
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Purpose
To compare the efficacy and outcome of phakic toric implantable collamer lens (TICL) and refractive clear lens extraction with AcrySof Toric intraocular lens (TIOL) implantation for the treatment of myopic astigmatism.
Patients and methods
This study assessed eyes with myopic astigmatism >−1 D and ≤−4 D with a spherical equivalent >10 D or <10 D if the patients were unsuitable for corneal refractive surgery. These eyes were divided into group A, in which Visian Toric ICL™ Phakic TICL was implanted, and group B, which involved clear lens extraction with implantation of an AcrySof IQ toric SN60T3-9™ IOL. The outcome and complications were evaluated.
Results
This study enrolled 63 eyes of 38 patients with a follow-up period of at least 6 months. The mean postoperative spherical equivalent was −0.19±0.31 D in group A and −0.21±0.28 D in group B (P=0.69). The mean postoperative cylinder value was −0.46±0.53 D in group A and −0.32±0.41 D in group B (P=0.35). Postoperative cylinder was <1 D in 76.47% and 79.31% of eyes in groups A and B, respectively. The mean endothelial cell count was reduced by 4.32% in group A and by 5.32% in group B (P=0.003). The mean postoperative intraocular pressure increased insignificantly in group A (P=0.22) and reduced significantly in group B (P=0.004). The complication rate was 11.76% in group A and 6.90% in group B.
Conclusion
Both procedures showed predictable results and good visual results. However, the loss of accommodation and risk of retinal complications in the TIOL group suggest that the use of TICL for myopic astigmatism is a better choice in younger patients.
Introduction
Astigmatic correction has become a longstanding topic of debate, from the traditional use of spectacles and contact lenses to the era of keratotomy and laser-assisted in situ keratomileusis (LASIK).Citation1 Although LASIK is widely accepted among ophthalmologists, its effects on the clear, central, corneal zone are associated with a number of intraoperative and postoperative complications such as regression, haze, dry eyes, diffuse lamellar keratitis, undercorrection, and overcorrection, which have been reported to increase with increased ablation depth.Citation2–Citation5 Simultaneously, changes in corneal shape, especially in high laser ablation, may result in poor visual quality.Citation6
Techniques for surgical correction of myopic astigmatism with the implantation of toric intraocular lens (TIOL; phakic or aphakic) have advanced in the past few years.Citation7 Phacoemulsification with TIOL implantation is used not only for cataract surgeryCitation8,Citation9 but also for refractive surgery.Citation10,Citation11 TIOLs may provide greater reversibility or adjustability than some keratorefractive procedures.Citation10,Citation12–Citation14 However, this procedure is associated with an increased risk of retinal complications such as retinal detachment and cystoid macular edema.Citation15,Citation16
The AcrySof Toric IOL (Alcon Laboratories, Inc., Fort Worth, TX, USA) has the same design as the AcrySof single-piece IOL, with an additional toric component on the posterior optic surface and axis indentations indicating the flat meridian of the optic.Citation17 In contrast, the phakic toric implantable collamer lens (TICL; Visian Toric ICL™; STAAR Surgical AG, Nidau, Switzerland) was approved by a Food and Drug Administration (FDA) study for the treatment of moderate-to-high myopic astigmatism and found to show efficient and predictable results.Citation1 The use of this lens allows preservation of accommodation, stability, and reversibility,Citation2,Citation18–Citation23 but it is more expensive and can be complicated by cataract and/or glaucoma.Citation24–Citation29
Both TICL and TIOL are used for the treatment of myopic astigmatism, but the implantation techniques differ between the lenses. Both procedures have advantages and disadvantages, but there has been no prior study to compare the efficacy and safety of these two procedures.
The aim of this study was to retrospectively compare the efficacy and safety of the use of phakic TICL with refractive clear lens extraction with AcrySof TIOL implantation for the treatment of myopic astigmatism in patients aged ≤45 years.
Patients and methods
This retrospective, nonrandomized, comparative observational study was approved by the Medical Ethics Committee of Sohag Faculty of Medicine, Sohag University, and followed the tenets of the Declaration of Helsinki. All patients signed an informed consent form that explained the details of the procedure and possible complications. All cases fulfilling the inclusion criteria and with procedures that took place between August 2013 and December 2014 were included in this study.
Inclusion criteria
We included patients who were between 21 and 45 years of age with stable refraction for at least 1 year and who were seeking surgical correction of their myopic astigmatism. Eyes that showed myopic astigmatism with spherical equivalent (SE) >10 D or myopic astigmatism with SE <10 D if the patients were unsuitable for corneal refractive surgery according to guidelines suggested in the literature and had astigmatism of >1 and ≤4 D (the maximum astigmatism correction by AcrySof IQ toric is 4.11 D by the SN60T9 model) were included. For TICL cases, the anterior chamber depth (ACD) was required to be >280 µm from the endothelium. The ACDs were measured by Scheimpflug tomography (Wavelight Allegro Oculyzer; Alcon Surgical, Hünenberg, Switzerland) following the manufacturer’s recommendations.
The exclusion criteria included any ocular disease other than myopic astigmatism (cataract, glaucoma, corneal opacities, uveitis, retinal disorders), history of any ocular surgery, and corneal endothelial cell count (ECC) of <2,500 cells/mm as measured by specular microscopy.
Selection of the procedure type was dependent on clinical evaluation of every case. Eyes with ACD ≥2.8 mm were assigned for TICL implantation. Eyes with ACD <2.8 mm were assigned for phacoemulsification and TIOL implantation. The age of the patient was another factor in group assignment: TICL was used for younger patients when ACD was appropriate, whereas older patients aged >40 years underwent phacoemulsification and TIOL implantation.
The study was initially carried out on 71 eyes of 43 patients. Eight eyes of five patients were excluded from the study due to an incomplete follow-up period (they were presented to follow-up visits for 3 months, but they missed the sixth month follow-up visit), leaving a total of 63 eyes of 38 patients included in the study and with a completed follow-up period of at least 6 months.
The eyes were divided into two groups. Group A included the eyes that underwent implantation of the posterior chamber phakic TIOL for the correction of moderate-to-high myopic astigmatism (TICL group). Group B included the eyes that underwent clear lens extraction with implantation of an AcrySof IQ toric SN60T IOL (TIOL group). The number of eyes that were not candidate for corneal refractive surgery with SE <10 D was 10 eyes of five patients in group A and six eyes of three patients in group B.
Preoperative assessment
All patients underwent a complete ophthalmologic examination. This evaluation included assessments of manifest and cycloplegic refractions, uncorrected visual acuity (UCVA) and best-corrected visual acuity (BCVA) measured by chart projector and expressed as Snellen’s decimal fraction, slit-lamp microscopy, and Goldmann applanation tonometry. A peripheral retinal examination was performed to detect treatable retinal lesions. Wavelight Allegro Oculyzer was used to perform pachymetry, determine the ACD, and exclude keratoconus. Specular microscopy (Topcon SP-IP08; Topcon Corporation, Tokyo, Japan) was used to evaluate the endothelium. IOLMaster biometry (Carl Zeiss Meditec AG, Jena, Germany) was used to calculate IOL power for all cases. For group A, biometry was performed to ensure availability of these data in the future in case of cataract development in TICL patients. This was done to avoid a bias in IOL calculation in the presence of ICL. Horizontal white-to-white measurement was performed by a manual caliper to choose the appropriate TICL size. The target refraction was emmetropia in all cases.
TICL power calculation
TICL power calculations were performed according to the manufacturer’s recommendations using the astigmatic decomposition method described by Sarver and Sanders.Citation30 This formula calculates the appropriate ICL cylinder using the patient’s manifest refractive cylinder.
TICLs were manufactured to minimize rotation and required the surgeon to rotate the ICL no more than 22.5 degrees from the horizontal meridian. The size of the TICL was also chosen by the manufacturer on the basis of the horizontal white-to-white diameter and ACD. When the horizontal white-to-white diameter is
11.0 mm, we selected 12.1 mm size of TICL;
11.5 mm, we selected 12.6 mm size of TICL;
12.0 mm, we selected 13.2 mm size of TICL;
12.5 mm, we selected 13.7 mm size of TICL.
But when the horizontal white-to-white diameter is in between these sizes, eg, 11.75 mm, here the selection depends on the AC depth, ie, when AC is relatively shallow, ie, between 2.8 and 3 mm, we used the smaller size of 12.6 to avoid intraocular pressure (IOP) increase and vice versa.
Each TICL was sent to the surgeon with a guide demonstrating the amount and direction of rotation of the TICL from the horizontal axis to align the ICL cylinder axis to the patient’s required cylinder correction. The model of TICL used was V4B, which requires peripheral iridectomy to prevent pupillary block glaucoma.
TIOL power calculation
Intraocular lens cylinder power and alignment axis were calculated using a web-based TIOL calculator program (http://www.acrysoftoriccalculator.com), which considers the IOLMaster biometry and keratometry data as well as the surgically induced astigmatism.
Surgical technique for TICL
Pupil dilation was performed with cyclopentolate HCl 1% and phenylephrine 2.5% eye drops administered 1 hour before surgery. A horizontal axis marking at slit lamp was performed immediately before surgery to avoid the cyclotorsion effect in the supine position. The TICL was inserted through a 3-mm temporal clear corneal incision with a STAAR injector (Visian Toric ICL; STAAR Surgical AG) after anterior chamber formation with Provisc (sodium hyaluronate; Alcon Laboratories, Inc.). The four haptics were tucked under the iris with the manipulator provided by the manufacturer, and rotation of the ICL to the desired axis was done before pupil constriction by intracameral carbachol USP 0.01% w/v (carbodol; Sunways India Pvt Ltd, Mumbai, India). One peripheral iridectomy was done using the vitreous cutter of the Alcon infinity machine (Alcon Laboratories, Inc.) set at a cut rate of 10 cuts/min, flow rate of 15 cc/min, and vacuum of 150 mmHg. These parameters can usually yield single-round peripheral iridectomy. Irrigation was performed to remove the sodium hyaluronate, and the wounds were hydrated.
Surgical technique for TIOL
Pupil dilation was performed with cyclopentolate HCl 1% and phenylephrine 2.5% eye drops instilled 1 hour prior to surgery. A horizontal axis marking at slit lamp was performed immediately before surgery to avoid the cyclotorsion effect in the supine position. Operations were done under peribulbar local anesthesia. The intended axis of IOL placement was marked. The standard technique of sutureless coaxial phacoemulsification through a 2.4-mm temporal incision was performed using the Alcon infinity machine. Meticulous polishing of the posterior capsule and cleaning of the subcapsular epithelium were done routinely to reduce the chance of subsequent posterior capsule opacification. TIOL was injected using a Monarch 3 injector with cartridge D into the capsular bag. The viscoelastic was removed from below the IOL before the final rotation of the TIOL to the desired axis, after which the remaining viscoelastic was removed and stromal wound hydration was performed.
Postoperative treatment
Topical antibiotic eye drops containing moxifloxacin 0.3% (Vigamox; Alcon Laboratories, Inc.) were administered five times a day for 1 week. Topical eye drops containing 1% prednisolone acetate (PRED FORTE; Allergan, Inc., Irvine, CA, USA) were administered five times a day for 1 week and then gradually tapered over a period of 4 weeks.
Postoperative assessment
Postoperative visits were performed at 1 day, 1 week, 1 month, 3 months, and 6 months. Uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), slit-lamp examination, refraction, fundoscopy, and tonometry were evaluated. Wavelight Allegro Oculyzer and specular microscopy were performed at the 6-month follow-up visit. Measurements at 6 months were considered to be the final follow-up values.
Axis of rotation was measured 6 months postsurgery. Full pupil dilation was done to see the axis mark on both TICL and TIOL in the periphery. Slit lamp with rotating slit was used to determine the toric lens alignment axis and to compare it with the preoperative target axis of alignment.
Power vector analysis
Spherocylindrical refraction results were converted to power vectors expressed by three dioptric powers: M, J0, and J45, where M is equal to the SE of the given refractive error and J0 and J45 are the two Jackson cross-cylinder equivalents to the conventional cylinder. Manifest refractions were recorded in conventional script notation (sphere, cylinder, and axis) and then converted to the power vector coordinates described by Thibos and HornerCitation31 and to the overall blurring strength by the following formulas:
where M is the spherical lens equal to the SE of the given refractive error, S is the sphere, C is the cylinder, J0 represents the Jackson cross-cylinder axes at 180 degrees and 90 degrees, J45 is the Jackson cross-cylinder axes at 45 degrees and 135 degrees, α is the cylinder angle, and B is the overall blurring strength of the spherocylindrical refractive error.
Statistical analysis
Nonparametric tests were used because the data were not normally distributed. Comparison of variables was done using the Mann–Whitney U test for between-group comparisons and Wilcoxon signed rank test for comparisons within the same group. All tests were two-tailed, and a P-value of 0.05 was considered statistically significant. All statistical calculations were done using SPSS version 10.0 (SPSS Inc., Chicago, IL, USA).
Results
This study included 63 eyes of 38 patients (21 females) divided into two groups: group A underwent TICL implantation and included 34 eyes of 20 patients and group B underwent TIOL and included 29 eyes of 18 patients. and – present the pre- and postoperative data. The groups were not statistically different in any parameters except for age and ECC. The age of group B was significantly higher than that of group A (P=0.0001), which can be explained by the tendency to perform clear lens extraction in older patients. The preoperative ECC was significantly higher in group B (P=0.002).
Figure 1 Preoperative and postoperative SE.
Abbreviations: SE, spherical equivalent; TICL, toric implantable collamer lens; TIOL, refractive clear lens extraction with AcrySof Toric intraocular lens.
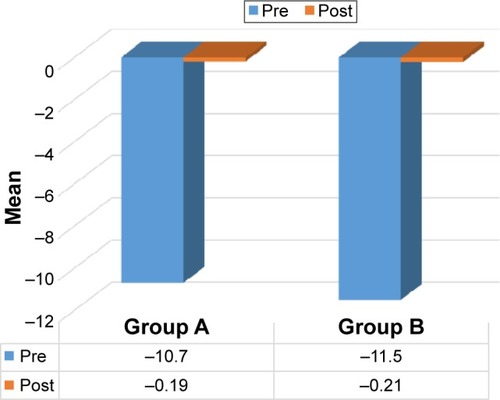
Figure 2 Preoperative and postoperative cylinder.
Abbreviations: TICL, toric implantable collamer lens; TIOL, refractive clear lens extraction with AcrySof Toric intraocular lens.
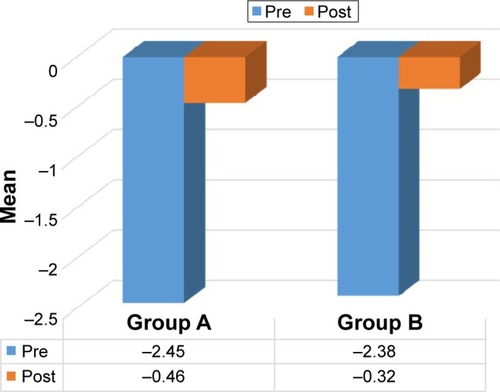
Figure 3 Preoperative and postoperative UDVA.
Abbreviations: UDVA, uncorrected distance visual acuity; TICL, toric implantable collamer lens; TIOL, refractive clear lens extraction with AcrySof Toric intraocular lens.
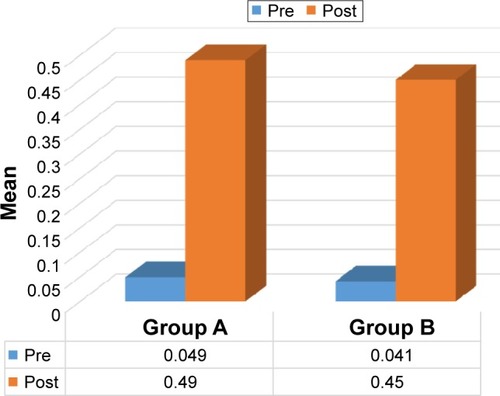
Figure 4 Preoperative and postoperative CDVA.
Abbreviations: CDVA, corrected distance visual acuity; TICL, toric implantable collamer lens; TIOL, refractive clear lens extraction with AcrySof Toric intraocular lens.
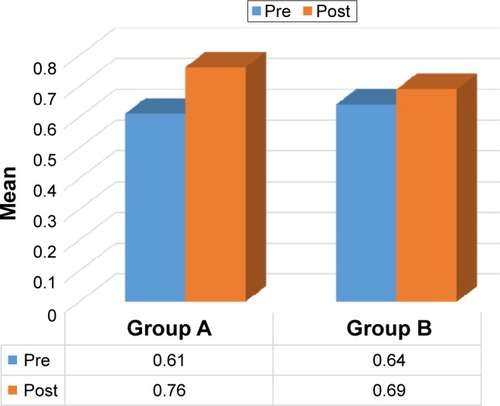
Table 1 Preoperative and postoperative data for both groups
The mean ACD was 3.17±0.21 mm (range, 2.80–3.69 mm) in group A and 2.63±0.18 mm (range, 2.42–3.01 mm) in group B. This difference between the groups was statistically significant (P<0.0001).
Treatment resulted in a significant improvement in most outcome parameters in both groups. In group A, 24 of 34 eyes (71%) showed within ±1 D SE of emmetropia postsurgery, while all eyes showed within ±2 D SE of the target refraction postsurgery. In group B, 21 of 29 eyes (72%) showed within ±1 D SE of emmetropia postoperatively, while all eyes showed within ±2 D SE of the target refraction postoperatively.
As regards safety, no eyes lost two or more lines from the preoperative CDVA in both groups.
As regards efficacy index, which is the ratio of the postoperative UDVA to the preoperative CDVA, both groups presented good efficacy index with statistically insignificant difference between both groups (P=0.21) ().
Table 2 Comparison between the efficacy index for group A and group B
The mean ECC showed a 4.32% reduction in group A and a 5.30% reduction in group B. The preoperative IOP did not show a statistically significant intergroup difference (P=0.45), while the postoperative value showed a statistically significant intergroup difference (P=0.004). Compared with the mean preoperative IOP, the mean postoperative IOP was increased in group A, but this change was not significant (P=0.22). However, in group B, the postoperative IOP was significantly reduced (P=0.004).
Power vector analysis of the astigmatism showed that both groups were comparable in all components both pre- and postoperatively. There was a statistically significant postoperative reduction in astigmatism components in both groups (). With regard to astigmatic correction, 94.12% of eyes were within ±1 D of J0 and 97.06% of eyes were within ±1 D of J45 for their astigmatic components in group A. For group B, 96.55% of eyes were within ±1 D of J0 and all eyes were within ±1 D of J45 for their astigmatic components. The difference in the vector components of the astigmatism between the groups was not statistically significant. Correlation coefficient analysis was done using Spearman’s correlation analysis to the vector components and revealed a significant positive correlation coefficient between preoperative and postoperative J0 and J45 for both groups A and B (; and ).
Figure 5 Correlation between pre- and postoperative J0.
Abbreviations: TICL, toric implantable collamer lens; TIOL, refractive clear lens extraction with AcrySof Toric intraocular lens.
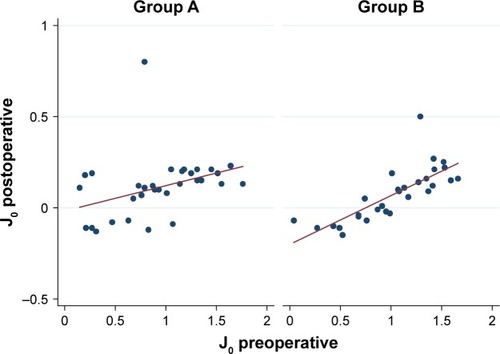
Figure 6 Correlation between pre- and postoperative J45.
Abbreviations: TICL, toric implantable collamer lens; TIOL, refractive clear lens extraction with AcrySof Toric intraocular lens.
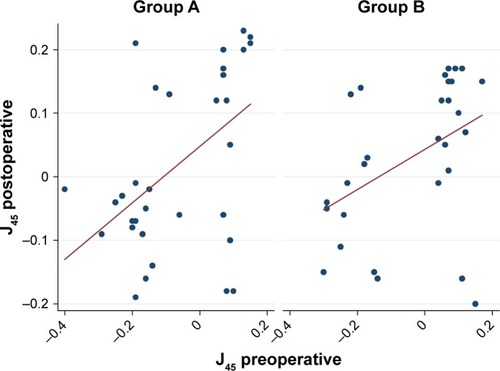
Table 3 Power vector analysis of pre- and postoperative astigmatism in both groups
Table 4 Correlation between pre- and postoperative J0 and J45
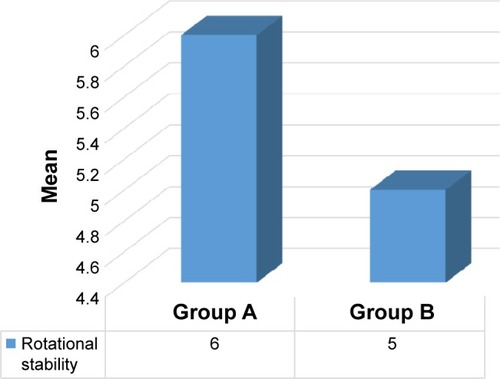
As for the rotational stability at 6 months follow-up, the mean TICL rotation in group A was 6±3.5 degrees, and in group B, the mean TIOL rotation was 5±2.9 degrees (). This difference between the groups was not statistically significant (P=0.23).
Figure 7 Comparison between the rotational stability for group A and group B.
Abbreviations: TICL, toric implantable collamer lens; TIOL, refractive clear lens extraction with AcrySof Toric intraocular lens.
Complications
Group A
One eye (2.94%) showed a transient rise of 31 mmHg in IOP on the first postoperative day, mostly due to incomplete irrigation of the viscoelastic. However, the IOP reduced again with topical anti-glaucoma drops and systemic carbonic anhydrase inhibitor tablets for 3 days; an IOP of 16 mmHg and a BCVA of 0.9 were observed at 6 months postsurgery.
TICL rotation of 30 degrees occurred in one eye (2.94%), which required repositioning of the TICL 2 weeks post-surgery by simple dialing under topical anesthesia. The final SE was −0.5 D.
Lens opacity occurred in two cases (5.88%) during the follow-up period. These cases of anterior subcapsular lens opacity required no intervention as the complication was stationary and visually insignificant.
Group B
Posterior capsule opacification occurred in two eyes (6.90%). Both eyes were treated with neodymium-doped yttrium aluminum garnet (Nd:YAG) capsulotomy after 3 months postsurgery. No other complications were observed.
Discussion
Patients with high astigmatism and high myopia and those with borderline corneal thickness and/or curvature are not candidates for corneal refractive surgery because the results are less predictable, the optical quality is lower,Citation32,Citation33 and there is an increased risk of corneal ectasia.Citation34 In such cases, intraocular procedures such as phakic TICL implantation and refractive clear lens extraction with TIOL implantation are used for the treatment of myopic astigmatism. These two techniques allow optical correction of refractive errors while preserving the normal physiologic corneal contour.
This study aimed to compare the effectiveness of phakic TICL with refractive clear lens extraction with AcrySof TIOL implantation for the treatment of myopic astigmatism. This is the first study to compare these two lens implantations for the treatment of myopic astigmatism. The findings showed a strong correlation between the postoperative refraction and the target preoperative refraction in both groups, with more than three quarters of the eyes having a postoperative cylinder <1 D. These differences in postoperative refraction between both groups were not statistically significant.
The power vector analysis of astigmatism showed that the postoperative cylindrical components of refraction were not significantly different from zero. Although group B showed slightly better results with regard to the vector components of the astigmatism, the intergroup difference was not statistically significant. The slightly better refractive results in group B can be explained by the differences in wound size. In the case of TICL, we used a 3 mm incision that was intended to induce with-the-rule astigmatism of ~0.5 D,Citation35 whereas the TIOL required an incision of 2.4 mm in order to induce less astigmatism.
The UCVA improved in both groups, and the intergroup difference was not statistically significant 6 months after surgery (P=0.27). Additionally, the mean IOP in group A showed an increase postsurgery, which was not statistically significant (P=0.22), while that in group B showed a statistically significant difference (P=0.004). The intergroup difference in the postoperative IOP was statistically significant (P=0.004), with the higher IOP in group A being attributable to the vaulting of the TICL with the subsequent forward iris push leading to a shallowing of the anterior chamber.Citation36,Citation37 In contrast, in group B, the IOP reduction may be explained by the decreased resistance to aqueous outflow due to the deepening of the anterior chamber after lens extraction and/or hyposecretion of the aqueous humor due to postoperative capsular bag fibrosis with traction on the ciliary body via the zonules.Citation38–Citation41
For group A, the postoperative mean IOP results were comparable to those obtained by Kamiya et alCitation42 and in accordance with an FDA studyCitation1 that reported no significant rise in IOP after TICL implantation. The mean ECC dropped by 4.32% in group A and by 5.32% in group B at 6 months postsurgery. This difference was statistically significant (P=0.003), and it can be explained by the greater intraocular manipulation and the larger amounts of irrigation fluid used with TIOL during the phacoemulsification, which results in greater endothelial cell loss. The percentage of ECC loss for group A was similar to that reported by Kamiya et al,Citation42 who described an ECC loss of 4.29% 6 months after TICL implantation. Additionally, both groups showed similarly good rotational stability 6 months after surgery, with negligible effect on the postoperative refraction.
We observed several complications associated with both procedures. One eye in group A (2.94%) developed a transient IOP increase of 31 mmHg on the first day post-surgery that was mostly due to residual viscoelastic. This was controlled with medical treatment for 3 days, and the IOP returned to 16 mmHg without medication during the follow-up period without any effect on vision (BCVA was 0.9 at 6 months). Also, one eye (2.94%) in group A showed spontaneous rotation of the TICL 10 days postsurgery with a sudden drop in vision, and TICL repositioning by simple dialing under topical anesthesia was performed 2 weeks postsurgery with a final BCVA of 0.8 at the end of the follow-up period. Two eyes (5.88%) developed subcapsular cataracts, which were stationary and visually insignificant (one of these was the eye that required dialing). In group B, two eyes (6.9%) developed subsequent cataract that required YAG laser capsulotomy 3 months postoperatively without affecting the final BCVA. No other complications were observed in group B.
Retinal detachment is the most dangerous complication of intraocular surgery in highly myopic eyes, with an incidence ranging from 0% to 8% in clear lens extraction for myopiaCitation16,Citation43,Citation44 and an incidence ranging from 0.61% to 4.8% for anterior chamber phakic IOL for myopia.Citation18,Citation45–Citation48 However, no cases of retinal detachment occurred in this study. This may be attributed to careful preoperative evaluation of the retina, exclusion of cases with suspicious retina or retinal tears, and exclusion of cases showing extreme myopia because of unavailability of TICL >−18 D and of TIOL <+6 D. The short follow-up period of 6 months may be another reason for the zero incidence of retinal detachment.
Both procedures show predictable results with slightly (but not statistically significant) better refractive and visual results in the TIOL group. However, the loss of accommodation in the TIOL group represents a major disadvantage for its use in younger patients. However, the TIOL is essentially a minor modification of the routine phacoemulsification procedure, while the TICL requires new skills and instruments. Additionally, the TICL is much more expensive than the TIOL. However, the rare but extremely serious complication of retinal detachment with refractive lens extraction represents a major risk, while the worst two complications associated with TICL are both correctable, ie, glaucoma can be corrected by TICL explantation and cataract can be corrected by TICL explantation and phacoemulsification with TIOL implantation. That is why refractive lens exchange with TIOL implantation should be used only when no other refractive solution is available to solve the refractive problem of a really demanding patient to get rid of his/her spectacles.
Our study was limited by two main factors. 1) The short follow-up period may have limited the evaluation of long-term complications and 2) the intergroup age differences and the nonrandomized design may have served as sources of potential bias.
Conclusion
The choice of a suitable procedure to correct myopic astigmatism is complex because there are many advantages and disadvantages to the options that are available. Both the procedures we investigated show predictable results with low complication rates and good visual results, but the loss of accommodation in the TIOL group is a major disadvantage that suggests that TICL should be used for myopic astigmatism treatment in younger patients even though TICL is more expensive.
Acknowledgments
The abstract of this article was presented at the XXXIV Congress of the ESCRS in Copenhagen as a presented poster talk with interim findings. The poster’s abstract was published in “Poster Abstracts” at the XXXIV Congress of the ESCRS in Copenhagen Journal with the link below to the abstract http://www.escrs.org/Copenhagen2016/programme/poster-village-details.asp?id=26842&day=0.
Disclosure
The authors report no conflicts of interest in this work.
References
- SandersDRSchneiderDMartinRToric implantable col-lamer lens for moderate to high myopic astigmatismOphthalmology20071141546117198849
- SandersDRVukichJADoneyKGastonMUS Food and Drug Administration clinical trial of the implantable contact lens for moderate to high myopiaOphthalmology2003110925526612578765
- NettoMVMohanRRAmbrósioRJrHutcheonAEZieskeJDWilsonSEWound healing in the cornea: a review of refractive surgery complications and new prospects for therapyCornea200524550952215968154
- DayanirVAzarDTLASIK complicationsYanoffMDukerJOphthalmology2nd edSt LouisMosby2002179185
- AbadJCAzarDTCurrent concepts, classification, and history of refractive surgeryYanoffMDukerJOphthalmology2nd edSt LouisMosby2004123132
- ApplegateRAHowlandHCRefractive surgery, optical aberrations, and visual performanceJ Refract Surg19971332952999183761
- AlfonsoJFFernández-VegaLFernandesPGonzález-MéijomeJMMontés-MicóRCollagen copolymer toric posterior chamber phakic intraocular lens for myopic astigmatism, one-year follow-upJ Cataract Refract Surg201036456857620362847
- Ferrer-BlascoTMontés-MicóRPeixoto-de-MatosSCGonzález-MéijomeJMCerviñoAPrevalence of corneal astigmatism before cataract surgeryJ Cataract Refract Surg2009351707519101427
- MendicuteJIrigoyenCAramberriJOndarraAMontés-MicóRFoldable toric intraocular lens for astigmatism correction in cataract patientsJ Cataract Refract Surg200834460160718361982
- DickHBAlióJBianchettiMToric phakic intraocular lens; European multicenter studyOphthalmology2003110115016212511361
- SandersDRDoneyKPocoMICL in Treatment of Myopia (ITM) Study GroupUnited States Food and Drug Administration clinical trial of the implantable collamer lens (ICL) for moderate to high myopia; three-year follow-upOphthalmology200411191683169215350323
- RuhswurmIScholzUZehetmayerMHanselmayerGVassCSkorpikCAstigmatism correction with a foldable toric intraocular lens in cataract patientsJ Cataract Refract Surg20002671022102710946194
- TehraniMDickHBIncisional keratotomy to toric intraocular lenses: an overview of the correction of astigmatism in cataract and refractive surgeryInt Ophthalmol Clin20034334352
- MendicuteJIrigoyenCRuizMIllarramendiIFerrer-BlascoTMontés-MicóRToric intraocular lens versus opposite clear corneal incisions to correct astigmatism in eyes having cataract surgeryJ Cataract Refract Surg200935345145819251137
- GoldbergMFClear lens extraction for axial myopia. An appraisalOphthalmology19879455715823299203
- BarraquerCCavelierCMejiaLFIncidence of retinal detachment following clear-lens extraction in myopic patients. Retrospective analysisArch Ophthalmol199411233363398129658
- HollandELaneSHornJDErnestPArleoRMillerKMThe AcrySof Toric intraocular lens in subjects with cataracts and corneal astigmatism, a randomized, subject-masked, parallel-group, 1-Year StudyOphthalmology2010117112104211120846724
- AlióJLde la HozFPérez-SantonjaJJRuiz-MorenoJMQuesadaJAPhakic anterior chamber lenses for the correction of myopia: a 7-year cumulative analysis of complications in 263 casesOphthalmology1999106345846610080200
- BenEzraDCohenEKarshaiIPhakic posterior chamber intraocular lens for the correction of anisometropia and treatment of amblyopiaAm J Ophthalmol2000130329229611020407
- LacknerBPiehSSchmidingerGOutcome after treatment of ametropia with implantable contact lensesOphthalmology2003110112153216114597523
- MenezoJLPeris-MartinezCCisnerosALMartinez-CostaRPhakic intraocular lenses to correct high myopia: adatomed, Staar, and ArtisanJ Cataract Refract Surg2004301334414967266
- PesandoPMGhiringhelloMPTagliavacchePPosterior chamber collamer phakic intraocular lens for myopia and hyperopiaJ Refract Surg199915441542310445712
- Pineda-FernandezAJaramilloJVargasJJaramilloMGalindezAPhakic posterior chamber intraocular lens for high myopiaJ Cataract Refract Surg2004302277228315519075
- BylsmaSSZaltaAHFoleyEOsherRHPhakic posterior chamber intraocular lens pupillary blockJ Cataract Refract Surg200228122222222812498864
- GonversMBornetCOthenin-GirardPImplantable contact lens for moderate to high myopia: relationship of vaulting to cataract formationJ Cataract Refract Surg200329591892412781276
- Jiménez-AlfaroIBenítez del CastilloJMGarcía-FeijoóJGil de BernabéJGSerrano de La IglesiaJMSafety of posterior chamber phakic intraocular lenses for the correction of high myopia: anterior segment changes after posterior chamber phakic intraocular lens implantationOphthalmology20011081909911150270
- LacknerBPiehSSchmidingerGLong-term results of implantation of phakic posterior chamber intraocular lensesJ Cataract Refract Surg200430112269227615519074
- MenezoJLPeris-MartinezCCisneros-LanuzaALMartinez-CostaRRate of cataract formation in 343 highly myopic eyes after implantation of three types of phakic intraocular lensesJ Refract Surg200420431732415307392
- Sánchez-GaleanaCASmithRJSandersDRLens opacities after posterior chamber phakic intraocular lens implantationOphthalmology2003110478178512689902
- SarverEJSandersDRAstigmatic power calculations for intraocular lenses in the phakic and aphakic eyeJ Refract Surg200420547247715523959
- ThibosLNHornerDPower vector analysis of the optical outcome of refractive surgeryJ Cataract Refract Surg2001271808511165859
- Montés-MicóRFerrer-BlascoTContrast sensitivity loss in the peripheral visual field following laser in situ keratomileusisJ Cataract Refract Surg20073361120112217531714
- KohnenTMahmoudKBuhrenJComparison of corneal higher-order aberrations induced by myopic and hyperopic LASIKOphthalmology200511210169216140381
- RandlemanJBWoodwardMLynnMJStultingRDRisk assessment for ectasia after corneal refractive surgeryOphthalmology20081151375017624434
- KamiyaKShimizuKAizawaDIgarashiAKomatsuMSurgically induced astigmatism after posterior chamber phakic intraocular lens implantationBr J Ophthalmol200993121648165119692357
- Abela-FormanekCKrugerAJDejaco-RuhswurmIPiehSSkorpikCGonioscopic changes after implantation of a posterior chamber lens in phakic myopic eyesJ Cataract Refract Surg200127121919192511738905
- EmarahAMEl-HelwMAYassinHMComparison of clear lens extraction and collamer lens implantation in high myopiaClin Ophthalmol2010444745420505837
- TongJTMillerKMIntraocular pressure change after sutureless phacoemulsification and foldable posterior chamber lens implantationJ Cataract Refract Surg19982422562629530602
- PohjalainenTVestiEUusitaloRJLaatikainenLIntraocular pressure after phacoemulsification and intraocular lens implantation in nonglaucomatous eyes with and without exfoliationJ Cataract Refract Surg200127342643111255056
- ShingletonBJGamellLSO’DonoghueMWBaylusSLKingRLong-term changes in intraocular pressure after clear corneal phacoemulsification: normal patients versus glaucoma suspect and glaucoma patientsJ Cataract Refract Surg199925788589010404361
- CekicOBatmanCHyposecretion of aqueous: another mechanism for reduced intraocular pressure after phacoemulsificationJ Cataract Refract Surg1998245574
- KamiyaKShimizuKKobashiHIgarashiAKomatsuMThree-year follow-up of posterior chamber toric phakic intraocular lens implantation for moderate to high myopic astigmatismPLoS One201382e5645323409187
- ColinJRobinetAClear lensectomy and implantation of low-power posterior chamber intraocular lens for the correction of high myopiaOphthalmology199410111071128302541
- FritchCDRisk of retinal detachment in myopic eyes after intraocular lens implantation: a 7 year studyJ Cataract Refract Surg19982410135713609795851
- FossAJRosenPHCoolingRJRetinal detachment following anterior chamber lens implantation for the correction of ultra-high myopia in phakic eyesBr J Ophthalmol19937742122138494856
- AlióJLRuiz-MorenoJMArtolaARetinal detachment as a potential hazard in surgical correction of severe myopia with phakic anterior chamber lensesAm J Ophthalmol199311521451488430722
- Ruiz-MorenoJMAlióJLPérez-SantonjaJJde la HozFRetinal detachment in phakic eyes with anterior chamber intraocular lenses to correct severe myopiaAm J Ophthalmol1999127327027510088735
- BaikoffGPhakic anterior chamber intraocular lensesInt Ophthalmol Clin199131175861997455