
Abstract
Background
Rheumatoid arthritis (RA) is a systemic autoimmune inflammatory disease, wherein late diagnosis and treatment leads to deformities and disability.
Objective
The aim of the study was to assess and describe the clinical and immunological characteristics, activity status of the disease, and functional capacity in a cohort of Ecuadorian patients with RA.
Methods
This is a cross-sectional, descriptive study conducted on a population of patients with prediagnosed RA from public and private Ecuadorian rheumatology clinics. This study investigated 400 patients with a mean age of 50 years, 353 (82.25%) of which were female.
Results
The study showed that 44.3%, 83.5%, 60.3%, 41.8%, 37.5%, and 11.5% had an acute onset of the disease, symmetrical polyarthritis, morning stiffness exceeding 1 h, dry eyes, dry mouth, and rheumatoid nodules, respectively. A total of 89.7% presented with positive rheumatoid factor, and 96.5% were anti-citrullinated protein antibody positive.
Conclusion
This is the largest Ecuadorian cohort of patients with RA; clinical features are similar to those of other Latin American populations.
Keywords:
Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune, progressive, incapacitating, and multifactorial inflammatory disease. It most typically presents with bilateral and symmetrical polyarthritis, which causes joint pain and deformity, resulting in disability. Its extra-articular manifestations are heterogeneous and cover a wide range of affected organs; these manifestations are associated with a less favorable prognosis.Citation1
Its chronic course is a cause of increased morbidity/mortality, resulting in the deterioration in the patient’s quality of life.
Some factors, such as presence of rheumatoid factor, anti-cyclic citrullinated peptide (anti-CCP) antibodies, high disease activity, delay in consulting a specialist doctor, and therefore late diagnosis, have been considered representative of an unfavorable prognosis.Citation2
Diagnosis is clinical, based on the RA classification criteria established by the American College of Rheumatology (ACR) in 1987, which were updated in 2010.Citation3
Detailed assessment of patients with suspected RA is essential to confirm its diagnosis, monitor the patient, and provide a prognosis for the course of the disease. This includes the number of painful and swollen joints, assessment of the disease activity and pain using visual scales, assessment of functional capacity through approved questionnaires, assessment of acute phase reactants such as C-reactive protein (CRP), assessment of globular sedimentation rate, and analysis of structural damage through X-ray images of the hands.Citation4
The progress of the disease can cause deformity and disability in patients with RA, which has become a public health problem principally in Latin America, where RA is becoming more and more frequent.Citation5
The aim of the study is to assess and describe the clinical and immunological characteristics, activity status of the disease, and functional capacity in a cohort of Ecuadorian patients with RA.
Patients and methods
A cross-sectional, descriptive study was conducted on a population of Ecuadorian patients with a preexisting diagnosis of RA in accordance with the ACR 1987 classification criteria from public and private rheumatology clinics in the cities of Quito, Guayaquil, Manta, and Portoviejo.Citation6
The patients signed an informed consent form, which reflects the approval of the clinical study according to article 361 of the Political Constitution of the Republic of Ecuador, article 7 of the Organic Health Law, and article 15-16 of the Code of Medical Ethics of Ecuador. The study was approved by the Ethics and Teaching Committee of the Centro de Reumatología y Rehabilitación (CERER) with a registration number: No.001/2015; Folio 01: Book of Acts No.1. Patient anonymity of data was respected throughout the entire investigative process, and it was explained to the participants that the data collected would be used solely for the study.
A database was created to collect patient information, including the following variables: demographic data, clinical manifestations, comorbidities, habits, and treatment. To stratify disease activity, the Disease Activity Score-28 with C-reactive protein (DAS-28-CRP) was used, the number of painful joints among 28 joints was assessed, and visual analog scale (VAS) of pain was completed by the patient. The DAS-28-CRP was calculated by using the DAS score program version 1.1.Citation7 Depending on the values obtained, the patient was classified as in remission (score lower than 2.6), with low activity (2.6–3.2), with moderate activity (3.2–5.1), and with high disease activity (higher than 5.1).
The Spanish version of the Health Assessment Questionnaire Disability Index (HAQ-DI), approved in 1993, was used to assess the patient’s functional capacity and establish their degree of disability. This questionnaire has eight categories and a score between 0 and 3. Based on the degree of difficulty a patient presents in each activity, a score of more than 1.25 is considered as disability, and a score of 3 as severe disability.Citation7 The questionnaire was completed by the patients in their native language (Spanish).
The data was analyzed in the SPSS V.22 statistical program (IBM, Armonk, NY, USA), which was used to calculate measures of central tendency (mean) for quantitative variables and descriptive statistical measures, such as absolute and relative frequencies, for qualitative variables; also, the odds ratio (confidence interval: 95%) with Pearson correlation and Fisher correction in the study group was calculated. Values with two-tailed p<0.001 were considered statistically significant.
Results
We investigated 400 patients, of whom 353 and 47 (11.75%) were females and males, respectively. The mean age was 50 years (18–90 years).
A total of 93.75% (375), 3.5% (14), 1.5% (6), and 1.25% (5) of the patients were mixed race, white, and indigenous Afro-Ecuadorian, respectively.
Depending on the health system the patients came from, 32% (129), 23% (92), and 45% (179) received private, state, and mixed care (hospital and private care), respectively.
The study showed that 55.75% (223), 15.5% (62), 12% (48), 8.5% (34), 8.25% (33) were married, single, widowed, divorced, and cohabiting, respectively ().
Table 1 General characteristics
The mean age of onset of the disease was 41 years (10–89 years), and the mean time taken before the first appointment with the specialist was 29 months (0–332 months), with a mean monitoring time of 52 months (0–504 months).
Depending on the place of the origin sector, 11.75% (47) and 88.25% (353) were from the city and country areas, respectively.
With regard to occupational activities, 53.5% (214), 40% (160), 6% (24), and 0.5% (2) were performing domestic chores, working in different fields, unemployed, and students, respectively.
The study also showed that 9.5% (38), 7.5% (30), 0.5% (2) were active smokers, alcoholic beverage drinkers, and taking illegal/illicit drugs, respectively.
Depending on the characteristics of the disease, 44.3% (177) started with an acute onset, 55.5% (222) started gradually, 83.5% (334) presented symmetrical polyarthritis, 11.8% (47) asymmetrical polyarthritis, 5.3% (21) oligoarthritis, and 0.3% (1) monoarthritis.
Depending on the symptomatology, 60.3% (241), 48.5% (194), 41.8% (167), 37.5% (150), 22.8% (91), 35.5% (142), 11.5% (46), 3.3% (13), and 30.8% (123) reported morning stiffness lasting more than 1 h, fatigue, dry eyes, dry mouth, fever, myalgias, rheumatoid nodules, Raynaud’s phenomenon, and weight loss, respectively.
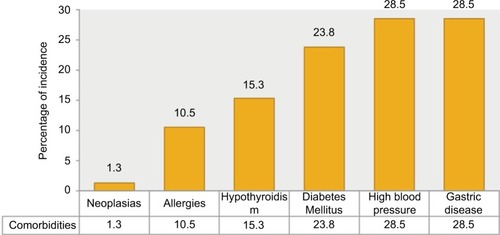
The study group’s comorbidities were hypertension, gastric disease, diabetes, hypothyroidism, allergies, and neoplasia, accounting for: 23.8% (95), 28.5% (114), 23.8% (95), 15.3% (61), 10.5% (2), and 1.3% (5), respectively ().
Figure 1 Comorbidities of patients with RA.
Disease activity score, calculated with the DAS-28-CRP, had a mean value of 3.37 (0.67–7.59) ().
Figure 2 Determination of disease activity using DAS-28-CRP.
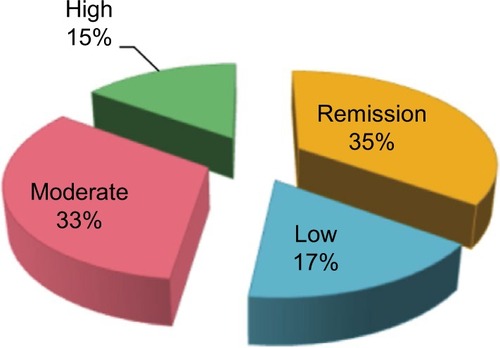
Based on these results, 35.5% (142) were in remission, 16.8% (67) had low disease activity, 32.8% (131) had moderate activity, and 15% (60) had high activity. The mean number of painful and swollen joints was approximately 5 (0–28) and 4 (0–28), respectively.
The mean VAS reported by the patients was 3.9 (0–10), whereas the VAS measured by the doctor was 3.4 (0–10).
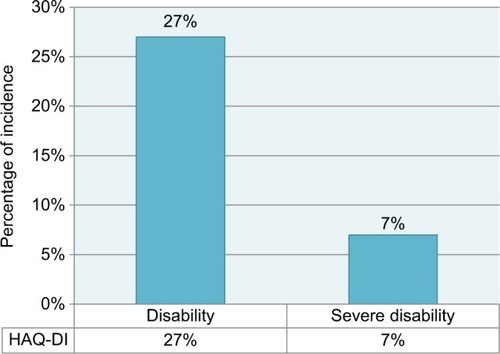
The mean HAQ-DI disability questionnaire score was 0.8 (0–3), and 66% (264) of the study population had no disability, whereas 34% (136) experienced some degree of disability, with 27% (108) and 7% (28) being functional and severe, respectively ().
Figure 3 Determination of disability in patients with RA, using HAQ-DI questionnaire.
Laboratory results showed that 8.3% (33), 6% (24), 2.3% (9), 5.3% (21), 89.7% (270/301), and 96.5% (193/200) of the study population had leukocytosis, thrombocytosis, thrombocytopenia, anemia, positive rheumatoid factor, and positive anti-CCP, respectively.
Depending on the treatment, 94.75% (379), 18% (72), 78.3% (313), 4.3% (17), 7.8% (31), 73.5% (294), and 66.5% (266) were administered disease-modifying antirheumatic drugs (DMARD), antimalarials, methotrexate, sulfasalazine, leflunomide, corticoids, and nonsteroidal anti-inflammatory drugs, respectively.
Of the total population, 12.5% (50) were administered biologic drugs: 4.7% (19) etanercept, 2.75% (11) tocilizumab, 2% (8) rituximab, 1.75% (7) adalimumab, and 1.3% (5) Infliximab.
Discussion
RA is a chronic systemic autoimmune inflammatory disease of unknown etiology that most frequently affects females in the reproductive age. It is characterized by polyarticular inflammation of the small and large joints, with systemic involvement.Citation1
The symptomatology and serology of this disease vary between different countries. In Ecuador, no epidemiological studies or data described the clinical and serological characteristics of Ecuadorian patients with RA.
The results obtained from this sample of Ecuadorian patients with RA show data similar to those obtained from the Latin American patient cohort, with early RA in the GLADAR (Grupo Latino Americano de Estudio de Artritis Reumatoidea [Latin American Rheumatoid Arthritis Study Group]) study in 2006,Citation7 wherein 51 Ecuadorian patients also participated among patients from other countries.
In both studies, RA most frequently affected females (88% Ecuador vs 85% GLADARCitation8). The mean age for onset of the disease was in the fourth decade (41 years for Ecuador vs 46 years for GLADAR). The disease presented in the majority of patients as symmetrical polyarthritis (84% Ecuador vs 95% GLADAR). Fatigue presented similar values in both studies (49% Ecuador vs 43% GLADAR) for the manifestations, whereas some differences were observed for other manifestations, perhaps due to the monitoring time of these patients (52 weeks); for example, the presence of Sicca syndrome was more prevalent in the Ecuadorian population compared with that in the GLADAR study (42% Ecuador vs 14% GLADAR), as were myalgias (36% Ecuador vs 11% GLADAR) and rheumatoid nodules (12% Ecuador vs 6% GLADAR).
The frequency of rheumatoid factor in the Ecuadorian population was higher than that in the GLADAR group (90% Ecuador vs 76% GLADAR), which might be because this study only included patients with a preexisting diagnosis of RA. Finally, the results for administering disease-modifying drugs were similar in both population groups (95% Ecuador vs 92% GLADAR), with methotrexate as the most common drug used for treatment.Citation9,Citation10
In Argentina, two studies have been conducted investigating the prevalence of RA. Spindler et alCitation11 studied a cohort of 695 patients with RA, wherein 86% were females, a value similar to this study (88% Ecuador vs 86% Argentina), with a mean age of 45 years at diagnosis (41 Ecuador vs 45 Argentina), with a total prevalence of 1.97 per 1,000 (95% CI, 1.8–2).
Soriano et alCitation12 also had similar findings in their studies of RA in the Hospital Italiano de Buenos Aires (Buenos Aires Italian Hospital), where they also studied the incidence rate, which was 2.4 per 10,000 people/yr; RA was higher in females (3.3 per 10,000 people/yr) than in males (1.1 per 10,000 people/yr).
Remembering that the prognosis for this disease depends first on its early diagnosis and treatment is important. Houssien et alCitation8 showed that patients being referred to a rheumatology clinic within the first year after the onset of symptoms had improved functional capacity.Citation5 They, and other studies, have shown the importance of administering early treatment in patients with RA and concur that a delay of 3 months in starting an appropriate treatment decreases the chances of remission from arthritis.Citation13
In our population, the delay in obtaining an appointment with the specialist was 29 months. Van der LindenCitation14 et al studied the relationship between the total delay from the onset of symptoms to an appointment with the rheumatologist (including delays on the patient’s part, accessing primary health care, and providing care on the rheumatologist’s part), joint damage, and the probability of achieving remission. They found that 69% of the patients with RA were provided care after 12 weeks or more; this was linked with a hazard ratio of 1.87 of not achieving remission free of DMARD and 1.3 more chance of greater joint damage in 6 years compared with the group who were provided care within the first 12 weeks.
Guevera et alCitation15 studied a cohort of 52 patients with a preexisting diagnosis of RA with mean time of 10.9 years affected by the disease; 82.7% of the patients were anti-CCP positive, and 82.7% were positive for rheumatoid factor.
Corominas et alCitation16 analyzed the diagnostic and therapeutic delay in RA and its relationship with health care departments in Catalunya. He found that the mean time from the onset of symptoms to the prescription of a disease-modifying drug in patients with RA was 11 months and that those patients who visited health care departments, such as clinics specializing in primary health care and arthritis, were treated sooner with disease-modifying drugs.
Another study with similar results is the ESORDIGCitation17 study conducted in Greece, which concludes that an early appointment with the rheumatologist and combined therapy with DMARDs are linked with a better prognosis for the disease.
Results similar to those in our study were obtained in Raza et al’sCitation18 study. They studied 482 patients with RA from 10 centers and obtained a mean delay of 24 weeks from the onset of symptoms to an appointment with a rheumatologist. They concluded that despite some centers attempting to minimize the delays, more intervention is required to ensure early treatment.
In 2005, a Peruvian study describing the epidemiological aspects of RA in patients in a Rheumatology Department at the Hospital Nacional Guillermo Almenara Irigoyen de Salud (Guillermo Almenara Irigoyen National Hospital of Health) in Lima identified 661 patients with RA not using biologic drugs, with a mean age of 44.5; 91.68% were positive for rheumatoid factor, a value similar to the Ecuadorian cohort (90%).Citation19
Based on the disease activity assessed by DAS-28-CRP, 47.8% of the population studied presented activity between moderate and severe. Based on the assessment of the patients’ functional capacity measured by HAQI, 37% of the population presented disability, including severe disability. This data reflected the high aggressiveness of the disease and the significant deterioration in the quality of life of the cohort studied.
Conclusion
The population studied is the largest cohort of patients with RA in Ecuador. The clinical characteristics did not differ greatly from populations in other studies, considering that descriptive studies of this disease are reported in Latin America, with the biggest probably being the GLADAR study, which revealed a situation very similar to that in Ecuador.
The conclusion must also be drawn that the cohort analyzed showed a very active, as well as incapacitating, disease, given that nearly 50% of the patients presented DAS-28 levels, which indicated activity between moderate and sever. This figure may well be related to the mean delay of 29 months in being assessed by a rheumatologist, and therefore a late diagnosis and treatment.
Acknowledgments
We acknowledge Maria Jose Intriago, Claudia Aguirre, Jenny Cárdenas, Víctor Avila from Universidad de Especialidades Espíritu Santo; Dr Rafael López, Dr Jose Martínez, Dr Nelson Córdova from Hospital Luis Vernaza; Dr Letty Moreno from Rheumatology and Rehabilitation Center and Dr Jose Nuñez, Dr Ivonne Quezada from Ecuadorian Society of Rheumatology for their contribution to the study.
Disclosure
The authors report no conflicts of interest in this work.
References
- Maldonado-CoccoJCiteraGReumatología. 1era. Edic. Azurras2010
- Villaverde GarcíaVBalsa CriadoAFactores pronósticos de la artritis reumatoideRev Esp Reum20022911015
- AletahaDNeogiTSilmanA2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiativeAnn Rheum Dis20106991580158820699241
- Sociedad Española de ReumatologíaClinical practice guideline for the management of Rheumatoid Arthritis in Spain2011 Available from: http://www.ser.es/wp-content/uploads/2016/01/GUIPCAR_31Marzo2012_ENG.pdf
- Sociedad Argentina de ReumatologíaGuías Argentinas de Práctica Clínica en el Tratamiento de la Artritis ReumatoideaRev Argent Reumatol2008193293
- ArnettFEdworthySBlochDThe American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritisArthritis Rheum19883133153243358796
- CardielMAbello-BanfiMRuiz-MercadoRAlarcon-SegoviaDHow to measure health status in rheumatoid arthritis in non-English speaking patients: validation of a Spanish version of the Health Assessment Questionnaire Disability Index (Spanish HAQ-DI)Clin Exp Rheum1993112117121
- CardielMHFirst Latin American position paper on the pharmacological treatment of rheumatoid arthritisRheumatology (Oxford)200645Suppl 2ii7ii2216709584
- CardielMHPANLAR, GLADARFirst Latin American position paper on the pharmacological treatment of rheumatoid arthritisRheumatology200645ii7ii2216709584
- CardielMPons-EstelBSacnunMTreatment of early rheumatoid arthritis in a multinational inception cohort of Latin American patients: the GLADAR experienceJ Clin Rheumatol201218732733523047532
- SpindlerABellomioVBermanAPrevalence of rheumatoid arthritis in Tucuman, ArgentinaJ Rheumatol2002291166117012064829
- SorianoECarriónJSchpillbergMFigarSImamuraPCattogioLIncidence and prevalence of rheumatoid arthritis in health management organization in ArgentinaRheumatology2003421130
- SørensenJHetlandMDiagnostic delay in patients with rheumatoid arthritis, psoriatic arthritis and ankylosing spondylitis: results from the Danish nationwide DANBIO registryAnn Rheum Dis2015743e1224534758
- van der LindenMle CessieSRazaKLong term impact of delay in assessment of patients with early arthritisArthritis Rheum201062123537354620722031
- GuevaraSOchoaMVintimillaJAntígenos HLA de clase II en pacientes con artritis reumatoide ecuatorianos y asociación con el factor reumatoide, anticuerpos anti-citrulinados y nódulos reumatoidesRev la Fac Ciencias Médicas la Univ Cuenca20143216677
- CorominasHNarvaézJDíaz-TórneCDiagnostic and therapeutic delay of rheumatoid arthritis and its relationship with health care devices in Catalonia. The AUDIT studyReum Clin201612146150
- AndrianakosATrontzasPChristoyannisFPrevalence and management of rheumatoid arthritis in the general population of Greece–the ESORDIG studyRheumatology200645121549155416690763
- RazaKStackRKumarKCorrection: delays in assessment of patients with Rheumatoid Arthritis: variations across EuropeAnn Rheum Dis2011701822182521821867
- Acevedo-VásquezEAlgunos aspectos de la artritis reumatoide en PerúRev Soc Peru Med Interna20122513137