
Abstract
Approximately 50% of all pregnancies in women with epilepsy (WWE) occur unplanned. This is worrying, given the increased occurrence of obstetrical complications in WWE, including the risk of seizures and their possible consequences for both the mother and the unborn child. Hormonal contraception is usually regarded as highly effective, but it is subject to numerous bidirectional drug interactions with several antiepileptic drugs. These interactions may lead to loss of seizure control or contraceptive failure. Further concerns are loss of bone mineral density and increased seizure activity due to hormonal effects. Many physicians lack sufficient knowledge regarding these issues, and most WWE have never received adequate counseling. Moreover, several studies show that a large proportion of WWE do not take their medicines regularly. This article reviews all of these issues and offers practical recommendations for the management of contraception in WWE.
Introduction
With an estimated prevalence of 0.3%–0.7%, epilepsy is one of the most frequent neurological diseases.Citation1 Women with epilepsy (WWE), like healthy women, use different kinds of contraceptive methods, ie, hormonal contraception (HC), intrauterine devices (IUDs), barrier methods, or combinations of them. HC includes combined oral contraceptives (COCs), progestin-only pills, intramuscular injections, subdermal implants, skin patches, hormone-releasing IUDs, and vaginal rings. However, most WWE also use antiepileptic drugs (AEDs). Many of these drugs do interact with HC, which may lead to contraceptive failure or impaired seizure control.Citation2,Citation3 Either of these complications may have serious social, psychological, professional, and economic consequences. Additionally, many AEDs possess teratogenic potential and/or may exert a negative impact on cognitive and psychomotor skills of children exposed to these AEDs in the womb.Citation4–Citation6
Given the above, it is deeply concerning that ∼50% of all pregnancies among WWE occur unintended.Citation7,Citation8 This is about the same proportion as found in the general population.Citation9,Citation10 Risk factors for unintended pregnancy include low socioeconomic status, low education, and ethnicity.Citation8 Also, only half of all WWE using contraception do so with a highly effective method (HC, IUDs, or surgery). Moreover, many WWE use enzyme-inducing AEDs that may impair the efficacy of highly effective HC.Citation8
It might be speculated whether better education of WWE could reduce the proportion of unplanned pregnancies. However, several studies show that a large proportion of doctors, including neurologists and gynecologists, lack sufficient knowledge about reproductive health issues of WWE and how these may be affected by AEDs.Citation11–Citation13 Hence, the current treatment guidelines may not be followed.Citation14 More recent surveys found a trend from prescribing older AEDs toward newer AEDs with a more favorable interaction and safety profile, which may indicate a growing awareness among doctors.Citation15–Citation18 However, most WWE do not receive necessary information.Citation19,Citation20 A 2015 survey found that <7% of women received contraceptive counseling.Citation21 Even when information is provided, many WWE do not recall the information they were given.Citation22 Consequently, most WWE have only limited knowledge about interactions between HC and AEDs and potentially harmful effects of AEDs on the child.Citation23,Citation24
Apart from drug interactions between HC and AEDs, contraception for WWE comprises further questions. Does HC aggravate seizures? Is there an increased risk of osteoporosis? Is adherence an issue? The answers to these questions affect treatment options and need to be discussed with the patient. Hence, the attending physician should have thorough knowledge.
Epilepsy, AEDs, and female fertility
While many WWE will have normal sex lives and normal pregnancies, they in general have lower fertility rates than healthy women. Also, anovulatory cycles, irregular menstrual bleedings, or oligo-/amenorrhea occur more frequently in WWE than in women without epilepsy.Citation25 This is more common with antiepileptic polytherapy than with monotherapy, which suggests a causal role of AEDs. However, available data also suggest that seizures and epileptic discharges, especially temporal lobe epilepsy, may negatively affect ovarian function and ovulation via disturbances in the hypothalamic–pituitary axis.Citation25–Citation27
It is well established that enzyme-inducing AEDs may increase sex hormone-binding globulin and induce the metabolism of sex steroid hormones, thus reducing the serum concentration of free and total sex hormones.Citation28,Citation29
Valproate, one of the most frequently used AEDs, can induce polycystic ovary syndrome.Citation30 This syndrome consists of polycystic ovaries, hyperandrogenism, menstrual disturbances, and anovulatory cycles. The underlying mechanisms are not completely understood, but an interaction of valproate with sex steroid synthesis and metabolism in the ovary is presumed.Citation25
WWE also have a higher risk for complications during pregnancy and delivery, eg, hypertension, preeclampsia, bleedings, preterm birth, or small for gestational age. The frequency of cesarean section is also higher.Citation31
In conclusion, current evidence suggests that both epilepsy itself as well as drug treatment with AEDs may affect female fertility and cause complications during pregnancy and delivery. These findings underline the importance of pregnancy planning, which includes contraception.
What AEDs do to HC
Many of the “old” or “first-generation” AEDs (phenytoin, phenobarbital, primidone, carbamazepine) and several of the “new” or “second-generation” AEDs (oxcarbazepine, eslicarbazepine, topiramate, felbamate, rufinamide, perampanel) have more or less pronounced enzyme-inducing effects. They may induce either cytochrome P450 (CYP) enzymes, uridine-diphosphate-glucuronosyltransferase (UGT) enzymes, or both, thereby accelerating the metabolism of steroid hormones. Contraceptive failure provoked by enzyme-inducing AEDs is common and may affect both oral and nonoral HC.Citation32–Citation34 The estrogen compound used in combined HC usually is ethinyl estradiol (EE), which has been used for decades. EE has a well-known pharmacokinetic and interaction profile. It is mainly metabolized by CYP 3A4, but conjugation by UGT also plays a role.Citation35 Besides EE, there is a plethora of older and newer progestins used for HC.Citation36,Citation37 Their metabolism and possible interactions with AEDs are much less studied. In general, their metabolism is inducible like that of EE. Thus, their contraceptive effect may fail when they are coadministered with carbamazepine or other enzyme-inducing AEDs. Examples for this include oral levonorgestrel, oral norethindrone, and the subdermal etonogestrel implant.Citation32,Citation33,Citation38,Citation39 The interaction potential of depot medroxyprogesterone acetate (DMPA) intramuscular injection has not been specifically studied. However, if an AED has been found to induce the metabolism of one specific progestin, it appears reasonable to assume that other progestins may be affected as well.
On the other hand, there are many different HC preparations available, and they may contain not only different hormones, but also different doses of EE and different doses of the same progestin. The conclusions drawn from one study investigating one HC preparation may not necessarily apply to another HC preparation with the same active substances but different doses. Hence, even if the available data suggest that an interaction is unlikely to occur in a specific HC–AED combination, the attending physician and the patient should take any irregular bleeding as a sign of possible contraceptive failure.
As a consequence of the pharmacokinetic interaction between enzyme-inducing AEDs and HC, the “classic” recommendation has been to use high-dose HC, ie, a daily EE dose of at least 50 µg.Citation40–Citation42 However, this advice is theoretically derived, has not been clinically proven, and has considerable conceptual weaknesses, one of them being that the ovulation-suppressing dose of EE is ∼100 µg.Citation43 Given the ever decreasing dose of EE in COCs, it may also be hard to find a contraceptive pill with such a high estrogen content. Moreover, despite this decades-old recommendation, a recent study from the Netherlands reported that 43.5% of WWE taking enzyme-inducing AEDs used a low dose of EE.Citation44 A similar study performed in the UK found even a figure of 56%.Citation12
More recent recommendations take into account the mechanism of action of modern HC and focus on a high progestin dose instead, since in modern HC preparations, ovulation inhibition is mediated via the progestin, not EE.Citation43 Modern HC contains EE mainly for the purpose of creating a hormonal balance with the progestin component. Indeed, modern oral HC preparations typically contain ∼1.5–2 times the ovulation-inhibiting progestin dose.Citation43 However, as enzyme induction affects not only EE but also progestins,Citation45 even the contraceptive effect of a “high” progestin dose may be impaired by enzyme-inducing AEDs, and clinical evidence for the “high progestin” concept is lacking. Consequently, neither high-dose EE nor high-dose progestin guarantees safe contraception in WWE taking enzyme-inducing AEDs, and additional contraceptive measures, eg, barrier methods, should be considered. This applies to combined (EE plus progestin) as well as progestin-only HC (oral or depot-formulations).
Hormone-releasing IUDs release a progestin and act locally on the endometrium. In contrast to systemic HC (oral, patch, vaginal ring, or implants), their contraceptive effect may not – at least in theory – be impaired by hepatic enzyme induction. Preliminary data from one study indeed suggest that this method is not affected by AEDs, which would make them a suitable alternative to systemic HC.Citation46 However, this study has not been confirmed. There is also one case report on contraceptive failure with a progestin-releasing intracervical device, presumably due to simultaneous use of carbamazepine.Citation47 However, there are no further such reports. Nevertheless, caution is advisable until possible interactions of locally acting HC with enzyme-inducing AEDs have been studied more systematically.
The most obvious solution to this drug interaction problem would be to not use enzyme-inducing AEDs together with HC. With today’s spectrum of available AEDs (>20 in most Western countries), chances for the neurologist to avoid enzyme- inducing AEDs in fertile WWE are good. Indeed, recent surveys indicate that more and more WWE are prescribed newer, nonenzyme-inducing AEDs.Citation15–Citation18 In many countries however, these new AEDs may either not be available or just be too expensive. One of the “old”, nonenzyme-inducing AEDs is valproate. It is very effective in a large variety of epileptic seizures and syndromes, usually well-tolerated, inexpensive, and a first-line drug for the treatment of epilepsy. It is one of the most used AEDs worldwide. Alas, it has considerable teratogenic potential and may negatively affect the cognitive outcome of children exposed in utero.Citation5,Citation6 This is a substantial risk, especially because half of all pregnancies in WWE occur unplanned. Moreover, typical side effects of valproate include hair loss and weight gain. Valproate may also cause polycystic ovary syndrome and metabolic disturbances. It is therefore prescribed less frequently for WWE,Citation15–Citation18 and the European Medicines Agency has advised physicians to not prescribe valproate to fertile women unless other treatments are ineffective or not tolerated.Citation48 If valproate is prescribed to fertile women, highly effective contraception and adequate adherence should be ensured.
When enzyme-inducing AEDs cannot be avoided, HC should be combined with barrier methods. Recently, it has also been recommended to use HC in an extended-cycle pattern when enzyme-inducing AEDs are used simultaneously.Citation43 Without the pill-free week, gonadotropin secretion and ovarian function will be continuously suppressed, which will enhance contraceptive efficacy compared to the usual pattern of use (3 weeks “on”, 1 week “off ”). Whether this alone provides reliable contraception despite enzyme induction remains to be proven. Until then, HC should be regarded as non-safe when combined with enzyme-inducing AEDs, and additional contraceptive methods (barrier methods) be employed.
In any case, WWE using enzyme-inducing AEDs and HC must be informed of this problem and possible solutions be presented, so that they can make an informed decision on which contraceptive method (and/or which AED) to choose. It may also be helpful to discuss this issue directly with the patient’s neurologist.
What HC does to AEDs
While it has been known for over 40 years that enzyme-inducing AEDs may impair the contraceptive effect of HC,Citation49,Citation50 the possibility of the opposite had practically been ignored until 2001, when it was demonstrated that COCs may reduce the serum levels of lamotrigine by >60% and lead to loss of seizure control.Citation51 Later studies confirmed these findings and showed that it is the estrogen component (EE) that is responsible for this interaction.Citation52,Citation53 In fact, it has been known long before 2001 that EE may affect the metabolism of quite many other drugs.Citation54,Citation55 Interestingly, EE has a unique dual effect on drug-metabolizing enzymes: while the activity of several CYP enzymes may be reduced, the activity of some UGTs may be increased.Citation54 Thus, the clinical efficacy of AEDs that undergo elimination by glucuronidation may be reduced. Surprisingly, studies on the possible effects of EE on the metabolism of AEDs are still sparse.
So far, an effect of EE on the metabolism of AEDs has been demonstrated only for lamotrigine (discussed in Lamotrigine section) and, to a lesser degree, for valproate. In contrast to lamotrigine, the effect on valproate is only moderate and much less well documented (only two small studies).Citation56,Citation57 However, as with lamotrigine, there is large interindividual variation, and in some patients this interaction may gain clinical relevance, ie, lead to increased seizure activity.Citation57 Oxcarbazepine and its derivative eslicarbazepine, as well as retigabine/ezogabine, are also subject to glucuronidation, but a possible effect of EE on their metabolism has not been examined so far.
It must be emphasized that, according to the current knowledge, only EE affects the metabolism of AEDs. There is no convincing data suggesting any clinically relevant effect of progestins (“mini-pill”, implants, depot injections, hormonal IUDs, emergency pill) on the metabolism of lamotrigine or any other AED. In one small study, a desogestrel-only pill caused a 20%–100% increase in lamotrigine concentrations, but only in seven out of ten women.Citation58 However, this study from the year 2004 still exists only in an abstract form and it has not been confirmed by others.
It should also be noted that EE is used not only in oral preparations (COCs) but also in skin patches and the vaginal ring. Accordingly, it has been found that the EE-releasing vaginal ring may reduce lamotrigine serum concentrations in a similar manner as COCs.Citation52,Citation59 Although not specifically studied, such an effect should also be anticipated for the EE-releasing skin patch.
Lamotrigine
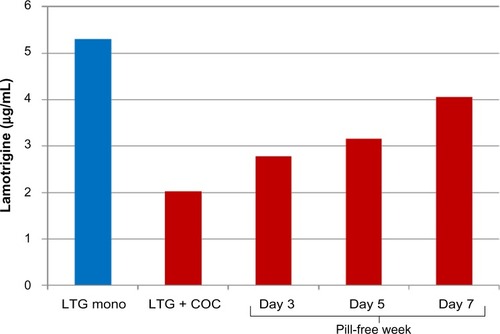
Lamotrigine is metabolized by UGT enzymes that are inducible by EE. The use of EE together with lamotrigine may become challenging. First, lamotrigine concentrations fall by ∼50%–60% and seizure aggravation may occur when EE is added.Citation51–Citation53 This usually requires a considerable increase, and often a doubling, of the lamotrigine dose, in order to avoid seizure breakthrough. Second, lamotrigine levels rise (with considerable interindividual variation) and may even double within the pill-free week.Citation53,Citation59,Citation60 This may provoke or aggravate adverse effects if the dose is not reduced during this period (). In clinical practice though, most WWE will not experience relevant problems with side effects in the pill-free week. Finally, lamotrigine has a comparatively long half-life of 20–30 hours, which means that the pharma cokinetic steady state after dose changes or addition/removal of interacting comedication will be achieved first after 4–5 days.
Figure 1 Impact of addition and withdrawal of combined oral contraception on lamotrigine (LTG) serum concentration.
Abbreviation: COC, combined oral contraceptive; mono, monotherapy.
Together, all this means that COC users may have large fluctuations of the lamotrigine serum concentration during the menstrual cycle, with the possibility of both subtherapeutic and toxic levels, if the dose remains unchanged all the time. Likewise, because of the large fluctuations, serum-level measurements of lamotrigine may be considerably misleading if not always taken exactly at the same time relative to the menstrual cycle.
If active measures become necessary, dynamic dose adjustments (increase while EE is taken, decrease in the pill-free week) might prevent the loss of seizure control or the occurrence of adverse effects, but such a strategy is unrealistic as it would require great efforts from the attending neurologist and the patient, including tight clinical follow-up and regular measurement of the lamotrigine serum level over a long period of time.
All in all, the combination of lamotrigine with EE (COCs, patch, or vaginal ring) appears unfavorable. When this combination cannot be avoided, a practical solution would be to omit the pill-free week, ie, to use EE continuously. This would require only one initial dose adjustment of lamotrigine. Such “long-cycle” or “extended-cycle” regimens have been proven safe and convenient, and are becoming increasingly popular among fertile women.Citation61,Citation62 Recently, a COC designed for an 84-day regimen that results in bleeding only four times a year has been introduced. HC preparations for even longer cycles, 6 and 12 months, are currently being developed.Citation62
As stated earlier, progestins apparently do not affect lamotrigine metabolism. These preparations may therefore be preferred over EE-containing HC when the patient uses lamotrigine. One caveat exists though. It has been found in one study that lamotrigine reduced the area under the curve of levonorgestrel by 19%. This is a comparatively small effect, and the authors conclude from low progesterone serum concentrations that suppression of ovulation still was maintained.Citation53 No case of contraceptive failure due to lamotrigine has been published so far. However, it cannot be ruled out that in some patients, the contraceptive effect may become uncertain. Caution is therefore advisable, especially with low-dose progestin preparations ().
Table 1 Pharmacokinetic interactions between HC and AEDs
Does HC affect epilepsy?
The complex interaction between sexual hormones and epileptic brain activity has recently been reviewed.Citation27 In general, neuronal excitability is increased by estrogens and reduced by progesterone. There are certain exceptions to this rule,Citation27 but estrogens are mainly regarded as proconvulsants while progesterone is ascribed to anticonvulsant effects. This is also illustrated by the phenomenon of catamenial epilepsy, ie, epileptic seizures that occur predominantly in certain phases of the menstrual cycle.Citation63 Neuroactive, progesterone-derived steroids, such as allopregnanolone and ganaxolone, are being clinically studied for their potential as AEDs.Citation64 So far, although HC has been used for ∼50 years now, there is no conclusive evidence supporting the idea that EE or HC in general may aggravate epileptic seizures.Citation65–Citation67
Osteoporosis and bone fracture risk
It has long been known that patients taking enzyme-inducing AEDs (phenytoin, phenobarbital, carbamazepine, topiramate, and others) are at a significantly higher risk for developing osteoporosis.Citation68,Citation69 HC has also been associated with decreased bone mineral density and increased risk of fractures. This is best documented for DMPA, particularly when used for more than 2 years. Regarding the effects of other contraceptive progestins or EE, recent meta-analyses conclude that data still are conflicting despite a large number of published studies.Citation70–Citation72 Some, but not all, studies show that EE may reduce bone mineral density, although this effect may depend on dose and/or treatment duration. Patients must be informed about this issue. Most importantly, the effects of HC (especially DMPA) and enzyme-inducing AEDs on bone mineral density may add up, which is another reason to avoid this problematic combination.
Adherence
Even the best drug treatment regimen will not work properly if the drug is not used as prescribed. Adherence to long-term therapy for chronic illnesses averages as low as 50% in developed countries. This includes potentially life-threatening conditions such as diabetes, asthma, or epilepsy. In developing countries, the rate is even lower.Citation73,Citation74 Irregular drug intake is also very common among HC users. Different studies found that up to 71% of women using COCs were taking their pills irregularly.Citation75,Citation76 These numbers match well with population studies demonstrating that approximately half of all pregnancies occur unintended.Citation9 Once a woman becomes pregnant, marked physiologic changes occur, including increased metabolic capacity, increased renal blood flow, and increased volume of distribution. Accordingly, it has been shown for several AEDs that their serum levels decrease by half during pregnancy, often leading to breakthrough seizures. Moreover, many patients may fear harmful effects to their unborn child and stop taking their antiepileptic medication once they discover that they are pregnant. Given the serious and potentially fatal consequences of uncontrolled epilepsy for both the mother and the unborn child, as well as the significant risk of harmful pre- and postnatal effects that several AEDs may have on the child, unplanned pregnancy in WWE should be avoided and adherence be improved.
Many factors are negatively correlated with adherence; some of them are difficult to change, such as socioeconomic status, low education, ethnicity, or co-payments.Citation77 Apart from such factors, it may seem obvious that better patient education is a key factor to improve patient adherence. However, a large proportion of doctors lack the necessary knowledge, and many patients never receive adequate information.Citation11–Citation14,Citation19–Citation24 Also, although knowledge among doctors and patient education may have improved somewhat during recent years, still only half of WWE are able to recall the information they have been given.Citation14 A recent study in WWE showed that an educational intervention using an informational handout led to increased knowledge on HC and drug interactions with AEDs, compared to standard information without the handout, although this effect was time limited.Citation78 However, sufficient knowledge alone may not guarantee a high degree of adherence, as it has been found in a recent study that the level of knowledge was the same among adherent and non-adherent patients with epilepsy (Samsonsen C, Trondheim, Norway, unpublished data). It might therefore be speculated that many patients simply forget to take their medication. Indeed, it has been demonstrated that regular reminders such as an alarm app on the smartphone, text messages, or a digital pill dispenser improve regular pill intake significantly.Citation79,Citation80
Thus, in addition to purely educative measures, continuous follow-up of the patient, behavioral interventions, and systematic reminders (in the office, via telephone or mail/e-mail, smartphone apps, or digital pill dispensers) may be useful to improve adherence and regular drug intake.Citation81,Citation82
Practical recommendations
In patients taking AEDs that interact with HC (phenytoin, phenobarbital, primidone, carbamazepine, topiramate, oxcarbazepine, eslicarbazepine, felbamate, rufinamide, perampanel): add other form for contraception (eg, barrier method, IUD, or a combination of them) or alternatively, discuss with the patient’s neurologist if switching to a nonenzyme-inducing AED is possible.
In patients taking lamotrigine: avoid HC that contains EE (COCs, patch, vaginal ring) or alternatively, omit EE-free week (extended-cycle regimen).
Inform and educate patient well on: available contraceptive methods and their strengths and weaknesses; frequency and possible consequences of nonadherence; possible drug interactions between AEDs and HC; and possible pre- and postnatal adverse effects of antiepileptic medication: size and nature of teratogenic risks of AEDs and possible negative cognitive effects of AEDs.
Advocate for long-acting nonoral contraceptive measures (IUD, implant) to avoid risk of missed pills.
If the patient prefers oral contraception, suggest to use smartphone app (pill-reminder), digital tablet dispenser, or other measures to minimize number of missed pills.
Schedule frequent follow-ups (in the office, via phone, or via mail/e-mail) and repeat given information (may be done by trained nurses).
Establish regular communication with the patient’s neurologist.
Keep yourself updated on drug interactions with HC.
Disclosure
The author reports no conflicts of interest in this work.
References
- BanerjeePNFilippiDAllen HauserWThe descriptive epidemiology of epilepsy-a reviewEpilepsy Res2009851314519369037
- GaffieldMECulwellKRLeeCRThe use of hormonal contraception among women taking anticonvulsant therapyContraception2011831162921134499
- ReimersABrodtkorbESabersAInteractions between hormonal contraception and antiepileptic drugs: clinical and mechanistic considerationsSeizure201528667025843765
- TomsonTXueHBattinoDMajor congenital malformations in children of women with epilepsySeizure201528465025777785
- CohenMJMeadorKJBrowningNNEAD study groupFetal antiepileptic drug exposure: adaptive and emotional/behavioral functioning at age 6 yearsEpilepsy Behav201329230831524012508
- CummingsCStewartMStevensonMMorrowJNelsonJNeurodevelopment of children exposed in utero to lamotrigine, sodium valproate and carbamazepineArch Dis Child201196764364721415043
- FairgrieveSDJacksonMJonasPPopulation based, prospective study of the care of women with epilepsy in pregnancyBMJ2000321726267467510987772
- DavisARPackAMKritzerJYoonACamusAReproductive history, sexual behavior and use of contraception in women with epilepsyContraception200877640540918477488
- SinghSSedghGHussainRUnintended pregnancy: worldwide levels, trends, and outcomesStud Fam Plann201041424125021465725
- FinerLBZolnaMRUnintended pregnancy in the United States: incidence and disparities, 2006Contraception201184547848522018121
- KraussGLBrandtJCampbellMPlateCSummerfieldMAntiepileptic medication and oral contraceptive interactions: a national survey of neurologists and obstetriciansNeurology1996466153415398649543
- ShorvonSDTallisRCWallaceHKAntiepileptic drugs: coprescription of proconvulsant drugs and oral contraceptives: a national study of antiepileptic drug prescribing practiceJ Neurol Neurosurg Psychiatry200272111411511784837
- MorrellMJSartoGEShaferPOBordaEAHerzogACallananMHealth issues for women with epilepsy: a descriptive survey to assess knowledge and awareness among healthcare providersJ Womens Health Gend Based Med20009995996511103095
- KampmanMTJohansenSVStenvoldHAcharyaGManagement of women with epilepsy: are guidelines being followed? Results from case-note reviews and a patient questionnaireEpilepsia20054681286129216060941
- ManSLPetersenIThompsonMNazarethIAntiepileptic drugs during pregnancy in primary care: a UK population based studyPLoS One2012712e5233923272239
- MeadorKJPenovichPBakerGANEAD Study GroupAntiepileptic drug use in women of childbearing ageEpilepsy Behav200915333934319410654
- NicholasJMRidsdaleLRichardsonMPAshworthMGullifordMCTrends in antiepileptic drug utilisation in UK primary care 1993–2008: cohort study using the General Practice Research DatabaseSeizure201221646647022608976
- VajdaFJHollingworthSGrahamJChanging patterns of antiepileptic drug use in pregnant Australian womenActa Neurol Scand20101212899320015108
- CrawfordPHudsonSUnderstanding the information needs of women with epilepsy at different lifestages: results of the ‘Ideal World’ surveySeizure200312750250712967580
- RussellAJMacphersonHCairnieVBrodieMJThe care of pregnant women with epilepsy – a survey of obstetricians in ScotlandSeizure1996542712778952012
- BhaktaJBainbridgeJBorgeltLTeratogenic medications and concurrent contraceptive use in women of childbearing ability with epilepsyEpilepsy Behav201552pt A21221726460786
- BellGSNashefLKendallSInformation recalled by women taking antiepileptic drugs for epilepsy: a questionnaire studyEpilepsy Res200252213914612458030
- PackAMDavisARKritzerJYoonACamusAAntiepileptic drugs: are women aware of interactions with oral contraceptives and potential teratogenicity?Epilepsy Behav200914464064419435578
- ManskiRDennisAA mixed-methods exploration of the contraceptive experiences of female teens with epilepsySeizure201423862963524878105
- VerrottiAD’EgidioCMohnACoppolaGParisiPChiarelliFAntiepileptic drugs, sex hormones, and PCOSEpilepsia201152219921121204821
- CummingsLNGiudiceLMorrellMJOvulatory function in epilepsyEpilepsia19953643553597607113
- TaubollESvebergLSvalheimSInteractions between hormones and epilepsySeizure20152831125765693
- IsojarviJILaatikainenTJPakarinenAJJuntunenKTMyllylaVVMenstrual disorders in women with epilepsy receiving carbamazepineEpilepsia19953676766817555984
- LossiusMITaubollEMowinckelPMorkridLGjerstadLReversible effects of antiepileptic drugs on reproductive endocrine function in men and women with epilepsy – a prospective randomized double-blind withdrawal studyEpilepsia200748101875188217555526
- HuXWangJDongWFangQHuLLiuCA meta-analysis of polycystic ovary syndrome in women taking valproate for epilepsyEpilepsy Res2011971–2738221820873
- BorthenIObstetrical complications in women with epilepsySeizure201528323425843764
- LangeJTealSTocceKDecreased efficacy of an etonogestrel implant in a woman on antiepileptic medications: a case reportJ Med Case Rep201484324517576
- SchindlbeckCJanniWFrieseKFailure of Implanon contraception in a patient taking carbamazepin for epilepsiaArch Gynecol Obstet2006273425525616208481
- BackDJGrimmerSFOrmeMLProudloveCMannRDBreckenridgeAMEvaluation of Committee on Safety of Medicines yellow card reports on oral contraceptive-drug interactions with anticonvulsants and antibioticsBr J Clin Pharmacol19882555275323408633
- ZhangHCuiDWangBPharmacokinetic drug interactions involving 17alpha-ethinylestradiol: a new look at an old drugClin Pharmacokinet200746213315717253885
- KuhlHPharmacology of estrogens and progestogens: influence of different routes of administrationClimacteric20058suppl 1363
- StanczykFZPharmacokinetics and potency of progestins used for hormone replacement therapy and contraceptionRev Endocr Metab Disord20023321122412215716
- RosenfeldWEDooseDRWalkerSANayakRKEffect of topiramate on the pharmacokinetics of an oral contraceptive containing norethindrone and ethinyl estradiol in patients with epilepsyEpilepsia19973833173239070594
- DavisARWesthoffCLStanczykFZCarbamazepine coadministration with an oral contraceptive: effects on steroid pharmacokinetics, ovulation, and bleedingEpilepsia201152224324721204827
- MattsonRHCramerJADarneyPDNaftolinFUse of oral contraceptives by women with epilepsyJAMA198625622382403723710
- CrawfordPChadwickDJMartinCTjiaJBackDJOrmeMThe interaction of phenytoin and carbamazepine with combined oral contraceptive steroidsBr J Clin Pharmacol19903068928962126946
- Practice parameter: management issues for women with epilepsy (summary statement). Report of the Quality Standards Subcommittee of the American Academy of NeurologyNeurology19985149449489781510
- SchwenkhagenAMStodieckSRWhich contraception for women with epilepsy?Seizure200817214515018178110
- WangHBosJHde Jong-van den BergLTCo-prescription of antiepileptic drugs and contraceptivesContraception2012851283122067799
- HaukkamaaMContraception by Norplant subdermal capsules is not reliable in epileptic patients on anticonvulsant treatmentContraception19863365595653095023
- BoundsWGuillebaudJObservational series on women using the contraceptive Mirena concurrently with antiepileptic and other enzyme-inducing drugsJ Fam Plann Reprod Health Care2002282788012396777
- RatsulaKClinical performance of a levonorgestrel-releasing intracervical contraceptive device during the first year of useContraception19873666596663128429
- European Medicines Agency (EMA)CMDh Agrees to Strengthen Warnings on the Use of Valproate Medicines in Women and GirlsLondonEuropean Medicines Agency (EMA)2014 Vol EMA/709243/2014
- JanzDSchmidtDLetter: anti-epileptic drugs and failure of oral contraceptivesLancet1974178661113
- HillierKDrug interaction with oral contraceptivesFertil Contracept1978215812308946
- SabersABuchholtJMUldallPHansenELLamotrigine plasma levels reduced by oral contraceptivesEpilepsy Res2001471–215115411673029
- ReimersAHeldeGBrodtkorbEEthinyl estradiol, not progestogens, reduces lamotrigine serum concentrationsEpilepsia20054691414141716146436
- SidhuJJobSSinghSPhilipsonRThe pharmacokinetic and pharmacodynamic consequences of the co-administration of lamotrigine and a combined oral contraceptive in healthy female subjectsBr J Clin Pharmacol200661219119916433873
- ShenfieldGMOral contraceptives. Are drug interactions of clinical significance?Drug Saf19939121378347289
- BreckenridgeAMBackDJOrmeMInteractions between oral contraceptives and other drugsPharmacol Ther197973617626392564
- GalimbertiCAMazzucchelliIArbasinoCCaneviniMPFattoreCPeruccaEIncreased apparent oral clearance of valproic acid during intake of combined contraceptive steroids in women with epilepsyEpilepsia20064791569157216981874
- HerzogAGBlumASFarinaELValproate and lamotrigine level variation with menstrual cycle phase and oral contraceptive useNeurology2009721091191419273825
- SchwenkhagenAMStodieckSRGInteraction between lamotrigine and a progestin-only contraceptive pill containing desogestrel 75-µg (Cerazette)Epilepsia200445suppl 7144
- ContinMAlbaniFAmbrosettoGVariation in lamotrigine plasma concentrations with hormonal contraceptive monthly cycles in patients with epilepsyEpilepsia20064791573157516981875
- ChristensenJPetrenaiteVAttermanJOral contraceptives induce lamotrigine metabolism: evidence from a double-blind, placebo-controlled trialEpilepsia200748348448917346247
- EdelmanAMicksEGalloMFJensenJTGrimesDAContinuous or extended cycle vs. cyclic use of combined hormonal contraceptives for contraceptionCochrane Database Syst Rev20147CD004695
- BenagianoGCarraraSFilippiVSafety, efficacy and patient satisfaction with continuous daily administration of levonorgestrel/ethinylestradiol oral contraceptivesPatient Prefer Adherence2009313114319936155
- HerzogAGCatamenial epilepsy: update on prevalence, pathophysiology and treatment from the findings of the NIH Progesterone Treatment TrialSeizure201528182525770028
- BialerMJohannessenSILevyRHPeruccaETomsonTWhiteHSProgress report on new antiepileptic drugs: a summary of the Twelfth Eilat Conference (EILAT XII)Epilepsy Res20151118514125769377
- DuttonCFoldvary-SchaeferNContraception in women with epilepsy: pharmacokinetic interactions, contraceptive options, and managementInt Rev Neurobiol20088311313418929078
- MattsonRHRebarRWContraceptive methods for women with neurologic disordersAm J Obstet Gynecol19931686 pt 2202720328512048
- HardenCLLeppikIOptimizing therapy of seizures in women who use oral contraceptivesNeurology20066712 suppl 4S56S5817190925
- ShenCChenFZhangYGuoYDingMAssociation between use of antiepileptic drugs and fracture risk: a systematic review and meta-analysisBone20146424625324780876
- HahnTJBone complications of anticonvulsantsDrugs1976123201211789046
- LopezLMChenMMullins LongSCurtisKMHelmerhorstFMSteroidal contraceptives and bone fractures in women: evidence from observational studiesCochrane Database Syst Rev20157CD009849
- LopezLMGrimesDASchulzKFCurtisKMChenMSteroidal contraceptives: effect on bone fractures in womenCochrane Database Syst Rev20146CD006033
- World Health Organization [webpage on the Internet]Medical Eligibility Criteria for Contraceptive Use5th ed Available from: http://www.who.int/reproductivehealth/publications/family_planning/Ex-Summ-MEC-5/en/Accessed January 21, 2016
- World Health Organization [webpage on the Internet]Adherence to Long Term Therapies: Evidence for Action Available from: http://www.who.int/chp/knowledge/publications/adherence_report/en/Accessed January 21, 2016
- SamsonsenCReimersABrathenGHeldeGBrodtkorbENonadherence to treatment causing acute hospitalizations in people with epilepsy: an observational, prospective studyEpilepsia20145511e125e12825252007
- AubenyEBuhlerMColauJCVicautEZadikianMChildsMOral contraception: patterns of non-compliance. The Coraliance studyEur J Contracept Reprod Health Care20027315516112428935
- LeteIDovalJLPerez-CamposESelf-described impact of noncompliance among users of a combined hormonal contraceptive methodContraception200877427628218342651
- KazerooniRVuKTakizawaABroadheadCMorrealeAPAssociation of copayment and socioeconomic status with hormonal contraceptive adherence in a female veteran populationWomens Health Issues2014242e237e24124533983
- ModySKHaunschildCFaralaJPHonerkamp-SmithGHurVKansalLAn educational intervention on drug interactions and contraceptive options for epilepsy patients: a pilot randomized controlled trialContraception2016931778026197260
- WiegratzIElliesenJPaolettiAMWalzerAKirschBAdherence with ethinylestradiol 20 µg/drospirenone 3 mg in a flexible extended regimen supported by the use of a digital tablet dispenser with or without acoustic alarm: an open-label, randomized, multicenter studyInt J Womens Health20157192925609999
- CastanoPMBynumJYAndresRLaraMWesthoffCEffect of daily text messages on oral contraceptive continuation: a randomized controlled trialObstet Gynecol20121191142022143257
- HalpernVLopezLMGrimesDAStocktonLLGalloMFStrategies to improve adherence and acceptability of hormonal methods of contraceptionCochrane Database Syst Rev201310CD004317
- SmithCGoldJNgoTDSumpterCFreeCMobile phone-based interventions for improving contraception useCochrane Database Syst Rev20156CD011159