
Abstract
Background
Central corneal thickness (CCT) can be used to assess the corneal physiological condition as well as the pathological changes associated with ocular diseases. It has an influence on the measurement of intraocular pressure and is being used as a screening tool for refractive surgery candidates. The aim of this study was to determine the median CCT among normal Pakistani population and to correlate CCT with age, sex, and refractive errors.
Methods
We conducted a retrospective analysis of 5,171 healthy eyes in 2,598 patients who came to Hashmanis Hospital, Karachi, Pakistan. The age of the patients ranged from 6 to 70 years. The refractive error was gauged by an auto-refractometer, and CCT was measured using Oculus Pentacam®.
Results
The median CCT of our study was 541.0 μm with an interquartile range (IQR) of 44.0 μm. The median age was 26.0 years (IQR: 8.0). Median spherical equivalent (SE) of the patients was −4.3 D (IQR: 3.3) with the median sphere value as −4.0 D (IQR: 3.8). Lastly, the median cylinder was −1.0 D (IQR: 1.3). Age has a weak negative correlation with CCT (r=−0.058) and shows statistical significance (P<0.001). Additionally, males had thinner CCT readings than females (P=0.001). The cylinder values, on the other hand, had a significant (P=0.004) and positive correlation (r=0.154). Three values showed no significant correlation: sphere (P=0.100), SE (P=0.782), and the left or right eye (P=0.151).
Conclusion
Among the Pakistani population, CCT was significantly affected by three variables: sex, age, and cylinder. No relationship of CCT was observed with the left or right eye, sphere, and SE.
Introduction
Central corneal thickness (CCT) is a key indicator of corneal health status and helps to assess corneal diseases. The normal corneal thickness is about 540 μm and mainly consists of the stroma, which is estimated at 450 μm in the center. The stroma provides vital structural integrity and plays a key role in helping maintain transparency.Citation1 It has been reported, however, that CCT follows a diurnal pattern being 10 μm thicker in the morning due to reduced evaporation of water from underneath the closed eyelids.Citation1,Citation2
Usually, CCT is measured using a device known as the ultrasonic pachymeter. With recent advances, however, it is possible to measure this value using Oculus Pentacam® (Pentacam HR; Oculus, Wetzlar, Germany), which maps the entire surface of the cornea. Additionally, it has been reported that CCT aids in estimating corneal barrier and endothelial pump function.Citation3
CCT is a measure of corneal rigidity and has an impact on the accuracy of intraocular pressure (IOP) measurement by applanation tonometry. A greater resistance is offered by thicker corneas to the applanation tonometer, resulting in an artificially higher IOP reading.Citation3–Citation5 In addition, many studies have demonstrated that CCT is greater in patients with ocular hypertension as compared to the general population.Citation6–Citation8 Furthermore, CCT is important in assessing eligibility in refractive surgery candidates where it is used to exclude those in danger of postoperative ectasia.Citation9
CCT in the general population is associated with many demographic and ocular factors. Recent studies have shown that sex, race and/or ethnicity, and age may influence CCT. Specifically, it is found to be thinner in older individuals, Mongolians, and African-Americans than in whites.Citation10–Citation12 It was found that CCT of normotensive Nigerian adults reduces with increasing age and is not influenced by sex, corneal curvature, and corneal diameter.Citation13 A German research showed a positive correlation with IOP, sex (men had thicker corneas), and spherical equivalent (SE),Citation14 whereas an Iraqi research showed negative correlation between CCT and age, but it was not affected by sex.Citation15
So far, two studies have already been conducted in Pakistan that examined the effect of age and ethnicity on CCT; however, these were limited in their sample size with 100Citation16 and 1,000 patients,Citation17 respectively. Additionally, the latter study only included adults and excluded those with refractive errors. We, therefore, wanted to study the effect of age, sex, and SE on CCT in a larger sample size of 5,171 eyes in the Pakistani population presenting to Hashmanis Hospital.
Methods
Study design
This was a retrospective analysis of 5,171 eyes in 2,598 patients who came to Hashmanis Hospital, Karachi, Pakistan. The study period lasted from January 2014 to December 2016. The study was approved by the Ethics Committee of Hashmanis Hospital, and informed consent was obtained for both inclusion in the study and for administration of the procedure.
Inclusion and exclusion criteria
All our patients underwent the routine eye examination: uncorrected visual acuity, best spectacle-corrected visual acuity, both cycloplegic and subjective refractive error, slit lamp examination, dilated retinal exam, keratometry, and Oculus Pentacam measurement.
Those with significant corneal pathology, such as scarring, edema, or dystrophy, were excluded. Additionally, those with a history of recent contact lens wear, ocular surgery, ocular trauma, glaucoma, or an IOP of greater than 22 mmHg were excluded. Lastly, patients who had evidence of systemic disease or pregnancy were also excluded.
Refraction
We measured refraction using an auto-refractometer (KR-800; Topcon Medical Systems, Inc., Fukuoka, Japan). Each refraction measurement was in diopters (D) and had three values: sphere, cylinder, and SE. The SE was defined as the sum of the sphere value and half of the cylinder. Additionally, refractive outcomes were available in 4,915 eyes.
Oculus Pentacam
All patients underwent Oculus Pentacam measurement for the assessment of CCT. Every patient followed the same protocol during the scan. Their chin was positioned on the chin rest and, at the same time, their forehead was rested on the provided forehead strap. The patient was asked to stare at the blue fixation ring, while the examiner adjusted the focus and alignment of the machine. The machine marked the pupil at three points: the pupil edge, center, and corneal apex. Additionally, all patients were awake at least 1 hour prior to administration of the test. All scans were conducted between 10:00 AM and 4:00 PM.
This Pentacam system utilizes the blue light-emitting diode and a rotating Scheimpflug camera to take pictures of the anterior segment of the eye. At the time of study, the machine used Pentacam Software V1.20r87. We used the pachy apex value for CCT.
Classifications
First of all, we classified eyes into age groups by decades: 11–20, 21–30, 31–40, and 41–50 years. We had two different classifications for refractive outcomes. First, we divided each into a broad range of myopia (SE <−0.25 D), emmetropia (SE −0.25 to 0.25 D), and hyperopia (SE >0.25 D). Subsequently, we divided the myopic eyes into mild (SE >−3 D), moderate (SE −3 to −6 D), and severe myopia (SE <−6 D). Likewise, we divided the hypermetropic eyes into mild (SE 0.25 to 3 D) and moderate hypermetropia (SE >3 D).
Statistical analysis
We used AppSheet software to collect data into Google sheets, which were then imported into the Statistical Package for the Social Sciences v23 software. All subsequent analyses were carried out using the program. We used descriptive statistics to calculate the median and interquartile ranges (IQR) all values; median values were used as the data were not normally distributed, as indicated by Shapiro-Wilk test.
Subsequently, Mann-Whitney U test was used to test for statistical significance between sexes and eyes. For all other variables, Pearson product-moment correlation was used. Lastly, the linear regression model was used for values that were statistically significant.
Results
General characteristics
We retrospectively analyzed the data for 5,171 eyes (2,573 left; 2,598 right) in 2,598 patients (1,596 males; 1,002 females) who came to Hashmanis Hospital for refractive surgery. The median CCT for this study was 541.0 μm with an IQR of 44.0 μm. The median age was 26.0 years (IQR: 44.0). Median SE of the patients was −4.3 D (IQR: 3.3) with the median sphere value as −4.0 D (IQR: 3.8). Lastly, the median cylinder was −1.0 D (IQR: 1.3 D). This is shown in along with the P-values and r-values.
Table 1 General characteristics
Correlation with age
When analyzing the relationship of age with CCT, we divided our sample into four age groups: 11–20, 21–30, 31–40, and, 41–50 years. The median CCTs of these groups were found to be progressively falling, being 547.0 μm (IQR: 49), 540.0 μm (IQR: 45), 537.0 μm (IQR: 42), and 535.0 μm (IQR: 39), respectively (P-value =0.001). Other age groups were excluded due to low sample size. This is shown in . Additionally, it can be seen that age is weakly but negatively correlated with CCT with an r-value of −0.058. This relationship is shown in .
Figure 1 Correlation of central corneal thickness with age.
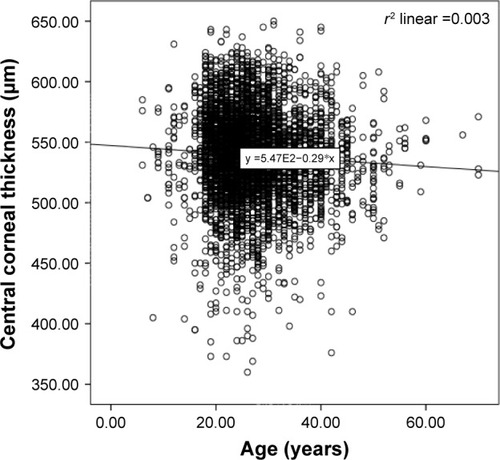
Table 2 Central corneal thickness by age groups
Association with sex
The median CCT in male individuals was 538.0 μm (IQR: 45), whereas in females it was 542.0 μm (IQR: 44). Males had statistically significant thinner CCT readings than females (P=0.001). This is shown in .
Table 3 Central corneal thickness by sex
Correlation with spherical equivalent
We found no statistical significance when correlating all refractive errors with CCT (P=0.782). The median CCT was 541.0 μm (IQR: 44), 540.0 μm (IQR: 50), and 542.0 μm (IQR 43) in myopic, emmetropic, and hyperopic patients, respectively. We ran a separate analysis for these major classifications and found no significance among the three (P=0.587, P=0.906, P=0.606, respectively).
When further sub-classified, those with severe myopia had a median CCT of 541 μm (IQR: 47), those with moderate myopia had a median CCT of 541 μm (IQR: 42), and those with mild myopia had a median CCT of 539 μm (IQR: 49). Additionally, patients with mild hypermetropia had a median CCT of 542 μm (IQR: 47) and those with severe hypermetropia had a median CCT of 544 μm (IQR: 39). The relationship between SE and CCT had a weakly positive correlation (r=0.004) but did not reach statistical significance (P=0.782). These data are shown in .
Correlation with astigmatism
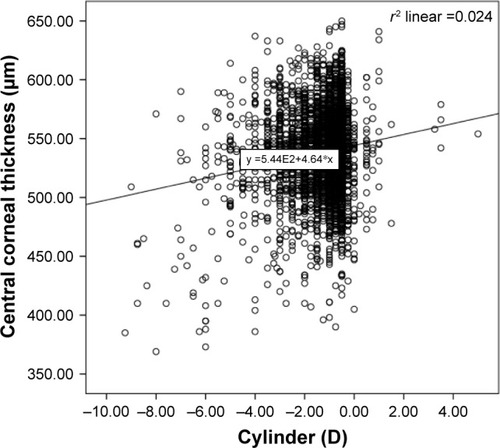
The cylinder values had a positive correlation with CCT, with an r-value of 0.154, and were found to be statistically significant (P≤0.001). This relationship is shown in .
Figure 2 Correlation of central corneal thickness with cylinder.
Discussion
The median CCT found in our study was 541.0 μm with IQR of 44.0 μm. Our results are similar when compared to the study performed by Channa et al, who found a mean CCT of 531.08 μm.Citation16 However, another study performed in the country by Tayyab et al reported a significantly thinner mean CCT of 503.96 μm.Citation17 The first study, like ours, was conducted in Karachi, which is at a far lower elevation when compared to Islamabad, which is the location of the latter study. This may explain the difference between the studies as it has been theorized that CCT is thinner in those who are at a higher altitude; however, the mechanism of this effect is yet to be understood.Citation18
Age is an important factor that affects corneal measurements. In our sample, age had a statistically significant and weak negative correlation with the median CCT reading (P<0.001, r=−0.058). Tayyab et al agree with our finding and found a decrease of 0.12 μm in CCT per year.Citation17 Other studies around the globe had similar results. For example, a research in Tehran concluded that volunteers younger than 20 years had thicker corneas when compared to those who were older.Citation19 The sub-Saharan study also showed that CCT values decreased significantly with older age (P=0.002).Citation20 However, not all studies agree, with one study in a large population in the USA showing no association of CCT with age.Citation21
In our study, we showed that men had significantly thinner corneas than females (P=0.001) with a median CCT of 538 μm and 542 μm, respectively. Another study carried out in KarachiCitation16 did not find a significant relationship of CCT with variables like age, sex, or presence of comorbidity. Conversely, in Japanese, African, and Chinese studies, it was found that men had thicker CCTs.Citation20,Citation22,Citation23 CCT has been said to have a diurnal variation in thickness.Citation24 Additionally, CCT in females has been linked to additional variables such as oral contraceptive pill (OCP) useCitation25 and menstrual cycle.Citation26 Perhaps, these factors could explain the discrepancy between our data and that of the global community, as we did not account for these.
We found astigmatism to have a significant positive correlation with CCT (P<0.001, r=0.154). A few papers have looked at this relationship previously. For example, one paper found a thicker CCT in patients with against the rule astigmatism.Citation27 Another study tried to find the relationship between CCT and surgically induced astigmatism. The study found a negative correlation postoperatively that was lost after 2 months.Citation28 We recommend further investigation into this relationship.
The SE in our research did not seem to have a significant correlation with CCT (P=0.782). Also, there was a negative but insignificant correlation between sphere component and CCT (P=0.100, r=−0.024). A similar research was conducted in China and no relationship was found between the SE and the CCT, as in our study.Citation29 Conversely, a study in Iraqi people found a statistically significant positive correlation with the same variables.Citation15 As shown in , the thickest corneas appear at the end of the two refractive spectrums: severe myopia and moderate hypermetropia. We, therefore, suspected that a separate analysis of the three classifications would yield a significant correlation. However, this was not found to be the case.
Table 4 Central corneal thickness divided by refractive classifications
Several limitations must be kept in mind while reading this paper. Firstly, this is a retrospective study and, therefore, all associated limitations must be considered. Secondly, since this study was conducted in a single city, the effects of the environment could not be assessed. Lastly, factors affecting the female CCT, like the menstrual cycle and OCP use, were not known.
Conclusion
The median CCT in Pakistani population was 541.0 μm. CCT was significantly affected by three variables: sex, age, and cylinder. No relationship of CCT was seen with the left or right eye, sphere, and SE.
Acknowledgments
The research was funded by Hashmanis Foundation.
Disclosure
Dr Nauman Hashmani is the son of Dr Sharif Hashmani. Dr Misbahul Aziz is the chairman of the Ethics Committee at Hashmanis Hospital. The authors report no other conflicts of interest in this work.
References
- TasmanWJaegerEAOphthalmology13th edPhiladelphiaLippincott Williams & Wilkins2012
- YanoffMDukerJSAyadAFMatthewVBSoongHKMohsinARamos-EstebanJCKatzLJOphthalmologyChinaElsevier Saunders2014
- EhlersNBramsenTSperlingSApplanation tonometry and central corneal thicknessActa Ophthalmol (Copenh)197553134431172910
- HerndonLWChoudhriSACoxTDamjiKFShieldsMBAllinghamRRCentral corneal thickness in normal, glaucomatous, and ocular hypertensive eyesArch Ophthalmol19971159113711419298054
- OrssengoGJPyeDCDetermination of the true intraocular pressure and modulus of elasticity the human cornea in vivoBull Math Biol199961355157217883231
- BrandtJDBeiserJAKassMAGordonMOCentral corneal thickness in the Ocular Hypertension Treatment Study (OHTS)Ophthalmology2001108101779178811581049
- HermanDCHodgeDOBourneWMIncreased corneal thickness in patients with ocular hypertensionArch Ophthalmol2001119333433611231765
- ArgusWAOcular hypertension and central corneal thicknessOpthalmology19951021218101812
- HashemiHMehravaranSCentral corneal thickness measurement with Pentacam, Orbscan II, and ultrasound devices before and after laser refractive surgery for myopiaJ Cataract Refract Surg200733101701170717889763
- WolfsRCKlaverCCVingerlingJRGrobbeeDEHofmanAde JongPTDistribution of central corneal thickness and its association with intraocular pressure. The Rotterdam StudyAm J Ophthalmol199712367677729535620
- FosterPJBaasanhuJAlsbirkPHMunkhbayarDUranchimegDJohnsonGJCentral corneal thickness and intraocular pressure in a Mongolian populationOphthalmology199810569699739627643
- FaragherRGMulhollandBTuftSJSandemanSKhawPTAging and the corneaBr J Ophthalmol199781108148179486017
- IyamuEOsuobeniEAge, gender, corneal diameter, corneal curvature, and central corneal thickness in Nigerians with normal intra ocular pressureJ Optom2012528797
- HoffmannEMLamparterJMirshahiADistribution of central corneal thickness and its association with ocular parameters in a large central European cohort: the Gutenberg health studyPLoS One201388e6615823936291
- KadhimYJFarhoodQKCentral corneal thickness of Iraqi population in relation to age, gender, refractive errors, and corneal curvature: a hospital-based cross-sectional studyClin Ophthalmol2016102369237627932859
- ChannaRMirFShahMNAliAAhmadKCentral corneal thickness of Pakistani adultsJ Pak Med Assoc200959422522819402284
- TayyabAMasrurAAfzalFIqbalFNaseemKCentral corneal thickness and its relationship to intra-ocular and epidemiological determinantsJ Coll Physicians Surg Pak201626649449727353987
- PatyalSAroraAYadavASharmaVKCorneal thickness in highlandersHigh Alt Med Biol2017181566027996304
- HashemiHYazdaniKMehravaranSCorneal thickness in a population-based, cross-sectional study: the Tehran Eye StudyCornea200928439540019411957
- MerciecaKOdoguVFiebaiBArowoloOChukwukaFComparing central corneal thickness in a sub-Saharan cohort to African Americans and Afro-CaribbeansCornea200726555756017525651
- PrasadAFryKHershPSRelationship of age and refraction to central corneal thicknessCornea201130555355521107245
- WangQLiuWWuYMaYZhaoGCentral corneal thickness and its relationship to ocular parameters in young adult myopic eyesClin Exp Optom2017100325025427757993
- NomuraHAndoFNiinoNShimokataHMiyakeYThe relationship between age and intraocular pressure in a Japanese population: the influence of central corneal thicknessCurr Eye Res2002242818512187477
- HarperCLBoultonMEBennetDDiurnal variations in human corneal thicknessBr J Ophthalmol19968012106810729059272
- KurtulBEInalBOzerPAKabatasEUImpact of oral contraceptive pills on central corneal thickness in young womenIndian J Pharmacol201648666566828066104
- GiuffrèGDi RosaLFiorinoFBubellaDMLodatoGVariations in central corneal thickness during the menstrual cycle in womenCornea200726214414617251801
- TurkeyHBostanciCTokluYRelationship between Type of Astigmatism and Central Corneal ThicknessMilanEuropean Society of Cataract and Refractive Surgeons2012
- WooSJLeeJHEffect of central corneal thickness on surgically induced astigmatism in cataract surgeryJ Cataract Refract Surg20032912401240614709304
- OliveiraCTelloCRitchRLiebmannJMCorrelation between central corneal thickness, scleral thickness and refractive errorInvest Ophthalmol Vis Sci20044513963