
Abstract
Purpose
Long-term outcomes of pars plana vitrectomy (PPV) for macular edema (ME) associated with branch retinal vein occlusion (BRVO) have been previously reported, but the studies did not report the number of additional treatments after surgery. During 5 years of follow-up, we therefore investigated the efficacy and safety of PPV for BRVO and evaluated the incidence of additional treatments.
Methods
We retrospectively reviewed the medical records of 25 eyes of 24 patients who underwent PPV for ME associated with BRVO and were followed up for at least 5 years. Best-corrected visual acuity was measured, and foveal thickness was assessed by optical coherence tomography. Additional treatments were also investigated.
Results
The logarithm of the minimal angle of resolution (logMAR) improved from 0.53±0.23 at baseline to 0.16±0.25 at 5 years (P<0.0001). The foveal thickness decreased from 535±222 µm at baseline to 205±143 µm at 5 years (P<0.0001). For the eyes with residual ME, the following additional treatments were performed within 5 years of follow-up: sub-Tenon injection of triamcinolone acetonide in two eyes, intravitreal injection of bevacizumab in three eyes, grid laser photocoagulation in one eye, and direct photocoagulation of macroaneurysm in one eye. Additional surgeries were performed in two eyes: for one eye, phacoemulsification extraction of the ocular lens and intraocular lens implantation were performed because of cataract progression, and for the other eye, additional PPV was done for postoperative retinal detachment.
Conclusion
PPV was effective for resolution of ME associated with BRVO and improved visual acuity with a small number of additional treatments during long-term follow-up.
Introduction
Macular edema (ME) is a major cause of visual impairment in patients with branch retinal vein occlusion (BRVO). Many treatments for this disorder have been reported, such as photocoagulation,Citation1,Citation2 intravitreal or sub-Tenon injection of triamcinolone acetonide (STTA),Citation3–Citation9 intravitreal tissue plasminogen activator injection,Citation10,Citation11 and dexamethasone intravitreal implantation.Citation12 It has also been reported that pars plana vitrectomy (PPV) is effective for reducing ME and improving visual acuity (VA) in patients with BRVO.Citation2,Citation13–Citation18 Although the precise mechanism by which PPV reduces ME is unknown, it has been suggested that PPV may have beneficial effects on retinal ischemia by allowing oxygenated fluid to circulate in the vitreous cavity,Citation19 releasing vitreomacular attachment in persistent ME,Citation17,Citation20 improving perifoveal microcirculation,Citation21 and/or increasing the clearance of VEGF in the vitreous cavity.Citation22 Recently, intravitreal injection of anti-VEGF drugs (eg, bevacizumab, ranibizumab, and aflibercept) has been widely used and reported to be effective against ME associated with BRVO.Citation23–Citation28 However, recurrence of ME was often observed. In these cases, patients needed repeated injections, which could lead to increased risk of surgical complications as well as economic burdens. Therefore, it would be of benefit to the patients suffering from BRVO if the resolution of ME and improvement in VA could be maintained with minimal additional treatments. In this study, we investigated 5-year results of PPV for ME associated with BRVO to evaluate the efficacy and safety of the treatment as well as the incidences of additional treatments.
Subjects and methods
All procedures conformed to the tenets of the Declaration of Helsinki, and the study design was approved by the institutional review board of the Kobe City Medical Center General Hospital. The review board waived the need for written informed consent because the study design consisted of a retrospective chart review.
We retrospectively examined consecutive nonrandomized patients who underwent PPV for BRVO from September 2003 to October 2007 and completed a 5-year follow-up. Inclusion criteria were ME associated with BRVO, and best-corrected visual acuity (BCVA) was ≤0.6 in decimal VA. Exclusion criteria were proliferative diabetic retinopathy, vitreous hemorrhage, severe cataract, and other eye diseases that could contribute to visual loss. Eyes that were treated with PPV prior to the surgical intervention for BRVO were excluded. Eyes with previous scatter photocoagulation were included, but those with previous grid pattern photocoagulation were excluded.
BCVA was measured using Landolt ring charts and converted into the logarithm of the minimal angle of resolution (logMAR). Optical coherence tomography (OCT) was performed to measure foveal thickness using an OCT 2 (Carl Zeiss, Oberkochen, Germany), 3D OCT-1000 (Topcon, Tokyo, Japan), or Spectralis OCT (Heidelberg Engineering, Dossenheim, Germany). A standard three-port PPV was performed using a 20-G system or a 23-G system. A posterior vitreous detachment was induced if the cortical vitreous adhered to the retina. If the ME showed no improvement within 3 months after surgery, additional treatments such as STTA, grid laser photocoagulation, and intravitreal injection of bevacizumab (IVB) were performed.
All values were presented as mean ± standard deviation. Paired t-tests were used to compare preoperative and postoperative BCVAs. To compare preoperative and postoperative foveal thicknesses, Welch’s t-tests were used because of missing values. Differences were considered statistically significant when the P-values were <0.01 following the Bonferroni correction.
Results
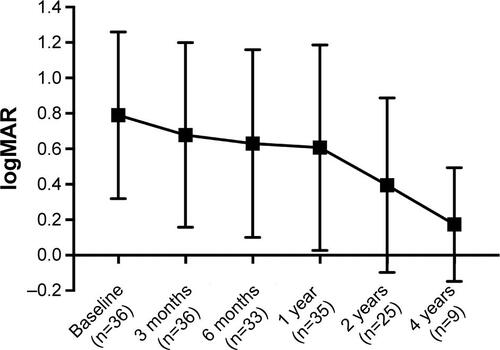
From September 2003 to October 2007, 61 eyes of 59 patients underwent PPV for ME associated with BRVO. Among these cases, 35 patients (36 eyes) withdrew before the 5-year follow-up visit. The change in BCVA of the dropped out patients is shown in Figure S1. As a result, 25 eyes of 24 patients with ME associated with BRVO were included in this study. All cases except one eye that had received STTA were treatment-naïve. The baseline characteristics of the study patients are summarized in . The mean age of the patients at surgery was 66.7±8.8 years (range, 51–87 years) and included 14 male (one case who underwent PPV in both eyes was counted as two) and 11 female eyes. The major branch of the retinal vein was occluded in 13 eyes, and the macular branch was occluded in 12 eyes. Fluorescein angiography revealed that 6 eyes were ischemic (≥5 disk areas of capillary nonperfusion) and 19 were nonischemic. The mean estimated elapsed time from the onset of the disease to surgery was 6.2±9.2 months (range: 0.5–36 months). The lens status before surgery was phakic in 23 eyes and pseudophakic in 2 eyes. For 22 of 23 phakic eyes, phacoemulsification of the ocular lens and intraocular lens (IOL) implantation were performed together with PPV to avoid postoperative nuclear sclerosis (). Intravitreal injection of triamcinolone acetonide (TA), arteriovenous sheathotomy, and internal limiting membrane peeling were combined with PPV in eight, four, and four eyes, respectively (). Endophotocoagulation was performed in five cases: four for intraoperative iatrogenic retinal tears and one for capillary nonperfusion ( and ). Temporary elevation of intraocular pressure (>21 mmHg) was observed in four eyes, which was controlled with temporary topical antiglaucoma medication in all cases (). In one case, rhegmatogenous retinal detachment (RD) developed 3 months after the initial PPV (). An additional PPV was performed, and the retina was reattached (case 2 in ). For one eye in which the physiological lens was preserved during the PPV, phacoemulsification and IOL implantation were performed at 19 months after the initial surgery because of cataract progression (case 7 in ). Five of the 23 eyes in which phacoemulsification and IOL implantation had been performed simultaneously or subsequently to PPV required Nd:YAG laser posterior capsulotomy within the 5-year follow-up (cases 1, 5, 7, 8, and 9 in ). Five of the 25 eyes required additional treatments for persistent ME that lasted >3 months postoperatively: STTA in two eyes, IVB in three eyes, grid laser photocoagulation in one eye, and direct photocoagulation of a macroaneurysm in one eye (cases 3, 4, 5, 6, and 10 in ). There were no eyes that underwent repeated STTA or IVB.
Table 1 Baseline characteristics of the patients
Table 2 Combined procedures with PPV
Table 3 Intra- and postoperative complications
Table 4 Characteristics of the eyes that required additional treatments
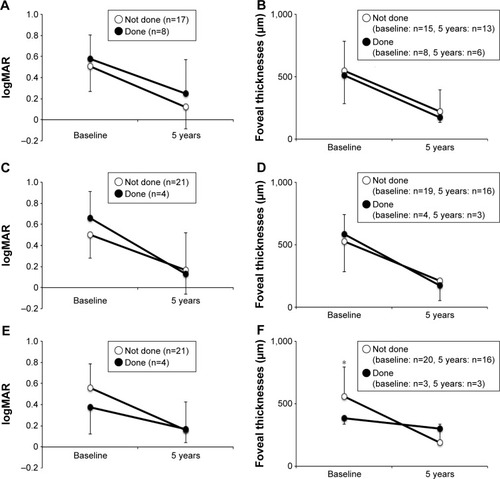
The mean logMAR converted from the BCVA was 0.53±0.23 at baseline (). Postoperatively, the mean BCVA changed to 0.43±0.29 (P=0.13) after 3 months, 0.33±0.27 (P=0.004) after 6 months, 0.32±0.30 (P=0.005) after 1 year, 0.26±0.29 (P=0.001) after 2 years, and 0.16±0.25 (P<0.0001) after 5 years (). The mean BCVAs at the 6-month visit or later after surgery were significantly improved compared with baseline. The mean foveal thickness at baseline was 535±222 µm (n=23; ). Postoperatively, the mean foveal thickness significantly decreased to 315±94 µm (P=0.0003) after 3 months (n=15) and was maintained at a significant reduction until the 5-year visit: 370±112 µm (P=0.008) after 6 months (n=12), 327±161 µm (P=0.002) after 1 year (n=16), 257±139 µm (P=0.0003) after 2 years (n=10), and 205±143 µm (P<0.0001) after 5 years (n=19; ). Baseline and 5-year results of BCVA and foveal thickness with or without combined procedures such as intravitreal injection of TA, arteriovenous sheathotomy, and internal limiting membrane peeling were not significantly different, except for the baseline foveal thickness with or without internal limiting membrane peeling ().
Figure 1 Changes in pre- and postoperative logMAR.
Abbreviation: logMAR, logarithm of the minimal angle of resolution.
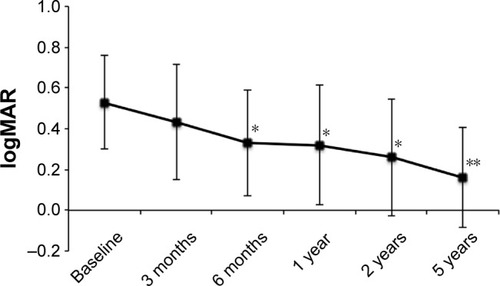
Figure 2 Changes in pre- and postoperative foveal thicknesses.
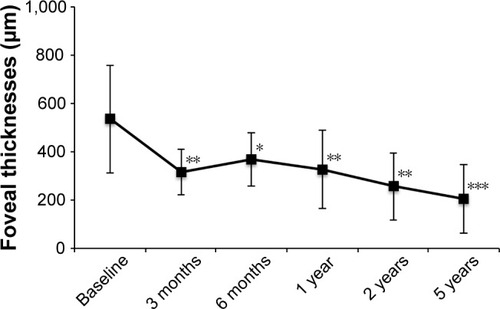
Figure 3 Five-year results of visual acuity (A, C, E) and foveal thickness (B, D, F) with or without simultaneously performed procedures such as intravitreal injection of TA (A, B), arteriovenous sheathotomy (C, D), or internal limiting membrane peeling (E, F).
Abbreviations: TA, triamcinolone acetonide; logMAR, logarithm of the minimal angle of resolution.
Discussion
This study provided long-term results of PPV for ME associated with BRVO. Tachi et alCitation17 reported that significant visual improvement was observed after PPV for BRVO in a follow-up period ranging from 12 to 32 months. Long-term outcomes of PPV with or without arteriovenous sheathotomy for BRVO have been previously reported.Citation14,Citation15,Citation29 These reports showed improvement in VA from the baseline 31–48 months after PPV; however, they did not report the incidences of additional treatments after the initial surgical intervention. In this study, we investigated 5-year results of PPV for ME associated with BRVO to evaluate the efficacy and safety of treatment as well as the incidences of additional treatments. Resolution of ME and improvement in VA were achieved at 3 and 6 months after the initial surgery, respectively, and lasted as long as 5 years ( and ). The effects of combined procedures such as intravitreal injection of TA, arteriovenous sheathotomy, and internal limiting membrane peeling, albeit small numbers, were not clear on 5-year results of BCVA and foveal thickness (). The most frequent additional treatment performed during the 5-year follow-up was Nd:YAG laser capsulotomy for posterior capsule opacification in 5 out of 23 eyes in which phacoemulsification and IOL implantation were performed simultaneously or subsequently to the PPV (22%; ). The number of eyes that received additional treatments against residual ME, such as STTA, IVB, grid laser photocoagulation, and direct photocoagulation of macroaneurysms, was five (20%; ), indicating that the majority of the eyes treated with PPV could maintain resolution of ME and improvement in VA without additional treatments for an extended period of time.
Recently, injections of anti-VEGF drugs such as bevacizumab, ranibizumab, pegaptanib, and aflibercept into the vitreous cavity have become a first-line treatment for ME associated with BRVO.Citation23–Citation28,Citation30 Campochiaro et alCitation31 reported 4-year outcomes for intravitreal injection of ranibizumab against BRVO and indicated that 50% of the patients had resolution of ME, defined as no intraretinal fluid without injection of ranibizumab for at least 6 months, with a mean follow-up of 50.2 months, suggesting that half of the patients could withdraw from anti-VEGF drugs longitudinally, while the other half still needed repeated injections, even in the fourth year.
Intravitreal anti-VEGF injections have been reported to have low complication rates. Recent studies reported that the incidences of rhegmatogenous RD after anti-VEGF injections were 0.013%–0.10%.Citation32–Citation34 Endophthalmitis occurred in 0.036–0.09% of the eyes after intravitreal injection of anti-VEGF drugs.Citation32,Citation35 On the other hand, Savastano et alCitation36 reported that RD developed in 1.77% of the eyes that underwent 25-G high-speed PPV. A recent large-scale study reported that the incidences of postoperative endophthalmitis were 0.020% (4 of 19,865 eyes), 0.028% (3 of 10,845 eyes), and 0.021% (1 of 4,717 eyes) for 20-G, 23-G, and 25-G systems, respectively.Citation37
Summarizing these reports, the risk of postoperative RD in PPV was 10- to 100-fold higher than that in intravitreal injection. Indeed, postoperative RD occurred in one case in the present study ( and ). In contrast, the incidences of postoperative endophthalmitis were not so much different between PPV and intravitreal injections. It is possible that multiple injections increased the risk of endophthalmitis, potentially more than that of a single PPV. Therefore, although the application of PPV should be restricted, it may have an advantage in cases that require repeated injections of anti-VEGF drugs for maintaining resolution of ME.
Limitations of this study involve the retrospective data collection and the relatively small number of cases. More than half of the patients did not complete 5-year follow-up. It is possible that the patients with poor VA stopped to come to hospital before 5-year follow-up. To minimize the bias, we analyzed the patients who had completed 5-year follow-up; however, we cannot eliminate the possibility described earlier. Nonuniformity of surgical procedure among cases, such as intravitreal injection of TA, arteriovenous sheathotomy, and internal limiting membrane peeling, is another drawback of this study. However, we believe that our study provides valuable insight into the long-term outcomes of PPV for BRVO.
Conclusion
PPV was effective for improvement in VA and resolution of ME associated with BRVO. The effects lasted at least 5 years with minimal additional treatments. Although the incidences of postoperative RD were higher than that in intravitreal injections, PPV may have an advantage in cases that require repeated injections of anti-VEGF drugs, because a smaller number of additional treatments can avoid the risks associated with repeated injections. Further investigation is required to clarify whether PPV is also effective for anti-VEGF-treated eyes.
Acknowledgments
The authors confirmed no financial support was received for this study.
Supplementary material
Figure S1 Changes in pre- and postoperative logMAR of the patients who withdrew before the 5-year follow-up visit.
Abbreviation: logMAR, logarithm of the minimal angle of resolution.
Disclosure
The authors report no conflicts of interest in this work.
References
- The Branch Vein Occlusion Study GroupArgon laser photocoagulation for macular edema in branch vein occlusionAm J Ophthalmol19849832712826383055
- HarinoSBesshoKKidaTProspective multicenter study of visual outcomes following three different treatments for macular edema associated with branch retinal vein occlusion: a study by the Japanese BRVO study groupJpn J Ophthalmol201256325026122358585
- CekicOChangSTsengJJIntravitreal triamcinolone injection for treatment of macular edema secondary to branch retinal vein occlusionRetina200525785185516205563
- ChenSDSundaramVLochheadJPatelCKIntravitreal triamcinolone for the treatment of ischemic macular edema associated with branch retinal vein occlusionAm J Ophthalmol2006141587688316527226
- KaracorluMOzdemirHKaracorluSAResolution of serous macular detachment after intravitreal triamcinolone acetonide treatment of patients with branch retinal vein occlusionRetina200525785686016205564
- KawajiTHirataAAwaiNTrans-Tenon retrobulbar triamcinolone injection for macular edema associated with branch retinal vein occlusion remaining after vitrectomyAm J Ophthalmol2005140354054216139011
- LeeHShahGKIntravitreal triamcinolone as primary treatment of cystoid macular edema secondary to branch retinal vein occlusionRetina200525555155516077348
- OhJYSeoJHAhnJKHeoJWChungHEarly versus late intravitreal triamcinolone acetonide for macular edema associated with branch retinal vein occlusionKorean J Ophthalmol2007211182017460427
- PatelPJZaheerIKariaNIntravitreal triamcinolone acetonide for macular oedema owing to retinal vein occlusionEye2008221606416902493
- García-ArumíJMartinez-CastilloVBoixaderaABlascoHCorcosteguiBManagement of macular edema in branch retinal vein occlusion with sheathotomy and recombinant tissue plasminogen activatorRetina200424453054015300073
- MurakamiTTakagiHKitaMIntravitreal tissue plasminogen activator to treat macular edema associated with branch retinal vein occlusionAm J Ophthalmol2006142231832016876516
- HallerJABandelloFBelfortRJrOZURDEX GENEVA Study GroupRandomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusionOphthalmology201011761134.e1146.e20417567
- FigueroaMSTorresRAlvarezMTComparative study of vitrectomy with and without vein decompression for branch retinal vein occlusion: a pilot studyEur J Ophthalmol2004141404715005584
- KumagaiKFurukawaMOginoNLarsonEUemuraALong-term visual outcomes after vitrectomy for macular edema with foveal hemorrhage in branch retinal vein occlusionRetina200727558458817558320
- KumagaiKFurukawaMOginoNUemuraALarsonELong-term outcomes of vitrectomy with or without arteriovenous sheathotomy in branch retinal vein occlusionRetina2007271495417218915
- SaikaSTanakaTMiyamotoTOhnishiYSurgical posterior vitreous detachment combined with gas/air tamponade for treating macular edema associated with branch retinal vein occlusion: retinal tomography and visual outcomeGraefes Arch Clin Exp Ophthalmol20012391072973211760031
- TachiNHashimotoYOginoNVitrectomy for macular edema combined with retinal vein occlusionDoc Ophthalmol1999973–446546910896365
- YamamotoSSaitoWYagiFTakeuchiSSatoEMizunoyaSVitrectomy with or without arteriovenous adventitial sheathotomy for macular edema associated with branch retinal vein occlusionAm J Ophthalmol2004138690791415629280
- WilliamsonTHPoonWWhitefieldLStrothidisNJaycockPA pilot study of pars plana vitrectomy, intraocular gas, and radial neurotomy in ischaemic central retinal vein occlusionBr J Ophthalmol20038791126112912928281
- TakahashiMKHikichiTAkibaJYoshidaATrempeCLRole of the vitreous and macular edema in branch retinal vein occlusionOphthalmic Surg Lasers19972842942999101567
- NomaHFunatsuHSakataKMimuraTHoriSMacular microcirculation before and after vitrectomy for macular edema with branch retinal vein occlusionGraefes Arch Clin Exp Ophthalmol2010248344344519956967
- LeeSSGhosnCYuZVitreous VEGF clearance is increased after vitrectomyInvest Ophthalmol Vis Sci20105142135213820019364
- CampochiaroPAClarkWLBoyerDSIntravitreal aflibercept for macular edema following branch retinal vein occlusion: the 24-week results of the VIBRANT studyOphthalmology2015122353854425315663
- CampochiaroPAHafizGShahSMRanibizumab for macular edema due to retinal vein occlusions: implication of VEGF as a critical stimulatorMol Ther200816479179918362932
- CampochiaroPAHeierJSFeinerLBRAVO InvestigatorsRanibizumab for macular edema following branch retinal vein occlusion: six-month primary end point results of a phase III studyOphthalmology201011761102111220398941
- PaiSAShettyRVijayanPBClinical, anatomic, and electrophysiologic evaluation following intravitreal bevacizumab for macular edema in retinal vein occlusionAm J Ophthalmol2007143460160617306753
- RabenaMDPieramiciDJCastellarinAANasirMAAveryRLIntravitreal bevacizumab (Avastin) in the treatment of macular edema secondary to branch retinal vein occlusionRetina200727441942517420692
- StahlAAgostiniHHansenLLFeltgenNBevacizumab in retinal vein occlusion-results of a prospective case seriesGraefes Arch Clin Exp Ophthalmol2007245101429143617356824
- OhIKKimSOhJHuhKLong-term visual outcome of arteriovenous adventitial sheathotomy on branch retinal vein occlusion induced macular edemaKorean J Ophthalmol20082211518323698
- UdaondoPGarcia-DelpechSSalomDGarcia-PousMDiaz-LlopisMIntravitreal pegaptanib for refractory macular edema secondary to retinal vein occlusionClin Ophthalmol2011594194421792283
- CampochiaroPASophieRPearlmanJRETAIN Study GroupLong-term outcomes in patients with retinal vein occlusion treated with ranibizumab: the RETAIN studyOphthalmology2014121120921924112944
- DaySAcquahKMruthyunjayaPGrossmanDSLeePPSloanFAOcular complications after anti-vascular endothelial growth factor therapy in Medicare patients with age-related macular degenerationAm J Ophthalmol2011152226627221664593
- MeyerCHMichelsSRodriguesEBIncidence of rhegmatogenous retinal detachments after intravitreal antivascular endothelial factor injectionsActa Ophthalmol2011891707521176118
- WuLMartinez-CastellanosMAQuiroz-MercadoHTwelve-month safety of intravitreal injections of bevacizumab (Avastin): results of the Pan-American Collaborative Retina Study Group (PACORES)Graefes Arch Clin Exp Ophthalmol20082461818717674014
- RayessNRahimyEStoreyPPostinjection endophthalmitis rates and characteristics following intravitreal bevacizumab, ranibizumab, and afliberceptAm J Ophthalmol2016165889326944277
- SavastanoASavastanoMCBarcaFPetrarchiniFMariottiCRizzoSCombining cataract surgery with 25-gauge high-speed pars plana vitrectomy: results from a retrospective studyOphthalmology2014121129930424139124
- WuLBerrocalMHArevaloJFEndophthalmitis after pars plana vitrectomy: results of the Pan American Collaborative Retina Study GroupRetina201131467367821394065