
Abstract
Kawasaki disease is a mysterious childhood vasculitis. It presents with multi-systemic involvement in which the prolonged high-grade fever and mucocutaneous and lymph node manifestations are the prominent features. Sometimes, the disease has an unusual, atypical or incomplete presentation. Herein, we present a child with hilar lymphadenopathy as a manifestation of Kawasaki disease.
Introduction
Kawasaki disease (KD) is the most common acute primary medium-size vasculitis in childrenCitation1 which predominantly involves coronary arteries.Citation2 KD is classified into classic and atypical according to clinical features. Cervical lymphadenopathy is one of the major presenting manifestations of Kawasaki disease.Citation3 However, lymphadenopathy in other anatomical sites such as mediastinal lymphadenopathy is not frequently seen in this disease.Citation4 We report a case of Kawasaki disease with mediastinal lymphadenopathy, as a rare presenting feature in this disease.
Case Presentation
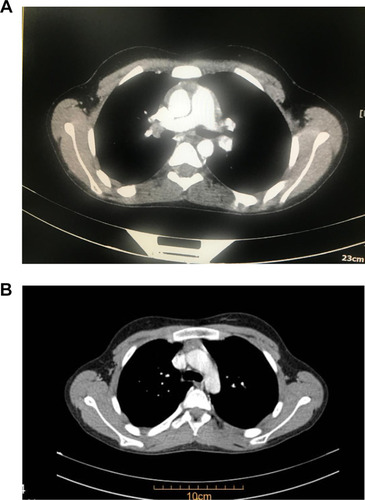
A previously healthy 11-year-old boy was referred to our pediatric rheumatology department due to fever and neck swelling for two weeks. He was previously prescribed amoxicillin-clavulanic acid. In the next three days, neck swelling resolved but fever persisted and a generalized macular rash was added to his symptoms. Two days later he had red lips and tongues. He was admitted and received ceftriaxone in another medical center with suspicion of an infective process. As his condition did not improve and arthralgia was added to his problems, he was brought to our center. Physical examination revealed, ill appearance, erythematous throat, large tonsils, bilateral non-purulent conjunctivitis and desquamation of extremities. No cervical lymphadenopathy was detected. The patient had no obvious respiratory difficulty. Laboratory tests showed white blood count (WBC): 7200/μL (neutrophils: 65%, lymphocytes: 27%), hemoglobin: 12.3 mg/dL, platelet count: 490,000/μL, C-reactive protein (CRP): 38mg/L, and erythrocyte sedimentation rate (ESR): 49mm/h. Culture samples taken from Blood and throat were negative. The mediastinal widening was seen in Chest X-ray. An echocardiogram revealed dilatation of the left main coronary artery (internal diameter: 4mm). On Computed tomography (CT) of the chest, a prominent right hilar lymph node measuring about 15 mm × 15 mm was detected (). Workups for finding other sites of lymphadenopathy were negative. The ACE level was normal. PPD Test was negative. Upon re-evaluation of his clinical course and results of laboratory and echocardiography investigations, the diagnosis of KD was considered and intravenous immunoglobulin (IVIG) at 2 g/kg along with aspirin at 30 mg/kg/day was given. Fever subsided within 12 hours after administration.
Figure 1 Mediastinal lymphadenopathy in a child with Kawasaki disease: (A) at presentation; (B) eight weeks later.
Follow-Up
Regarding hilar lymphadenopathy, the patient was visited by the pediatric pulmonologist consultant. As no other site of lymphadenopathy was detected and the patient had a negative PPD test and ACE level the watch and wait strategy was considered for him. The patient was discharged with aspirin, and re-evaluation with echocardiography and chest CT scan was done 8 weeks later. No more hilar lymphadenopathy was seen in the follow-up chest CT scan and the normal coronary artery (internal diameter: 2.8 mm) was seen on the echography after 8 weeks.
Discussion
KD is one of the most common systemic vasculitides in childhood. Since no definite diagnostic test is available, inevitably KD diagnosis is dependent on clinical and laboratory criteria.Citation3 We presented a case that fulfilled American Heart Association (AHA) criteria: persistent fever as essential criteria, unilateral cervical lymphadenopathy (neck swelling), non-purulent bilateral conjunctivitis, changes of the lip and oral cavity, rash and changes of peripheral extremities. As the patient had hilar lymphadenopathy and this is not a common feature in KD, we had to rule out lymphoproliferative disease, mycobacterium tuberculosis, and sarcoidosis.
Mediastinal lymphadenopathy was once reported as an unusual presentation of KD in 1996, accordingly, it was suggested that lymphadenopathy other than cervical may occur during KD.Citation5 In 2010, Kashef et al also reported a case of atypical KD who was found to have para-aortic lymphadenopathy.Citation4 In both mentioned cases the common feature was the resolution of the lymphadenopathy after 6 to 8 weeks. Therefore, we decided to repeat chest CT scan 8 weeks later. The CT scan revealed shrinkage of mediastinal lymph node and reaching right hilar lymph node size to 8 mm ×8 mm. With 12 months follow up, the patient did not have any cardiac morbidity. We propose in the context of clinical and laboratory findings; the physicians should consider KD as one of the causes of mediastinal or hilar lymphadenopathy.
Data Sharing Statement
Available on request from the contact author.
Ethical Considerations
The aim of report was initially explained to the patient’s parents. Then, a written informed consent was obtained from them. No extra costs were imposed on the parents besides having the advantage of a free visit by the pediatric rheumatologists and their team work. All patients’ data were regarded as confidential. Institutional approval was not required to publish the case details.
Consent for Publish
We confirm that the written informed consent form has been provided by the parents to have the case details published.
Disclosure
The authors report no conflicts of interest in this work.
References
- Yu JJ. Diagnosis of incomplete Kawasaki disease. Korean J Pediatr. 2012;55(3):83–87. doi:10.3345/kjp.2012.55.3.8322474462
- Kawasaki T. Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children. Arerugi. 1967;16:178–222.6062087
- Mc Crindle BW, Rowley AH, Newburger JW, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135(17):e927–99. doi:10.1161/CIR.000000000000048428356445
- Kashef S, Momen T, Heidari B, Amin R. Para-aortic Lymphadenopathy Associated with Kawasaki Disease. Iran J Pediatr. 2010;20(4):476–478.23056749
- Bosch Marcet J, Serres Creixams X, Penas Boira M, Inaraja Martinez L. Mediastinal lymphadenopathy: a variant of incomplete Kawasaki disease. Acta Paediatr. 1998;87(11):1200–1202. doi:10.1111/j.1651-2227.1998.tb00932.x9846926