
Abstract
Certolizumab pegol (CZP) is a pegylated humanized tumor necrosis factor-α inhibitor (TNFi) approved for the treatment of psoriatic arthritis (PsA) in Europe, the USA, and Latin American countries. CZP neutralizes TNF-α at its soluble and membrane portions. Due to the lack of Fc region, it does not induce complement or antibody-dependent cytotoxicity in vitro, unlike other TNFi. RAPID-PsA study, the only randomized clinical trial performed in PsA, is a Phase III clinical trial conducted in 409 PsA patients during 24 weeks. Patients were randomized to CZP (200 mg every 2 weeks or 400 mg every 4 weeks) or placebo. Patients in CZP arms reported improvements in skin disease, joint involvement, dactylitis, enthesitis, and quality of life. Safety profile was similar to that reported for other TNF-α inhibitors in PsA patients. This article summarizes the pharmacology and reviews the efficacy and tolerability of this drug in PsA. CZP is the newest TNFi with proved efficacy in all manifestations of psoriasis disease, except for axial involvement where the evidence has been derived from response to axial spondyloarthritis.
Introduction
Psoriatic arthritis (PsA) is a chronic inflammatory musculoskeletal disease associated with psoriasis (Ps). The prevalence of PsA in the general population has been found to vary among different countries and different studies, with a median of 180 cases per 105 population.Citation1,Citation2 Between 6% and 42% of patients with Ps have PsA.Citation3 PsA that was once thought as a benign rheumatic disease is nowadays considered a progressive disease, where a substantial number of patients can develop erosions and major structural damage.Citation4–Citation7 PsA has a negative impact on the quality of life, both physically and emotionally, compared with the general population and with Ps patients. Also, as described in patients with rheumatoid arthritis (RA), PsA patients have impaired functional capacity, and increased mortality rate, particularly from cardiovascular disease.Citation8–Citation11
PsA is a complex and heterogeneous disease, since there are different facets in the phenotypic expression of the disease. The response to different treatments may vary according to axial or peripheral joint involvement, and also, extra-articular manifestations (skin, nails), enthesitis, and dactylitis.Citation12 Another factor to keep in mind for assessing response to treatment is the presence of metabolic syndrome. Metabolic syndrome is associated with a lower probability of achieving minimal disease activity (MDA) in PsA patients on therapy with tumor necrosis factor inhibitors (TNFi).Citation13 In a similar way, patients with PsA who are overweight and obese are less likely to achieve MDA, compared with normal-weight patients.Citation14 In addition, patients treated with etanercept and adalimumab (ADA) showed significant improvement of the various components of the metabolic syndrome (waist circumference, triglycerides, high-density lipoprotein cholesterol, and glucose), as compared with the group treated with methotrexate (MTX).Citation15 As seen in RA, new paradigms in the treatment of PsA have emerged in recent years and have gained great acceptance in the rheumatology community.Citation16 These include early treatment,Citation17 remission as a therapeutic goal,Citation18 the assessment of joint and extra-articular involvement of this heterogeneous disease,Citation19 and frequent measurement of disease activity in order to adjust the treatment according to the principles of Treat to Target.Citation20
Treatment of PsA has changed dramatically in recent years, despite the limited knowledge about its etiology and pathogenesis and the relative paucity of randomized controlled clinical trials, due to the introduction of biologic agents, especially TNFi. Nonbiologic disease-modifying antirheumatic drugs (DMARDs), such as MTX, sulfasalazine, and leflunomide, however, remain as the first-line therapy recommended by all clinical guidelines, even though evidence of their efficacy is scarce.Citation16,Citation21–Citation23 This recommendation is based on rheumatologists’ clinical experience and evidence from observational studies.Citation24 There are five TNFi approved by the US Food and Drug Administration for use in PsA: infliximab (IFX), etanercept, ADA, golimumab, and most recently, certolizumab pegol (CZP).Citation25–Citation29 TNF-α is a proinflammatory cytokine that is found in soluble form or bounded to the membrane of macrophages and lymphocytes. Elevated levels of TNF-α have been found in the targeted tissues of patients with different chronic inflammatory diseases. This finding, together with data on the clinical efficacy of pharmacological blockade of this cytokine, has confirmed the essential role of TNF-α in the pathogenesis of conditions such as RA, spondyloarthropathies, PsA, and Crohn’s disease.Citation30 TNF-α plays a key role in the pathogenesis of Ps and PsA by inducing the production of other inflammatory cytokines such as interleukin (IL)-1, IL-6, IL-8, and several matrix metalloproteinases. Also, it causes joint damage by stimulating bone resorption and inhibiting bone formation. TNF-α also contributes to vascular proliferation, the relevant phenomenon in many inflammatory diseases. Treatments that block some of these cytokines have shown not only improvement on joint damage but also prevention of cardiovascular damage as well.Citation31
All anti-TNF agents have shown comparable efficacy in the treatment of peripheral arthritis in PsA and there is also strong evidence that they improve skin involvement, dactylitis, and enthesitis.Citation32,Citation33 An important difference from RA is that biologic agents in PsA may be used as monotherapy, although data from some registers have shown increased survival of anti-TNF with the concomitant use of MTX.Citation16 In this review, we describe the evidence for the use of CZP in the treatment of active PsA, with focus on its mechanism of action, efficacy, and safety.
Certolizumab pegol
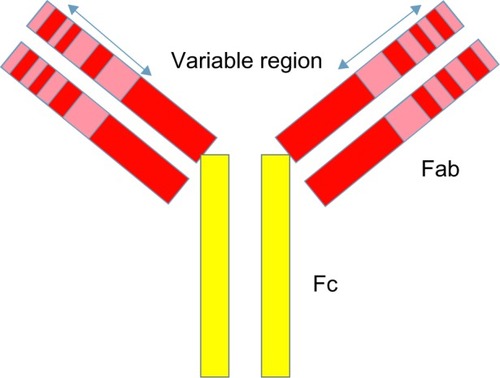
There are two important regions of antibodies, the fragment antigen-binding (Fab) and the fragment crystallizable (Fc) regions (). The Fab region contains complementarity-determining regions, unique sequences of amino acids responsible for binding antigen. The Fc region is not antigen specific, but is necessary for other antibody functions such as complement fixation and cell lysis.
Figure 1 Antibody structure. Each chain is divided into regions or domains.
Abbreviations: Fab, fragment antigen-binding; Fc, fragment crystallizable.
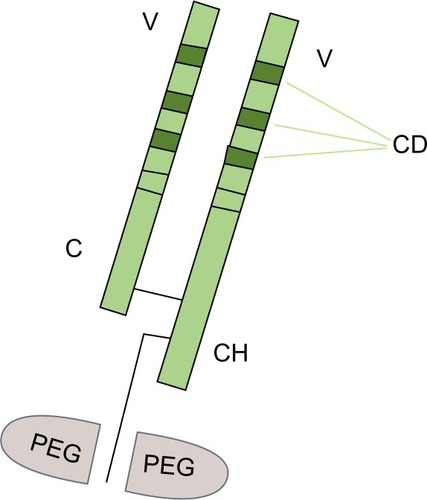
CZP is a novel TNFi formed by a humanized Fab fragment (50 kDa) fused to a 40 kDa polyethylene glycol (PEG) moiety (a nontoxic and nonimmunogenic polymer) (). The lack of Fc region in CZP prevents activities such as complement fixation and antibody-mediated cytotoxicity. The attachment of the 40 kDa PEG moiety to the Fab fragment markedly increases the half-life of CZP to a value comparable with that of a whole antibody product.Citation30,Citation31
Figure 2 Certolizumab pegol.
Abbreviations: C, constant region; CD, complimentary domain; CH, constant heavy chain region; PEG, polyethylene glycol; TNF, tumor necrosis factor; V, variable region; Fab, fragment antigen-binding.
Mechanism of action
CZP specifically recognizes and neutralizes human TNF, both the soluble and membrane-bound forms, in a dose-dependent manner. Its mechanism of action was studied in vitro and compared with that of IFX, ADA, and etanercept, which showed that affinity and neutralizing activity to human soluble TNF was superior to IFX and ADA.Citation34 The abilities of CZP to neutralize membrane TNF-mediated signaling are comparable to ADA and IFX, while etanercept may be somewhat less potent. CZP does not induce apoptosis in cultured lymphocytes and monocytes obtained from peripheral blood of healthy donors.Citation35,Citation36 Like IFX and ADA (but not etanercept), it inhibits lipopolysaccharide-induced production of IL-1β.Citation34 As this nanomolecule does not require glycosylation for function, this drug can be produced in Escherichia coli, a bacterial host. This makes the production of CZP potentially less expensive than the existing anti-TNF-α therapies.Citation37
Pharmacological properties
The pharmacological properties can be summarized as follows:Citation38
inhibits soluble and membrane-bounded TNF in a dose-dependent manner;
inhibits lipopolysaccharide-induced TNF-α and IL-1β production in human monocytes;
due to the lack of the Fc region, does not induce complement or antibody-dependent cytotoxicity in vitro;
induces nonapoptotic cell death, probably via signaling transmembrane TNF-α;
probably because of PEGylation, it is distributed into inflamed tissues to a greater extent than IFX and ADA.
CZP has the following pharmacokinetic characteristics:
Its circulatory half-life is approximately 14 days for all doses administered.
Pharmacokinetics of the PEG moiety is dependent on renal function, as it is excreted through the kidneys.
Following subcutaneous administration, peak plasma concentration is reached between 54 and 171 hours, and bioavailability after subcutaneous injection is 80% compared with the intravenous route.
Coadministration of CZP and MTX has no significant effect on the pharmacokinetics of the latter.
MTX-treated patients have lower rates of anti-CZP antibodies; therefore, therapeutic plasma levels of CZP tend to last longer when administered together with MTX.
Clinical efficacy
In 2009, the European Commission approved CZP for the treatment of active PsA in adults with inadequate response to previous DMARD therapy. In 2013, the US Food and Drug Administration approved CZP for the treatment of adult patients with active PsA. The recommended dose of CZP for adult patients with PsA is 400 mg (given as two subcutaneous injections of 200 mg each) initially and at weeks 2 and 4, followed by 200 mg every other week or 400 mg every 4 weeks (Q4W) for maintenance dosing.Citation11
RAPID-PsA, a 24-week double-blind and placebo-controlled trial of CZP in 409 patients with active PsA, was the pivotal study for CZP approval.Citation27 Patients with diagnosis of PsA according to the Classification Criteria for Psoriatic Arthritis with active disease (≥3 tender joints, ≥3 swollen joints, erythrocyte sedimentation rate ≥28 mm/h (Westergren) or C-reactive protein >7.9 mg/L) were recruited. Patients had previously failed ≥1 DMARD. Concomitant and permitted DMARDs were MTX, with doses up to 25 mg/week, sulfasalazine, up to 3 g/day, and leflunomide, up to 20 mg/day, and were used by 70% of patients. Almost 20% of recruited patients had received one previous TNFi. At baseline, 26% of patients had dactylitis and 64% had enthesitis. Patients were randomized 1:1:1 to placebo every 2 weeks (Q2W), or 400 mg CZP at weeks 0, 2, and 4, followed by either 200 mg CZP Q2W or 400 mg CZP Q4W.
At week 12, statistically significant numbers of CZP patients achieved the clinical primary endpoint: American College of Rheumatology 20% (ACR20) responses (58% CZP 200 every other week, 52% CZP 400 Q4W) compared with 24% of patients receiving placebo (P<0.001). The other primary endpoint was radiographic progression from baseline to week 24 as measured by van der Heijde modified Total Sharp Score (mTSS), which would be discussed in the “Radiographic progression” section.
Secondary endpoints included ACR20/50/70 at week 24, physical function measured by change in Health Assessment Questionnaire-Disability Index (HAQ-DI), and 75% and 90% reduction in the Psoriasis Area and Severity Index (PASI 75/90).Citation27,Citation39 At week 24, mean change from baseline in Health Assessment Questionnaire was –0.50 (CZP combined arms) versus –0.19 (placebo).
At week 24, statistically significant higher number of patients in CZP group achieved PASI 75 response (62% of patients receiving CZP 200 mg Q2W and 60% of patients receiving CZP 400 mg Q4W) compared with 15% of patients receiving placebo.Citation27 In addition, PASI 90 response rates were higher in CZP groups compared with placebo through week 24. At these points, MDA was achieved in 33% of patients receiving CZP 200 mg Q2W and 34% of patients receiving CZP 400 mg Q4W, compared with 6% of patients in the placebo group.Citation27 ACR20/50/70 responses, MDA, HAQ-DI, pain (visual analog scale), and PASI 75 remained stable from week 24 to 48 in the CZP groups ().Citation40
Table 1 Efficacy of CZP in patients with psoriatic arthritis (RAPID-PsA trial)
In patients with or without previous TNFi treatment, ACR response rates were higher in patients in CZP arms.Citation40
MTX was the most common concomitant DMARD, with similar use across treatment groups.Citation27 Concomitant DMARD use did not appear to affect response to CZP as there were similar ACR20 (56.8 vs 50.0) and PsA response criteria (68.3 vs 73.0) responses at week 12 for patients with and without concomitant DMARD use, respectively.Citation27
Improvements in joints involvement, skin, enthesitis, dactylitis, and nail disease were seen as soon as only 1 week and maintained over time.Citation27
Patient-reported outcomes
In 2014, Gladman et alCitation39 published the impact of CZP on patient-reported outcomes (PROs) in patients with PsA with or without previous exposure to the use of TNFi from the RAPID-PsA trial.Citation27 The PROs assessed were HAQ-DI, health status (measured by the Short Form-36 health survey), Psoriatic Arthritis Quality of Life, Fatigue Assessment Scale, patient assessment of pain (visual analog scale), and Dermatology Life Quality Index. At baseline, all patients had a significant impairment in functionality and quality of life. CZP led to rapid and significant improvement in all PROs at week 24, irrespective of previous TNFi exposure. In contrast with other TNFi studies, in this trial, PROs had poor correlation with clinical outcomes.
Productivity
PsA has a great impact on the state of employment and labor productivity, both outside and within the home. A high proportion of patients with PsA suffer severe disability and loss of work productivity, and many of them are forced to early retirements due to inability to perform work activities.Citation41,Citation42 Kavanaugh et alCitation43 evaluated, in the RAPID-PsA study, the effect of CZP on productivity outside and within the home. The authors used the Work Productivity Survey, which is an innovative validated questionnaire assessing the impact of arthritis on patient productivity in the workplace and at home, and on participation in family, social, and leisure activities. CZP led to quick and significant improvements in the workplace and household productivity. This was accomplished as soon as 4 weeks and continued through week 24. CZP treatment allowed reducing absenteeism and presenteeism for employed patients in both active drug treatment groups, compared with placebo, and also improved productivity within the home, with fewer days of lost participation in family, social, and leisure activities per month.
Radiographic progression
Radiographic progression was one of the primary endpoints in the RAPID PsA study, and was measured as a change from baseline to week 24, of the van der Heijde mTSS.Citation44 The mTSS nonprogression rate was higher in CZP than in placebo group in all analyses.Citation44 This effect was maintained in CZP groups up to week 48.Citation44
Multiple post hoc analyses demonstrated that CZP inhibited radiographic progression compared with placebo, particularly in patients with high baseline mTSS and C-reactive protein levels.Citation44
Axial involvement
Treatment recommendations for axial disease are derived from diagnostic criteria, screening, monitoring, and response to therapy in ankylosing spondylitis since these data are not available for axial PsA.Citation23 The RAPID trial did not assess axial involvement in PsA.Citation27 In the RAPID-axSpA trial, CZP rapidly reduced the signs and symptoms of axial Spondyloarthritis (axSpA).Citation45 In that trial, patients with PsA and axial involvement were not excluded, but were not reported separately. Experts in PsA agree from own experience that efficacy of TNFi on axial involvement in PsA is similar to that in axSpA.Citation23,Citation46
Safety
CZP showed a good safety profile in randomized clinical trials in patients with RA.
In patients with PsA, nasopharyngitis (8.7% in CZP group vs 7.4% in placebo) and upper respiratory tract infections (7.8% in CZP group vs 5.1% in placebo) were the most common adverse events in CZP combined group through week 24.Citation27 The most common noninfectious adverse events were headache (3.6% in CZP vs 1.5% in placebo) and diarrhea (3.6% in CZP vs 2.9% in placebo).Citation27
Increases in liver enzymes were more frequently reported in CZP patients.Citation27
Injection site reactions such as erythema, hematoma, itching, pain, and swelling were more frequently observed in CZP groups than in placebo group.Citation27
Antibodies to CZP were detectable in approximately 11.7% of patients at week 24.Citation47
Two deaths occurred during the first 24 weeks; one myocardial infarct in the CZP 200 mg Q2W group and one sudden death of unknown cause in the CZP 400 mg Q4W group. Both deaths were considered unrelated to study medication by the investigators.Citation27
In patients with PsA, three malignancies (two cases of breast cancer and one case of lymphoma) were reported during the dose-blind and open-label periods, of which two were fatal (lymphoma and one case of breast cancer).Citation47 The profile of malignancies with CZP in patients with PsA was generally similar to that seen earlier in patients with RA.
Pregnancy
CZP cross-placental transfer is different from that of other TNFi. Because it is not actively transported across the placenta, concentrations in the fetus would be expected to be lower, and hence, its use is potentially safer during pregnancy than the other TNFi currently available.
Recently, 31 pregnant women with inflammatory bowel disease receiving IFX (n=11), ADA (n=10), or CZP (n=10) were studied.Citation48 Serum concentrations of the drugs were measured at birth in the mother, infant, and in cord blood, and then monthly in the infant until the drugs were undetectable. Drug concentrations in the cord and in the infant at birth were compared with those of the mother. Concentrations of IFX and ADA, but not CZP, were higher in infants at birth and their cords than in their mothers. The levels of CZP in infants and their cords were <2 g/mL. The median level of IFX in the cord was 160% that of the mother, the median level of ADA in the cord was 153% that of the mother, and the median level of CZP in the cord was 3.9% that of the mother. IFX and ADA could be detected in the infants for as long as 6 months. No congenital anomalies or serious complications were reported.Citation48
In a retrospective analysis of the UCB Pharma global safety database, all medically confirmed cases of pregnancy during clinical trials of CZP and postmarketing reports through March 28, 2013, were included. Of 625 reported pregnancies, 372 (59.5%) had known outcomes. Paternal exposure pregnancies (n=33) reported 27 live births, four miscarriages, one induced abortion, and one stillbirth. Maternal exposure pregnancies (n=339) reported 254 live births, 52 miscarriages, 32 induced abortions, and one stillbirth. Almost all reported pregnancies had exposure to CZP in the first trimester, when organogenesis takes place, and a third of them continued the drug into the second and/or third trimesters. The most frequent indications for maternal CZP use were Crohn’s disease (192/339) and rheumatic diseases (118/339). Twelve cases of congenital malformation and a single neonatal death were reported. Out of 253 pregnancies with known outcomes, 191 (75.5%) resulted in live births, 37 (14.6%) in spontaneous miscarriages, and 25 (9.9%) women had elective terminations.Citation49 Of the 191 live births after maternal CZP exposure, there were three reported cases of congenital disorder. These rates are similar to what is observed in the general population; none of these events were considered related to CZP administration by the treating physicians.Citation50,Citation51
CZP loading dose
The recommendation for treatment of RA with CZP includes an initial loading dose (LD) of 400 mg at weeks 0, 2, and 4, followed by a maintenance dose of CZP 200 mg Q2W or 400 mg Q4W. Several other anti-TNFs also employ a boosted dosing regimen during the initial phase of treatment. For example, the IFX dosing schedule for RA treatment specifies short intervals between the first three infusions (3 mg/kg at 0, 2, and 6 weeks), followed by a dosing interval of every 8 weeks during the maintenance phase.Citation52 In addition, ADA requires an initial LD in several diseases including Crohn’s disease, ulcerative colitis, and plaque Ps.Citation53 The rationale for an LD is that it produces higher drug concentrations during early treatment time points, accelerates response to the drug, and reduces the production of anti-monoclonal drug antibodies. Takeuchi et alCitation54 published a post hoc analysis of two Japanese clinical studies comparing the efficacy and safety of CZP with and without LD in RA patients. Patients randomized to CZP 200 mg Q2W groups starting with LD (400 mg weeks 0/2/4) (in the J-RAPIDCitation55 trial: n=82, and in the HIKARICitation56 trial: n=116) and patients randomized to placebo groups who subsequently started CZP Q2W without LD in the Open Level Extension study (no-LD group; J-RAPID: n=61, HIKARI: n=99) were analyzed.Citation54 In both trials, the LD groups showed more rapid initial ACR20/50/70 kinetics, maintained higher ACR50/70 responses until 24 weeks, and developed anti-CZP antibodies less frequently (J-RAPID: 1.2% vs 4.9%; HIKARI: 17.2% vs 27.3%) compared to the no-LD groups. Similar safety profiles were reported between LD and no-LD groups.Citation54 This analysis, even with its limitations, provides data to support what was expected based in theory considerations.
Place in therapy
TNFi are placed in all international and local guidelines after traditional DMARDs failure,Citation21 and would remain in that place in the European League Against Rheumatism and Group for Research and Assessment of Psoriasis and Psoriatic Arthritis new recommendations that are going to be published soon. In that sense, CZP should be placed as another TNFi option. The evidence of efficacy in all domains including dactylitis and enthesitis might incline rheumatologists to choose this TNFi in patients in whom these conditions predominate. Also, the fact that CZP has evidence from randomized controlled trial for its efficacy in TNFi failures favors its use in that population. Because of the low cross-placental transfer and no detectable transfer in breast milk, CZP may be considered the TNFi of choice in pregnant patients and in the female patient considering pregnancy; however, the ultimate decision needs to be based on the clinical picture and patient preference. The risks and benefits of therapy should be individualized balancing the neonatal risks against the risk of disease flare or the course of a pregnancy with a very active disease, which might have far more consequences to neonatal development. In any case, if a pregnant patient is doing well on other TNFi, there is no indication, and even a potential risk, of switching to CZP.
Conclusion
CZP, the newest original TNFi, has shown similar efficacy when compared with the existing TNF blockers in several manifestations of Ps disease.
In a market with many options for TNF blockage, is this new TNFi offering anything different? CZP has some features that might make it an attractive option: a long half-life that allows a fortnightly or monthly subcutaneous drug regime; the lack of complement fixation with potentially less immunosuppressive effect and less cross-placental transfer; pegylation that improves distribution into inflamed tissues; and evidence that with a loading dose, quick and long-lasting efficacy could be obtained, reducing the generation of anti-TNFi (anti-ADA) antibodies.
Its safety profile looks similar to other TNFi up to now, although more data from registries are needed.
In summary, CZP is a promising TNFi with a novel composition, which is already performing according to the expectations.
Until not long ago, therapeutic options for patients with PsA were limited and of little efficacy. New options are very much welcomed by rheumatologists and patients alike.
Disclosure
ERS has received grants and/or speaking fees from and/or provided expert advice to UCB Pharma, AbbVie, Pfizer, BMS, Novartis, and Roche. JR has received speaking fees from AbbVie and Pfizer. The authors report no other conflicts of interest in this work.
References
- AlamanosYVoulgariPVDrososAAIncidence and prevalence of psoriatic arthritis: a systematic reviewJ Rheumatol20083571354135818464305
- SorianoERRosaJVelozoEIncidence and prevalence of psoriatic arthritis in Buenos Aires, Argentina: a 6-year health management organization-based studyRheumatology (Oxford)201150472973421134962
- GladmanDDAntoniCMeasePCleggDONashPPsoriatic arthritis: epidemiology, clinical features, course, and outcomeAnn Rheum Dis200564Suppl 2ii14ii1715708927
- Torre AlonsoJCRodriguez PerezAArribas CastrilloJMBallina GarciaJRiestra NoriegaJLLopez LarreaCPsoriatic arthritis (PA): a clinical, immunological and radiological study of 180 patientsBr J Rheumatol19913042452501863819
- GladmanDDShuckettRRussellMLThorneJCSchachterRKPsoriatic arthritis (PSA) – an analysis of 220 patientsQ J Med1987622381271413659255
- OryPAGladmanDDMeasePJPsoriatic arthritis and imagingAnn Rheum Dis200564Suppl 2ii55ii5715708938
- SiannisFFarewellVTCookRJSchentagCTGladmanDDClinical and radiological damage in psoriatic arthritisAnn Rheum Dis200665447848116126794
- RosenCFMussaniFChandranVEderLThavaneswaranAGladmanDDPatients with psoriatic arthritis have worse quality of life than those with psoriasis aloneRheumatology (Oxford)201251357157622157469
- HustedJAGladmanDDFarewellVTLongJACookRJValidating the SF-36 health survey questionnaire in patients with psoriatic arthritisJ Rheumatol19972435115179058658
- HustedJAGladmanDDFarewellVTCookRJHealth-related quality of life of patients with psoriatic arthritis: a comparison with patients with rheumatoid arthritisArthritis Rheum200145215115811324779
- HansenRBKavanaughACertolizumab pegol for the treatment of psoriatic arthritisExpert Rev Clin Immunol201511330731825651776
- GossecLSmolenJSGaujoux-VialaCEuropean League against rheumatism recommendations for the management of psoriatic arthritis with pharmacological therapiesAnn Rheum Dis201271141221953336
- CostaLCasoFRamondaRMetabolic syndrome and its relationship with the achievement of minimal disease activity state in psoriatic arthritis patients: an observational studyImmunol Res2015611–214715325395342
- EderLThavaneswaranAChandranVCookRJGladmanDDObesity is associated with a lower probability of achieving sustained minimal disease activity state among patients with psoriatic arthritisAnn Rheum Dis201574581381724431392
- CostaLCasoFAttenoMImpact of 24-month treatment with etanercept, adalimumab, or methotrexate on metabolic syndrome components in a cohort of 210 psoriatic arthritis patientsClin Rheumatol201433683383923959447
- SorianoERAcosta-FelquerMLLuongPCaplanLPharmacologic treatment of psoriatic arthritis and axial spondyloarthritis with traditional biologic and non-biologic DMARDsBest Practice Res Clin Rheumatol2014285793806
- GladmanDDEarly psoriatic arthritisRheum Dis Clin North Am201238237338622819090
- Acosta FelquerMLFerreyra GarrottLMarinJRemission criteria and activity indices in psoriatic arthritisClin Rheumatol20143391323133024820142
- GladmanDDMeasePJStrandVConsensus on a core set of domains for psoriatic arthritisJ Rheumatol20073451167117017477480
- SchoelsMMBraunJDougadosMTreating axial and peripheral spondyloarthritis, including psoriatic arthritis, to target: results of a systematic literature search to support an international treat-to-target recommendation in spondyloarthritisAnn Rheum Dis201473123824223740234
- SorianoERTreatment guidelines for psoriatic arthritisInt J Clin Rheumatol20094329342
- CasoFCostaLDel PuenteAPharmacological treatment of spondyloarthritis: exploring the effectiveness of nonsteroidal anti-inflammatory drugs, traditional disease-modifying antirheumatic drugs and biological therapiesTher Adv Chronic Dis20156632833826568809
- CoatesLCKavanaughAMeasePJGroup for research and assessment of psoriasis and psoriatic arthritis: Treatment recommendations for psoriatic arthritis 2015Arthritis Rheumatol Epub201618
- SorianoERThe actual role of therapy with traditional disease- modifying antirheumatic drugs in psoriatic arthritisJ Rheumatol Suppl201289677022751597
- MeasePJGoffeBSMetzJVanderStoepAFinckBBurgeDJEtanercept in the treatment of psoriatic arthritis and psoriasis: a randomised trialLancet2000356922738539010972371
- MeasePJGladmanDDRitchlinCTAdalimumab for the treatment of patients with moderately to severely active psoriatic arthritis: results of a double-blind, randomized, placebo-controlled trialArthritis Rheum200552103279328916200601
- MeasePJFleischmannRDeodharAAEffect of certolizumab pegol on signs and symptoms in patients with psoriatic arthritis: 24-week results of a Phase 3 double-blind randomised placebo-controlled study (RAPID-PsA)Ann Rheum Dis2014731485523942868
- AntoniCEKavanaughAvan der HeijdeDTwo-year efficacy and safety of infliximab treatment in patients with active psoriatic arthritis: findings of the Infliximab Multinational Psoriatic Arthritis Controlled Trial (IMPACT)J Rheumatol200835586987618381786
- KavanaughAMcInnesIMeasePGolimumab, a new human tumor necrosis factor alpha antibody, administered every four weeks as a subcutaneous injection in psoriatic arthritis: Twenty-four-week efficacy and safety results of a randomized, placebo-controlled studyArthritis Rheum200960497698619333944
- Delgado FriasEDiaz GonzalezJFCertolizumab pegolRheumatol Clin20116S3S7S11 Spanish
- ChimentiMSSaracenoRChiricozziAGiuntaAChimentiSPerriconeRProfile of certolizumab and its potential in the treatment of psoriatic arthritisDrug Des Devel Ther20137339348
- FelquerMLSorianoERNew treatment paradigms in psoriatic arthritis: an update on new therapeutics approved by the U.S. Food and Drug AdministrationCurr Opinion Rheumatol201527299106
- CasoFLubranoEDel PuenteAProgress in understanding and utilizing TNF-alpha inhibition for the treatment of psoriatic arthritisExpert Rev Clin Immunol2015117
- NesbittAFossatiGBerginMMechanism of action of certolizumab pegol (CDP870): in vitro comparison with other anti-tumor necrosis factor alpha agentsInflamm Bowel Dis200713111323133217636564
- LugeringASchmidtMLugeringNPauelsHGDomschkeWKucharzikTInfliximab induces apoptosis in monocytes from patients with chronic active Crohn’s disease by using a caspase-dependent pathwayGastroenterology200112151145115711677207
- ShenCAsscheGVColpaertSAdalimumab induces apoptosis of human monocytes: a comparative study with infliximab and etanerceptAliment Pharmacol Ther200521325125815691299
- RosaJSabelliMSorianoERPrefilled certolizumab pegol (Cimzia((®))) syringes for self-use in the treatment of rheumatoid arthritisMed Devices (Auckl)20103253122915918
- DhillonSCertolizumab pegol: a review of its use in patients with axial spondyloarthritis or psoriatic arthritisDrugs2014749999101624919863
- GladmanDFleischmannRCoteurGWolteringFMeasePJEffect of certolizumab pegol on multiple facets of psoriatic arthritis as reported by patients: 24-week patient-reported outcome results of a phase III, multicenter studyArthritis Care Res (Hoboken)20146671085109224339179
- MeasePFleischmannRWollenhauptJEffect of certolizumab pegol over 48 weeks on signs and symptoms in patients with psoriatic arthritis with and without prior tumor necrosis factor inhibitor exposureArthritis Rheum201365SupplS132
- TillettWde-VriesCMcHughNJWork disability in psoriatic arthritis: a systematic reviewRheumatology (Oxford)201251227528321752872
- MeasePJMenterMAQuality-of-life issues in psoriasis and psoriatic arthritis: outcome measures and therapies from a dermatological perspectiveJ Am Acad Dermatol200654468570416546593
- KavanaughAGladmanDvan der HeijdeDPurcaruOMeasePImprovements in productivity at paid work and within the household, and increased participation in daily activities after 24 weeks of certolizumab pegol treatment of patients with psoriatic arthritis: results of a phase 3 double-blind randomised placebo-controlled studyAnn Rheum Dis2015741445124942382
- van der HeijdeDFleischmannRWollenhauptJEffect of different imputation approaches on the evaluation of radiographic progression in patients with psoriatic arthritis: results of the RAPID-PsA 24-week phase III double-blind randomised placebo-controlled study of certoli-zumab pegolAnn Rheum Dis201473123323723942869
- LandewéRBraunJDeodharAEfficacy of certolizumab pegol on signs and symptoms of axial spondyloarthritis including ankylosing spondylitis: 24-week results of a double-blind randomised placebo-controlled Phase 3 studyAnn Rheum Dis2014731394724013647
- NashPLubranoECauliATaylorWJOlivieriIGladmanDDUpdated guidelines for the management of axial disease in psoriatic arthritisJ Rheumatol201441112286228925362712
- European Medicines AgencyAnnex 1: summary of product characteristics (Cimzia) Available from: www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/001037/WC500069763.pdfwww.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/001037/WC500069763.pdfAccessed October 18, 2014
- MahadevanUWolfDCDubinskyMPlacental transfer of anti-tumor necrosis factor agents in pregnant patients with inflammatory bowel diseaseClin Gastroenterol Hepatol2013113286292 quiz e22423200982
- ClowseMEWolfDCForgerFPregnancy outcomes in subjects exposed to certolizumab pegolJ Rheumatol201542122270227826523031
- WakefieldIStephensSFoulkesRNesbittABourneTThe use of surrogate antibodies to evaluate the developmental and reproductive toxicity potential of an anti-TNFalpha PEGylated Fab’ monoclonal antibodyToxicol Sci2011122117017621507990
- MarchioniRMLichtensteinGRTumor necrosis factor-alpha inhibitor therapy and fetal risk: a systematic literature reviewWorld J Gastroenterol201319172591260223674866
- Remicade (infliximab) prescribing information2013 Available from: http://www.remicade.com/shared/product/remicade/prescribing-information.pdfAccessed March 10, 2016
- Humira (adalimumab) prescribing information2014 Available from: http://www.rxabbvie.com/pdf/humira.pdfAccessed March 10, 2016
- TakeuchiTYamamotoKYamanakaHPost-hoc analysis showing better clinical response with the loading dose of Certolizumab pegol in Japanese patients with active rheumatoid arthritisMod Rheumatol2015126
- YamamotoKTakeuchiTYamanakaHEfficacy and safety of certolizumab pegol plus methotrexate in Japanese rheumatoid arthritis patients with an inadequate response to methotrexate: the J-RAPID randomized, placebo-controlled trialMod Rheumatol201424571572424313916
- YamamotoKTakeuchiTYamanakaHEfficacy and safety of certolizumab pegol without methotrexate co-administration in Japanese patients with active rheumatoid arthritis: the HIKARI randomized, placebo-controlled trialMod Rheumatol201424455256024981319