
Abstract
Anakinra is an interleukin (IL) receptor antagonist that works by blocking the biological activity of IL-1 by competitively inhibiting binding of IL-1 to the type 1 interleukin receptor. IL-1 production is induced in response to inflammatory stimuli and mediates various physiological mechanisms, including inflammation and immunological reactions. Patients with neonatal onset multisystem inflammatory disease (NOMID) produce excess IL-1β, a major proinflammatory cytokine that regulates innate immune responses. Anakinra binds competitively and this results in a rapid reduction in disease severity. NOMID, also known as chronic infantile neurologic, cutaneous, articular syndrome, is the most severe clinical phenotype in the spectrum of cryopyrin-associated periodic syndromes. It is characterized by cutaneous symptoms, arthropathy, and central nervous system involvement. Extensive studies in patients with NOMID have led to advances in characterizing the extent of organ-specific involvement and damage that occurs with chronic overproduction of IL-1β. NOMID is caused predominantly by mutations in the NLRP3/CIAS1 gene that encodes for the protein cryopyrin, leading to activation of the “NLRP3 inflammasome complex”. This in turn regulates the maturation and secretion of the inflammatory cytokine, IL-1β. The clinical value of IL-1β has been demonstrated by the positive response of patients after treatment with anakinra, with rapid improvement in clinical symptoms, markers of inflammation, and a significant decrease in major organ manifestations.
Introduction
Neonatal onset multisystem inflammatory disease (NOMID) is a monogenic autoinflammatory syndrome and constitutes one of the three known cryopyrin-associated periodic syndromes (CAPS). These syndromes occur as a result of an autosomal dominant or de novo mutation of the cold-induced autoinflammatory syndrome 1 (CIAS1) gene on chromosome 1q44.Citation1 The three clinical entities that belong to the group of diseases known as CAPS were discovered at different times, and initially described separately as distinct diseases. It was not until a common genetic defect was identified that these three diseases were recognized as separate clinical phenotypes of the same disease mechanism. The three forms of CAPS are familial cold autoinflammatory syndrome (FCAS), Muckle–Wells syndrome (MWS), and NOMID, or as it is known in Europe, chronic infantile neurological, cutaneous, articular (CINCA) syndrome. The discovery of a common etiology for these diseases is an important step in the understanding of autoinflammatory disease. The clinical spectrum, including both similarities and differences in presentation of the three diseases, adds to the intrigue surrounding the common genetic defect. Why does a single common defect lead to such diverse clinical symptoms and signs?
Along the clinical spectrum of CAPS, all three diseases present in the neonatal period, although there have been reports of presentation after infancy and even into adulthood. Common features of these diseases include inflammation of the skin, eyes, bones, joints, and meninges. In addition, severe fatigue, fever, myalgia, chronic anemia, and learning disabilities are some of the other symptoms which are commonly seen.Citation2 The similarities and differences of these diseases are shown in . These diseases make up a group of rare hereditary autoinflammatory diseases, with an estimated population frequency in the range of 1–3 per million.Citation3
Table 1 Similarities and differences between CAPS with symptom progression from the mildest form to the most severe form of the disease
The discovery of a genetic basis for these disorders has significantly impacted new approaches to treatment. The CIAS1 gene, which is mutated in CAPS patients, has been discovered to be involved in inflammation and apoptosis.Citation4 In response to inflammation, interleukin (IL)-1β is secreted and is known to mediate the peripheral immune response during infection and inflammation. It has been reported that patients with NOMID and other CAPS disorders have higher IL-1β levels compared with their healthy counterparts. Thus, the mutation in CAPS is a gain-of-function mutation.
As a result of the pathogenesis, targeting the IL-1β pathway has proven to be a successful approach in the treatment of patients with CAPS, specifically NOMID. Recent advances in the development of drugs targeting IL-1β have led to the introduction of several anti-IL-1β drugs, including anakinra, rilonacept, and canakinumab.
Cryopyrin-associated periodic syndromes
The three cryopyrin-associated periodic syndromes are FCAS, MWS, and NOMID. Chronic inflammation, with recurrent fever, cutaneous rash, and joint symptoms, are common characteristics of these diseases. As they progress from the mildest form to the most severe form, the rash becomes less prominent, and other more severe features dominate the clinical presentation.Citation5 This spectrum of disease severity is shown in .
Familial cold autoinflammatory syndrome
FCAS is the mildest phenotype of the autoinflammatory diseases and is characterized by urticarial rash, low grade fever, polyarthralgias, and conjunctivitis induced by exposure to cold, occurring primarily in infancy.Citation6 These episodes are generally self-limiting and resolve within 24 hours. Other symptoms induced by cold exposure include profuse sweating, drowsiness, headache, extreme thirst, and nausea.Citation7 Although these symptoms have a significant impact on quality of life, they are not associated with organ damage or disability. Laboratory studies show elevated neutrophil counts, erythrocyte sedimentation rate, and C-reactive protein.
Muckle–Wells syndrome
MWS is the intermediate phenotype and is characterized by recurrent episodes of rash and fever that may develop in the first few years of life. The rash can be cold-induced, urticarial, or erythematous. Musculoskeletal symptoms include arthralgia, arthritis, and myalgias. These features occur episodically and can last anywhere from one day to 2 weeks. Sequelae of MWS may include sensorineural hearing loss and secondary renal amyloidosis with nephropathy (a complication of late stage disease).Citation8 The hearing loss is progressive, likely leading to deafness by adolescence, and the amyloidosis may progress to impaired renal function. Laboratory findings include generalized leukocytosis and elevations in acute-phase reactants.
Neonatal onset multisystem inflammatory disease
NOMID is the most severe phenotype, with the course of disease being more chronic than recurrent. It manifests in the first few weeks of life with an urticarial-like rash, arthropathy, and central nervous system involvement.Citation9 The rash is typically nonpruritic and can vary with disease activity. Fever is usually mild in this disease. Individuals have atypical “facies”, including frontal bossing, a saddle-back nose, and mid-face hypoplasia. The disease also causes bony overgrowths predominantly involving the knees and the distal extremities of the hands and feet. Chronic inflammatory polyarthritis may also be present, resulting in bone erosions. The severity of bone and joint involvement is variable, with approximately two thirds of patients developing arthralgia and transient swelling during flares, and the remaining one third developing severe and disabling arthropathy, resulting in gross deformity of the patella and epiphyses of the long bones.Citation10
The radiographic findings in severe cases are characterized by a “bread crumb” appearance of the patella and epiphyses. Central nervous system manifestations can be the most devastating, and include chronic septic meningitis, increased intracranial pressure, cerebral atrophy, ventriculomegaly, sensorineural hearing loss, and chronic papilledema with associated optic nerve atrophy and loss of vision. Mental retardation and seizures are also present.Citation9
Findings suggestive of an ongoing inflammatory process include lymphadenopathy, splenomegaly, elevations in acute-phase reactants (erythrocyte sedimentation rate and C-reactive protein), leukocytosis, cerebrospinal fluid neutrophilia, hyperglobulinemia, and chronic anemia. Failure to control the inflammation can lead to irreversible organ damage and disability. Therefore, it is imperative to start treatment as soon as the disease is suspected.
Pathophysiology of autoinflammatory syndromes
Genetics of cryopyrin
The discovery of a genetic basis for NOMID has led to its placement among the other cryopyrinopathies, all of which are caused by mutations in the CIAS1 gene. The genetic defect was first defined in FCAS in 2000, and subsequently the same gene was found to be responsible for MWS.Citation7,Citation11 The genetic defect was identified in NOMID in 2002. There are many mutations that lead to CAPS, and are located in exon 3 of the CIAS1 gene. All are gain-of-function mutations and are essential to the activation of intracellular caspase-1 and processing of IL-1β.Citation12
Mechanism of action of cryopyrin
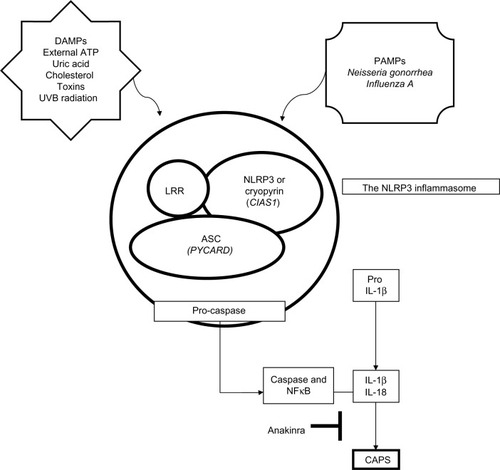
CIAS1 encodes the cryopyrin molecule, which combines with a group of interacting proteins to form a macromolecular complex called the “inflammasome,” that is important in the innate immune response due to its role as a molecular platform.Citation13 There are at least four inflammasomes, designated NLRP1, NLRP3, NLRC4, and AIM2.Citation14 The NLRP3 inflammasome, which is directly responsible for CAPS, contains three separate components that are all involved in the activation of proinflammatory cytokines, such as IL-1β and IL-18. These components include NLRP3/cryopyrin, an apoptosis-associated speck-like protein (ASC) containing a CARD (caspase activation and recruitment domain) and a leucine-rich repeat domain.
The signals leading to inflammasome activation and generation of proinflammatory cytokines such as IL-1β include danger-associated molecular patterns and pathogen-associated molecular patterns. There have been many danger-associated molecular patterns described, including cholesterol or uric acid, toxins, adenosine triphosphate (ATP), and ultraviolet B radiation.Citation15–Citation17 Pathogen-associated molecular patterns that have been shown to activate NALP3 include bacteria such as Neisseria gonorrhea and viruses such as Influenza A.Citation18,Citation19 Once NLRP3 is stimulated, it oligomerizes and binds the adaptor protein ASC. ASC interacts with cryopyrin, leading to activation of nuclear factor kappa B and caspase-1, and apoptosis.Citation20
Activation of caspase-1 results in cleavage of pro-IL-1β and pro-IL-18 into their mature forms (IL-1β and IL-18, respectively) which are secreted by the cell.Citation21 Thus, activated cryopyrin induces release of the active form of IL-1β. This process is illustrated in . In all three phenotypes of CAPS, the gain-of-function mutation of the NLRP3 gene forms a defect in this pathway, resulting in increased inflammasome activation, which enhances and accelerates production of IL-1β, leading to the inflammatory symptoms seen in NOMID.Citation22
Figure 1 Pathophysiology of CAPS. Activation of the NLRP3 inflammasome is triggered by exposure of immune cells to a variety of danger-associated molecular patterns and pathogen-associated molecular patterns. The leucine-rich repeat domain of the NLRP3 is thought to serve as an autoinhibitor by self-folding. The molecule spreads out, dimerizes, and associates through homotypic interaction with the ASC adaptor protein to mediate the proteolytic processing of pro-caspase 1 to caspase-1. The ASC protein also interacts with cryopyrin. When cryopyrin binds to ASC it can result in NFκB and caspase-1 activation. Once caspase-1 is activated, it results in cleavage of pro-IL-1β and pro-IL-18 into their mature forms IL-1β and IL-18, respectively, which is secreted by the immune cell. Thus, activated cryopyrin induces release of the active form, IL-1β.
Therapeutic targets and strategies
The disorders caused by CIAS1 mutations are not distinct diseases, but represent a clinical continuum of phenotypes. It was discovered that the same nucleotide substitution in CIAS1 may be associated with a different clinical subtype in different patients.Citation23 It is also interesting that various mutations in CIAS1 result in different levels of caspase-1 activation, thereby leading to such extreme clinical spectrum ranges as seen in the different phenotypes of CAPS.Citation24 In addition, CIAS1 mutations may not always be the culprit in diseases involving cryopyrin. This has been evident in several patients with FCAS, MWS, and NOMID who do not have mutations in CIAS1, but have the classic disease phenotype.
Most CIAS1 mutations are inherited in an autosomal dominant pattern, although de novo cases have been reported. Mutations in CIAS1 were found in 50% of NOMID patients and mutations occurred de novo in five of seven patients with NOMID syndrome.Citation25 This suggests that the severity and presence of the disease is likely to be influenced by other genetic and environmental factors.Citation26
The CIAS1 mutation in CAPS is a gain-of-function mutation in cryopyrin, leading to activation of proinflammatory cytokines. IL-1, one of the proinflammatory cytokines activated in CAPS, is the primary target for drugs such as anakinra. It was originally thought that anakinra should be used in the treatment of NOMID patients with CIAS1 mutations only. However, a number of studies have demonstrated that anakinra is effective for treatment of the disease regardless of the gene defect present. For example, recent work by Lovell et al demonstrated improvement of NOMID symptoms in a patient with a normal CIAS1 gene sequence after treatment with anakinra.Citation27 In another study by Hawkins et al, three patients were diagnosed with NOMID on clinical grounds and later revealed no CIAS1 mutations. After receiving anakinra, all three patients had resolution of fever, rash, joint inflammation, and headache, with normalization of C-reactive protein and erythrocyte sedimentation rate.Citation28 These findings suggest that regardless of the upstream mechanism, such as CIAS1 defects, correction of the downstream effect including IL-1β overproduction ameliorates symptoms of the disease.
Another observation has been the presence of somatic mosaicism in patients with CIAS1-related disease. Tanaka et al were able to identify that NOMID/CINCA resulted from the mutant NLRP3 gene in these cases of somatic mosaicism, in which mutant cells accounted for 4.2%–35.8% of all blood cells.Citation29
Treatment
Traditional treatment
Traditional treatment of CAPS has utilized anti-inflammatory agents such as glucocorticoids, nonsteroidal anti-inflammatory agents, antihistamines, and other immunosuppressive medications, all without significant success. While there have been modest improvements with high-dose oral corticosteroids and thalidomide, these agents have not been well tolerated due to their side effect profile. Because of the discovery that IL-1β is a potent proinflammatory cytokine which is upregulated by mutations in CIAS1, three new therapies have been identified which use different approaches to achieve the same goal.
Anakinra: an IL-1 receptor antagonist
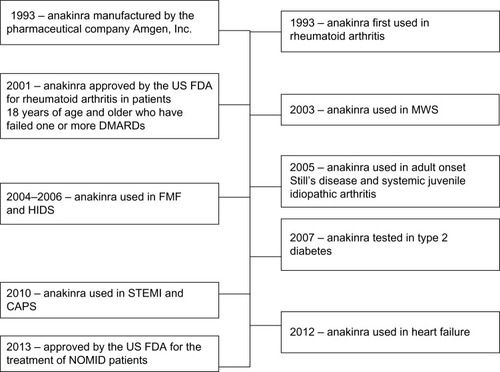
Exploration of IL-1 receptors started in 1993 with the introduction of anakinra, a recombinant, nonglycosylated version of IL-1 receptor antagonist (IL-1RA) prepared from cultures of genetically modified Escherichia coli using recombinant DNA technology. It consists of 153 amino acids and differs from native human IL-1RA in that it has the addition of a single methionine residue on its amino terminus. Since 1993, anakinra has been well studied and has been shown to control many diseases, including CAPS. Use of anakinra in different diseases is shown in a timeline in . Anakinra currently dominates the field of IL-1 therapeutics, mostly because of its excellent safety profile and tolerability by pediatric and adult patients. Anakinra was approved by the US Food and Drug Administration in January 2013 for the treatment of NOMID, and its use is expected to increase, given that it may have a beneficial effect in other disease states.
Figure 2 Timeline highlighting use of anakinra in various disease states.
A role for anakinra in the treatment of CAPS has been evident in prevention of clinical symptoms and acute-phase elevations in patients with FCAS,Citation30 an ability to induce complete remission in MWS, and resolution of symptoms including uveitis, rash, and fever in NOMID patients.Citation31,Citation32 The possibility of reducing the clinical symptoms of inflammation and improvement in quality of life makes this discovery extremely important. The safety and efficacy of anakinra have been tested in a number of studies, with promising results.
The short-term efficacy and rapid response to anakinra was first reported in a study by Hawkins et al, who followed three severely ill family members carrying NALP3/CIAS1 mutations. It was reported that clinical features such as rash, fever, conjunctivitis, and arthralgia improved within 4 hours after the first injection, and serologic remission was achieved within one week. The study also reported a rapid decrease in C-reactive protein levels and a resolution of hematologic abnormalities in all patients.Citation33
Immediate resolution of clinical symptoms was also evident in a retrospective study by Leslie et al, who demonstrated complete remission of rash, fever, conjunctivitis, and rheumatic aches within 4–12 hours of starting anakinra in 15 patients treated for 39 months. These patients were treated starting with daily 100 mg subcutaneous injections and then reduced to 20–50 mg to determine efficacy at lower doses. All patients improved on the lower doses, except for two children who continued to receive 100 mg daily injections. Monthly measurements of C-reactive protein and serum amyloid A levels were reviewed, and demonstrated normalization within one week in all patients. In addition, nephrotic syndrome remitted within 8–33 months in three patients with AA amyloidosis.Citation34
In a prospective study, Goldbach-Mansky et al demonstrated improvement in symptoms such as urticarial-like rash and acute-phase reactants, in addition to improvements in hearing and neurosensory deficits in 18 children with CINCA/NOMID (12 with identifiable CIAS1 mutations) followed for 6 months. The treatment was able to effectively control most of the clinical manifestations, including chronic meningitis and papilledema. Abnormal cochlear enhancement was detected in 17 patients on magnetic resonance imaging, and although 13 of these patients had improvement of cochlear enhancement, one had a regression and three had no improvement after 3 months of therapy. Primary outcomes were decreases in C-reactive protein, erythrocyte sedimentation rate, and serum amyloid A levels, as well as daily improvement in ratings of symptoms at 3 months, all of which also remained low at 6 months. In total, eight of 18 patients showed remission of inflammatory symptoms after 3 months and the remaining ten patients after 6 months. Furthermore, treatment with anakinra reduced secretion of IL-1β from cultured peripheral blood mononuclear cells after 6 months of therapy.Citation32
Not only has anakinra been useful in NOMID patients, but it has also shown improvement in patients with other CAPS disorders. In a study by Kuemmerle-Deschner et al, anakinra proved to be an effective and safe therapy in 12 children and adults with severe MWS over a median of 11 (5–14) months. There was rapid resolution of constitutional symptoms, severe disease-associated fatigue, and musculoskeletal, skin, and eye symptoms after 2 weeks of therapy. Classical markers of inflammation improved in the majority of these patients. The erythrocyte sedimentation rate normalized in all but one patient (92%), and the C-reactive protein value normalized in 45% of those who had an elevation at baseline. While improvement in erythrocyte sedimentation rate was detectable as early as 2 weeks and then plateaued, C-reactive protein levels continued to improve further until the last follow-up visit.Citation35
Similar observations were reported in a study by Hoffman et al, in which anakinra was able to prevent cold-associated acute inflammation in four patients with FCAS subjected to cold challenge. When subjected to cold challenge without anakinra treatment, the patients with FCAS developed low grade fever, rash, and arthralgia starting 1–2 hours after cold challenge. The patients with FCAS treated with anakinra before cold challenge did not develop any of the signs or symptoms that they had developed during the previous cold challenge. These patients did develop a mild rash after the initial dose, but had no symptoms after the second dose and remained symptom-free for 24–48 hours.Citation30
Given that use of IL-1RA is relatively new, its efficacy and safety on a long-term basis is not well documented. Several studies have assessed the long-term effects of IL-1 antagonists in different phenotypes of CAPS patients, including NOMID/CINCA. Lepore et al demonstrated the long-term effects and sustainability of control of inflammatory manifestations in ten CINCA patients who were followed for 26–42 months. They demonstrated complete control of the inflammatory manifestations, such as skin rash, arthritis/arthralgia, elevated acute-phase reactants, and inflammatory anemia for up to almost 5 years of follow-up. Continuous treatment with anakinra completely controlled some of the neurologic manifestations such as chronic meningitis and headache (although control of papilledema and amelioration of hearing loss was not achieved).Citation36 In a study by Neven et al, the long-term effects of anakinra for up to 26–42 months have also been demonstrated in treating a broad range of systemic manifestations, neurologic involvement, and growth parameters. The magnitude of these responses was dose-dependent, with improvement in constitutional symptoms such as fever, rash, and arthralgia at 1 mg/kg/day. Higher doses (2–3 mg/kg/day) were necessary in five patients with persistent headache and papilledema after one year of therapy in order to achieve ongoing normalization of biologic inflammation marker levels and decreases in central nervous system inflammation.Citation10 However, central nervous system inflammation normalized in only one patient, with improvement and stabilization in a total of four patients. These data indicate that long-term remission is possible, but this is difficult to achieve in severe cases of NOMID.
Leslie et al also demonstrated a positive outcome in 15 MWS patients followed for a median of 17 (1–39) months. All patients showed a sustained response to drug therapy without dosage adjustments to prevent recurrence of symptoms. There was significant improvement in renal disease measured by scintigraphic scan for amyloidosis.Citation34
Based on the studies to date, it is clear that anakinra is a major advance in the management of NOMID and other CAPS phenotypes. To date, there have been very few side effects demonstrated with administration of anakinra. Local injection site reactions, including itching, swelling and redness, have been reported to occur in 42% of patients.Citation35 Similar rates of local site reactions were reported in the other studies mentioned above.Citation32–Citation34 However, injection site reactions are uncommon after the first month of therapy. Despite the success of anakinra, the short half-life of 4–6 hours requires daily subcutaneous injections. Treatment becomes a lifelong process, because drug withdrawal leads to disease flares. As discussed below, other IL-1-blocking agents with longer half-lives are also being developed and tested with success.
Rilonacept: IL-1 trap
Rilonacept, an IL-1 trap cytokine inhibitor, has been used effectively in the treatment of many diseases. Rilonacept utilizes cytokine trap technology, which allows for effective inhibition due to multicomponent “traps” containing binding sites for the cytokine as well as their accessory proteins. Cytokine traps have been very effective in autoinflammatory diseases because they bind to their respective cytokines with high affinity.Citation37 Rilonacept was first approved by the US Food and Drug Administration in 2008 specifically for FCAS and MWS patients over the age of 11 years. The drug has a half-life of 8.6 days, which makes weekly injections an improvement over daily injections of anakinra. The safety and efficacy of weekly subcutaneous injections (160 mg/week) of rilonacept have recently been evaluated in patients with FCAS and MWS. The efficacy of treatment was confirmed in a one-year study, with five FCAS patients having confirmed mutations.Citation38 All five patients showed improvement of symptoms, with the maximum improvement at days 6–10. All patients were given doses of 160 mg weekly, although remission did not occur in four patients, who were then given doses of 320 mg. All five patients tolerated the drug very well with no injection site reactions, and showed long-term efficacy at the 2-year follow-up.
In two sequential, double-blind, placebo-controlled trials of patients with FCAS or MWS, all patients had positive CIAS1 gene mutations. In the first study, a randomized 6-week trial, 47 patients received either rilonacept at a dose of 160 mg/week or placebo. The patients receiving the drug showed a decrease in disease activity score of 84% compared with 13% in patients receiving placebo. In the second study, patients were enrolled in a 9-week, single-blind treatment period followed by a 9-week, double-blind withdrawal period. Patients on rilonacept therapy during the “withdrawal” period demonstrated improved efficacy compared with the group on placebo.Citation39 Patients treated with rilonacept had mild injection site reactions.
Canakinumab: IL-1β monoclonal antibody
Canakinumab is a human IL-1β monoclonal antibody with very good efficacy in the treatment of CAPS patients. It has a long half-life of 26 days, which allows for a dosing schedule of subcutaneous injections every 8 weeks. This dosing schedule is favorable compared with that of anakinra (daily) and rilonacept (weekly). Canakinumab was approved by the US Food and Drug Administration in 2009 for use in CAPS patients over 4 years of age. The first open-label clinical trial for canakinumab was completed in 2008 in seven mutation-confirmed CAPS patients. In these patients, IL-1β production fell to levels similar to those seen in unaffected healthy controls after 8 weeks of therapy.Citation40
In another double-blind, randomized trial in 2008, 35 CAPS patients (all with confirmed NLRP3 mutations), enrolled in a three-part, 48-week trial to receive 150 mg of canakinumab every 8 weeks. In the first part, 34 of the 35 patients had a complete response in as little as 8 days, which was confirmed by physician assessment of disease activity and rash, as well as C-reactive protein and serum amyloid A levels. In the second part of the study, 15 patients received the drug and 16 patients received placebo. All 15 patients in the treatment group experienced remission of symptoms, while 13 of those in the placebo group experienced disease flares and increased C-reactive protein. In the third part, the 31 patients showed sustained clinical remission with minimal disease activity, disappearance of rash, and normalization of C-reactive protein and serum amyloid A levels. Complete remission was seen in 97% of the patients on treatment, and randomization to placebo led to disease flares in 81% of patients, whereas all patients who received the drug remained in remission. Injection site reactions occurred in up to 9% of patients, and up to 14% of the patients developed vertigo.Citation41
Side effects of biological modulators of IL-1/IL-1R
The primary side effects of anakinra in NOMID have been reported to be local injection site reactions, including redness, rash, itchiness, or pain. Other skin reactions such as bruising or bleeding can occur, but are very rare. Skin reactions usually resolve after 1–2 weeks. Biological modulators carry a risk of infection, and this has been reported when anakinra is used to treat rheumatoid arthritis but not NOMID. Other reactions may include headaches, vomiting, arthralgias, pyrexia, and nasopharyngitis. The most common side effects of canakinumab in the treatment of CAPS include nasopharyngitis, diarrhea, nausea, influenza, and headache. A similar side effect profile was also described with rilonacept, with injection site reactions being the most common adverse effect.
Discussion
Remarkable advances have been made in our understanding of the molecular and genetic pathways responsible for the clinical phenotypes of NOMID. Studying patients with NOMID has allowed us to define the extent of disease damage caused by overproduction and secretion of IL-1β due to mutations in the CIAS1 gene. The discovery of these gene mutations has led to major advances in the treatment of this rare disease and led to rapid resolution of its inflammatory manifestations. IL-1 blocking agents have been found to be helpful not only in NOMID and other milder forms of CAPS, but also in other IL-1-mediated diseases, such as familial Mediterranean fever, gout/pseudogout, osteoarthritis, rheumatoid arthritis, type 2 diabetes mellitus, pyoderma gangrenosum, and other diseases as noted in . Numerous studies have shown positive effects of anakinra in patients with the above disorders. Significant studies are described in . Anakinra offers an ideal treatment option for many of these diseases due to its excellent safety profile and ease of administration subcutaneously or intravenously. The short half-life of 4–6 hours offers an additional safety benefit and allows for short-term use.
Table 2 Examples of conditions treated by anakinra
Table 3 Diseases showing positive effects of treatment with anakinra
Studies of patients with NOMID have been imperative in characterizing the extent of organ-specific inflammatory manifestations. The disease severity in NOMID is extreme and requires close monitoring of the involved organs and aggressive treatment to control both systemic and organ-specific manifestations. It is important for patients with NOMsID to receive an early diagnosis and prompt treatment, because cumulative inflammation can lead to progressive and permanent organ damage. Lepore et alCitation36 reported on patients who received an early diagnosis and prompt treatment, and had not shown any new disease-related manifestations such as hearing loss, papilledema, chronic meningitis, or mental retardation. These observations illustrate the need for prompt recognition and treatment of all CAPS phenotypes, including NOMID.
As demonstrated in the many studies of diseases treated by anakinra, the upstream mechanism or gene defect in a disease does not have as much influence as the downstream effects, including IL-1β overproduction. In NOMID syndrome, mutations in CIAS1 are found in about 50% of patients, and appear to be only one of the underlying genetic defects in this group of diseases. Recent studies suggest that treatment of patients with normal CIAS1 genetic sequencing may be successful by correction of the downstream effects (IL-1β overproduction) regardless of the upstream mechanism (CIAS1 defect). This imbalance of IL-1β production can be alleviated by administration of anakinra. Anakinra has been shown to achieve rapid and sustained clinical remission for the majority of CAPS patients, including NOMID syndrome, and many other disease states.
Disclosure
The authors report no conflicts of interest in this work.
References
- StojanovSKastnerDLFamilial autoinflammatory diseases: genetics, pathogenesis and treatmentCurr Opin Rheumatol200517558659916093838
- DhimoleaEInterleukin-1beta inhibitors for the treatment of cryopyrin-associated periodic syndromeAppl Clin Genet20114212723776364
- CuissetLJeruIDumontBMutations in the autoinflammatory cryopyrin-associated periodic syndrome gene: epidemiological study and lessons from eight years of genetic analysis in FranceAnn Rheum Dis201170349549921109514
- DamianoJSOliveiraVWelshKReedJCHeterotypic interactions among NACHT domains: implications for regulation of innate immune responsesBiochem J2004381Pt 121321915107016
- Montealegre SanchezGAHashkesPJNeurological manifestations of the Mendelian-inherited autoinflammatory syndromesDev Med Child Neurol200951642042819563585
- StychBDobrovolnyDFamilial cold auto-inflammatory syndrome (FCAS): characterization of symptomatology and impact on patients’ livesCurr Med Res Opin20082461577158218423104
- HoffmanHMWandererAABroideDHFamilial cold autoinflammatory syndrome: phenotype and genotype of an autosomal dominant periodic feverJ Allergy Clin Immunol2001108461562011590390
- MuckleTJWellsmUrticaria, deafness, and amyloidosis: a new heredo-familial syndromeQ J Med19623123524814476827
- PrieurAMGriscelliCArthropathy with rash, chronic meningitis, eye lesions, and mental retardationJ Pediatr198199179837252669
- NevenBMarvilletITerradaCLong-term efficacy of the interleukin-1 receptor antagonist anakinra in ten patients with neonatal-onset multisystem inflammatory disease/chronic infantile neurologic, cutaneous, articular syndromeArthritis Rheum201062125826720039428
- HoffmanHMMuellerJLBroideDHWandererAAKolodnerRDMutation of a new gene encoding a putative pyrin-like protein causes familial cold autoinflammatory syndrome and Muckle–Wells syndromeNat Genet200129330130511687797
- SutterwalaFSOguraYSzczepanikMCritical role for NALP3/CIAS1/Cryopyrin in innate and adaptive immunity through its regulation of caspase-1Immunity200624331732716546100
- AgostiniLMartinonFBurnsKMcDermottMFHawkinsPNTschoppJNALP3 forms an IL-1beta-processing inflammasome with increased activity in Muckle–Wells autoinflammatory disorderImmunity200420331932515030775
- BauernfeindFAblasserABartokEInflammasomes: current understanding and open questionsCell Mol Life Sci201168576578321072676
- MartinonFPetrilliVMayorATardivelATschoppJGout-associated uric acid crystals activate the NALP3 inflammasomeNature2006440708123724116407889
- MariathasanSWeissDSNewtonKCryopyrin activates the inflammasome in response to toxins and ATPNature2006440708122823216407890
- FeldmeyerLKellerMNiklausGHohlDWernerSBeerHDThe inflammasome mediates UVB-induced activation and secretion of interleukin-1beta by keratinocytesCurr Biol200717131140114517600714
- ThomasPGDashPAldridgeJRJrThe intracellular sensor NLRP3 mediates key innate and healing responses to influenza A virus via the regulation of caspase-1Immunity200930456657519362023
- DuncanJAGaoXHuangMTNeisseria gonorrhoeae activates the proteinase cathepsin B to mediate the signaling activities of the NLRP3 and ASC-containing inflammasomeJ Immunol2009182106460646919414800
- ManjiGAWangLGeddesBJPYPAF1, a PYRIN-containing Apaf1-like protein that assembles with ASC and regulates activation of NF-kappa BJ Biol Chem200227713115701157511786556
- MariathasanSNewtonKMonackDMDifferential activation of the inflammasome by caspase-1 adaptors ASC and IpafNature2004430699621321815190255
- FedericiSCaorsiRGattornoMThe autoinflammatory diseasesSwiss Med Wkly2012142w1360222714396
- DodeCLe DuNCuissetLNew mutations of CIAS1 that are responsible for Muckle–Wells syndrome and familial cold urticaria: a novel mutation underlies both syndromesAm J Hum Genet20027061498150611992256
- JanssenRVerhardELankesterATen CateRvan DisselJTEnhanced interleukin-1beta and interleukin-18 release in a patient with chronic infantile neurologic, cutaneous, articular syndromeArthritis Rheum200450103329333315476236
- AksentijevichINowakMMallahMDe novo CIAS1 mutations, cytokine activation, and evidence for genetic heterogeneity in patients with neonatal-onset multisystem inflammatory disease (NOMID): a new member of the expanding family of pyrin-associated autoinflammatory diseasesArthritis Rheum200246123340334812483741
- AksentijevichID PutnamCRemmersEFThe clinical continuum of cryopyrinopathies: novel CIAS1 mutations in North American patients and a new cryopyrin modelArthritis Rheum20075641273128517393462
- LovellDJBowyerSLSolingerAMInterleukin-1 blockade by anakinra improves clinical symptoms in patients with neonatal-onset multisystem inflammatory diseaseArthritis Rheum20055241283128615818707
- HawkinsPNBybeeAAgannaEMcDermottMFResponse to anakinra in a de novo case of neonatal-onset multisystem inflammatory diseaseArthritis Rheum20045082708270915334488
- TanakaTTakahashiKYamaneMInduced pluripotent stem cells from CINCA syndrome patients as a model for dissecting somatic mosaicism and drug discoveryBlood201212061299130822723549
- HoffmanHMRosengrenSBoyleDLPrevention of cold-associated acute inflammation in familial cold autoinflammatory syndrome by interleukin-1 receptor antagonistLancet200436494471779178515541451
- RynneMMacleanCBybeeAMcDermottMFEmeryPHearing improvement in a patient with variant Muckle–Wells syndrome in response to interleukin 1 receptor antagonismAnn Rheum Dis200665453353416531551
- Goldbach-ManskyRDaileyNJCannaSWNeonatal-onset multisystem inflammatory disease responsive to interleukin-1beta inhibitionN Engl J Med2006355658159216899778
- HawkinsPNLachmannHJAgannaEMcDermottMFSpectrum of clinical features in Muckle–Wells syndrome and response to anakinraArthritis Rheum200450260761214872505
- LeslieKSLachmannHJBruningEPhenotype, genotype, and sustained response to anakinra in 22 patients with autoinflammatory disease associated with CIAS-1/NALP3 mutationsArch Dermatol2006142121591159717178985
- Kuemmerle-DeschnerJBTyrrellPNKoetterIEfficacy and safety of anakinra therapy in pediatric and adult patients with the autoinflammatory Muckle–Wells syndromeArthritis Rheum201163384084921360513
- LeporeLPaloniGCaorsiRFollow-up and quality of life of patients with cryopyrin-associated periodic syndromes treated with anakinraJ Pediatr20101572310315.e31120472245
- EconomidesANCarpenterLRRudgeJSCytokine traps: multi-component, high-affinity blockers of cytokine actionNat Med200391475212483208
- Goldbach-ManskyRShroffSDWilsonMA pilot study to evaluate the safety and efficacy of the long-acting interleukin-1 inhibitor rilonacept (interleukin-1 Trap) in patients with familial cold autoinflammatory syndromeArthritis Rheum20085882432244218668591
- HoffmanHMThroneMLAmarNJEfficacy and safety of rilonacept (interleukin-1 Trap) in patients with cryopyrin-associated periodic syndromes: results from two sequential placebo-controlled studiesArthritis Rheum20085882443245218668535
- LachmannHJLowePFelixSDIn vivo regulation of interleukin 1beta in patients with cryopyrin-associated periodic syndromesJ Exp Med200920651029103619364880
- LachmannHJKone-PautIKuemmerle-DeschnerJBUse of canakinumab in the cryopyrin-associated periodic syndromeN Engl J Med2009360232416242519494217
- LequerreTQuartierPRoselliniDInterleukin-1 receptor antagonist (anakinra) treatment in patients with systemic-onset juvenile idiopathic arthritis or adult onset Still disease: preliminary experience in FranceAnn Rheum Dis200867330230817947302
- LarsenCMFaulenbachMVaagAInterleukin-1-receptor antagonist in type 2 diabetes mellitusN Engl J Med2007356151517152617429083
- WendlingDPratiCAubinFAnakinra treatment of SAPHO syndrome: short-term results of an open studyAnn Rheum Dis20127161098110022219141
- RiganteDAnsuiniVBertoniBTreatment with anakinra in the hyperimmunoglobulinemia D/periodic fever syndromeRheumatol Int20062719710016871408
- TanALMarzo-OrtegaHO’ConnorPFraserAEmeryPMcGonagleDEfficacy of anakinra in active ankylosing spondylitis: a clinical and magnetic resonance imaging studyAnn Rheum Dis20046391041104515066864
- BotsiosCSfrisoPFurlanAPunziLDinarelloCAResistant Behcet disease responsive to anakinraAnn Intern Med2008149428428618711165
- BacconnierLJorgensenCFabreSErosive osteoarthritis of the hand: clinical experience with anakinraAnn Rheum Dis20096861078107919435727
- Stankovic StojanovicKDelmasYTorresPUDramatic beneficial effect of interleukin-1 inhibitor treatment in patients with familial Mediterranean fever complicated with amyloidosis and renal failureNephrol Dial Transplant20122751898190121931121
- NordstromDKnightALuukkainenRBeneficial effect of interleukin 1 inhibition with anakinra in adult-onset Still’s disease. An open, randomized, multicenter studyJ Rheumatol201239102008201122859346
- GhoshPChoMRawatGSimkinPAGardnerGCTreatment of acute gouty arthritis in complex hospitalized patients with anakinraArthritis Care Res (Hoboken)20136581381138423650178