenia (nocturnal groaning) have been heterogeneous, possibly due to various disease subtypes. In this study, we used K-mean cluster analysis on 66 patients diagnosed with catathrenia to explore phenotypes and identified two distinct clusters of catathrenia, primary catathrenia, and catathrenia associated with upper airway obstruction. Patients’ sex, respiratory and groaning events, and upper airway dimension differ between subgroups. It is suggested respiratory events and upper airway structures might be related to the etiology of catathrenia, with implications for its treatment.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We thank all the patients who participated in the study.
Data Sharing Statement
The data underlying this article cannot be shared publicly for the privacy of individuals who participated in the study. The data will be shared on reasonable request to the corresponding author.
Additional information
Funding
References
- American Acadamy of Sleep Medicine. The International Classification of Sleep Disorders, Diagnostic and Coding Manual. Westchester, IL: American Acadamy of Sleep Medicine; 2005:165–167.
- Alonso J, Camacho M, Chhetri DK, Guilleminault C, Zaghi S. Catathrenia (nocturnal groaning): a social media survey and state-of-the-art review. Revi J Clini Sleep Med. 2017;13(4):613–622. doi:10.5664/jcsm.6556
- De Roeck J, Van Hoof E, Cluydts R. Sleep-related expiratory groaning: a case report. Sleep Res. 1983;12(237):295–307.
- Pevernagie DA, Boon PA, Mariman AN, Verhaeghen DB, Pauwels RA. Vocalization during episodes of prolonged expiration: a parasomnia related to REM sleep. Article Sleep Medicine. 2001;2(1):19–30. doi:10.1016/S1389-9457(00)00039-3
- Vetrugno R, Provini F, Plazzi G, Vignatelli L, Lugaresi E, Montagna P. Catathrenia (nocturnal groaning): a new type of parasomnia. Neurology. 2001;56(5):681–683. doi:10.1212/wnl.56.5.681
- Brunner DP, Gonzalez HL. Catathrenia: a rare parasomnia with prolonged groaning during clusters of central or mixed apneas. J Sleep Res. 2004;13(Suppl. 1):1.
- Oldani A, Manconi M, Zucconi M, Castronovo V, Ferini-Strambi L. ‘Nocturnal groaning’: just a sound or parasomnia? Article. Journal of Sleep Research. 2005;14(3):305–310. doi:10.1111/j.1365-2869.2005.00460.x
- Grigg-Damberger M, Brown LK, Casey KR. A cry in the night: nocturnal moaning in a 12-year-old boy. Sleep-related groaning (Catathrenia). J Clinical Sleep Med. 2006;2(3):354–357.
- Guilleminault C, Hagen CC, Khaja AM. Catathrenia: parasomnia or uncommon feature of sleep disordered breathing? Article. Sleep. 2008;31(1):132–139. doi:10.1093/sleep/31.1.132
- Manconi M, Zucconi M, Carrot B, Ferri R, Oldani A, Ferini-Strambi L. Association between bruxism and nocturnal groaning. Article. Mov Disord. 2008;23(5):737–739. doi:10.1002/mds.21885
- Iriarte J, Alegre M, Urrestarazu E, Viteri C, Arcocha J, Artieda J. Continuous positive airway pressure as treatment for catathrenia (nocturnal groaning). Article. Neurology. 2006;66(4):609–610. doi:10.1212/01.WNL.0000198503.93340.10
- Salhan D, Relia S, Dayyat E, Schoumacher R, Freire AX. Teenager with a noisy breathing in sleep-A rare case of catathrenia. Sleep. 2018;41:A420.
- Prihodova I, Sonka K, Kemlink D, Volna J, Nevsimalova S. Arousals in nocturnal groaning. Article. Sleep Med. 2009;10(9):1051–1055. doi:10.1016/j.sleep.2008.09.019
- Muraki H, Okura M, Imai R, et al. Temporal relationship between EEG arousal, bruxism and nocturnal groaning (Catathrenia). Sleep Medicine. 2011; 12:S39.
- Øverland B, Akre H, Berdal H, Skatvedt O. Sleep-related groaning: prevalence and characteristics in a cohort of patients with suspected obstructive sleep apnea. Acta Otolaryngol. 2012;132(1):90–95. doi:10.3109/00016489.2011.624119
- Gomez T, Casal A, De Miguel M, Rodriguez PR, Acevedo MFT, De Blas FE. Catathrenia resolved with the lowest CPAP pressure settings. Pulmonology. 2020;26(2):107–110. doi:10.1016/j.pulmoe.2019.07.010
- Yu M, Wen Y, Xu L, Han F, Gao X. Polysomnographic characteristics and acoustic analysis of catathrenia (nocturnal groaning). Physiol Meas. 2020;41(12):125012. doi:10.1088/1361-6579/abd235
- Songu M, Yilmaz H, Yuceturk AV, Gunhan K, Ince A, Bayturan O. Effect of CPAP therapy on catathrenia and OSA: a case report and review of the literature. Article Sleep Breath. 2008;12(4):401–405. doi:10.1007/s11325-008-0194-6
- Hoey L. Catathrenia: did you hear that?! Conference Abstract. Sleep Biol Rhythms. 2015;13:90. doi:10.1111/sbr.12132
- Yu M, Hao Z, Xu L, Wen Y, Han F, Gao X. Mandibular advancement device as treatment trial for catathrenia (nocturnal groaning). J Clinical Sleep Med. 2021;17(9):1767–1776. doi:10.5664/jcsm.9290
- American Academy of Sleep Medicine. International Classification of Sleep Disorders. Darien, IL: American Academy of Sleep Medicine; 2014.
- Iriarte J, Campo A, Alegre M, Fernandez S, Urrestarazu E. Catathrenia: respiratory disorder or parasomnia? Sleep Med. 2015;16(7):827–830. doi:10.1016/j.sleep.2014.12.026
- Pevernagie DA. Why catathrenia is a parasomnia. Editorial. Sleep Med. 2017;32:227–228. doi:10.1016/j.sleep.2016.11.008
- Benjamins JS, Migliorati F, Dekker K, et al. Insomnia heterogeneity: characteristics to consider for data-driven multivariate subtyping. Sleep Med Rev. 2017;36:71–81. doi:10.1016/j.smrv.2016.10.005
- Gool JK, Zhang Z, Oei M, et al. Data-Driven Phenotyping of Central Disorders of Hypersomnolence With Unsupervised Clustering. Neurology. 2022;98(23):e2387–e2400. doi:10.1212/WNL.0000000000200519
- Ye L, Pien GW, Ratcliffe SJ, et al. The different clinical faces of obstructive sleep apnoea: a cluster analysis. Europ resp J. 2014;44(6):1600–1607. doi:10.1183/09031936.00032314
- Keenan BT, Kim J, Singh B, et al. Recognizable clinical subtypes of obstructive sleep apnea across international sleep centers: a cluster analysis. Sleep. 2018;41(3). doi:10.1093/sleep/zsx214
- Kim J, Keenan BT, Lim DC, Lee SK, Pack AI, Shin C. Symptom-based subgroups of Koreans with obstructive sleep apnea. J Clinical Sleep Med. 2018;14(3):437–443. doi:10.5664/jcsm.6994
- Mazzotti DR, Keenan BT, Lim DC, Gottlieb DJ, Kim J, Pack AI. Symptom subtypes of obstructive sleep apnea predict incidence of cardiovascular outcomes. Am J Respir Crit Care Med. 2019;200(4):493–506. doi:10.1164/rccm.201808-1509OC
- Joosten SA, Hamza K, Sands S, Turton A, Berger P, Hamilton G. Phenotypes of patients with mild to moderate obstructive sleep apnoea as confirmed by cluster analysis. Respirology. 2012;17(1):99–107. doi:10.1111/j.1440-1843.2011.02037.x
- Lacedonia D, Carpagnano GE, Sabato R, et al. Characterization of obstructive sleep apnea-hypopnea syndrome (OSA) population by means of cluster analysis. J Sleep Res. 2016;25(6):724–730. doi:10.1111/jsr.12429
- Nakayama H, Kobayashi M, Tsuiki S, Yanagihara M, Inoue Y. Obstructive sleep apnea phenotypes in men based on characteristics of respiratory events during polysomnography. Sleep & Breathing = Schlaf & Atmung. 2019;23(4):1087–1094. doi:10.1007/s11325-019-01785-8
- Kim JW, Won TB, Rhee CS, Park YM, Yoon IY, Cho SW. Polysomnographic phenotyping of obstructive sleep apnea and its implications in mortality in Korea. Sci Rep. 2020;10(1):13207. doi:10.1038/s41598-020-70039-5
- Vavougios GD, George DG, Pastaka C, Zarogiannis SG, Gourgoulianis KI. Phenotypes of comorbidity in OSAS patients: combining categorical principal component analysis with cluster analysis. J Sleep Res. 2016;25(1):31–38. doi:10.1111/jsr.12344
- Turino C, Bertran S, Gavalda R, et al. Characterization of the CPAP-treated patient population in Catalonia. PLoS One. 2017;12(9):e0185191. doi:10.1371/journal.pone.0185191
- Zinchuk AV, Jeon S, Koo BB, et al. Polysomnographic phenotypes and their cardiovascular implications in obstructive sleep apnoea. Thorax. 2018;73(5):472–480. doi:10.1136/thoraxjnl-2017-210431
- An HJ, Baek SH, Kim SW, Kim SJ, Park YG. Clustering-based characterization of clinical phenotypes in obstructive sleep apnoea using severity, obesity, and craniofacial pattern. Eur J Orthod. 2020;42(1):93–100. doi:10.1093/ejo/cjz041
- Kim SJ, Alnakhli WM, Alfaraj AS, Kim KA, Kim SW, Liu SY. Multi-perspective clustering of obstructive sleep apnea towards precision therapeutic decision including craniofacial intervention. Sleep & Breathing = Schlaf & Atmung. 2021;25(1):85–94. doi:10.1007/s11325-020-02062-9
- Huang L, Xu Y, Gong X, Gao X. Anatomical phenotype of obstructive sleep apnea patients based on cluster analysis. Orthod Craniofac Res. 2023;26:608–617. doi:10.1111/ocr.12653
- Xu PH, Fong DYT, Lui MMS, Lam DCL, Ip MSM. Cardiovascular outcomes in obstructive sleep apnoea and implications of clinical phenotyping on effect of CPAP treatment. Thorax. 2023;78(1):76–84. doi:10.1136/thoraxjnl-2021-217714
- Gagnadoux F, Le Vaillant M, Paris A, et al. Relationship Between OSA Clinical Phenotypes and CPAP Treatment Outcomes. Chest. 2016;149(1):288–290. doi:10.1016/j.chest.2015.09.032
- Saaresranta T, Hedner J, Bonsignore MR, et al. Clinical Phenotypes and Comorbidity in European Sleep Apnoea Patients. PLoS One. 2016;11(10):e0163439. doi:10.1371/journal.pone.0163439
- Pien GW, Ye L, Keenan BT, et al. Changing faces of obstructive sleep apnea: treatment effects by cluster designation in the Icelandic sleep apnea cohort. Sleep. 2018;41(3):1.
- Berry RB, Brooks R, Gamaldo CE, Harding SM, Marcus CL. Vaughn BV for the American Academy of Sleep Medicine. The AASM coding manual for the Scoring of Sleep and Associated Events: rules, Terminology and Technical Specifications, Version 2.0. In: www.aasmnet.org. Darien, Illinois: American Academy of Sleep Medicine; 2012.
- Drakatos P, Higgins S, Duncan I, et al. Catathrenia, a REM predominant disorder of arousal? Article. Sleep Med. 2017;32:222–226. doi:10.1016/j.sleep.2016.06.010
- Muraki H, Okura M, Kato T, Taniguchi M, Ohi M. A stereotyped sequence from EEG arousals to nocturnal groaning events with or without the intervening sleep bruxism in catathrenia. Article Sleep Medicine. 2017;32:1–3. doi:10.1016/j.sleep.2016.03.015
- Batool F, Hennig C. Clustering with the Average Silhouette Width. Comput Stat Data Anal. 2021;158:107190. doi:10.1016/j.csda.2021.107190
- Hao Z, Xu L, Zhang J, Lan X, Gao X, Han F. Anatomical characteristics of catathrenia (nocturnal groaning) in upper airway and orofacial structures. Article Sleep Breath. 2016;20(1):103–111. doi:10.1007/s11325-015-1191-1
- Yu M, Hao ZL, Xu LY, Wen YF, Han F, Gao XM. Craniofacial anatomical Characteristics of patients with catathrenia. Zhonghua Kou Qiang Yi Xue Za Zhi. 2023;58(7):659–669. doi:10.3760/cma.j.cn112144-20230429-00175
- Kim YH, Atwal P, Weinstein M, Cataletto M. Sleep-related catathrenia: an enigma. Chest. 2012;142(4):1. doi:10.1378/chest.1389913
- Ramar K, Olson EJ, Morgenthaler TIC. Article. Sleep Med. 2008;9(4):457–459. doi:10.1016/j.sleep.2007.08.011
- Dias C, Sousa L, Batata L, Teixeira F, Moita J, Moutinho Dos Santos J, CPAP treatment for catathrenia. Letter. Revista Portuguesa de Pneumologia. 2017;232:101–104. doi:10.1016/j.rppnen.2016.12.008
- Muraki H, Okura M, Sugita H, Ohi M, Taniguchi M. Is nocturnal groaning (catathrenia) a parasomnia or sleep related breathing disorder? Sleep. 2015;38:A205.
- Wen Y, Xu F, Dong X, et al. Catathrenia phenomenon are common in obstructive sleep apnea. Proceedings of 2021 3rd Congress of Asian Society of Sleep Medicine & The 13th Symposium of Chinese Sleep Research Society; 2021.
- Abbasi AA, Morgenthaler TI, Slocumb NL, Tippmann-Peikert M, Olson EJ, Ramar K. Nocturnal moaning and groaning - Catathrenia or nocturnal vocalizations. Article Sleep Breath. 2012;16(2):367–373. doi:10.1007/s11325-011-0503-3
- Dias C, Sousa L, Batata L, Teixeira MF, Santos JM. Catathrenia: a 10 year revision. Europ Respirat J. 2015;46:1. doi:10.1183/13993003.congress2015.PA2381.
- Poli F, Ricotta L, Vandi S, et al. Catathrenia under sodium oxybate in narcolepsy with cataplexy. Article Sleep Breath. 2012;16(2):427–434. doi:10.1007/s11325-011-0520-2
- Kazaglis L. The value of a well-trained ear: incidental detection of catathrenia on home sleep apnea tests in patients with low probability for obstructive sleep apnea. J Clinical Sleep Med. 2018;14(12):2083–2086. doi:10.5664/jcsm.7544
- Siddiqui F, Walters AS, Chokroverty S. Catathrenia: a rare parasomnia which may mimic central sleep apnea on polysomnogram. Article Sleep Medicine. 2008;9(4):460–461. doi:10.1016/j.sleep.2007.10.012